
Abstract
Background
Short birth interval (SBI) has profound implications for the health of both mothers and children, yet there remains a notable dearth of studies addressing wealth-based inequality in SBI and its associated factors in India. This study aims to address this gap by investigating wealth-based disparities in SBI and identifying the underlying factors associated with SBI in India.
Methods
We used information on 109,439 women of reproductive age (15–49 years) from the fifth round of the National Family Health Survey (2019-21). We assessed wealth-based inequality in SBI for India and its states using the Erreygers Normalised Concentration Index (ECI). Additionally, we used a multilevel binary logistic regression to assess the factors associated with SBI in India.
Results
In India, the prevalence of SBI was 47.8% [95% CI: 47.4, 48.3] during 2019-21, with significant variation across states. Bihar reported the highest prevalence of SBI at 61.2%, while Sikkim the lowest at 18.1%. SBI prevalence was higher among poorer mothers compared to richer ones (Richest: 33.8% vs. Poorest: 52.9%). This wealth-based inequality was visible in the ECI as well (ECI= -0.13, p < 0.001). However, ECI varied considerably across the states. Gujarat, Punjab, and Manipur exhibited the highest levels of wealth-based inequality (ECI= -0.28, p < 0.001), whereas Kerala showed minimal wealth-based inequality (ECI= -0.01, p = 0.643). Multilevel logistic regression analysis identified several factors associated with SBI. Mothers aged 15–24 (OR: 12.01, p < 0.001) and 25–34 (2.92, < 0.001) were more likely to experience SBI. Women who married after age 25 (3.17, < 0.001) and those belonging to Scheduled Caste (1.18, < 0.001), Scheduled Tribes (1.14, < 0.001), and Other Backward Classes (1.12, < 0.001) also had higher odds of SBI. Additionally, the odds of SBI were higher among mothers in the poorest (1.97, < 0.001), poorer (1.73, < 0.001), middle (1.62, < 0.001), and richer (1.39, < 0.001) quintiles compared to the richest quintile. Women whose last child had passed away were also significantly more likely to have SBI (2.35, < 0.001). Furthermore, mothers from communities with lower average schooling levels (1.18, < 0.001) were more likely to have SBI. Geographically, mothers from eastern (0.67, < 0.001) and northeastern (0.44, < 0.001) regions of India were less likely to have SBI.
Conclusion
The significant wealth-based inequality in SBI in India highlights the need for targeted interventions focusing on economically disadvantaged women, particularly in states with high SBI prevalence. Special attention should be given to younger mothers and those from socially disadvantaged groups to enhance maternal and child health outcomes across the country.
Similar content being viewed by others


Introduction
Birth intervals, the duration between two consecutive births, hold significant implications for maternal and child health. World Health Organization (WHO) recommends an interval of 24 months for birth-to-pregnancy and 33 months for birth-to-birth, assuming a gestation of 9 months for a healthy pregnancy and birth [1]. A birth interval of lesser than 33 months is termed a ‘short birth interval’ (SBI). An adequate birth interval is crucial for a mother’s recovery from the physical demands of pregnancy and childbirth, adequate lactation, nutrition, and equitable distribution of resources among all children [2]. In contrast, an SBI can lead to various health issues and morbidities for both the mother and child. These may include poor nutrition, underweight and stunting, less time spent breastfeeding, infections, high blood pressure, complications for the mother, and incomplete healing of the uterus [3,4,5,6]. When birth-to-birth spacing is extremely short, it may result in serious complications such neonatal and infant death, preterm delivery, reduced birth weight, smaller-than-expected size for gestational age, early membrane rupture, uterine tearing, placental separation, abnormal placental position, and pregnancy-induced hypertension [2, 5, 7,8,9,10].
Previous research conducted in low-and-middle-income countries, including India, has examined the issue of SBI and found that women’s demographic characteristics, including age, education, age at marriage, contraceptive use, parity, survival status of previous child, gender of previous child, preference for a son, and duration of breastfeeding of the previous child, have a significant impact on birth intervals [2, 5, 6, 8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. Similarly, socioeconomic and geographical factors, such as social group, religion, household wealth, autonomy, mass media exposure, place of residence, and region of residence have also been found to be associated with SBI [8, 13, 22, 31]. A few studies have attempted to investigate socioeconomic inequality in the prevalence of SBI [11, 15].
Health inequality or disparity across socioeconomic groups is an unjust difference in health and this is often viewed as objectionable from a human rights perspective [32]. Socioeconomic inequalities in health-related outcomes are common in most low-and-middle-income countries [15]. Therefore, health inequalities challenges have become a priority area for global organizations like WHO [1, 33] and United Nations Population Fund [34]. As the SBI could contribute to neonatal mortality, the Goal 3 of Sustainable Development Goals established by the United Nations, specifically targets 3.2.1 and 3.2.2, aim to eradicate preventable deaths among neonates and under-5 children. Each nation strives to achieve a reduction in neonatal mortality to below 12 deaths per 1,000 live births and under-five mortality to below 25 deaths per 1,000 live births by 2030, as shorter birth intervals have been linked to higher neonatal mortality rates. Additionally, the goal 10 of the SDGs seeks to reduce inequality within and among nations [35].
