
Abstract
Objective
Physical activity (PA) has a profound impact on health and development in children. Parental behaviors (i.e., modeling and support) represent an obvious important factor in child PA. The purpose of this paper was to provide a comprehensive meta-analysis that overcomes the limitations of prior narrative reviews and quantitative reviews with small samples.
Methods
Ten major databases were used in the literature search. One-hundred and fifteen studies passed the eligibility criteria. Both fixed and random effects models with correction for sampling and measurement error were examined in the analysis. Moderator analyses investigating the effects of child’s developmental age, study design, parental gender, measurement of child PA, and quality rating were performed.
Results
Based on the random effects model, the results showed that parental modeling was weakly associated with child PA (summary r = .16, 95% CI .09-.24) and none of the proposed moderators were significant. Separate analyses examining the moderating effects of parental gender and boys’ PA found that that father-son PA modeling (r = .29, 95% CI .21-.36) was significantly higher compared to mother-son PA (r = .19, 95% CI .14-.23; p < .05). However, parental gender did not moderate the relationship between parental modeling and girls’ PA (p > .05). The random effects model indicated an overall moderate effect size for the parental support and child PA relationship (summary r = .38, 95% CI .30-.46). Here, the only significant moderating variable was the measurement of child PA (objective: r = .20, 95% CI .13-.26; reported: r = .46, 95% CI .37-.55; p < .01).
Conclusions
Parental support and modeling relate to child PA, yet our results revealed a significant degree of heterogeneity among the studies that could not be explained well by our proposed moderators.
Similar content being viewed by others

It has been widely acknowledged by health researchers that participation in regular physical activity (PA) is linked to various health benefits and prevention of chronic disease. In spite of the overwhelming evidence that supports an association between PA and health, much of the populace does not commensurate with the national recommendations. Particularly, many children in North America are insufficiently active to reap the health benefits associated with regular PA. A recent Canadian national survey estimated that 9% of boys and 4% of girls between the ages of six to nineteen met the current recommendations [1]. Likewise, data from the United States showed that more than half of the children surveyed were insufficiently active [2]. At this juncture, intervention efforts to improve child PA levels have produced very modest results [3]. Thus moving forward, it will be crucial to properly identify the key correlates in child and adolescent PA to further the planning and development of PA interventions [4].
Presently, a total of 14 review papers [5-18] and three reviews of reviews [19-21] have been published in this area. From these reviews, parental modeling of PA and parental support of child PA have emerged as major themes. However, many of these reviews have discordant findings. For instance, 12 review papers examining the relationship between parent and child PA have shown variable results [5-9,12-14,16,19-21]. Three of the 12 reviews do not support a link between parent PA and child PA [14,20,21], while eight reviews have suggested the association as inconclusive [5-7,9,12,13,17,19]. Unlike the findings for parental modeling and child PA, parental support has emerged as a consistent correlate of child and adolescent PA in a number of narrative reviews [6-9,11,12,14,16,18-21]. The more striking absence in this theme is the limited quantitative synthesis in order to provide a point-estimate of the parental support-PA relationship. Only one meta-analysis has examined parental support (r = .23), but it is several years old and was restricted to three studies [8].
Another pertinent issue that surrounds parental support as a correlate of child PA has been how support has been defined and measured. Parental support has often been measured as an omnibus of various support behaviours and has no consistent set of behaviours [22]. In some cases, researchers have grouped and measured multiple support behaviours as tangible (e.g., providing transportation, financial support) and intangible forms of support (e.g., praise and encouragement). Through these forms of measurement, it is unclear to which specific individual support behaviours may be important in child PA. A more comprehensive synthesis of these support factors is needed.
Finally, prior reviews on this topic have been restricted to very specific age-ranges, which reduces our understanding to whether modeling and support vary across the developmental spectrum. No prior meta-analyses have explored the parental correlates according to developmental stages (i.e., preschool, childhood, and adolescence). A meta-analysis is necessary to consolidate and clarify the overall information.
With these limitations in mind, the aim of this meta-analysis was to provide a cohesive and comprehensive examination of the parental correlates, and potential moderators, of child PA. Here, the five postulated moderators included the child’s developmental age, method in which child PA is measured (objective or reported), geographical location of the sample population, study design, and quality of the study. Moreover, we investigated the possibility of intergenerational gender interactions between parent and child behaviours. It was hypothesized that overall parental PA would have a negligible to small correlation with child and adolescent PA, explaining the prior inconsistencies among the narrative reviews; whereas overall parental support will have a small to medium correlation. Among the individual support behaviours, it was postulated that a small effect size will be found for the various support behaviours and child PA. Our analysis of intergenerational gender interactions between parental and child was considered exploratory.
Methods
Eligibility criteria
To ensure transparency and complete reporting, the protocols for this study were in accordance to the recommendations put forth by the PRISMA statement for conducting systematic reviews and meta-analyses [23]. Studies were included if: 1) children were between 2.5 and 18.0 years; 2) an assessment of parental/family support, individual parental support behaviour(s), or parental PA as the independent variable; 3) a measurement of children’s PA as the dependent variable; and 4) an effect size illustrating the relationship between independent and dependent variables or the availability of statistics to calculate an effect size (e.g., means and standard deviation). Studies were excluded from the review if: 1) social support measures consolidated parental sources with teachers, peers, or friends; 2) the study was qualitative; and 3) not published in English.
PA was defined as “any bodily movement produced by skeletal muscles that results in energy expenditure” [24]. This definition encompassed both structured (e.g., organized sports, lessons) and unstructured PA (e.g.. leisure-time PA, play). Encouragement to be active, parent–child co-activity, praising the child’s activity, watching the child be active, informing the child that they are performing well, telling the child that PA is beneficial, and providing transportation to PA venues were classified as parental support behaviours. Other behaviours such as supplying the child with PA equipment and financial support, and enrolling the child in PA programs were classified as individual parent support behaviours.
