
Abstract
Background
Nicotine vaping products (NVPs) are increasingly popular worldwide. They may provide public health benefits if used as a substitute for smoking, but may create public health harms if used as a gateway to smoking or to discourage smoking cessation. This paper presents the Smoking and Vaping Model (SAVM), a user-friendly model which estimates the public health implications of NVPs in the USA.
Methods
SAVM adopts a cohort approach. We derive public health implications by comparing smoking- and NVP-attributable deaths and life-years lost under a No-NVP and an NVP Scenario. The No-NVP Scenario projects current, former, and never smoking rates via smoking initiation and cessation rates, with their respective mortality rates. The NVP Scenario allows for smoking- and NVP-specific mortality rates, switching from cigarette to NVP use, separate NVP and smoking initiation rates, and separate NVP and smoking cessation rates. After validating the model against recent US survey data, we present the base model with extensive sensitivity analyses.
Results
The SAVM projects that under current patterns of US NVP use and substitution, NVP use will translate into 1.8 million premature smoking- and vaping-attributable deaths avoided and 38.9 million life-years gained between 2013 and 2060. When the NVP relative risk is set to 5%, the results are sensitive to the level of switching and smoking cessation rates and to a lesser extent smoking initiation rates. When the NVP relative risk is raised to 40%, the public health gains in terms of averted deaths and LYL are reduced by 42% in the base case, and the results become much more sensitive to variations in the base case parameters.
Discussion
Policymakers, researchers, and other public health stakeholders can apply the SAVM to estimate the potential public health impact of NVPs in their country or region using their own data sources. In developing new simulation models involving NVPs, it will be important to conduct extensive sensitivity analysis and continually update and validate with new data.
Conclusion
The SAVM indicates the potential benefits of NVP use. However, given the uncertainty surrounding model parameters, extensive sensitivity analysis becomes particularly important.
Similar content being viewed by others


Background
Smoking prevalence has markedly declined in the USA over the past 50 years [44, 92]. During that time, cigarette taxes were substantially increased, and smoke-free air policies, media campaigns, youth access policies and smoking cessation treatments were implemented [92]. These policies have been shown to be effective [54], and can explain much of the reduction in smoking prevalence [44, 50, 92, 101, 102]. Despite this progress, the harms from cigarette smoking remain unacceptably high [92]. More than 480,000 Americans die each year due to smoking, and two-thirds of long-term smokers die prematurely of a smoking-attributable disease [11, 48, 91]. To drastically reduce the harms of smoking on population health, innovative approaches are needed.
The rising use of nicotine vaping products (NVPs), also known as e-cigarettes or electronic nicotine delivery systems (ENDS), has been a source of both promise and controversy [51, 52]. NVPs, especially later generation models, have been shown to more efficiently deliver nicotine [24, 28, 33, 99, 106] and have sensorimotor effects and throat irritation similar to smoking [26, 34, 38, 98], thus potentially serving as a substitute for cigarettes. NVPs are increasingly being used by smokers to quit [10, 30, 32], and recent studies indicate their effectiveness [9, 39, 55, 107]. If smokers switch entirely to NVPs, the health benefits could be substantial since NVPs deliver only a fraction of the toxicants delivered by smoking [35, 36, 41, 77, 80, 82, 83]. However, there is also concern about increased use of these products by youth [20] and their potential to increase youth cigarette smoking [84, 104], inhibit smoking cessation [70, 73], and promote relapse [5, 22].
The US Food and Drug Administration has the authority to regulate NVPs [29] and must now consider “the risks and benefits of the tobacco product to the population as a whole” [93]. In their review of NVPs, the agency evaluates the toxicity of the product and its effect on the uptake and cessation of existing tobacco products from a public health perspective. The impact of NVP use (“vaping’) on population health will depend on its use in relation to cigarette use (“smoking”) [51, 52]. As a reduced risk alternative, vaping would improve public health when used by those who would have otherwise initiated smoking or by those who would not have otherwise quit smoking. Vaping would worsen public health when used by those who would not have otherwise initiated NVPs or smoking (i.e., as a gateway to smoking) or if used by those who would have otherwise quit smoking. The ability to accurately predict these impacts will depend on the ability to incorporate transitions between NVPs and smoking, but knowledge of the relevant transitions is often lacking.
