
Abstract
Background
Sedentary behavior occurs largely subconsciously, and thus specific behavior change techniques are needed to increase conscious awareness of sedentary behavior. Chief amongst these behavior change techniques is self-monitoring of sedentary behavior. The aim of this systematic review and meta-analysis was to evaluate the short-term effectiveness of existing interventions using self-monitoring to reduce sedentary behavior in adults.
Methods
Four electronic databases (PubMed, Embase, Web of Science, and The Cochrane Library) and grey literature (Google Scholar and the International Clinical Trials Registry Platform) were searched to identify appropriate intervention studies. Only (cluster-)randomized controlled trials that 1) assessed the short-term effectiveness of an intervention aimed at the reduction of sedentary behavior, 2) used self-monitoring as a behavior change technique, and 3) were conducted in a sample of adults with an average age ≥ 18 years, were eligible for inclusion. Relevant data were extracted, and Hedge’s g was used as the measure of effect sizes. Random effects models were performed to conduct the meta-analysis.
Results
Nineteen intervention studies with a total of 2800 participants met the inclusion criteria. Results of the meta-analyses showed that interventions using self-monitoring significantly reduced total sedentary time (Hedges g = 0,32; 95% CI = 0,14 − 0,50; p = 0,001) and occupational sedentary time (Hedge’s g = 0,56; 95% CI = 0,07 − 0,90; p = 0,02) on the short term. Subgroup analyses showed that significant intervention effects were only found if objective self-monitoring tools were used (g = 0,40; 95% CI = 0,19 − 0,60; p < 0,001), and if the intervention only targeted sedentary behavior (g = 0,45; 95% CI = 0,15-0,75; p = 0,004). No significant intervention effects were found on the number of breaks in sedentary behavior.
Conclusions
Despite the small sample sizes, and the large heterogeneity, results of the current meta-analysis suggested that interventions using self-monitoring as a behavior change technique have the potential to reduce sedentary behavior in adults. If future – preferably large-scale studies – can prove that the reductions in sedentary behavior are attributable to self-monitoring and can confirm the sustainability of this behavior change, multi-level interventions including self-monitoring may impact public health by reducing sedentary behavior.
Similar content being viewed by others

Background
Adults’ sedentary behavior levels are high in developed countries [1, 2]. A study pooling accelerometer data from adults (aged between 20 and 75 years) of four different European countries revealed an average sedentary time of 8.83 h/day [3]. Another study, in which results of accelerometer-measured sedentary time in older adults (aged above 60 years) were summarized, showed a daily mean of 9.40 h/day [4]. Reducing these high prevalence rates is a public health priority, as excessive sedentary behavior is associated with a plethora of negative health outcomes, ranging from non-communicable diseases (e.g. cardiovascular disease and type II diabetes) and poor mental health, to all-cause mortality [5,6,7,8]. Although no international consensus regarding specific guidelines for adults’ sedentary behavior has been reached, a meta-analysis conducted by Chau and colleagues suggested that adults’ sedentary time should be limited to 7 to 8 h/day [9]. Apart from general advise to reduce sedentary behavior, several national public health guidelines have also recommended to break up sedentary time every 30 min [10,11,12].
Unfortunately, evidence on effective intervention strategies to target adults’ sedentary behavior is still limited [5, 10, 13]. Existing sedentary behavior interventions have mainly focused on reducing occupational sedentary behavior, whereas there is a lot to be gained in other domains of sedentary behavior. Leisure time for example is proportionally the most sedentary domain [14]. Moreover, they have been largely informed by social-cognitive models of behavioral change (e.g. Theory of Planned Behavior) [15, 16]. Most of these models are based on an expectancy-value framework in which behavior is determined by expected outcomes and the value that is placed on them [17]. As such, these models do not adequately capture processes underlying unintentional and habit-like behavior. Given that a large part of sedentary behavior is habitual (i.e. it involves little reasoning and is performed without conscious decision making) [18], specific behavior change techniques (BCTs) are needed to better control sedentary behavior. One powerful strategy to disrupt habits is to change the circumstances, so that habit cueing does not occur anymore [19], or to alter the external cues that lead to habit execution [20]. However, these strategies have practical difficulties, since manipulating or avoiding cues is often impossible, or not always seen as ethical [21, 22]. Therefore, another way to disrupt undesired habits is preferred, namely by bringing habitual behavior and its context into conscious awareness. This might be achieved by means of self-monitoring [21].
Self-monitoring – defined by Michie and colleagues as keeping a record of a specified behavior as a method for changing behavior [23] – has been identified in the review of Gardner et al. as a promising behavior change technique to reduce sedentary behavior in adults [15]. Within the review of Gardner, the aim was to consider how sedentary behavior in adults might best be reduced, by describing the behavior change strategies used in sedentary behavior reduction intervention evaluations. However, it should be noted that the eligibility of interventions in the latter review was dependent on outcomes, such that any behavior change intervention was eligible where primary quantitative data were available in at least one indicator of sedentary behavior. Interventions that did not explicitly target sedentary behavior were thus included if sedentary behavior data were available. Given previous mentioned eligibility criteria, and the fact that research on sedentary behavior was still in its infancy at the time of the review, the majority of the studies included in review of Gardner aimed to increase physical activity rather than to reduce sedentary behavior [15]. As such, most of the included intervention studies used a pedometer as a self-monitoring tool [15].
More recently, bodily worn electronic devices, that allow to self-monitor sedentary behaviors, have emerged as a result of technological advances. These electronic devices have reduced the burden (i.e. time and task demand) of traditional paper-based methods and have increased assessment accuracy, which might have resulted in improved adherence, and in turn, greater achievement of sedentary behavior goals [24].