There is dearth of studies exploring socioeconomic disparity in SBI in India. The previous studies carried out in India on the issue of SBI mainly investigate significant correlates of birth interval on the national level, while some others have been conducted at smaller scales [3, 6, 12, 13, 18, 20, 21, 36]. While small-scale studies offer valuable insights into health behaviours, their findings cannot be applied to larger populations due to limited geographic representation and small sample sizes, which restrict their statistical power. The studies conducted at national level have used mostly the data from the nationally representative surveys such as the fourth round of the National Family Health Survey (NFHS) with hierarchical sampling designs. However, these studies have not used appropriate regression models for such data sets. Therefore, this study aims to address these gaps by pursuing two main objectives: firstly, measuring and analysing wealth-based inequality in SBI across different states of India, and secondly, examining the factors associated with SBI using a multilevel modelling approach.
Data and methods
Data source
We utilized data from the fifth round of the NFHS conducted during 2019-21. This survey covers a number of issues related to reproductive and child health, fertility, family planning, morbidity and mortality among Indian population. A two-stage sampling design was adopted in NFHS-5. Further details about the sampling design can be found in the NFHS-5 national reports [37]. NFHS-5 covered a sample of 724,115 women of reproductive age (15–49 years) from 636,699 households. The response rate was close to 97%. For this study, a subset of 109,439 women aged 15–49 from various Indian states and union territories (UT) was selected. The details of how we arrived at this sample of 109,439 women are provided in Fig. 1. We had to exclude 7696 observations due to missing values. Over 80% of these were excluded due to missing values in the variable ‘social group’. The rest of the excluded observation were either missing or inconsistent in variables related to age at marriage and birth history. Upon comparing the characteristics of excluded (missing) and included (non-missing) observations in our study dataset, we found only minor differences between these two groups (see Table A1 in Appendix).

Flow chart showing the process of sample selection from the NFHS-5 dataset
Statistical analysis
We initially calculated the prevalence of SBI for India and its states. Following this, we computed the Erreygers Normalised Concentration Index at both national and state levels to analyse wealth-based inequalities. We used the words disparity and inequality interchangably throughout the paper. Finally, multilevel logistic regression analysis was employed to identify the factors affecting SBI occurrence in India.
Erreygers normalised concentration index
We used Erreygers Normalised Concentration Index (ECI) to assess wealth-based inequality in SBI for India and each of its states and union territories. The ECI is modified version of the widely used Concentration Index (CI) which is a useful tool for measuring socioeconomic inequality in health sector variables. Mathematically “the concentration index is defined as twice the area between the concentration curve and the line of equality (the 45-degree line)”, which can be equated as [38]:
Where C is the concentration index, µ is the mean of the health variable, h is the health variable, and r is the cumulative percentage. The index ranges between − 1 to + 1 for an unbounded variable and µ-1 to 1- µ for a bounded variable.
However, when the health variable is binary, the mean of the distribution determines the limits of the potential values of the concentration index: as the mean increases, the range of possible concentration index values narrows [39]. Wagstaff suggested a normalization formula to address this limitation. He proposes dividing the health concentration index by its upper bound [39, 40]. This modified Wagstaff index for binary health variables only fulfils the transfer property, mirror property, and the level of independence property, but not the cardinal invariance. To develop a socio-economic inequality index that is rank-dependent and satisfies all four properties, Erreygers has introduced a corrected concentration index (also known as Erreygers Normalised Concentration Index) as [40]:
Where the n is the sample size, bh is the maximum value of the health variable, ah is the minimum value of the health variable, zi =\(\frac{n+1}{2}- \lambda\)i, and hi is a binary health variable that is equal to 0 when the woman with no SBI and takes a value of 1 otherwise.
Multilevel binary logistic regression
A multilevel binary logistic regression approach was utilized to explore the association of various factors at the individual, community, and district levels on SBI. Opting for a three-level logistic regression over a simple regression approach was deliberate, as it accommodates the hierarchical structure of the NFHS-5 dataset, where individuals (mothers) are nested within communities or primary sampling units (PSUs), and communities within districts. This multilevel framework is well-suited for such nested datasets, providing standard errors (SEs) adjusted for clustering effects. Conversely, relying on SEs estimated through a simple binary logistic regression model may underestimate SEs when the dataset used is hierarchical in nature, potentially impacting the interpretation of regression outcomes.
Before applying the three-level regression, we examined the extent to which the outcome of interest varies at higher levels (community and district levels). We fitted a null model, also known as empty model, contained no independent variables. We found that a considerable proportion of the total variation in SBI was at community and district levels. This suggested fitting a multilevel model made sense in our context. In Model 2, factors at the individual, community, and district levels were collectively incorporated. The fixed effects, indicating measures of association, are presented as odds ratios (ORs) with 95% confidence intervals. Meanwhile, the random effects, indicating measures of variation, are displayed as variance partition coefficients (VPCs) [41]. To evaluate multicollinearity in the regression model, we employed the variance inflation factor (VIF). All VIF values were comfortably below 2.4, a threshold indicating concern for multicollinearity affecting results (see Appendix Table A2). We utilized Stata 16 and MLwiN to carry out the multilevel logistic regression analysis [42].