Search strategy
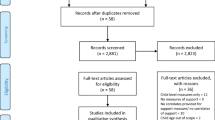
Publications from January 1970 to November 2014 were systematically reviewed for this paper (Figure 1). Ten databases were used to locate relevant articles: EBSCO (Academic Search Complete, Academic Search Premier, CINAHL, Health Source, MEDLINE, PsycINFO, Social Sciences, SPORTDiscus), PubMed, and ISI Web of Science. The following key terms were used: physical activity, exercise, sport, adolescent, youth, children, preschool, parental support, parental physical activity, role modeling, parental influence, and parental correlates. One author conducted the search and manually cross-referenced studies to ensure saturation of the literature. The eligibility criteria and search strategy followed a protocol used in previously published meta-analyses and reviews [25,26]. The reference sections of reviews and individual studies were carefully inspected to locate any additional publications.

PRISMA flow-chart.
Screening
Using the inclusion criteria previously established by both reviewers, one reviewer initially screened citations based on the title and abstract. Potentially relevant abstracts were selected and the full article was located if it was deemed suitable for the study. A full consensus by the two reviewers was required in order for the studies to be included in the analysis.
Data abstraction
Information regarding authors, publication year, country, sample (number of participants, age, gender), study design (cross-sectional/prospective), measurement tools (i.e., PA and social support measures), reliability of the measures, parental gender, and reported effect sizes, were abstracted onto a Word document. Once the coded data was entered, the file was imported into the Comprehensive Meta-Analysis version 2 program for further analyses [27].
Analyses
Based on the hypothesized moderators, the studies included in the analysis were categorized and coded by developmental age (preschool 2–5.4 yrs, childhood 5.5-12.4 yrs, adolescence 12.5-18 yrs), geographical location (Australia & New Zealand, Asia, Canada, Europe, USA), study design (cross-sectional, prospective), type of PA measure used to determine child PA (objective: accelerometer, pedometer, heart rate monitor; reported), and quality (high, moderate, low). Upon further investigation of previous meta-analyses and reviews, some of the studies included did not appropriately categorize effect sizes that represented the overall effect sizes for parental-child PA variables. For instance, samples only examining girls’ or boys’ PA were previously amalgamated into overall child associations rather than conducted in separate analyses. In our analyses, the correlates for boys, girls, and mixed samples were abstracted, categorized, and analyzed separately.
In the case that more than one type of PA measure was reported (ex. overall PA levels versus moderate to vigorous PA), the variable that best reflected the national recommendations for PA (i.e., moderate to vigorous PA) was incorporated into the analysis. Studies that incorporated a family support measure were included in the analysis.
To assess the potential risk of bias and methodological quality, each study was critically appraised using an adapted version of Downs and Black’s [28] 22-item assessment tool. This modified tool is comparable to the Cochrane Collaboration’s instrument for assessing risk of bias and has been used in several published reviews [25,26,29]. For the purposes of this study, items from the original checklist pertaining to experimental studies and items that were not applicable to this study were excluded. The adapted version utilized a 14-point scoring scheme, where each item was scored one point based on a yes (1) or no (0) response. Studies scoring 12–14 points were deemed high-quality studies, 8–11 points were regarded as moderate-quality studies, and lower quality studies were below 7 points. Studies that scored 4 points or less were excluded.
Effect sizes included in the analysis were further corrected for sample size and attenuated for potential measurement error. Correction of measurement error procedures was based on the reported reliabilities of the measures found in the study. In the case that the reliability of the measure was not detailed, an rxy = .70 was used. Based on previous publications, this reliability has been identified as a conservative, yet acceptable estimate for reliability [30]. For accelerometer measures that have obtained 4–9 days of data, the recommended reliability estimate of .80 was used [31]. No subsequent correction procedures were conducted for effect sizes derived from structural equation models or hierarchical linear models as these forms of analyses account for measurement error.
Both fixed and random effects models were used to determine the overall effect sizes for both uncorrected and corrected effect sizes. However, only corrected effect sizes from the random effects model will be discussed. The strength of the correlation was categorized based on Cohen’s recommendations [32]. According to these guidelines, a correlation of .09 or less was considered as a null effect, .10 a small effect, .30 a medium effect, and .50 a large effect. In addition to the overall effect sizes, 95% confidence intervals were calculated. To determine heterogeneity among the effect sizes, a Q-statistic and I2 was computed. The Q-statistic identifies whether the observed variance in effect sizes is no greater than that expected by sampling error alone, whereas the I2 denotes the dispersion. For the purposes of this study, I2 values of 25 were categorized as having a low dispersal, 50 as a moderate dispersal, and 75 as a high dispersal. Moderator analyses investigating the effects of child’s developmental age, study design, parental gender, measurement of child PA, and quality rating were performed using the corrected r’s with fixed and random effects models. A minimum of 4 studies was required in each moderator analysis to deem it as a valid moderator. To identify the correlations between the intergenerational relationships between parent and child, separate analyses were used to examine whether the parents’ gender moderated boys’ and girls’ PA. To assess the extent of publication bias in our samples, Rosenthal’s classic fail-safe N [33] and Duval and Tweedie’s Trim and Fill procedures [34,35] were conducted. All data was analyzed in February 2013 using Comprehensive Meta-Analysis.
Results
A total of 2,293 potentially relevant citations were identified in the initial search. The screening procedures resulted in a total of 112 studies, with 11 studies extracted from the reference listing of the included articles (see Figure 1). Table 1 describes the characteristics of the 115 independent samples included for the investigation. Details of the included studies are presented in Tables 2,3,4,5,6 and 7. Duplicated studies were not included in the analysis.
Parental modeling as a correlate
Overall effect size
A total of 36 effect sizes were used in the analysis to determine the overall relationship between parent and child PA (Table 8). Based on the fixed effects model and correcting for measurement error, parent and child PA associations approached a medium effect size (r = .29, 95% CI .28-.30). However, the results showed that the effect sizes in the sample were significantly heterogeneous Q (36) = 1597.52, p < .001. Due to the high degree of heterogeneity, using the point estimate from random effects model was appropriate, which resulted in a small effect size (r = .16, 95% CI .09-.24). Moreover, 98% of the observed variance was explained by true systematic effect size differences between studies.