Despite the large potential for behavior change and the rise of bodily worn electronic devices to self-monitor sedentary behavior, it remains unclear how effective this behavior change technique is to reduce sedentary behavior in adults. Therefore, this study aimed to systematically review and evaluate the existing evidence regarding the effectiveness of interventions using self-monitoring to reduce sedentary behavior in adults by means of a meta-analysis. Additionally, the current meta-analysis aimed to identify factors moderating the observed effectiveness. Firstly, the dose-response relationship will be explored by testing the moderating effect of the intervention duration. Based on previous physical activity research, it can be hypothesized that longer interventions might yield better results [25]. Secondly, the moderating effect of the specific self-monitoring tool will be assessed. Given that paper-based diaries or online recording forms of sedentary behavior are time-consuming, and often subject to error and recall bias [26], we expect higher effect sizes in intervention studies using objective self-monitoring tools. Moreover, better effects are expected from tools specifically developed to monitor sedentary behavior, compared to tools in which the main aim is to track physical activity. Thirdly, it will be examined if age acts as a moderator in the observed effectiveness. Considering the higher sedentary time [27], it might be expected that older adults have more potential to reduce their sedentary time. However, the stronger habits developed for sedentary behavior [16], and the experienced difficulties both while working with electronic devices [28], and by standing – due to for example pain, fatigue, and functional limitations [29, 30] – might be important barriers for older adults to reduce their sedentary time by means of self-monitoring. Fourthly, the moderating effect of health status will be tested, as it might be that participants with overweight/obesity or other clinical conditions might be more motivated to reduce their sitting time or find it harder. Fifthly, the intervention content will be included as a moderator in order to examine if self-monitoring in itself is enough to achieve behavior change or if it should be combined with other behavior change techniques. Finally, the focus of the intervention will be included as a moderator. Previous research has suggested that interventions targeting only sedentary behavior have a larger impact compared to interventions targeting both physical activity and sedentary behavior [31].
Methods
This review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines (see Additional file 1). The protocol of this review (see Additional file 2) was registered with PROSPERO, which is an internationally database of prospectively registered systematic reviews in health and social care (registration ID: CRD42018112735).
Data sources and search strategy
A systematic literature search of four electronic databases (PubMed, Embase, Web of Science, and The Cochrane Library) was performed in October 2018 – and updated at the end of May 2019 – to detect intervention studies meeting the inclusion criteria. Additionally, forward and backward reference checking of the included papers was applied, and grey literature was searched – as recommended in the current Cochrane Collaboration guidelines – using Google Scholar, and the International Clinical Trials Registry Platform. If an intervention trial was detected using the grey literature search, authors were contacted to request unpublished data. The search strategy was developed using the PICO (population, intervention, comparison, outcome) acronym. The population of interest was adults, the intervention included self-monitoring, the comparison group received no intervention or an intervention without self-monitoring, and (one of) the study primary outcome(s) was sedentary behavior. The search was limited to articles published in English between the beginning of 2000 and the end of May 2019. This start date was chosen since most older studies used the construct sedentary behavior as a synonym for physical inactivity. Details on the search strategy – which was adapted to the specific features of each database – are presented in Table 1.
After running the search strategy, duplicates were removed. Subsequently, the studies were screened by title, and abstract by the first author (SC). After this first selection, full texts were independently screened by two reviewers (SC and DVD) to determine their eligibility based on the inclusion criteria. When doubt regarding the inclusion of a study persisted, a third reviewer (ADS) was consulted.
Study selection
Studies were eligible for inclusion if they were conducted in adults with an average sample age of 18 years and above, and if they were assessing the short-term effectiveness of sedentary behavior interventions, included self-monitoring as a behavior change technique, and used a controlled intervention trial design (i.e. [cluster-]randomized controlled trial or non-randomized controlled trial). Short-term effectiveness was defined as effectiveness reported immediately post intervention. Interventions were considered to use self-monitoring as a behavior change technique, if the participants were asked to keep a record of their sedentary behavior or physical activity as a method for changing behavior [23]. Self-monitoring had to be an explicitly stated behavior change technique, as opposed to occurring as part of completing measures for research purposes. This could for example take the form of a diary, completing a questionnaire about their behavior, in terms of type, frequency, duration and/or intensity, and/or the use of an electronic device. Interventions were included in the current review if they aimed at either 1) the reduction of total sedentary behavior, 2) the reduction of domain-specific sedentary behavior (e.g. occupational sedentary behavior, leisure time sedentary behavior), or 3) the increase in the number of sedentary behavior interruptions. Interventions in which the sole aim was to increase physical activity were excluded as previous research has indicated that these interventions revealed no, or only small effects on sedentary behavior [13].
Data extraction
Data were extracted from the published articles when available and authors were contacted to request missing data. Data extraction was done by SC and DVD independently using a standardized form and included: source characteristics (i.e. author, year of publication, and country of publication); study design; sample characteristics (i.e. sample size, age, gender, healthy vs clinical); intervention characteristics (i.e. duration, focus, self-monitoring, other behavior change techniques,); control characteristics (i.e. no intervention or other behavior change techniques); sedentary behavior measure(s) (i.e. objective vs self-reported, total sedentary behavior vs domain-specific sedentary behavior and measurement instrument) and sedentary behavior outcome data (i.e. the means and standard deviations of each group for both pre and post assessment, or mean changes and SD differences, or F values for group differences between changes). Follow-up measurements were not extracted, as the majority of the included studies did not report/analyze long-term effectiveness. Consensus was used to resolve disagreement regarding the data extraction. If consensus could not be reached, inconsistencies were discussed with a third reviewer (ADS).