Dependent variable: The dependent variable was SBI defined as a minimum interval of 24 months between a live birth and attempting the subsequent pregnancy [1]. When accounting for the nine-month gestational period, this translates to a birth-to-birth spacing of 33 months. In the NFHS-5, women were asked about their children’s birth dates using the century month code. The variable “preceding birth interval” was created by subtracting the birth date of the last child from that of the previous child, resulting in the duration of the birth interval in months. We recoded the birth interval as “1” if its duration was less than 33 months and as “0” if it was 33 months or longer.
Independent variables: Building upon existing literature, we incorporated a range of biodemographic, socioeconomic, family planning, and geographical factors into our analysis [10, 11, 13, 15, 19, 23,24,25, 28, 29, 43]. These factors included the age of women, women’s education level, age at marriage, social group, religion, place of residence, exposure to mass media, number of children prior to the index child, survival status of previous children, sex of the previous child, preference for a son, level of poverty in the community, level of education in the community, level of exposure to mass media regarding family planning in the community, and region of residence. For detailed information on the coding of these variables, please refer to Table 1.
Results
Prevalence of SBI in India and its states
The prevalence of SBI in India in 2019-21 was 47.8% (95% CI: 47.4–48.3). The prevalence varied considerably across the states of India (see Fig. 2). The prevalence of SBI was more than 50% in the states such as Bihar (61.2%, 60.2–62.4), Andhra Pradesh (60.6%, 57.8–63.4), Telangana (56.2%, 54.0-58.4), Nagaland (55.7%, 52.6–58.7), Madhya Pradesh (55.6%, 54.3–57.1), Rajasthan (51.4%, 49.9–53.0), Haryana (50.0%, 48.1–52.0), and Karnataka (51.6%, 49.3–53.9). On the other hand, the prevalence was less than 25% in the states of Sikkim (18.1%, 12.4–25.8), Tripura (18.3%, 15.4–21.7), Assam (20.9%, 19.1–22.9), and Kerala (21.5%, 19.1–24.2).

Proportion of women aged 15–49 years reporting short birth intervals in India, NFHS-5, 2019–21
Wealth-based disparity in SBI in India and its states
The prevalence of SBI in India decreases with an increase in the household wealth (see Fig. 3a). Approximately 53% of women in the poorest quintile reported SBI in India, whereas only 34% of women in the richest quintile reported SBI. This disparity was captured by concentration curve (CC) and ECI as well (see Fig. 3b). The CC depicts the association between the cumulative proportion of women reporting SBI on the vertical axis ranked by the cumulative percentage of the population ranked by the household wealth on the horizontal axis. The line of equality is represented by a 45-degree line, which indicates that the ECI is zero. The CC for the SBI lies above the line of equality, demonstrating that SBI was concentrated among the women from poorer households. The ECI was − 0.13 (Standard Error: 0.0035 and p-value < 0.001) and confirmed that there is wealth-based inequality in SBI in India.

Wealth-based inequality in SBI in India, 2019-21
Further, we calculated ECI for each state and UT individually to examine the variation in wealth-based inequality in SBI across the Indian states and UTs (see Table 2). The investigation of state ECIs revealed pro-poor inequality in the majority of the states. Among the states, the magnitude of pro-poor inequality in SBI was highest in Gujarat (ECI= -0.28, p < 0.001). Besides Gujarat, inequality in SBI was high (>-0.20) in Punjab (ECI= -0.28, p < 0.001), Manipur (ECI= -0.28, p < 0.001), Goa (ECI= -0.25, p < 0.018), Maharashtra (ECI= -0.23, p < 0.001), Madhya Pradesh (ECI= -0.21, p < 0.001), and Uttarakhand (ECI= -0.20, p < 0.001) as well. On the other hand, the lowest inequality in SBI was observed in the states of Kerala (ECI= -0.01, p = 0.643), Andhra Pradesh (ECI=-0.01, p = 0.820), Telangana (ECI= -0.05, p = 0.017) and Jharkhand (ECI= -0.04, p = 0.020).
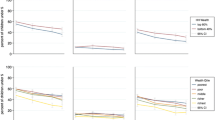
Figure 4a illustrates the distribution of states based on their prevalence of SBI and the magnitude of wealth-based inequality in SBI, categorized into four quadrants. Meanwhile, Fig. 4b illustrates SBI prevalence by wealth quintiles in each state (for estimates and their confidence interval, see Appendix Table A3). In the lower right quadrant states are the states with high prevalence of SBI (more than 35.0%) and high wealth-based inequality in SBI (ECI >− 0.15). This group of states includes the states of Himachal Pradesh (prevalence: 39.7%, ECI: -0.19), Uttarakhand (41.0%, -0.20), Punjab (39.4%, -0.28), Haryana (50.0%, -0.17), Rajasthan (51.4%, -0.16), Delhi (40.5%, -0.19), Madhya Pradesh (55.7%, -0.21), Gujarat (45.7%, -0.28), Maharashtra (44.4%, -0.23) in the northern and western regions, Karnataka (51.6%, -0.17) and Tamil Nadu (43.1%, -0.18) from the southern region, and Meghalaya (48.9%, -0.15) from the northeastern region. In contrast, states in the upper right quadrant which are Jammu and Kashmir (40%, -0.08), Uttar Pradesh (49.4%, -0.07), Bihar (61.3%, -0.04), Jharkhand (47.8%, -0.04), Telangana (56.2%, -0.05), Andhra Pradesh (60.7%, -0.01), and Nagaland (55.7%, -0.09) have high SBI prevalence but low wealth-based inequality in SBI. This is primarily due to a narrower gap in SBI between the rich and the poor in these states, as observed in Fig. 4b. Meanwhile, states in the lower left quadrant, including Ladakh (27.2%, -0.18), Odisha (25.9%, -0.18), West Bengal (27.9%, -0.18), Assam (20.9%, -0.18), Manipur (31.3%, -0.28), and Goa (28.8%, -0.25), demonstrate relatively low prevalence but high wealth-based inequality in SBI. This discrepancy is visually evident in Fig. 4b as well.