Moderators of child physical activity
Table 8 indicates that subsequent analyses did not find any of the proposed moderators of parent and child physical activity to be significant (p > .05).
Based on 49 effect sizes, our analyses found that parental gender moderated the relationship between boys’ PA and parents’ PA (Table 9). The results showed that father-son PA (r = .29, 95% CI .21-.36) was significantly higher than mother-son PA (r = .19, 95% CI .14-.23; p < .05). For parental modeling and girls’ PA, results from the 62 effect sizes showed that parental gender did not moderate the relationship. The correlation for father-daughter PA (r = .22, 95% CI 16-.27) and mother-daughter PA (r = .23, 95% CI .18-.27) were both similar in magnitude.
Parental support as a correlate
Overall effect size
A total of 34 effect sizes were used to estimate the relationship between overall parental support and child PA (Table 10). Both the fixed and random effects model found that the relationship between parental support and child PA was moderate in size (r = .38). Analyses from the fixed model also indicated that a significant degree of heterogeneity within the sample was present (Q (34) = 1204.70, p < .001) and that 97% of the observed variance was explained by true systematic effect size differences between studies.
According to the corrected random effects models, many of the effect sizes for the various individual support behaviours were small. Parent–child co-activity, praising the child for being active, watching the child participate in PA, providing transportation to a place where the child could be active, monitoring the child’s PA levels, and supplying the child with PA equipment ranged between r = .15-.28 (Table 10). The only support behaviour to have a moderate effect size was the relationship between parental encouragement and child PA (r = .34, 95% CI .25-.41). Overall, the dispersal of the effect sizes calculated was variable, ranging from 66 to 100%.
Moderators of child physical activity
Table 10 presented the potential moderators that were investigated in our analysis. In the analysis, child and adolescent PA was moderated by the type of measurement used to quantify the child’s PA (p < .001). When objective PA measures were used, the results showed a small effect of r = .20 (95% CI .13-.26) between a composite measure of parental support and child PA; whereas reported PA had a moderate effect size of r = .46 (95% CI .37-.55). Developmental age, study design, and geographical location were not significant moderators of overall parental support and child PA. Due to the limited number of prospective studies, moderator analyses were not conducted to examine the effects of study design.
Among individual supportive behaviours, only parental encouragement had an adequate amount of studies to examine potential moderating variables (Table 10). Moderating variables such as developmental age and geographical location were not significant moderators of the parental encouragement and child PA relationship (p > .05).
When examining the relationship between girls’ PA and parental support, the summary analysis of 10 effect sizes found that the parental gender did not significantly moderate this relationship (p > .05) (Table 9). Analyses exploring the moderating effects of parental gender in boys’ PA were limited by the number of studies and were not conducted.
Publication bias
Funnel plots were constructed to investigate the possibility of publication bias for parent and child PA, parental support and child PA, and individual support behaviours and child PA associations. When visually inspected, the resulting funnel plots suggested a potential publication bias for parent and child PA, and providing transportation for the child to be active and child PA associations.
A subsequent classic fail-safe N analysis for child–parent PA associations showed that 7590 studies with a mean effect of zero were necessary for the overall effect found to become statistically insignificant. Based on this relatively large computation, it indicated that the results were not skewed. However, for providing the child with transportation to opportunities to be active, only 198 studies needed to create a mean effect of zero for the effect to be insignificant, alluding to a skewed effect size. Subsequent trim and fill analyses specified that it was necessary to trim two studies from the computation. With the correction, the effect size for transporting the child to physical activities and child PA decreased from the original point estimate of r = .22 (95% CI .12-.31) to a corrected point estimate of r = .14 (95% CI .03-.24).
Discussion
The main objectives of this meta-analysis were to thoroughly investigate and quantify the strength of parental correlates and identify whether parent–child gender interactions are notable in child and adolescent PA. Previous systematic reviews have been narrative in nature and meta-analyses attempting to quantify the overall effects between parental support and modeling behaviours and child PA have been restricted to 20–30 studies [8,16] – resulting in a partial depiction of the parental correlates in child and adolescent PA. This meta-analysis encompasses 112 studies published to date and thus sheds a more definitive light on the relationship between parental behaviours and children’s PA.
One of the contentious topics has been whether parental modeling is an important correlate in child and adolescent PA. Recent narrative reviews have suggested that parent’s PA behaviours were unassociated with child and adolescent PA [14,20]. The meta-analysis conducted by Pugliese and Tinsley [8] found a small effect (r = .10) for parent and child PA. Our results, after correcting for measurement error, concurred with the previous meta-analysis showing a small overall association between parental and child PA.
During preadolescent years, parental modeling of PA plays an integral role in establishing a social norm regarding activity [7], but as the child matures, modeling behaviours in the PA domain may be drawn from the emergent influence of the child’s peers while the influence of parental modeling wanes. It is also possible that in early years of childhood parent–child coactivity is more prevalent; and as the child ages, the association between parent and child PA bifurcates and becomes more independent from each other. In any case, the results suggest the importance of family-based coactivity interventions in the early years of child development.
A number of narrative reviews have consistently identified an association between parental support and children’s PA [6-9,11,12,14,16,18-21]. This meta-analysis is the first to quantify the relationship between overall parental support and child PA as well as various individual supportive behaviours. In our analyses, overall parental support and child PA yielded a medium effect size. This effect is worthy of noting, particularly when compared to other correlates of child behaviour. For example, a recent meta-analysis examining children’s affective judgments in PA, found that affect had a small to medium an effect size (r = .26) between children’s affect and PA behaviour [25]. Based on these findings, it suggests that parental support for child and adolescent PA may be an important consideration for future PA intervention efforts.
In line with this thinking, it is important to examine whether any particular support behaviour is of critical value over others as a potential intervention target. Our analyses of specific behaviours such as praising the child, watching the child participate in PA, engaging in parent–child co-activity, transporting the child to places where the child could be active, and providing the child with equipment all had small effect sizes (r = .14-.28). The only individual support behaviour that was moderate in size was parental encouragement. To date, much quantitative reviews have only investigated the individual support behaviour of parental encouragement on child PA, which has been identified as a small correlation of r = .15-.18 [8,16], which is smaller than our results. However, it is important to mention that these correlations were not previously corrected for measurement error. Overall, based on these various small effect sizes, it may be important to consider the potency of parental support taken as an aggregate rather than any individual support behaviour.