Quality assessment
Methodological study quality was assessed using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for quantitative studies (https://merst.ca/ephpp/). Studies were independently reviewed by two researchers (SC and LP) and disagreements were resolved through discussion. Each of the following aspects were rated as weak, moderate or strong, using the EPHPP: selection bias, study design, confounders, blinding, data collection methods, withdrawals and drop-outs, intervention integrity and analyses. Because blinding of participants was not feasible in the context of self-monitoring based interventions aimed at the reduction of sedentary behavior, the overall risk of bias was calculated for each study without taking into account the blinding score. The impact of the study quality on overall effects was assessed by sensitivity analyses (see below).
Data analysis
Meta-analyses
Meta-analyses were conducted using Comprehensive Meta-analyses software version 3.3.070 (Biostat Inc., Englewood, NJ, USA). For each study an effect size was calculated with Hedges’ formula correcting for small samples [32]. By calculating Hedge’s g, all effect sizes were transformed to a common metric, which enabled us to include different outcome measures in the same analysis [33]. Subsequently, the unadjusted difference in means was calculated using the absolute time spent sedentary (min/day) as an effect size to gain insight into the difference in sedentary time between the intervention and the control groups. Random effects models were used for the meta-analyses. The random effects models estimated the mean of a distribution of effects [33]. Findings of the meta-analysis were presented using forest plots.
Test of heterogeneity and moderation analyses
The existence of heterogeneity was assessed using the Cochrane’s Q test, and the I2 statistics. A Q-value with a significance of p ≤ 0.05 was considered significant heterogeneity, while for the I2, a cut-off point of 50% was considered indicative of high heterogeneity [34]. If high heterogeneity was present, moderator analyses were conducted to test whether the heterogeneity could be explained by differences in 1) the intervention duration (≤ 12 weeks vs > 12 weeks), 2) the main purpose of the self-monitoring tool (sedentary behavior tool vs physical activity tool), 3) the way of self-monitoring (self-reported vs objective monitoring), 4) the age group of the participants (mean age ≤ 60 years vs mean age > 60 years) 5) the health status of the participants (healthy vs overweight/obese or other clinical condition), 6) the intervention content (only self-monitoring and general information on the link between behavior and health outcome vs combined with other behavioral change techniques) and 7) the focus of the intervention (only sedentary behavior or multiple behaviors). The median was used to calculate the cut-off point for intervention duration and mean age. The main purpose of the self-monitoring tool was determined using websites from manufacturers and the scoping review of Sander et al. [35] (see Additional file 2).
Sensitivity analyses and publication bias check
Sensitivity analyses were carried out to check the robustness of the statistical analysis. Concretely, main analyses were repeated without the study of Wyke et al. [36], as this study might have affected the results due to the large sample size and hence large contribution to the meta-analysis. Main analyses were also repeated without low quality studies, without cluster-randomized controlled trials, and without studies using subjective measurement instruments. The presence of publication bias was assessed using a funnel plot and Egger’s regression test.
Results
Study characteristics
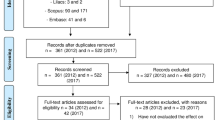
Figure 1 displays the number of studies identified, screened and excluded at each stage of the review process using the PRISMA flowchart. As a result, 19 articles met the inclusion criteria [36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52]. Of these, one study [53] was not included in the quantitative syntheses, as information was only provided on the longest bout of sedentary behavior.

PRISMA flowchart
Characteristics of the included studies are presented in Table 2. The majority of the included studies used a pretest posttest control group design (11/19) [36, 37, 39,40,41, 44, 46, 48, 50, 52, 54]. Five studies used a non-equivalent pretest posttest control group design [42, 45, 47, 49, 55], and three studies used a multigroup pretest posttest design [43, 51, 53]. Of the included studies, six studies were conducted in the USA [41, 46, 48, 50, 51, 55], four in the UK [40, 45, 49, 52], three in Belgium [43, 44, 54], two in Australia [37, 42] and one each in Canada [39], Japan [53] and Taiwan [47]. One study was conducted in multiple countries [36]. Only five studies were conducted in older adults (i.e. mean age above 60 years) [37, 39, 44, 48, 52], whereas 14 studies were conducted in adults (i.e. mean age between 18 and 60 years) [36, 40,41,42,43, 45,46,47, 49,50,51, 53,54,55]. More than half of the studies were conducted with healthy participants (11/19) [39, 42, 43, 45, 47,48,49, 51,52,53,54], five studies were conducted with overweight/obese participants [36, 40, 41, 50, 55], and one study each was conducted with Diabetes Type 2 patients [44], postmenopausal women diagnosed with stage I-III breast cancer [37] and Multiple Sclerosis patients [46]. Studies used a range of tools to self-monitor sedentary behavior. Specifically, six studies used a pedometer [41, 44, 47, 49, 50, 55], four studies used a traditional/electronic logbook or a questionnaire [43, 51, 52, 55], three studies used the Jawbone Up 24 [46, 48, 53], and one study each used the Shimmer accelerometer [54], the Fitbit One [39], the Gruve [40], the Lumoback [42], the Darma Crushion [45], the Garmin Vivofit 2 [37], and the SitFIT [36]. The shortest interventions lasted 1 week [53, 54], while the longest interventions lasted 1 year [40, 45]. Twelve studies focused only on sedentary behavior [38,39,40,41,42,43, 45, 49, 50, 52, 53, 55], whereas six studies focused on the combination of sedentary behavior and physical activity [36, 37, 44, 46,47,48]. One study focused on the combination of sedentary behavior, physical activity and dietary behavior [51]. Twelve studies objectively measured sedentary behavior [36, 37, 39, 41, 42, 44, 45, 48,49,50, 53, 54], four studies subjectively measured sedentary behavior [46, 47, 51, 52], and three studies combined both methods to estimate sedentary behavior [40, 43, 55].