(a) Prevalence and wealth-based inequality in SBI across states of India, 2019-21. Note: A & N Islands: Andaman and Nicobar Islands; DDDNH: Daman and Diu and Dadra and Nagar Haveli. (b) Prevalence of SBI by wealth quintiles in selected states of India, 2019-21
Results of multilevel binary logistic regression
The initial stage of the multilevel model analysis involved evaluating whether our data supported the need to examine random effects at both the community and district levels. The Table 3 shows the result of the empty model. There was considerable variation in SBI across districts and communities. According to the VPC value obtained from the empty model, 12.7% and 9.0% of the total variance in SBI was attributed to the variation across communities and districts, respectively. For the sample characteristics and the prevalence of SBI by the background characteristics, see appendix Table A4 and A5.
The final model consisted of individual, community and district-level variables, and the result of the final model is shown in Table 4. The variance in the SBI was reduced to 6.0% across both the community and district. The result of the multilevel model revealed that women aged 15–24 (OR: 12.01, p < 0.001) and 25–34 (OR: 2.92, p < 0.001) were more likely to experience SBI compared to the women aged 35–49. Women who married between the ages of 20–25 had increased odds of experiencing SBI (OR: 1.78, p < 0.001), while those who married after the age of 25 had even higher odds (OR: 3.17, p < 0.001), in contrast to those who married before the age of 20. Women from poorest and poorer wealth quintiles were 1.97 and 1.73 times more likely to experience SBI as compared to women from the richest wealth quintile. SC, ST, and OBC women had slightly higher odds of experiencing SBI than those categorised as ‘Other’. Similarly, Muslim women (OR: 1.07, p = 0.008) and women from religions categorised as ‘Other’ (OR: 1.11, p = 0.003) had slightly higher odds of SBI than Hindu women.
The odds of SBI were 1.5 times higher among women who had two or more children before the index child (OR: 1.54, p < 0.001) compared to women who had only one child before the index child. The odds of SBI were twice higher (OR: 2.35, p = 0.036) among women whose previous child was no more. Women who were not exposed to family planning messages through mass media were slightly more likely to experience SBI (OR: 1.05, p = 0.008) compared to those women who were exposed. The likelihood of SBI was slightly higher among women residing in rural areas (OR: 1.07, p = 0.002) compared to those in urban areas. Furthermore, women living in communities with a higher proportion of poor individuals exhibited increased odds of SBI, with those in high-poverty areas having an 8% higher likelihood (OR: 1.08, p = 0.004), and those in medium-poverty areas having a 6% higher likelihood (OR: 1.06, p = 0.014), compared to women in low-poverty communities.
Women living in the communities with low (OR: 1.18, p < 0.001) and medium (OR: 1.14, p < 0.001) average years of schooling were 18% and 14% more likely to experience SBI than those women who lived in communities with higher average years of schooling, respectively. The odds of experiencing SBI were 6% higher among women with a medium level of exposure to family planning messages through mass media (OR: 1.06, p = 0.002) than women in a community with a high level of exposure. Women residing in the Northeastern (OR: 0.44, p < 0.001) and Eastern (OR: 0.67, p < 0.001) regions were 56% and 33% less likely to experience SBI than women residing in the Northern region [see Table 4].
Discussion
The study aimed to investigate wealth-based disparities in SBI and to identify factors associated with SBI at various levels—individual, community, and district—in India. The findings revealed that approximately half of mothers in India experienced SBI, with a concentration of SBI among women from poorer households. Moreover, significant variation in wealth-based inequality in SBI was observed across Indian states, with states such as Gujarat, Maharashtra, Madhya Pradesh, Goa, Punjab, Uttarakhand, and Manipur exhibiting higher levels of inequality. Several factors emerged as statistically significant associates of SBI in India. These factors included age, age at marriage, wealth quintile, total number of children before the index child, and survival status of previous children.