To date, various studies have examined the moderating effect of parental gender in boys’ and girls’ PA, yet the finding has been unclear and speculative. In a systematic review, a positive association was found for father-son PA [7]. Similarly, among maternal relationships, mother-daughter PA was significantly related [7]. Our results brought forth a degree of transparency regarding parent–child gender interactions further supporting a stronger correlation for father-son PA. However, in our results no differences were found for mother-son and mother-daughter PA correlations. In the area of parental support, no differences were found for the maternal and paternal interaction for girls’ PA. However, the parental interaction regarding boys’ PA will require further investigation. Overall, these results suggested that the importance between the intergenerational relationship between father and son PA and may be an important consideration when targeting boys’ activity behaviour. As well, our findings indicated that the incorporation of parental support behaviours, irrespective of parental gender, were an essential component for prospective interventions that target girls’ PA.
The limitations of this review highlight the fact that additional research is needed in several areas to improve our understanding of the correlates in child and adolescent PA. First, the use of parental support instruments and reporting of the correlation between parental support and child PA in this meta-analysis have been quite diverse, which also has been documented in the previously published literature [18,22]. Moving forward, it may be important to utilize previously validated measures, such as the activity support scale [37], and report both individual support behaviours and parental support as a construct (see [22] for an overview of parental support measures). Second, an important consideration may be children’s peers and siblings and how they relate the child’s behaviour. Thus, future research will be needed to explore the role of socialization of the immediate social network outside of the family unit and whether other children provide more salient models or social support for PA. Third, much of the research has been limited to developed nations such as the United States, Australia, or Europe. More studies will be needed from other countries to explore whether cultural differences are present. Fourth, an important detail to underscore from this review was that many of the parental respondents were mothers. It may be important to investigate the roles of fathers in the area of parental support and child PA. Lastly, several individual support behaviours were unexamined due to the limited amount of research (e.g., informing the child that PA is beneficial or financial support). More research is needed to uncover the relationship these support behaviours and child PA and whether certain parental support behaviours are conducive to a specific type of PA (e.g., structured or unstructured PA).
In summary, this meta-analysis presents results that align with previous reviews but represent a larger and more robust assessment of the parental and child correlates literature and the consideration for measurement error and methodologic quality. The findings demonstrate that both parental modeling and support related to child and adolescent PA. However, overall parental support emerged as a sizeable correlate linked to child activity. In addition to this, our results revealed a significant degree of heterogeneity among the studies that could not be explained well by our proposed moderators. In order to advance our intervention approaches to increase PA in children and adolescents, it will be critical to consider the development of interventions based on the child’s developmental age. More notably, it will be essential to integrate parents as a source of social support to change child and adolescent PA behaviour.
Abbreviations
- PA:
-
Physical activity
References
Colley RC, Garriguet D, Janssen I, Craig CL, Clarke J, Tremblay MS. Physical activity of Canadian children and youth: accelerometer results from the 2007 to 2009 Canadian health measures survey. Health Rep. 2011;22:15–23.
Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40:181–8.
O’Connor TM, Jago R, Baranowski T. Engaging parents to increase youth physical activity: a systematic review. Am J Prev Med. 2009;37:141–9.
Baranowski T, Anderson C, Carmack C. Mediating variable framework in physical activity interventions. Am J Prev Med. 1998;15:266–97.
Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000;32:963–75.
Biddle SJH, Whitehead SH, O’Donovan TM, Nevill ME. Correlates of participation in physical activity for adolescent girls: a systematic review of recent literature. J Phys Act Heal. 2005;2:423–34.
Gustafson SL, Rhodes RE. Parental correlates of physical activity in children and early adolescents. Sports Med. 2006;36:79–97.
Pugliese J, Tinsley B. Parental socialization of child and adolescent physical activity: a meta-analysis. J Fam Psychol. 2007;21:331–43.
Van Der Horst K, Paw MJC, Twisk JWR, Van Mechelen W. A brief review on correlates of physical activity and sedentariness in youth. Med Sci Sports Exerc. 2007;39:1241–50.
Van Sluijs EMF, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. 2007;335:703.
Beets MW, Cardinal BJ, Alderman BL. Parental social support and the physical activity-related behaviors of youth: a review. Heal Educ Behav. 2010;37:621–44.
Edwardson CL, Gorely T. Parental influences on different types and intensities of physical activity in youth: a systematic review. Psychol Sport Exerc. 2010;11:522–35.
Craggs C, Corder K, van Sluijs EMF, Griffin SJ. Determinants of change in physical activity in children and adolescents: a systematic review. Am J Prev Med. 2011;40:645–58.
Trost S, Loprinzi PD. Parental influences on physical activity behavior in children and adolescents: a brief review. Am J Lifestyle Med. 2011;5:171–81.
Van Sluijs EMF, Kriemler S, McMinn AM. The effect of community and family interventions on young people’s physical activity levels: a review of reviews and updated systematic review. Br J Sports Med. 2011;45:914–22.
Mitchell J, Skouteris H, Mccabe M, Ricciardelli LA, Milgrom J, Baur LA, et al. Physical activity in young children: a systematic review of parental influences. Early Child Dev Care. 2012;182:1411–37.
Webber KJ, Loescher LJ. A systematic review of parent role modeling of healthy eating and physical activity for their young African-American children. J Spec Pediatr Nurs. 2013;18:173–88.
Mendonça G, Cheng LA, Mélo EN, de Farias Júnior JC. Physical activity and social support in adolescents: a systematic review. Health Educ Res. 2014;29:822–39.
Biddle SJH, Atkin AJ, Cavill N, Foster C. Correlates of physical activity in youth: a review of quantitative systematic reviews. Int Rev Sport Exerc Psychol. 2011;4:25–49.
Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJF, Martin BW. Correlates of physical activity: Why are some people physically active and others not? Lancet. 2012;380:258–71.