Methodological study quality
Detailed results of the quality assessment are presented for each study in Table 3. Shortly, four studies were rated as strong [40, 44, 47, 50], five as moderate [36, 38, 41, 42, 49] and ten as weak [37, 39, 43, 45, 46, 48, 51,52,53, 55]. Weak ratings were frequently caused by recruitment issues, and lack of reporting on potential confounders and reasons for drop-out.
Effects of interventions including self-monitoring on total sedentary behavior
Figure 2 shows the effects of 16 interventions on total sedentary behavior using a forest plot. The average effect size across all studies was significant (Hedges g = 0,32; 95% CI = 0,14-0,50; p = 0,001) indicating that interventions including self-monitoring as a behavior change technique have the potential to reduce total sedentary behavior in adults. The overall mean difference for total sedentary time between intervention and control groups was 34,37 min/day (95% CI = 14,48-54,25) (see Additional file 3). As such, the reduction in sedentary time is on average 34,37 min larger in the intervention group, compared to the control group. Results of the heterogeneity tests (Q(16) = 44,43; p < 0,001; I2 = 66,24) revealed significant heterogeneity, and thus, moderation analyses were carried out. A priori, it was decided to conduct moderation analyses on the intervention duration, the main purpose of the self-monitoring tool, the way of self-monitoring, the age group of the participants, the health status of the participants, the intervention content, and the focus of the intervention. Since all the included interventions have, however, used self-monitoring in combination with a range of other behavior change techniques, it was impossible to include intervention content as a moderator.

Forest plot for total sedentary behavior
Results of the moderation analyses are presented in Table 4. The way of self-monitoring (i.e. subjective versus objective) was the only significant moderator (Q = 5,67; p = 0,02). Subgroup analyses showed that significant effects were found for interventions using objective self-monitoring tools (g = 0,40; 95% CI = 0,19-0,02; p < 0,001), whereas non-significant effects were found for interventions in which self-monitoring was done subjectively (g = − 0,02; 95% CI = -0,29-0,26; p = 0,90). The focus of the intervention was close to significance (Q = 2,88; p = 0,09). Interventions only focusing on sedentary behavior showed significant effects (g = 0,45; 95% CI = 0,15-0,75; p = 0,004), whereas interventions focusing on both sedentary behavior and physical activity did not show significant effects (g = 0,16; 95% CI = 0,001-0,31; p = 0,11). The main purpose of the self-monitoring tool (Q = 1,95; p = 0,16), the intervention duration (Q = 1,93; p = 0,17), the age group of the participants (Q = 0,17; p = 0,68), and the health status of the participants (Q = 0,03; p = 0,86) did not significantly moderate the intervention effects.
Funnel plot and Egger’s Test (t(16) = 2,24; p = 0,05) indicated that publication bias was unlikely to have influenced the results (see Additional file 4). Sensitivity analyses showed that the effect sizes largely remained within the 95% confidence interval after removing the study of Wyke et al. (g = 0,35; 95% CI = 0,16-0,55; p < 0,001), after removing low quality studies (g = 0,29; 95% CI = 0,06-0,52; p = 0,012), after removing cluster-randomized controlled trials (g = 0,32; 95% CI = 0,12-0,52; p = 0,001), and after removing studies using subjective measurement instruments (g = 0,40; 95% CI = 0,17-0,62; p = 0,001).
Effects of interventions including self-monitoring on domain-specific sedentary behavior
Six of the included interventions assessed the influence on domain-specific sedentary behavior. Of these, one study examined the effect on leisure screen time [51], four on occupational sitting time [42, 45, 47, 49], and one on different domains of sedentary behavior (i.e. at work, for transport, computer time, television time and other leisure time) [43]. Given the lack of results on transport-related sedentary behavior and leisure time sedentary behavior, a meta-analysis was only conducted on occupational sedentary behavior. Results of this meta-analysis, which are presented by means of the forest plot in Fig. 3, show that occupational sedentary behavior significantly reduced after the intervention including self-monitoring (Hedge’s g = 0,49; 95% CI = 0,07-0,90; p = 0,02). Although significant heterogeneity was detected (Q(5) = 21,44; p < 0,001; I2 = 81,34), no moderation analyses were conducted due to the limited number of studies (i.e. at least three studies were required per category to perform the moderation analyses) [56].

Forest plot for occupational sedentary behavior
Funnel plot and Egger’s Test (t(5) = 0,45; p = 0,68) indicated that publication bias was unlikely to have influenced the results (see Additional file 4). Sensitivity analyses were not performed as there were no outliers, no studies with extreme large sample size, and only three studies with moderate or strong quality. Sample sizes of the latter three studies were too small to conduct meaningful analyses [56].
Effects of interventions including self-monitoring on the number of breaks in sedentary behavior
Only four of the included studies examined the effect of an intervention using self-monitoring on the number of breaks in sedentary behavior. The effect size of one of the studies [49] exceeded the outlier threshold of three standard deviations above the average effect size. This study was thus removed from the analyses. Figure 4 presents the effects of the remaining three studies, as well as the average effect size by means of a forest plot. The average effect size was not significant (Hedge’s g = 0,10; 95%CI = -0,18-0,37; p = 0,50), meaning that the existing interventions including self-monitoring were not able to increase the number of breaks in sedentary behavior. No significant heterogeneity was found. Funnel plot and Egger’s Test (t(3) = 0,90; p = 0,53) indicated that publication bias was unlikely to have influenced the results (see Additional file 4). Again, sensitivity analyses were not performed due to the low number of studies.