Our results indicate that SBI is associated with household wealth. This finding is consistent with earlier research [11, 13, 26, 30, 44, 45]. This finding may be attributed to the improvement in access to health education, family planning resources, and maternal healthcare services as women’s economic status improves. SBI disproportionately affect women from poorer backgrounds. This could be due to intertwined relationship between health and poverty, as poorer communities bear a heavier burden of ill health. Socioeconomic disparities hinder access to crucial health information and family planning resources to women, limiting their autonomy in reproductive decisions. This intensifies health inequalities, potentially compromising the well-being of both women and their children. Furthermore, a recent study indicated that higher socioeconomic status correlates with greater utilization of modern contraceptives, leading to a decreased likelihood of subsequent childbirth and thereby extending the interval between successive births [13, 26]. Mothers from economically disadvantaged households face significant barriers in accessing and utilizing effective contraception methods, increasing their vulnerability to SBI. Limited knowledge and financial constraints obstruct their ability to utilize modern and emergency contraceptive options, worsening the impact of economic disparities on reproductive health outcomes [15, 46, 47].
The prevalence of SBI decreased with the increase in woman’s age. Several previous studies have found a similar result; younger women are more likely to have a SBI when compared to older women [13, 19, 28]. This could be because women of younger age have motives to have their desired number of children quickly, whereas women of older age have a concern about infertility or menopause; in addition to that, older women have more autonomy and decision-making power about their reproductive choices [3, 6, 13].
The study found that women who married for the first time between the ages of 20–24 and 25–29 had higher probabilities of experiencing SBI between births compared to those who married before turning 20. Previous research on this topic has produced similar findings [48, 49]. This trend may be attributed to the fact that women who marry at an older age tend to want to complete their families more rapidly. Women marrying in their early to late twenties might be more conscious of their biological clocks and the potential risks associated with delayed childbearing, prompting them to expedite the process of having children [8, 19, 48].
Caste emerged as a significant predictor of SBI, and this result aligns with previous studies that have found that mothers from SC exhibits a higher likelihood of experiencing SBI [50, 51]. This could be because women from this social group are characterized by lower socioeconomic status, limited education, and lack of awareness about reproductive health and optimal birth interval [13].
Religion emerged as another significant factor associated with SBI, with Muslim women and women belonging to other religions slightly more likely to experience SBI. This finding aligns with previous research [26, 45, 51, 52] and the higher likelihood may be attributed to the underutilization of contraceptives and birth control methods among the followers of Muslim faith and other religions [53]. Additionally, factors such as low women’s autonomy and lack of awareness could contribute to the slightly elevated levels of SBI among the women of these faiths.
The study indicates that mothers with a birth order of two or more are more likely to experience SBI, which contradicts previous research [11, 28, 53]. One possible explanation for this discrepancy could that couples with higher birth orders may be intentionally seeking to have a larger family, which could lead them to have children in quick succession. Another reason could be a lack of knowledge and access to modern contraceptive methods, making it difficult for these couples to effectively plan and space their pregnancies. Additionally, these couples may not be fully aware of the potential disadvantages associated with having reduced intervals between births.
Mortality of a preceding child was associated with increased likelihood of SBI. This phenomenon may be attributed to the halt of breastfeeding following the death of the previous child, potentially leading to an earlier resumption of menstruation and ovulation among women. Consequently, some couples may unintentionally conceive another child within a reduced timeframe. Conversely, certain couples might intentionally seek to conceive another child expeditiously following the loss of the previous one. This finding aligns with earlier studies [8, 13, 19, 22, 31, 54].
Women exposed to mass media about family planning were slightly less likely to have SBI than those women without mass media exposure. The finding is similar to those of the existing literature. A reason for this finding could be that mass media plays an important role in creating awareness about small family size norms and family planning services, and women exposed to any type of mass media have a better understanding of the adverse effect the SBI can have on the health of both mother and child [5, 8, 11, 15, 22].
The study found place of residence a significant associate of SBI among women of reproductive age. Women residing in rural areas were more likely to experience SBI than their urban counterparts. The existing literature has also argued that despite government efforts, the rural residents still do not have easy access to modern healthcare services, exposure to information, and family planning methods [2, 5, 13, 15, 24, 29, 43]. This could one of the many reasons why women in rural areas still have a higher likelihood of experiencing SBI.
In 2017, the Government of India has launched ‘Mission Parivar Vikas’ to expand the accessibility of contraceptives and family planning services in the 146 high fertility districts. These districts are in the seven high-focus and high total fertility rates of Uttar Pradesh, Madhya Pradesh, Bihar, Rajasthan, Chhattisgarh, Jharkhand, and Assam. Under the initiative, there is a scheme of using ASHAs services for counselling newlywed couples to ensure a gap of two years in birth after the marriage and those couples with already one child to have an interval of three years after the birth of the first child. In addition to this, information, education and communication materials are used to raise awareness about the importance of ensuring appropriate space between childbirths [55, 56]. Under the scheme, ASHA is paid up to 1000 rupees in the form of incentives per couple. Every state except Kerala, Tamil Nadu, and Goa has approved the scheme’s spacing component.