Sterdt E, Liersch S, Walter U. Correlates of physical activity of children and adolescents: a systematic review of reviews. Health Educ J. 2013;73:72–89.
Sleddens EFC, Kremers SPJ, Hughes SO, Cross MB, Thijs C, De Vries NK, et al. Physical activity parenting: a systematic review of questionnaires and their associations with child activity levels. Obes Rev. 2012;13:1015–33.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62:1006–12.
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100:126–31.
Nasuti G, Rhodes RE. Affective judgment and physical activity in youth: review and meta-analyses. Ann Behav Med. 2013;45:357–76.
Rhodes RE, Fiala B, Conner M. A review and meta-analysis of affective judgments and physical activity in adult populations. Ann Behav Med. 2009;38:180–204.
Borenstein M, Hedges L, Higgins J, Rothstein H. Comprehensive meta-analysis. 2nd ed. Englewood, NJ: Biostat; 2005.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–84.
Kirk M, Rhodes RE. Occupation correlates of adults’ participation in leisure-time physical activity: a systematic review. Am J Prev Med. 2011;40:476–85.
Cohen J, Cohen P, West SG, Aiken L: Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences. Volume Third Edit. Erlbaum: NY; 2003:703 S.
Trost SG, McIver KL, Pate RR. Conducting accelerometer-based activity assessments in field-based research. Med Sci Sport Exerc. 2005;37:S531–43.
Cohen J. A power primer. Psychol Bull. 1992;1:155–9.
Rosenthal R: The file drawer problem and tolerance for null results. Psychol Bull 1979; 86:638–641.
Duval S, Tweedie R. A nonparametric “Trim and Fill” method of accounting for publication bias in meta-analysis. J Am Stat Soc. 2000;95:89–98.
Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56:455–63.
Alderman B, Benham-Deal TB, Jenkins JM. Change in parental influence on children’s physical activity over time. J Phys Act Health. 2010;7:60.
Ammouri AA, Kaur H, Neuberger GB, Gajewski B, Choi WS. Correlates of exercise participation in adolescents. Public Health Nurs. 2007;24:111–20.
Berge JM, Meyer C, MacLehose RF, Eisenberg ME, Neumark-Sztainer D. Nonresident parental influence on adolescent weight and weight-related behaviors: similar or different from resident parental influence? Int J Behav Nutr Phys Act. 2014;11:131.
Dempsey JM, Kimiecik JC, Horn TS. Parental influence on children’s moderate to vigorous physical activity participation: an expectancy-value approach. Pediatr Exerc Sci. 1993;5:151–67.
Dowda M, Pfeiffer KA, Brown WH, Mitchell JA, Byun W, Pate RR. Parental and environmental correlates of physical activity of children attending preschool. Arch Pediatr Adolesc Med. 2011;165:939–44.
Dzewaltowski D, Ryan GJ, Rosenkranz RR. Parental bonding may moderate the relationship between parent physical activity and youth physical activity after school. Psychol Sport Exerc. 2008;9:848–54.
Fredricks JA, Eccles JS. Family socialization, gender, and sport motivation and involvement. Sport Psychol. 2005;27:3–31.
Heitzler CD, Lytle LA, Erickson DJ, Barr-Anderson D, Sirard JR, Story M. Evaluating a model of youth physical activity. Am J Health Behav. 2010;35:593–607.
Hendrie G, Coveney J, Cox DN. Factor analysis shows association between family activity environment and children’s health behaviour. Aust N Z J Public Health. 2011;35:524–9.
Hennessy E, Hughes SO, Goldberg JP, Hyatt RR, Economos CD. Parent–child interactions and objectively measured child physical activity: a cross-sectional study. Int J Behav Nutr Phys Act. 2010;7:71.
Keresztes N, Piko BF, Pluhar ZF, Page RM. Social influences in sports activity among adolescents. J R Soc Promot Health. 2008;128:21–5.
Labree W, Lötters F, van de Mheen D, Rutten F, Rivera Chavarría A, Neve M, et al. Physical activity differences between children from migrant and native origin. BMC Public Health. 2014;14:819.
Lei WG, Phillips A, Reed JA. An investigation of the relationships between environmental factors and physical activity among Taiwanese high school students. Environ Factors Phys Act. 2004;40:43–9.
Loprinzi PD, Trost SG. Parental influences on physical activity behavior in preschool children. Prev Med. 2010;50:129–33.
Loprinzi PD, Schary DP, Beets MW, Leary J, Cardinal BJ. Association between hypothesized parental influences and preschool children’s physical activity behavior. Am J Heal Educ. 2013;44:9–18.
McMurray RG, Bradley CB, Harrell JS, Bernthal PR, Frauman AC, Bangdiwala SI. Parental influences on childhood fitness and activity patterns. Res Q Exerc Sport. 1993;64:249–55.
Moore LL, Lombardi DA, White MJ, Campbell JL, Oliveria SA, Ellison RC. Influence of parents’ physical activity levels on activity levels of young children. J Pediatr. 1991;118:215–9.
Mota J. Parents’ physical activity behaviors and children's physical activity. J Hum Mov Stud. 1998;35:89–100.
Østbye T, Malhotra R, Stroo M, Lovelady C, Brouwer R, Zucker N, et al. The effect of the home environment on physical activity and dietary intake in preschool children. Int J Obes. 2013;37:1314–21.
Patnode CD, Lytle L, Erickson DJ, Sirard JR, Barr-Anderson D, Story M. The relative influence of demographic, individual, social, and environmental factors on physical activity among boys and girls. Int J Behav Nutr Phys Act. 2010;7:79.
Perusse L, Tremblay A, Leblanc C, Bouchard C. Genetic and environmental influences on level of habitual physical activity and exercise participation. Am J Epidemiol. 1989;129:1012–22.
Pfeiffer KA, Dowda M, McIver KL, Pate RR. Factors related to objectively measured physical activity in preschool children. Pediatr Exerc Sci. 2009;21:196–208.
Poest C, Williams JR, Witt DD, Atwood ME. Physical activity patterns of preschool children. Early Child Res Q. 1989;4:367–76.