While many models have been developed that incorporate NVPs [6, 14, 17, 42, 49, 65, 76, 85, 103, 105], these models are often geared towards specific applications, lack the flexibility to be easily applied to other settings, require substantial efforts to understand, require data that is not generally available and have not been validated against real-world data. Because NVP model parameters are subject to considerable uncertainty, it is also important that sensitivity analysis can be easily conducted.
We present the Smoking and Vaping Model (SAVM), which aims to bridge these gaps. This user-friendly model is based on an earlier model [53], but provides greater flexibility by incorporating a wider range of initiation, cessation and switching parameters and can easily be adapted to other countries, states, or local areas. The SAVM differs from previous work in four ways. First, the SAVM adopts a cohort-based approach, thereby incorporating any dependence of NVP use patterns on the availability of NVPs and current policies in effect at a particular age and year (e.g., adolescents who initiated e-cigarette use prior to 2013 had less exposure to NVPs than adolescents who initiated after 2013). Second, the model has a simplified structure and is available in Excel, making it transparent and more easily adapted and applied. Third, the model is validated against recent national survey data. Finally, the model is developed to conduct comprehensive sensitivity analyses of the NVP parameters. This study presents the model and demonstrates its application to the USA.
Methods
The public health impact of NVP use among smokers and non-smokers is estimated by comparing two scenarios: a) the No-NVP Scenario which projects future cigarette use and associated mortality outcomes for each birth cohort in the absence of NVPs, and b) the NVP Scenario which incorporates NVP use patterns into each cohort’s cigarette use trajectory. To simplify the model and ensure that health outcomes reflect regular (i.e., stable) use patterns over time [48], we focus on the regular (rather than experimental) use of NVPs and cigarettes and the transitions between those uses.
The No-NVP Scenario
The SAVM begins with separate cohorts of males and females by individual age. Within each cohort, the population evolves with age. The No-NVP Scenario projects the prevalence of current and former smokers over time using age- and gender-specific initiation and cessation rates for each cohort that were previously developed using an age-period-cohort statistical smoking model [43, 45, 47, 88]. The initiation and cessation rates are projected forward based on data from the US National Health Interview Survey (NHIS) through the year 2013, before NVPs were in more widespread use [58] and thus reflects smoking patterns in the absence of NVPs. The transitions are shown in Fig. 1a.

a Transitions between smoking states in the No-NVP Scenario. b Transitions between regular smoking and nicotine vaping product use states in the NVP Scenario. NVP, nicotine vaping product. aSmoking initiation includes initiation into regular cigarette use net of any experimental NVP use and includes those who become regular dual users who smoke and regularly use NVPs. bNVP initiation includes initiation into regular NVP use net of any experimental cigarette use. cSwitching after age 35 includes those regular smokers who quit smoking and switch to regular NVP and are considered before former smokers using NVPs. dSwitching before age 35 includes those regular smokers who quit smoking and switch to regular NVP use, and considered exclusive NVP users due to the reduced risks of quitting smoking before age 35. eSmoking cessation includes cessation from regular cigarette use and dual users who quit both cigarette and NVP use, but may include those who quit smoking and temporarily use NVP. fFormer smoker using NVPs cessation includes those former smokers who quit NVPs and remain former smokers. NVP cessation includes those exclusive NVP users who quit NVP use
Individuals are born as never users, which in the context of the No-NVP model is just never smokers. For a given cohort, never users at age a and year t includes surviving never users in the previous year (age a-1, year t-1) who did not initiate smoking, where surviving never users are modeled as never users at age a-1 in year t-1 multiplied by (1—mortality rate of never usersa-1,t-1). Smoking initiation among never users can occur through age 40 and reflects the transition to becoming an established current smoker, defined as having smoked at least 100 cigarettes during one’s lifetime and currently smoking every day or some days. Smokers at age a and year t include surviving never users at age a-1 and year t-1 who initiated smoking and surviving smokers (using current smoker mortality rates) who did not quit since the previous year (age a-1, year t-1). Smoking cessation among current smokers reflects the permanent transition to becoming a former smoker and requires that the smoker quit at least 2 years; this avoids the need to model relapse and reflects the underlying inputs used for this and other tobacco models [44, 45, 88]. Former smokers include surviving former smokers (based on age- and former smoker-specific mortality rates) and surviving smokers who quit smoking for at least 2 years.
The NVP Scenario
Starting from the same initial current, former, and never smoking prevalence as in the No-NVP Scenario, the NVP Scenario is expanded to include current and former NVP use. The transitions are shown in Fig. 1b.