Forest plot for the number of breaks in sedentary behavior
Discussion
Results of the current meta-analyses suggest that interventions including self-monitoring have the potential to reduce sedentary behavior in adults, and may thus play a critical role in promoting public health. If future studies can prove that the positive effects on sedentary behavior are attributable to self-monitoring, this finding will be in line with the results of a recent review by Gardner et al., which identified self-monitoring as one of the most promising behavior change techniques in sedentary behavior reduction interventions [15]. Given that the effect sizes in the current meta-analyses were rather small, more research should be conducted to examine 1) if the reduction in sedentary time is clinically relevant, and 2) how the reduction in sedentary time might be enhanced.
Specifically, our results indicated that both total sedentary behavior, and occupational sedentary behavior significantly reduced after implementing a self-monitoring based intervention. These reductions were, however, only significant if an objective self-monitoring tool was used. This moderating effect is not surprising, and can be explained by the fact that sedentary behavior is a largely subconscious behavior, and thus difficult – and time-consuming – to self-report [57]. Using objective self-monitoring tools may reduce the burden and increase the adherence to the intervention, and thus result in better achievements towards the behavioral goals [35].
Next, our results suggested that interventions only focusing on the reduction of sedentary behavior are more effective in comparison to interventions focusing on both the reduction of sedentary behavior and the increase of physical activity. This finding corresponds with the results of the review of Prince et al. [58]. In their review, Prince et al. showed that interventions only targeting sedentary behavior have the largest impact on sedentary behavior (i.e. a mean reduction of 91 min per day). Interventions targeting both sedentary behavior and physical activity resulted in a mean reduction of 35 min sedentary behavior per day [58]. This difference in effect size might be explained by the fact that participants of interventions targeting both sedentary behavior and physical activity are more likely to focus on physical activity due to 1) the clearer guidelines for physical activity compared to sedentary behavior, 2) the better known negative health consequences of too little physical activity compared to sedentary behavior, and 3) the fact that physical inactivity is still considered a synonym for sedentary behavior in the general population [59]. This might be important, as existing self-monitoring devices often combine the information on sedentary behavior and physical activity. For example, the device used in the study of Wyke et al. (i.e. the SitFIT) provided information on the number of steps and on the time spent sedentary [36]. Participants of this study seemed to mostly look at the number of steps taken, and paid less attention to the amount spent sitting. They indicated that they were more familiar with the step counts, and they considered the sitting time feedback as complicated [36]. Based on these results, it could be concluded that in order to reduce sedentary time 1) self-monitoring devices should be developed only focusing on sedentary behavior, and 2) information on sitting time should be optimized. However, as the aim of most behavioral interventions is to maximize health benefits, it might be useful to target both sedentary behavior and physical activity. Both behaviors have the ability to induce beneficial health effects, and are part of the 24 h movement continuum [60]. As such, changing one behavior also affects another behavior [60].
Other potential moderators that were tested (i.e. intervention duration, main purpose of the self-monitoring tool, age group and health status) did not account for differences between effect sizes. This is in contrast with our expectations, as we predicted larger effects in longer interventions, and in interventions of which the self-monitoring tool was specifically developed to reduce sedentary behavior. Longer interventions were expected to yield better results due to the dose-response relationship. Nevertheless, based on the current results it is unclear if the dose was higher in longer interventions, as information on frequency, and intensity was incomplete [61], but other differences in intervention content might have played a role as well. Self-monitoring tools specifically developed to reduce sedentary behavior were expected to generate larger gains due to the fact that they are more appropriate to bring sedentary behavior into conscious awareness. More research is needed to understand why this was not the case. It might, however, be that existing physical activity devices include much more behavior change strategies (e.g. providing feedback, social support etc.) compared to the existing sedentary behavior devices, which are still in infancy [35]. Given that several of the included moderators were not significant, part of the heterogeneity remains unexplained, and should thus be examined in future studies. One of the main factors, that was not examined due to the lack of studies, and that might have caused the unexplained heterogeneity are the other behavior changes techniques included in the interventions. For instance, some of the interventions applied environmental restructuring, by for example, implementing standing desks at work [45]. Implementing standing desks has been shown to be successful in reducing sedentary behavior [62, 63]. As such, these interventions might have yielded larger effects.
Finally, it should be acknowledged that the few studies that analyzed the effect on the number of breaks were not able to detect significant increases. This is disappointing as previous research has emphasized that interrupting bouts of sedentary behavior with light-intensity physical activity might yield beneficial health effects [64]. More research is needed to understand the underlying reasons for the non-significant effects, although the lack of information on breaks of the existing self-monitoring tools might have played a crucial role [35].
Strengths and limitations
The main strength of this study is that this is the first study, to our knowledge, to synthesize and statistically analyze the existing evidence regarding the effectiveness of interventions that use self-monitoring as a behavioral change technique to reduce sedentary behavior in adults. Moreover, the study used a comprehensive search strategy across multiple databases to identify all relevant studies, including grey literature. Both the screening of eligible studies, and the quality assessment has been conducted by two independent reviewers, and the quality score has been used to conduct sensitivity analyses.