Polley DC, Spicer MT, Knight AP, Hartley BL. Intrafamilial correlates of overweight and obesity in African-American and Native-American grandparents, parents, and children in rural Oklahoma. J Am Diet Assoc. 2005;105:262–5.
Ruiz R, Gesell SB, Buchowski MS, Lambert W, Barkin SL. The relationship between Hispanic parents and their preschool-aged children’s physical activity. Pediatrics. 2011;127:888–95.
Rutkowski EM, Connelly CD. Self-efficacy and physical activity in adolescent and parent dyads. J Spec Pediatr Nurs. 2012;17:51–60.
Sallis JF, Patterson TL, Buono MJ, Atkins CJ, Nader PR. Aggregation of physical activity habits in Mexican-American and Anglo families. J Behav Med. 1988;11:31–41.
Singh GK, Kogan MD, Siahpush M, van Dyck PC. Prevalence and correlates of state and regional disparities in vigorous physical activity levels among US children and adolescents. J Phys Act Health. 2009;6:73–87.
Trost SG, Sallis JF, Pate RR, Freedson PS, Taylor WC, Dowda M. Evaluating a model of parental influence on youth physical activity. Am J Prev Med. 2003;25:277–82.
Vella S, Cliff DP, Okely AD. Socio-ecological predictors of participation and dropout in organised sports during childhood. Int J Behav Nutr Phys Act. 2014;11:62.
Welk GJ, Wood K, Morss G. Parental influences on physical activity in children: an exploration of potential mechanisms. Pediatr Exerc Sci. 2003;15:19–33.
Williams SL, Mummery WK. Links between adolescent physical activity, body mass index, and adolescent and parent characteristics. Heal Educ Behav. 2011;38:510–20.
Zecevic CA, Tremblay L, Lovsin T, Michel L: Parental influence on young children’s physical activity. Int J Pediatr 2010:1-9.
Zhao J, Settles BH. Environmental correlates of children’s physical activity and obesity. Am J Health Behav. 2014;38:124–34.
Ziviani J, Macdonald D, Jenkins D, Rodger S, Batch J, Cerin E. Physical activity of young children. Occup Particip Heal. 2005;26:4–15.
Ziviani J, Macdonald D, Ward H, Jenkins D, Rodger S. Physical activity of young children: a two-year follow-up. Phys Occup Ther Pediatr. 2008;28:25–39.
Barr-Anderson DJ, O’Brien-Robinson R, Haines J, Hannan P, Neumark-Sztainer D. Parental report vs. child perception of familial support: Which is more associated with child physical activity and television use? J Phys Act Health. 2010;7:364–8.
Davison KK, Nishi A, Kranz S, Wyckoff L, May JJ, Earle-Richardson GB, et al. Associations among social capital, parenting for active lifestyles, and youth physical activity in rural families living in upstate New York. Soc Sci Med. 2012;75:1488–96.
Hagger M, Chatzisarantis NLD, Hein V, Soós I, Karsai I, Lintunen T, et al. Teacher, peer and parent autonomy support in physical education and leisure-time physical activity: a trans-contextual model of motivation in four nations. Psychol Health. 2009;24:689–711.
Hamilton K, White KM. Extending the theory of planned behavior: the role of self and social influences in predicting adolescent regular moderate-to-vigorous physical activity. J Sport Exerc Psychol. 2008;30:56–74.
Heitzler CD, Martin SL, Duke J, Huhman M. Correlates of physical activity in a national sample of children aged 9–13 years. Prev Med. 2006;42:254–60.
Kim YH, Cardinal BJ. Psychosocial correlates of Korean adolescents’ physical activity behavior. J Exerc Sci Fit. 2010;8:97–104.
Langer SL, Crain L, Senso MM, Levy RL, Sherwood NE. Predicting child physical activity and screen time: parental support for physical activity and general parenting styles. J Pediatr Psychol. 2014;39:633–42.
Lawman HG, Wilson DK. Associations of social and environmental supports with sedentary behavior, light and moderate-to-vigorous physical activity in obese underserved adolescents. Int J Behav Nutr Phys Act. 2014;11:92.
Ommundsen Y, Klasson-Heggebø L, Anderssen SA. Psycho-social and envrionmental correlates of location-specific physical activity among 9- and 15- year-old Norwegian boys and girls: the European youth heart study. Int J Behav Nutr Phys Act. 2006;3:32.
Prochaska JJ, Rodgers MW, Sallis JF. Association of parent and peer support with adolescent physical activity. Res Q Exerc Sport. 2002;73:206–10.
Schaben JA, Welk GJ, Joens-Matre R, Hensley L. The predictive utility of the children’s physical activity correlates (CPAC) scale across multiple grade levels. J Phys Act Health. 2006;3:59–69.
Schary DP, Cardinal BJ, Loprinzi PD. Early child development and care parental support exceeds parenting style for promoting active play in preschool children. Early Child Dev Care. 2012;182:1057–69.
Taylor WC, Sallis JF, Dowda M, Freedson PS, Eason K, Pate RR. Activity patterns and correlates among youth: differences by weight status. Pediatr Exerc Sci. 2002;14:418–31.
Verloigne M, Veitch J, Carver A, Salmon J, Cardon G, De Bourdeaudhuij I, et al. Exploring associations between parental and peer variables, personal variables and physical activity among adolescents: a mediation analysis. BMC Public Health. 2014;14:966.
Zhang T, Solmon MA, Gao Z, Kosma M. Promoting school students’ physical activity: a social ecological perspective. J Appl Sport Psychol. 2012;24:92–105.
Aarnio M, Winter T, Kujala UM, Kaprio J. Familial aggregation of leisure-time physical activity: a three generation study. Int J Sports Med. 1997;18:549–56.
Anderssen N, Wold B. Parental and peer influences on leisure-time physical activity in young adolescents. Res Q Exerc Sport. 1992;63:341–8.
Anderssen N, Wold B, Torsheim T. Are parental health habits transmitted to their children? An eight year longitudinal study of physical activity in adolescents and their parents. J Adolesc. 2006;29:513–24.