Because SAVM focuses on measures of regular use, the NVP Scenario does not explicitly model individual youth transitions directly from short-term vaping to regular smoking. Any such transitions are however incorporated indirectly through a smoking initiation multiplier reflecting the net effect of vaping on smoking initiation rates. Similarly, the NVP Scenario does not explicitly model short-term NVP use leading to quitting both cigarettes and NVPs, but is indirectly incorporated through a smoking cessation multiplier reflecting the net effect of vaping on smoking cessation rates. In addition, the NVP Scenario does not distinguish dual cigarette and NVP users from exclusive smokers, because dual users have generally been found to either remain dual users or soon transition to either exclusive cigarette or exclusive NVP use [4, 8, 18, 78, 86, 89] and the health risks of dual users appear to be similar to those of exclusive smokers [36, 82, 83]. However, transitions from dual use to exclusive NVP use or neither cigarette nor NVP use are reflected in the switching and smoking cessation parameters.
Never users include surviving never users from the previous age and year who do not initiate into regular smoking or NVP use. The model directly relates the NVP Scenario to the No-NVP Scenario through separate linear multipliers applied to the smoking initiation rate in the No-NVP Scenario. Using a linear multiplier assures that NVP and smoking initiation follow the same age patterns for smoking initiation as in the No-NVP case, e.g., smoking initiation mostly occurs before age 21 and is minimal after age 30. NVP initiation is similarly tied to smoking initiation in the No-NVP Scenario, whereby a multiplier value less than (or greater than) 100% implies that NVP initiation rates are less than (or greater than) smoking initiation rates in the No-NVP Scenario.
In the NVP Scenario, smokers become former smokers in one of two ways: (1) they may switch to regular exclusive NVP use, or (2) they may quit both regular smoking and regular NVP use (e.g., dual users would quit both) and thereby become former smokers. In the latter case, the smoker may temporarily use NVPs but quit both smoking and vaping. The overall reduction in smokers in the NVP Scenario is the reduction in smokers from switching and complete cessation, and this sum may be less (e.g., harm reduction) or more (harm increasing) than the number of smokers in the No-NVP Scenario. Smokers age a in year t include surviving smokers at age a-1 and year t-1 who did not switch to exclusive vaping and who did not quit smoking, and surviving never users at age a-1 and year t-1 who initiated smoking.
Similar to the initiation process, smoking and vaping cessation are modeled as separate linear multipliers of smoking cessation in the No-NVP Scenario, so that smoking cessation follows the same age pattern in the No-NVP Scenario and tends to increase with age. Since studies to date do not indicate different age patterns, the smoking and vaping initiation and cessation multipliers are simply modeled as independent of age. In addition, these multipliers are assumed to remain constant over time, so that smoking and vaping initiation and cessation in the NVP Scenario follow the same temporal patterns as in the No-NVP Scenario.
Former smokers who either switch to or quit smoking before age 35 are distinguished from those who quit or switch at age 35 or above. Those who quit smoking (by switching to NVPs or cessation) before age 35 are classified the same as never smokers who vape rather than as former smokers, because mortality risks of smoking are minimal when quitting before age 35 [48]. Those who quit at age 35 or above maintain the former smoker status and its resulting mortality risks. Thus former smokers include surviving former smokers, surviving smokers (age > 35) who quit smoking and do not vape, surviving smokers who switched to vaping (age > 35), and surviving former smokers who at one point regularly vaped but quit vaping.
Exclusive NVP users include surviving never users who initiate vaping, surviving vapers who do not quit, and those switching to vaping from surviving current smokers before age 35. Similar to smokers, those who quit smoking before age 35 are treated the same as never smokers who vape rather than former smokers. Since former smokers using NVPs may quit vaping, former smokers using NVPs includes surviving former smokers using NVPs who do not quit vaping and smokers who switch to vaping (after age 35).
A detailed discussion of the parameters and equations used in both scenarios can be found in Supplement 1.
Public health outcomes
The SAVM considers two public health outcomes: (1) Smoking- and vaping-attributable deaths and (2) smoking- and vaping-attributable life-years lost (LYLs). Both are based on the excess risks of smoking or vaping and the number of current and former smokers and vapers.