Despite the government’s ongoing efforts and emphasis on family planning, the prevalence of SBI in India remains significantly higher than in many developing countries. Given the profound implications of SBI for maternal and child health, it is imperative for the government to intensify its efforts to reduce its prevalence. The observation that SBI varies considerably across states underscores the need for targeted interventions in specific geographical areas. Recognizing this variability, the government can tailor its strategies to address the unique challenges and socio-cultural factors influencing reproductive behaviours in different regions. Moreover, certain states exhibit both high levels of SBI and pronounced wealth-based inequalities in SBI. In these states, concerted efforts are required not only to reduce the overall proportion of women experiencing SBI but also to narrow the gap in SBI prevalence between socioeconomic groups. This necessitates a multifaceted approach that addresses both structural inequalities and barriers to accessing family planning services among marginalized populations. To effectively tackle the issue of higher prevalence of SBI and its associated health risks, the government should prioritize initiatives aimed at improving access to contraceptive services, promoting awareness about the importance of birth spacing, and addressing socioeconomic disparities that hinder equitable access to reproductive healthcare.
The key strengths of this study are as follows: it uses the latest nationally representative and population-based survey data to measure wealth-based inequality in SBI in India and its states. In the study, along with television, radio, and newspapers/magazines, we have included internet and hoardings while calculating the variable representing exposure for family planning messages through mass media. We also acknowledge that the study has a few limitations. First, we omitted a variable pertaining to the duration of breastfeeding before the index child as it had missing observations. Secondly, the absence of data on exact gestational periods in the NFHS-5 survey led us to assume an average gestational duration of nine months for all births. Third, we considered the birth interval of the most recent child only because the information about the previous child, which was needed in the analysis, could not be obtained due to data limitations. Additionally, the exclusion of missing observations in certain variables utilized for analysis was necessary to maintain the integrity of the study; however, it may have introduced bias into the results. Therefore, caution is advised when interpreting the findings.
Conclusion
The significant wealth-based inequality in SBI in India underscores the urgency of implementing targeted interventions that prioritize economically disadvantaged women, particularly in regions with high SBI prevalence. In addressing this disparity, special attention should be directed towards younger mothers and those belonging to socially disadvantaged groups. These vulnerable populations often face additional barriers to accessing reproductive healthcare services and may be at higher risk of adverse maternal and child health outcomes. Implementing targeted interventions tailored to the specific needs and circumstances of these groups is essential for achieving equitable access to reproductive healthcare services and ensuring the well-being of mothers and their children.
Data availability
The dataset analyzed during the current study is available in the Demographic and Health Surveys (DHS) repository, https://dhsprogram.com/data/available-datasets.cfm, and can be obtained for free by sending an online request. Codes used in the analysis can be made available from the corresponding author on request.
References
Cicely M. Report of a WHO Technical consultation on birth spacing. World Health Organization. Geneva; 2005.
RamaRao S, Townsend J, Askew I. Correlates of inter-birth intervals and implications of optimal birth spacing strategies in Mozambique. Popul Counc. 2006;40(3):1–19.
Das T, Roy TB. While inadequate birth interval becomes detrimental to health & nutritional outcome in infant and under-five year children; a systematic review through BLR and CPH model. Clin Epidemiol Glob Heal [Internet]. 2021;11(February):100714. https://doi.org/10.1016/j.cegh.2021.100714.
Kozuki N, Walker N. Exploring the association between short/long preceding birth intervals and child mortality: using reference birth interval children of the same mother as comparison. BMC Public Health. 2013;13(SUPPL.3).
Pimentel J, Ansari U, Omer K, Gidado Y, Baba MC, Andersson N, et al. Factors associated with short birth interval in low- and middle-income countries: a systematic review. BMC Pregnancy Childbirth. 2020;20(1):1–17.
Chungkham HS, Sahoo H, Marbaniang SP. Birth interval and childhood undernutrition: Evidence from a large scale survey in India. Clin Epidemiol Glob Heal [Internet]. 2020;8(4):1189–94. https://doi.org/10.1016/j.cegh.2020.04.012.
Molitoris J, Barclay K, Kolk M. When and where birth spacing matters for child survival: an International Comparison using the DHS. Demography. 2019;56(4):1349–70.
Shifti DM, Chojenta C, Holliday EG, Loxton D. Individual and community level determinants of short birth interval in Ethiopia: a multilevel analysis. PLoS ONE. 2020;15(1):1–17.
Rutstein SO. Effects of preceding birth intervals on neonatal, infant and under-five years mortality and nutritional status in developing countries: Evidence from the demographic and health surveys. Int J Gynecol Obstet. 2005;89(SUPPL. 1).
Nisha MK, Alam A, Islam MT, Huda T, Raynes-Greenow C. Risk of adverse pregnancy outcomes associated with short and long birth intervals in Bangladesh: evidence from six Bangladesh Demographic and Health Surveys, 1996–2014. BMJ Open. 2019;9(2):1–11.
Wegbom AI, Bademosi A, Edet CK, Green KI, Sapira-Ordu L, Fagbamigbe AF. Rural–urban disparities in birth interval among women of reproductive age in Nigeria. Sci Rep [Internet]. 2022;12(1):1–8. https://doi.org/10.1038/s41598-022-22142-y.
Jatrana S, Pasupuleti SSR. Women’s autonomy, education and birth intervals in India: Visiting the less familiar. Asian Popul Stud [Internet]. 2015;11(2):172–90. https://doi.org/10.1080/17441730.2015.1050083.
Chowdhury S, Singh A, Kasemi N, Chakrabarty M, Singh S. Short birth interval and associated factors in rural India: a cross-sectional study. J Biosoc Sci. 2022;1–20.