Bastos JP, Araujo CLP, Hallal PC. Prevalence of insufficient physical activity and associated factors in Brazilian adolescents. J Phys Act Health. 2008;5:777–94.
Bogaert N, Steinbeck KS, Baur LA, Brock K, Bermingham MA. Food, activity and family- environmental vs biochemical predictors of weight gain in children. Eur J Clin Nutr. 2003;57:1242–9.
Campbell PT, Katzmarzyk PT, Malina RM, Rao DC, Pérusse L, Bouchard C. Prediction of physical activity and physical work capacity (PWC150) in young adulthood from childhood and adolescence with consideration of parental measures. Am J Hum Biol. 2001;13:190–6.
Davison KK, Birch LL. Child and parent characteristics as predictors of change in girls’ body mass index. Int J Obes. 2001;25:1834–42.
Davison KK, Cutting TM, Birch LL. Parents’ activity-related parenting practices predict girls' physical activity. Med Sci Sport Exerc. 2003;35:1589–95.
Deflandre A, Lorant J, Gavarry O, Falgairette G. Determinants of physical activity and physical and sports activities in French school children. Percept Mot Ski. 2001;92:399–414.
Deflandre A, Lorant J, Gavarry O, Falgairette G. Physical activity and sport involvement in French high school students. Percept Mot Ski. 2001;92:107–20.
Eriksson M, Nordqvist T, Rasmussen F. Associations between parents’ and 12-year-old children’s sport and vigorous activity: the role of self-esteem and athletic competence. J Phys Act Health. 2008;5:359–73.
Fogelholm M, Nuutinen O, Pasanen M, Myöhänen E, Säätelä T. Parent–child relationship of physical activity patterns and obesity. Int J Obes. 1999;23:1262–8.
Fuemmeler BF, Anderson CB, Mâsse LC. Parent–child relationship of directly measured physical activity. Int J Behav Nutr Phys Act. 2011;8:17.
Hinkley T, Salmon J, Okely AD, Hesketh K, Crawford D. Correlates of preschool children’s physical activity. Am J Prev Med. 2012;43:159–67.
Jacobi D, Caille A, Borys J-M, Lommez A, Couet C, Charles M-A, et al. Parent-offspring correlations in pedometer-assessed physical activity. PLoS One. 2011;6:e29195.
Jago R, Sebire SJ, Wood L, Pool L, Zahra J, Thompson JL, et al. Associations between objectively assessed child and parental physical activity: a cross-sectional study of families with 5–6 year old children. BMC Public Health. 2014;14:655.
Kahn JA, Huang B, Gillman MW, Field AE, Austin SB, Colditz GA, et al. Patterns and determinants of physical activity in U.S. adolescents. J Adolesc Heal. 2008;42:369–77.
Madsen KA, McCulloch CE, Crawford P. Parent modeling: perceptions of parents’ physical activity predict girls' activity throughout adolescence. J Pediatr. 2009;154:278–83.
Martin-Matillas M, Ortega FB, Chillon P, Perez IJ, Ruiz JR, Castillo R, et al. Physical activity among Spanish adolescents: relationship with their relatives’ physical activity - The AVENA Study. J Sports Sci. 2011;29:329–36.
Nichols-English GJ, Lemmon CR, Litaker MS, Cartee SG, Yin Z, Gutin B, et al. Relations of Black mothers’ and daughters' body fatness, physical activity and behavior. Ethn Dis. 2006;16:172–9.
O’Loughlin J, Paradis G, Kishchuk N, Barnett T, Renaud L. Prevalence and correlates of physical activity behaviors among elementary schoolchildren in multiethnic, low income, inner-city neighborhoods in Montreal, Canada. Ann Epidemiol. 1999;9:397–407.
Ohta H, Kuroda T, Onoe Y, Nakano C, Yoshikata R, Ishitani K, et al. Familial correlation of bone mineral density, birth data and lifestyle factors among adolescent daughters, mothers and grandmothers. J Bone Miner Metab. 2010;28:690–5.
Pahkala K, Heinonen OJ, Lagström H, Hakala P, Sillanmäki L, Simell O. Leisure-time physical activity of 13-year-old adolescents. Scand J Med Sci Sports. 2007;17:324–30.
Raudsepp L. The relationship between socio-economic status, parental support and adolescent physical activity. Acta Paediatr. 2006;95:93–8.
Shropshire J, Carroll B. Family variables and children’s physical activity: influence of parental exercise and socio-economic status. Sport Educ Soc. 1997;2:95–116.
Siegel SR, Malina RM, Reyes MEP, Barahona EEC, Cumming SP. Correlates of physical activity and inactivity in urban Mexican youth. Am J Hum Biol. 2011;23:686–92.
Sigmund E, Turoňová K, Sigmundová D, Přidalová M. The effect of parents’ physical activity and inactivity on their children's physical activity and sitting. Acta Univ Palacki Olomuc. 2008;38:17–24.
Toftegaard-Støckel J, Nielsen G, Ibsen B, Andersen LB. Parental, socio and cultural factors associated with adolescents’ sports participation in four Danish municipalities. Scand J Med Sci Sports. 2011;21:606–11.
Trost SG, Pate RR, Saunders R, Ward DS, Dowda M, Felton G. A prospective study of the determinants of physical activity in rural fifth-grade children. Prev Med. 1997;26:257–63.
Trost SG, Pate RR, Ward DS, Saunders R, Riner W. Correlates of objectively measured physical activity in preadolescent youth. Am J Prev Med. 1999;17:120–6.
Wagner A, Klein-Platat C, Arveiler D, Haan MC, Schlienger JL, Simon C. Parent–child physical activity relationships in 12-year old French students do not depend on family socioeconomic status. Diabetes Metab. 2004;30:359–66.
Yang XL, Telama R, Laakso L. Parents’ physical activity, socioeconomic status and education as predictors of physical activity and sport among children and youths: a 12-year follow-up study. Int Rev Sociol Sport. 1996;31:273–91.
Anderson CB, Mâsse LC, Hergenroeder AC. Factorial and construct validity of the athletic identity questionnaire for adolescents. Med Sci Sport Exerc. 2007;39:59–69.