In the No-NVP Scenario, smoking-attributable deaths (SADs) by age and gender for current smokers are calculated by applying the excess risks of current smokers relative to never smokers (current smoker mortality ratea,t − never smoker mortality ratea,t) to the smoking population and for former smokers are calculated by applying the excess risks of former smokers relative to never smokers (former smoker mortality ratea,t − never smoker mortality ratea.t) to the former smoker population. SADs for current and former smokers are summed over all ages in a particular year to obtain total SADs in that year. LYLs are estimated as the number of premature deaths multiplied by the remaining life expectancy of a never smoker at age a in year t. The sum over all ages in a particular year obtains the LYLs in that year.
In the NVP Scenario, current and former smoker SADs are calculated in the same manner in the No-NVP Scenario as above except using their respective current and former smoker population sizes from the NVP scenario. For current and former exclusive NVP users, attributable deaths are a product of the number of NVP users and the excess risks of smoking adjusted by NVP relative risk, denoted by RiskNVP, i.e., RiskNVP*(current smoker mortality ratea,t − never smoker mortality ratea,t) for current users and RiskNVP*(former smoker mortality ratea,t − never smoker mortality ratea,t) for former users. As a special case in the NVP Scenario, the mortality rate of NVP users who previously smoked is determined by the mortality rate of former smokers plus the portion of excess NVP risk of current relative to former smokers. Smoking and vaping-attributable deaths (SVADs) for former smokers who currently use NVPs is measured as a product of the number of former smokers who currently use NVPs and the excess mortality risk of these users to never smokers, calculated as (former smoker using NVPs mortality ratea,t − never smoker mortality ratea,t). Total attributable deaths are calculated by summing SVADs over all ages in each year. LYLs in the NVP Scenario at each age are calculated as the product of SVADs and life-years remaining of never smokers. Summing over all ages in a particular year obtains the total LYLs in that year.
The public health impact of NVP use each year is evaluated as the difference in attributable deaths between the No-NVP and NVP Scenarios, and similarly for LYLs.
Data and parameter specification
In SAVM, the analysis of current, former and never smoking and vaping is in terms of their prevalence. These prevalence rates are translated into population numbers using actual and projected US population size estimates [12]. While the model itself does not explicitly incorporate projected births, mortality, and immigration, the CDC projections incorporate projected births, mortality, and immigration.
A detailed description of model parameters is provided in Table 1.
The No-NVP Scenario
The initial level of current, former and never smoking prevalence, the smoking initiation and cessation rates used to project these future prevalence rates, mortality rates by smoking status, and the life expectancy of never smokers used in the No-NVP model were previously developed [43,44,45, 79] available on the National Cancer Institute: Cancer Intervention and Surveillance Modeling Network (CISNET) website [16]. These measures apply data only through 2013 to incorporate trends prior to the time when NVPs became more widely used.
The NVP Scenario
The NVP Scenario requires six input parameters: NVP mortality risks, NVP switching rate, smoking initiation, vaping initiation, smoking cessation, and vaping cessation.
The NVP relative risk multiplier, RiskNVP, represents the relative risk of death associated with current NVP use as a percentage of the excess mortality risk experienced by current or former smokers as defined above. NVP relative mortality risk is designated at 5% of cigarette excess risks based on a multi-criteria decision analysis [75] and a Public Health England review [64]. Since others have suggested higher risks [23, 74, 90, 95], an NVP relative risk multiplier of 40% is also considered.
The NVP switching rate is the annual rate at which current smokers switch from smoking to NVP use, leading to a direct reduction in smoking prevalence. Baseline male (female) NVP yearly switching rates are based on weighted data by age group that we generated from the 2013/2014, 2014/2015, 2015/2016, and 2016/2017 Population Assessment of Tobacco and Health (PATH) surveys [94] averaged over years, as described in Supplement 2. These are: 8% (5%) age 10–17; 4.0% (2.5%) for ages 18–24, 2.5% (2.0%) for ages 25–34, 2.5% (1.6%) for age 35–44, 1.3% (1.4%) for ages 45–54, 1.2% (1.4%) for ages 55–64, and 0.6% (1.0%) for ages 65. We also consider switching rates that are 50% lower and 100% higher than the baseline estimates. These rates are initially assumed constant over time (i.e., 0% decay), but we also consider a 10% decay (i.e., annual rate of decline) to reflect the possibility of reduced innovation in NVPs over time and the tendency for those who are most amenable to switching to or quitting NVPs to have already switched, leaving a population less amenable to switching and quitting. However, because innovation in NVP design may increase their substitutability for cigarettes and potentially increase switching, we also consider an annual 5% increase rate for the first five years (2018–2022).