The main limitation of the current study is the fact that self-monitoring was never implemented as a stand-alone strategy in the existing interventions. All the included interventions, however, comprised a range of behavior change techniques, and thus it remains uncertain if the effects are attributable to self-monitoring in itself, or if (a combination with) other behavior change techniques induced the behavioral change. Future studies should try to disentangle the combinations of behavior change techniques in order to gain insight into the working mechanism of the separate behavior change techniques as well as their interactions. By doing so, effective interventions of minimal costs and efforts can be created. Secondly, several of the included studies were pilot studies, and thus, performed with small sample sizes. Studies with small sample sizes are often underpowered to detect small changes in sedentary behavior. This might have led to an underestimation of the actual effect size. Thirdly, many of the included studies had a low methodological quality, due to weak ratings on selection bias, confounders and withdrawals. Although these weak ratings might be due to a lack or reporting, this might have affected the results. More high quality studies are needed with larger samples and objective measures in future research. Finally, we were only able to analyze short-term effects, as the majority of the included interventions did not report long-term effects. As such, it remains unclear whether intervention effects will be sustained over time. Insight into the long-term effectiveness is of great importance to evaluate the actual public health impact of self-monitoring based sedentary behavior interventions [65].
Conclusion
Results of the current meta-analysis – which included 17 intervention studies – suggest that interventions including self-monitoring show promise to reduce short-term sedentary behavior in adults. Important to note, however, is that all the included interventions have employed multiple behavior change techniques, whereby it is impossible to determine if the beneficial effects on sedentary behavior are attributable to self-monitoring in itself, or to (a combination with) other behavior change techniques. Moderation analyses indicated that the reductions in sedentary behavior are larger if an objective self-monitoring tool was used, and if the intervention only focuses on sedentary behavior. Still, from a public health point of view, combined physical activity and sedentary behavior interventions would be preferred but more research is needed to effectively integrate both behaviors in intervention strategies. If future studies can confirm that previous mentioned positive effects are long-lasting, the development and implementation of sedentary behavior interventions including self-monitoring as a key behavior change technique should be encouraged.
Availability of data and materials
The dataset is available from the corresponding author on reasonable request.
Abbreviations
- CG:
-
Control group
- CI:
-
Confidence interval
- EPHPP:
-
Effective Public Health Practice Project
- IG:
-
Intervention group
- N:
-
Number of participants
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analysis
References
Ng SW, BM P. Time use and physical activity: a shift away from movement across the globe. Obes Rev. 2012;13:659–80.
Matthews CE, George SM, Moore SC, Bowles HR, Blair A, Park Y, Troiano RP, Hollenbeck A, Schatzkin AJ. Amount of time spent in sedentary behaviors and cause-specific mortality in US adults. Am J Clin Nutr. 2012;95:437–45.
Loyen A, Clarke-Cornwell AM, Anderssen SA, Hagströmer M, Sardinha LB, Sundquist K, Ekelund U, Steene-Johannessen J, Baptista F, Hansen BH. Sedentary time and physical activity surveillance through accelerometer pooling in four European countries. Sports Med. 2017;47(7):1421-35.
Harvey JA, Chastin SF, Skelton DA. How sedentary are older people? A systematic review of the amount of sedentary behavior. J Aging Phys Act. 2015;23:471–87.
de Rezende LF, Lopes MR, Rey-López JP, Matsudo VK, do Carmo Luiz O. Sedentary behavior and health outcomes: an overview of systematic reviews. PLoS One. 2014;21:8.
Biswas A, Oh PI, Faulkner GE, Bajaj RR, Silver MA, Mitchell MS, Alter DA. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med. 2015;162:123–32.
Rosenberg DE, Bellettiere J, Gardiner PA, Villarreal VN, Crist K, Kerr J. Independent associations between sedentary behaviors and mental, cognitive, physical, and functional health among older adults in retirement communities. J Gerontol Ser A Biol Med Sci. 2016;71:78–83.
Ekelund U, Steene-Johannessen J, Brown WJ, Fagerland MW, Owen N, Powell KE, Bauman A, Lee I-M, Series LPA, Group LSBW. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet. 2016;388:1302–10.
Chau JY, Grunseit AC, Chey T, Stamatakis E, Brown WJ, Matthews CE, Bauman AE, HP v d P. Daily sitting time and all-cause mortality: a meta-analysis. PLoS One. 2013;8:e80000.
Vlaams Instituut voor Gezondheidspromotie en Ziektepreventie: Syntheserapport sedentair gedrag; 2015. http://www.vigez.be/files/voedingenbeweging/syntheserapportsedentairgedrag.pdf.
Canadian Society for Exercise Physiology: Canadian physical activity guidelines, Canadian sedentary behaviour guidelines; 2012. http://www.csep.ca/CMFiles/Guidelines/CSEP_Guidelines_Handbook.pdf.
Australian Government Department of Health: Australia’s physical activity and sedentary behaviour Guidelines; 2014. http://www.health.gov.au/internet/main/publishing.nsf/content/health-pubhlth-strateg-phys-act-guidelines.
Martin A, Fitzsimons C, Jepson R, Saunders DH, van der Ploeg HP, Teixeira PJ, Gray CM, Mutrie N. Interventions with potential to reduce sedentary time in adults: systematic review and meta-analysis. Br J Sports Med. 2015;49:1056–63.
van der Ploeg HP, Venugopal K, Chau JY, van Poppel MN, Breedveld K, Merom D, Bauman AE. Non-occupational sedentary behaviors: population changes in the Netherlands, 1975–2005. Am J Prev Med. 2013;44:382–7.
Gardner B, Smith L, Lorencatto F, Hamer M, Biddle SJ. How to reduce sitting time? A review of behaviour change strategies used in sedentary behaviour reduction interventions among adults. Health Psychol Rev. 2016;10:89–112.
Maher JP, Conroy DE. A dual-process model of older Adults’ sedentary behavior. Health Psychol. 2016;35:262–72.