Anderson CB, Mâsse LC, Zhang H, Coleman KJ, Chang S. Contribution of athletic identity to child and adolescent physical activity. Am J Prev Med. 2009;37:220–6.
Arredondo EM, Elder JP, Ayala GX, Campbell N, Baquero B, Duerksen S. Is parenting style related to children’s healthy eating and physical activity in Latino families? Health Educ Res. 2006;21:862–71.
Beets MW, Vogel R, Forlaw L, Pitetti KH, Cardinal BJ. Social support and youth physical activity: the role of provider and type. Am J Health Behav. 2006;30:278–89.
De Bourdeaudhuij I, Lefevre J, Deforche B, Wijndaele K, Matton L, Philippaerts R. Physical activity and psychosocial correlates in normal weight and overweight 11 to 19 year olds. Obes Res. 2005;13:1097–105.
Gubbels JS, Kremers SPJ, Stafleu A, de Vries SI, Goldbohm RA, Dagnelie PC, et al. Association between parenting practices and children’s dietary intake, activity behavior and development of body mass index: the KOALA birth cohort study. Int J Behav Nutr Phys Act. 2011;8:18.
Hohepa M, Scragg R, Schofield G, Kolt GS, Schaaf D. Social support for youth physical activity: Importance of siblings, parents, friends and school support across a segmented school day. Int J Behav Nutr Phys Act. 2007;4:54.
Huang Y-J, Wong SH, Salmon J, Hui SS. Reliability and validity of psychosocial and environmental correlates measures of physical activity and screen-based behaviors among Chinese children in Hong Kong. Int J Behav Nutr Phys Act. 2011;8:16.
Klesges RC. The FATS: an observational system for assessing physical activity in children and associated parent behavior. Behav Assess. 1984;6:333–45.
Klesges RC, Malott JM, Boschee PF, Weber JM. The effects of parental influences on children’s food intake, physical activity, and relative weight. Int J Eat Disord. 1986;5:335–45.
Klesges RC, Eck LH, Hanson CL, Haddock CK, Klesges LM. Effects of obesity, social interactions, and physical environment on physical activity in preschoolers. Heal Psychol. 1990;9:435–49.
King KA, Tergerson JL, Wilson BR. Effect of social support on adolescents’ perceptions of and engagement in physical activity. J Phys Act Health. 2008;5:374–84.
Loucaides CA, Chedzoy SM, Bennett N, Walshe K. Correlates of physical activity in a Cypriot sample of sixth-grade children. Pediatr Exerc Sci. 2004;16:25–36.
Loucaides CA, Jago R. Correlates of pedometer-assessed physical activity in Cypriot elementary school children. J Phys Act Health. 2006;3:267–76.
Määttä S, Ray C, Roos E. Associations of parental influence and 10-11-year-old children’s physical activity: Are they mediated by children's perceived competence and attraction to physical activity? Scand J Public Health. 2014;42:45–51.
Mckenzie TL, Sallis JS, Nader PR, Patterson TL, Elder JP, Berry CC, et al. BEACHES: an observational system for assessing children’s eating and physical activity behaviors and associated events. J Appl Behav Anal. 1991;24:141–51.
McKenzie TL, Baquero B, Crespo NC, Arredondo EM, Campbell NR, Elder JP. Environmental correlates of physical activity in Mexican American children at home. J Phys Act Health. 2008;5:579–91.
Millstein RA, Strobel J, Kerr J, Sallis JF, Norman GJ, Durant N, et al. Home, school, and neighborhood environment factors and youth physical activity. Pediatr Exerc Sci Sci. 2011;23:487–503.
Moore JB, Davis CL, Baxter SD, Lewis RD, Yin Z. Physical activity, metabolic syndrome, and overweight in rural youth. J Rural Heal. 2008;24:136–42.
Moore JB, Beets MW, Morris SF, Kolbe MB. Day of the week is associated with meeting physical activity recommendations and engaging in excessive sedentary time in youth. J Phys Act Health. 2014;11:971–6.
Nelson MC, Gordon-Larsen P, Adair LS, Popkin BM. Adolescent physical activity and sedentary behavior: patterning and long-term maintenance. Am J Prev Med. 2005;28:259–66.
Pate RR, Trost SG, Felton GM, Ward DS, Dowda M, Saunders R. Correlates of physical activity behavior in rural youth. Res Q Exerc Sport. 1997;68:241–8.
Sabiston CM, Crocker PRE. Exploring self-perceptions and social influences as correlates of adolescent leisure-time physical activity. J Sport Exerc Psychol. 2008;30:3–22.
Beets MW, Pitetti KH, Forlaw L. The role of self-efficacy and referent specific social support in promoting rural adolescent girls’ physical activity. Am J Health Behav. 2007;31:227–37.
Brunet J, Sabiston CM, O’Loughlin J, Mathieu M-E, Tremblay A, Barnett T, et al. Perceived parental social support and moderate-to-vigorous physical activity in children at risk of obesity. Res Q Exerc Sport. 2014;85:198–207.
Butcher J. Socialization of adolescent girls into physical activity. Adolescence. 1983;18:753–66.
Butcher J. Longitudinal analysis of adolescent girls’ participation in physical activity. Sociol Sport J. 1985;2:130–43.
Kirby J, Levin KA, Inchley J. Parental and peer influences on physical activity among Scottish adolescents: a longitudinal study. J Phys Act Health. 2011;8:785–93.
Stucky-Ropp RC, DiLorenzo TM. Determinants of exercise in children. Prev Med. 1993;22:880–9.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
CY was responsible for the conception and drafting of the manuscript, and acquisition of data. RR was involved in revising the manuscript critically for important intellectual content. Both authors were responsible for the design of the manuscript, and analysis and interpretation of data. Both authors read and approved the final manuscript, and agree to be accountable for all aspects for the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigate and resolved.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Yao, C.A., Rhodes, R.E. Parental correlates in child and adolescent physical activity: a meta-analysis. Int J Behav Nutr Phys Act 12, 10 (2015). https://doi.org/10.1186/s12966-015-0163-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-015-0163-y