Since the smoking initiation in the NVP Scenario is measured relative to smoking initiation in the No-NVP Scenario, the smoking initiation multiplier is greater than 100% if NVP use increases net smoking initiation beyond the rate at which individuals would have otherwise initiated smoking in the absence of NVPs (i.e., gateway in > gateway out), and is less than 100% if those who would have initiated smoking tend to transition to exclusive NVP use instead of smoking (i.e., gateway out > gateway in). Based on the more rapid downward trend in US youth and young adult smoking as NVP use increased in recent years [57], the age- and year-invariant baseline smoking initiation multiplier is initially set at 75%, i.e., a 25% net decrease in smoking initiation due to vaping. A range of 25 to 125% is also considered.
The NVP initiation rate multiplier reflects the youth and young adult initiation of NVP use relative to smoking initiation rates in the No-NVP Scenario. If less than 100%, NVP initiation rates are lower than smoking initiation rates in the No-NVP Scenario. i.e., fewer individuals become regular NVP users than who would have become smokers in the No-NVP Scenario. Reflecting the increased US youth and young adults regular NVP users in recent years [20, 40, 51, 52, 68, 69], the age- and year-invariant baseline NVP initiation multiplier is initially set at 50%. Sensitivity analysis is conducted over the range of 25 to 75%.
Since smoking cessation in the NVP Scenario is measured relative to smoking cessation in the No-NVP Scenario, the smoking cessation multiplier is greater than 100% if smoking cessation rates are higher in the NVP Scenario than in the No-NVP Scenario, e.g., if the availability of NVPs leads to increased smoking cessation. A parameter less than 100% implies that smokers are less likely to quit smoking in the NVP Scenario compared with the No-NVP Scenario, e.g., NVP use leads to dual use (continued smoking) rather than complete cessation among smokers. The baseline smoking cessation rate multiplier is initially set at 100%, with sensitivity analysis at 50% and 150%.
The NVP cessation multiplier is greater than 100% if NVP cessation rates are higher than smoking cessation rates in the No-NVP Scenario, e.g., NVPs are less addictive than cigarettes. The parameter is less than 100% if NVP cessation rates are lower than smoking cessation rates in the No-NVP Scenario. The baseline NVP cessation multiplier is set at 100%, with sensitivity analysis at 50% and 150%.
Model validation and analysis
The model estimates the NVP effects over time for the prevalence of current and former smokers, current and former NVP users, and former smokers using NVPs, and for smoking-attributable and NVP-attributable deaths and LYLs. The model was first validated over the years 2013 to 2018 by comparing model predictions of current smoking prevalence to current smoking prevalence rates from the NHIS [13]. We focus on relative reductions over the period 2013–2018, because levels of model smoking prevalence in the initial year 2013 differ from those in the NHIS.
We also validated NVP use. Although NVP use was already occurring in 2013, the model itself begins with no NVP use that year and is adjusted to reach the 2018 levels [57]. Consequently, we validated NVP use prevalence against NHIS estimates for 2018, the latest year for which data was available rather than rely on prior trend data. We defined regular NVP users as those who used NVPs at least 10 of the past 30 days to reflect more regular use [3, 58].
Upon validating the model, we consider how NVP use affects smoking prevalence, smoking-attributable and NVP-attributable deaths, and LYLs. We conduct sensitivity analyses for the NVP transition and risk parameters over the plausible ranges specified above focusing on their impact on premature attributable deaths and LYLs.
Results
Validation of smoking prevalence
Using the initial (best estimate) input parameter estimates, the SAVM predictions are validated against smoking prevalence from NHIS data for 2013–2018 as shown in Table 2. For ages 18 and above, SAVM projects that male (female) smoking prevalence fell from 21.4% (15.9%) in 2013 to 16.7% (12.6%) in 2018, while NHIS shows a decline from 20.3% (15.4%) in 2013 to 15.8% (12.0%) in 2018. NHIS shows a 22.2% (22.1%) relative reduction between 2013 and 2018 compared with a 22.2% (20.7%) relative reduction in SAVM.