Welk GJ. The youth physical activity promotion model: a conceptual bridge between theory and practice. Quest. 1999;51:5–23.
Conroy DE, Maher JP, Elavsky S, Hyde AL, Doerksen SE. Sedentary behavior as a daily process regulated by habits and intentions. Health Psychol. 2013;32:1149.
Verplanken B, W W. Interventions to break and create consumer habits. J Pub Policy Marketing. 2006;25:90–103.
Aarts H, Dijksterhuis A. The silence of the library: environment, situational norm, and social behavior. J Pers Soc Psychol. 2003;84:18.
Hermsen S, Frost J, Renes RJ, Kerkhof P. Using feedback through digital technology to disrupt and change habitual behavior: a critical review of current literature. Comput Human Behav. 2016;57:61–74.
Quinn JM, Pascoe A, Wood W, Neal DT. Can’t control yourself? Monitor those bad habits. Pers Soc Psychol Bull. 2010;36:499–511.
Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A, French DP. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health. 2011;26:1479–98.
Turner-McGrievy GM, Beets MW, Moore JB, Kaczynski AT, Barr-Anderson DJ, Tate DF. Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mHealth weight loss program. J Am Med Inform Assoc. 2013;20:513–8.
Kang M, Marshall SJ, Barreira TV, JO L. Effect of pedometer-based physical activity interventions: a meta-analysis. Res Q Exerc Sport. 2009;80:648–55.
Matthews CE, Welk GJ Use of self-report instruments to assess physical activity. Phys Act Assess Health-Relat Res. 2002;107:107–23.
Leask CF, Harvey JA, Skelton DA, Chastin SF. Exploring the context of sedentary behaviour in older adults (what, where, why, when and with whom). Eur Rev Aging Phys Act. 2015;12:4.
Kang NE, Yoon WC. Age-and experience-related user behavior differences in the use of complicated electronic devices. Int J Human-Comput Stud. 2008;66:425–37.
Chastin SF, Fitzpatrick N, Andrews M, DicCoce N. Determinants of sedentary behavior, motivation, barriers and strategies to reduce sitting time in older women: a qualitative investigation. Int J Environ Res Public Health. 2014;11:773–91.
Mcewan T, Tam-Seto L, Dogra S. Perceptions of sedentary behavior among socially engaged older adults. Gerontologist. 2016;57:735–44.
Chin SH, Kahathuduwa C, M B. Is sedentary behaviour unhealthy and if so, does reducing it improve this? Int J Clin Pract. 2017;71:e12925.
Hedges LV. Distribution theory for Glass's estimator of effect size and related estimators. J Educ Stat. 1981;6:107–28.
Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Introduction to meta-analysis. New Jersey: Wiley; 2011.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557.
Sanders JP, Loveday A, Pearson N, Edwardson C, Yates T, Biddle SJ, Esliger DW. Devices for self-monitoring sedentary time or physical activity: a scoping review. J Med Internet Res. 2016;18:e90.
Wyke S, Bunn C, Andersen E, Silva MN, van Nassau F, McSkimming P, Kolovos S, Gill JMR, Gray CM, Hunt K, et al. The effect of a programme to improve men’s sedentary time and physical activity: the European fans in training (EuroFIT) randomised controlled trial. PLoS Med. 2019;16:e1002736.
Adams MM, Davis PG, DL G. A hybrid online intervention for reducing sedentary behavior in obese women. Front Public Health. 2013;1:45.
Arrogi A, Bogaerts A, Seghers J, Devloo K, Vanden Abeele V, Geurts L, Wauters J, Boen F. Evaluation of stAPP: a smartphone-based intervention to reduce prolonged sitting among Belgian adults. Health Promot Int. 2017;34(1):16-27.
Ashe MC, Winters M, Hoppmann CA, Dawes MG, Gardiner PA, Giangregorio LM, Madden KM, McAllister MM, Wong G, Puyat JH, et al. “Not just another walking program”: everyday activity supports you (EASY) model-a randomized pilot study for a parallel randomized controlled trial. Pilot Feasibility Stud. 2015;1:4.
Biddle SJ, Edwardson CL, Wilmot EG, Yates T, Gorely T, Bodicoat DH, Ashra N, Khunti K, Nimmo MA, Davies MJ. A randomised controlled trial to reduce sedentary time in Young adults at risk of type 2 diabetes mellitus: project STAND (sedentary time ANd diabetes). PLoS One. 2015;10:e0143398.
Carr LJ, Karvinen K, Peavler M, Smith R, Cangelosi K. Multicomponent intervention to reduce daily sedentary time: a randomised controlled trial. BMJ Open. 2013;3:e003261.
Brakenridge CL, Fjeldsoe BS, Young DC, Winkler EAH, Dunstan DW, Straker LM, Healy GN. Evaluating the effectiveness of organisational-level strategies with or without an activity tracker to reduce office workers’ sitting time: a cluster-randomised trial. Int J Behav Nutr Phys Act. 2016;13:115.
De Cocker K, De Bourdeaudhuij I, Cardon G, Vandelanotte C. The effectiveness of a web-based computer-tailored intervention on workplace sitting: a randomized controlled trial. J Med Internet Res. 2016;18:e96.
De Greef KP, Deforche BI, Ruige JB, Bouckaert JJ, Tudor-Locke CE, Kaufman JM, De Bourdeaudhuij IM. The effects of a pedometer-based behavioral modification program with telephone support on physical activity and sedentary behavior in type 2 diabetes patients. Patient Educ Couns. 2011;84:275–9.
Edwardson CL, Yates T, Biddle SJH, Davies MJ, Dunstan DW, Esliger DW, Gray LJ, Jackson B, O'Connell SE, Waheed G, Munir F. Effectiveness of the stand more AT (SMArT) work intervention: cluster randomised controlled trial. BMJ. 2018;363:k3870.