Brown W, Ahmed S, Roche N, Sonneveldt E, Darmstadt GL. Impact of family planning programs in reducing high-risk births due to younger and older maternal age, short birth intervals, and high parity. Semin Perinatol [Internet]. 2015;39(5):338–44. https://doi.org/10.1053/j.semperi.2015.06.006.
Shifti DM, Chojenta C, Holliday EG, Loxton D. Socioeconomic inequality in short birth interval in Ethiopia: a decomposition analysis. BMC Public Health. 2020;20(1):1–13.
Fazle Rabbi AM. Mass Media exposure and its impact on fertility: current scenario of Bangladesh. J Sci Res. 2012;4(2):383.
Gu H, Kou Y, You H, Xu X, Yang N, Liu J, et al. Measurement and decomposition of income-related inequality in self-rated health among the elderly in China. Int J Equity Health. 2019;18(1):1–11.
Kannaujiya AK, Kumar K, McDougal L, Upadhyay AK, Raj A, James KS et al. Interpregnancy Interval and Child Health Outcomes in India: evidence from Three Recent Rounds of National Family Health Survey. Matern Child Health J. 2022.
Nausheen S, Bhura M, Hackett K, Hussain I, Shaikh Z, Rizvi A, et al. Determinants of short birth intervals among married women: a cross-sectional study in Karachi, Pakistan. BMJ Open. 2021;11(4):1–10.
Yadava RC, Sharma SS. The distribution of consecutive closed birth intervals in females in Uttar Pradesh. J Biosoc Sci. 2007;39(2):189–99.
Hemochandra L, Singh NS, Singh AA. Factors Determining the Closed Birth Interval in Rural Manipur. J Hum Ecol [Internet]. 2010;29(3):209–13. https://doi.org/10.1080/09709274.2010.11906265.
Rabbi AMF, Karmaker SC, Mallick SA, Sharmin S. Determinants of Birth Spacing and Effect of Birth Spacing on Fertility in Bangladesh. Dhaka Univ J Sci. 2013;61(1):105–10.
Aychiluhm SB, Tadesse AW, Mare KU, Abdu M, Ketema A. A multilevel analysis of short birth interval and its determinants among reproductive age women in developing regions of Ethiopia. PLoS One [Internet]. 2020;15(8 August):1–13. https://doi.org/10.1371/journal.pone.0237602.
de Jonge HCC, Azad K, Seward N, Kuddus A, Shaha S, Beard J, et al. Determinants and consequences of short birth interval in rural Bangladesh: a cross-sectional study. BMC Pregnancy Childbirth. 2014;14(1):1–7.
Ahammed B, Kabir MR, Abedin MM, Ali M, Islam MA. Determinants of different birth intervals of ever married women: evidence from Bangladesh. Clin Epidemiol Glob Heal. 2019;7(3):450–6.
Tuz- Zahura F, Sen KK, Nilima S, Bari W. Can women’s 3E index impede short birth interval? evidence from Bangladesh Demographic and Health Survey, 2017-18. PLoS One [Internet]. 2022;17(1 January). https://doi.org/10.1371/journal.pone.0263003.
Afeworki R, Smits J, Tolboom J, Van Ven A, Der. Positive effect of large birth intervals on early childhood hemoglobin levels in Africa is limited to girls: cross-sectional DHS study. PLoS ONE. 2015;10(6):1–14.
Islam MZ, Islam MM, Rahman MM, Khan MN. Exploring hot spots of short birth intervals and associated factors using a nationally representative survey in Bangladesh. Sci Rep [Internet]. 2022;12(1):1–10. https://doi.org/10.1038/s41598-022-13193-2.
Yohannes S, Wondafrash M, Abera M, Girma E. Duration and determinants of birth interval among women of child bearing age in Southern Ethiopia. BMC Pregnancy Childbirth. 2011;11:2–7.
Chirwa TF, Mantempa JN, Kinziunga FL, Kandala JD, Kandala NB. An exploratory spatial analysis of geographical inequalities of birth intervals among young women in the democratic republic of Congo (DRC): a cross-sectional study. BMC Pregnancy Childbirth. 2014;14(1):1–10.
Karkee R, Lee AH. Birth spacing of pregnant women in Nepal: a community-based study. Front Public Heal. 2016;4(SEP):1–5.
Arcaya MC, Arcaya AL, Subramanian SV. Inequalities in health: definitions, concepts, and theories. Glob Health Action. 2015;8:27106.
World Health Organization. Birth spacing — report from a WHO technical consultation. Geneva; 2006.
Ministry of Health Development. Looking Beyond Numbers [Internet]. Republic of Somaliland. 2021. Available from: www.somalilandmohd.com.
Transforming Our World: The 2030 Agenda for Sustainable Development [Internet]. United Nations. 2016. Available from: sustainabledevelopemnt.un.org.
Ramesh P. Determinants of birth interval dynamics in Orissa, India. Heal (San Fr. 2006;1999(June):1–30.
International Institute of Population Sciences. National Family Health Survey (NFHS – 5), 2019-21 [Internet]. 2022. http://rchiips.org/nfhs/NFHS-5Reports/NFHS-5_INDIA_REPORT.pdf.