Klaren RE, Hubbard EA, Motl RW. Efficacy of a behavioral intervention for reducing sedentary behavior in persons with multiple sclerosis: a pilot examination. Am J Prev Med. 2014;47:613–6.
Lin YP, Hong OS, Lin CC, Lu SH, Chen MM, Lee KC. A “sit less, walk more” workplace intervention for office workers: long-term efficacy of a quasi-experimental study. J Occup Environ Med. 2018;60:E290–9.
Lyons EJ, Swartz MC, Lewis ZH, Martinez E, Jennings K. Feasibility and acceptability of a wearable technology physical activity intervention with telephone counseling for mid-aged and older adults: a randomized controlled pilot trial. JMIR Mhealth Uhealth. 2017;5:e28.
Maylor BD, Edwardson CL, Zakrzewski-Fruer JK, Champion RB, Bailey DP. Efficacy of a multicomponent intervention to reduce workplace sitting time in office workers: a cluster randomized controlled trial. J Occup Environ Med. 2018;60:787–95.
Smith RD. Intervention to reduce sedentary time and improve cardiometabolic risk factors among sedentary employees; 2012. p. 58.
Spring B, Pellegrini C, McFadden HG, Pfammatter AF, Stump TK, Siddique J, King AC, Hedeker D. Multicomponent mHealth intervention for large, sustained change in multiple diet and activity risk behaviors: the make better choices 2 randomized controlled trial. J Med Internet Res. 2018;20:e10528.
White I, Smith L, Aggio D, Shankar S, Begum S, Matei R, Fox KR, Hamer M, Iliffe S, Jefferis BJ, et al. On your feet to earn your seat: pilot RCT of a theory-based sedentary behaviour reduction intervention for older adults. Pilot Feasibility Stud. 2017;3:23.
Kitagawa T, Higuchi Y, Todo E, Ueda T, Ando S, Murakami T. Tailored feedback reduced prolonged sitting time and improved the health of housewives: a single-blind randomized controlled pilot study. Women Health. 2019:1–12.
Arrogi A, Schotte A, Bogaerts A, Boen F, Seghers J. Short- and long-term effectiveness of a three-month individualized need-supportive physical activity counseling intervention at the workplace. BMC Public Health. 2017;17:52.
Adams MM, Davis PG, Gill DL. A hybrid online intervention for reducing sedentary behavior in obese women. Front Public Health. 2013;1:45.
Hempel S, Miles JN, Booth MJ, Wang Z, Morton SC, PGJSr S. Risk of bias: a simulation study of power to detect study-level moderator effects in meta-analysis, vol. 2; 2013. p. 107.
Pressley M, Afflerbach P. Verbal protocols of reading: the nature of constructively responsive reading. London: Routledge; 2012.
Prince S, Saunders T, Gresty K, Reid RD. A comparison of the effectiveness of physical activity and sedentary behaviour interventions in reducing sedentary time in adults: a systematic review and meta-analysis of controlled trials. Obes Rev. 2014;15:905–19.
van der Ploeg HP, Hillsdon M. Is sedentary behaviour just physical inactivity by another name? Int J Behav Nutr Phys Act. 2017;14:142.
Chaput J-P, Carson V, Gray C. Importance of all movement behaviors in a 24 hour period for overall health. Int J Environ Res Public Health. 2014;11:12575–81.
Howlett N, Trivedi D, Troop NA, AM C. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl Behav Med. 2018;9:147–57.
Chambers AJ, Robertson MM, Baker NA. The effect of sit-stand desks on office worker behavioral and health outcomes: a scoping review. Appl Ergon. 2019;78:37–53.
Shrestha N, Kukkonen-Harjula KT, Verbeek JH, Ijaz S, Hermans V, Pedisic Z. Workplace interventions for reducing sitting at work. Cochrane Database Syst Rev. 2018;12:CD010912.
Chastin SF, Egerton T, Leask C, Stamatakis E. Meta-analysis of the relationship between breaks in sedentary behavior and cardiometabolic health. Obesity (Silver Spring). 2015;23:1800–10.
Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89:1322–7.
Acknowledgements
The authors wish to thank all authors of the included studies for providing supplementary information when requested.
Funding
Delfien Van Dyck (FWO/12/PDO/158), Ann DeSmet (FWO/16/PDO/060) and Louise Poppe (11Z4716N) are supported by the Research Foundation Flanders (FWO). Sofie Compernolle is supported by the Special Research Fund of Ghent University (BOF/PDO/2018/0006/01).
Author information
Authors and Affiliations
Contributions
All authors read, critically reviewed and approved the final manuscript. SC conducted the database searches, screened titles, abstracts and full-texts for eligibility, performed data extraction, data-analysis and wrote the manuscript. DVD reviewed full texts for eligibility criteria, and performed data extraction. ADS assisted in the data-analyses. LP assessed the study quality.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
NA.
Consent for publication
NA.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
PRISMA checklist. (DOC 63 kb)
Additional file 2:
Protocol of the meta-analysis. (DOCX 45 kb)
Additional file 3:
Difference in means for total sedentary time between the intervention group and the control group. (DOCX 117 kb)
Additional file 4:
Publication bias. (DOCX 111 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Compernolle, S., DeSmet, A., Poppe, L. et al. Effectiveness of interventions using self-monitoring to reduce sedentary behavior in adults: a systematic review and meta-analysis. Int J Behav Nutr Phys Act 16, 63 (2019). https://doi.org/10.1186/s12966-019-0824-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-019-0824-3