Donnell, Owen O’. Doorslaer, Eddy Van; Wagstaff, Adam; Linedelow M. Analyzing Health Equity Using Household Survey Data. Washington, D.C: World Bank; 2008.
Wagstaff A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ. 2005;14(4):429–32.
Erreygers G. Correcting the Concentration Index. J Health Econ. 2009;28(2):504–15.
Rasbash J, Steele F, Browne WJ, Goldstein H. A user’s guide to MLwiN. Cent Multilevel Model Univ Bristol; 2023.
StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LLC.; 2013.
Bumpass LL, Rindfuss RR, Palmore JA. Determinants of korean birth intervals: The confrontation of theory and data*. Popul Stud (NY) [Internet]. 1986;40(3):403–23. https://www.jstor.org/stable/2174583.
Belachew TB, Asmamaw DB, Negash WD. Short birth interval and its predictors among reproductive age women in high fertility countries in sub-Saharan Africa: a multilevel analysis of recent Demographic and Health Surveys. BMC Pregnancy Childbirth [Internet]. 2023;23(1):1–9. https://doi.org/10.1186/s12884-023-05403-0.
Kassie SY, Ngusie HS, Demsash AW, Alene TD. Spatial distribution of short birth interval and associated factors among reproductive age women in Ethiopia: spatial and multilevel analysis of 2019 Ethiopian mini demographic and health survey. BMC Pregnancy Childbirth [Internet]. 2023;23(1):1–14. https://doi.org/10.1186/s12884-023-05610-9.
Alhassan AR, Anyinzaam-Adolipore JN, Abdulai K. Short birth interval in Ghana: maternal socioeconomic predictors and child survival. Popul Med. 2022;4(January):1–8.
Islam MZ, Islam MM, Rahman MM, Khan MN. Prevalence and risk factors of short birth interval in Bangladesh: Evidence from the linked data of population and health facility survey. PLOS Glob Public Heal [Internet]. 2022;2(4):e0000288. https://doi.org/10.1371/journal.pgph.0000288.
Nath DC, Singh KK, Land KC, Talukdar PK. Age of marriage and length of the first birth interval in a traditional Indian society: life table and hazards model analysis. Hum Biol Int Rec Res. 1993;65(5):783–97.
Kannaujiya AK, Kumar K, Upadhyay AK, McDougal L, Raj A, Singh A. Short interpregnancy interval and low birth weight births in India: Evidence from National Family Health Survey 2015-16. SSM - Popul Heal [Internet]. 2020;12(November):100700. https://doi.org/10.1016/j.ssmph.2020.100700.
Kumar A, Singh A. Explaining the gap in the use of maternal healthcare services between social groups in India. J Public Heal (United Kingdom). 2016;38(4):771–81.
Yadava KNS, Jain SK, Kumar A. Correlates of birth intervals in rural northern India. Genus. 2000;56(1):55–76.
Ghosh P, Rohatgi P, Bose K. Determinants of time-trends in exclusivity and continuation of breastfeeding in India: An investigation from the National Family Health Survey. Soc Sci Med [Internet]. 2022;292(March 2021):114604. https://doi.org/10.1016/j.socscimed.2021.114604.
Gebrehiwot SW, Abera G, Tesfay K, Tilahun W. Short birth interval and associated factors among women of child bearing age in northern Ethiopia, 2016. BMC Womens Health. 2019;19(1):1–9.
Khan JR, Bari W, Latif AHMM. Trend of determinants of birth interval dynamics in Bangladesh. BMC Public Health [Internet]. 2016;16(1):1–11. https://doi.org/10.1186/s12889-016-3577-9.
Ministry of Health and Family Welfare. Annual Report-Family Planning [Internet]. New Delhi. 2018. https://mohfw.gov.in/sites/default/files/06Chapter.pdf.
Minsitry of Health and Family Welfare. Initiatives under the Family Planning Programme. Press Information Bureau, Government of India [Internet]. 2017; https://pib.gov.in/Pressreleaseshare.aspx?PRID=1680702.
Acknowledgements
The authors are grateful to the Demographic and Health Surveys (DHS) for providing the dataset for this study. Dr. Aditya Singh acknowledges the support provided by Banaras Hindu University’s Institute of Eminence (IOE) Seed Grant No. 48726, while Anshika Singh acknowledges the support received in the form of a Junior Research Fellowship from the University Grants Commission, India (Reference Number: 210510846284).
Funding
The authors received no funding for this work.
Author information
Authors and Affiliations
Contributions
A.D.S.: conceptualization, design, data analysis, interpretation of data, visualization, supervision, writing – original draft, writing – review and editing. A.N.S.: data curation, data analysis, writing – original draft, writing – review and editing. M.C.: data analysis, supervision, writing – original draft, writing – review and editing. S.S. & P.T.: writing – review, and editing.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The present study used secondary data, which is available in the public domain. The dataset has no identifiable information about the survey participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Singh, A., Singh, A., Chakrabarty, M. et al. Wealth-based disparities in the prevalence of short birth interval in India: insights from NFHS-5. Popul Health Metrics 22, 14 (2024). https://doi.org/10.1186/s12963-024-00334-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12963-024-00334-0