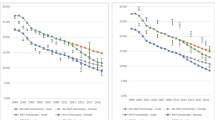
The SAVM and NHIS smoking prevalence for males ages 18 and above is shown in Fig. 2a (including NHIS estimates with 95% confidence intervals) with male SAVM prevalence rates scaled by the ratio of survey estimate to the SAVM level in 2013, e.g., NHIS 20.3%/ SAVM 21.4% = 94.9%). Female prevalence rates are shown in Fig. 2b., with female SAVM prevalence scaled by 96.9%.

a Male smoking prevalence (ages 18 and above), original and scaled SAVM and NHIS estimates, 2013–2018. b Female smoking prevalence (ages 18 and above), original and scaled SAVM and NHIS estimates, 2013–2018
By age group, SAVM projects that male (female) prevalence for ages 18–24 fell by 33.0% (33.7%) in relative terms between 2013 and 2018 compared with 60.8% (52.6%) from NHIS over the same time period. For ages 25–44, SAVM projects a relative decline of 21.0% (17.6%) compared with 17.2% (16.6%) from NHIS. For ages 45–64, SAVM projects a relative decline of 19.9% (18.1%) compared with 15.2% (20.9%) from NHIS. For ages 65 and above, SAVM projects a relative decline of 16.6% (20.3%) compared with 6.3% (4.0%) from NHIS.
Thus, while predicting smoking prevalence well for the overall adult population, SAVM tends to under-predict relative reductions in smoking prevalence at younger ages and over-predict relative reduction at older ages. While SAVM estimates for 2018 are often outside the NHIS confidence intervals, upon scaling all years by the initial year (2013) from SAVM relative to the initial year in NHIS for comparability, the SAVM 2018 estimates are generally within the NHIS confidence intervals, with the exceptions of the 18–24 age group for males and the 65 and above age group for females.
Validation of NVP prevalence
The SAVM predictions for exclusive NVP use are validated against the overall NVP prevalence from NHIS for 2018 as shown in Table 3. For ages 18 and above, SAVM projects a 2018 NVP prevalence of 3.0% compared with 3.1% (95% CI: 2.7–3.5%) from NHIS for males, and 1.8% compared with 1.5% (95% CI: 1.3–1.8%) for females. By age group for males, the SAVM projection against NHIS (with confidence intervals) for 2018 are 7.5% vs 6.8% (95% CI:4.8–8.8%) for ages 18–24, 4.2% vs. 4.7% (95% CI: 3.8–5.6%) for ages 25-44, 1.4% vs. 1.5% (95% CI: 1.0–1.9%) for ages 45–64, and 0.5% vs. 0.6% (95% CI: 0.3–0.9%) for ages 65 and above. For females, SAVM projections vs. NHIS estimates are 4.9% vs. 3.1% (95% CI: 1.8–4.5%) for ages 18–24, 2.4% vs. 1.9% (95% CI: 1.4–2.3%) for ages 25–44, 1.0% vs. 1.3% (95% CI: 1.0–1.7%) for ages 45–64, and 0.4% vs. 0.5% (95% CI: 0.3–0.7%) for ages 65 and above. SAVM predictions fell within the 95% confidence intervals estimated from NHIS data for overall and by age groups, except for females ages 18–24 and 25-44.
Public health impact under the baseline NVP and No-NVP Scenario
Table 4 presents US smoking and NVP use prevalence, deaths, and LYLs for males and females ages 18–99 over the modeling period 2013–2060 for all existing and new birth cohorts. We focus on prevalence estimates for the year 2023 as an indication of short-term projection and for the year 2060 as an example of long-term projections. We first apply the baseline parameters: RiskNVP = 5% that of smoking, with multipliers for smoking initiation = 75%, NVP initiation = 50%, smoking cessation = 100%, NVP cessation = 100%, and with switching rates remaining constant over time.
In the No-NVP Scenario, smoking prevalence for ages 18 and above is 21.4% in 2013 declining to 17.4% in 2023, and 12.2% in 2060 for males, 15.9% in 2013 declining to 12.7% in 2023, and 8.7% in 2060 for females. Cumulative (2013–2060) SADs are 12.6 million for males and 5.0 million for females, while cumulative LYLs are 141.5 million for males and 54.1 million for females.
In the NVP Scenario, male (female) smoking prevalence declines to 12.9% (10.1%) in 2023 and then declines to 4.5% (4.1%) in 2060. Exclusive NVP users include those who initiated NVP use from never users (de novo) at all ages and those who switched to NVP use from smoking before age 35. Male (female) exclusive NVP use increases from 0% (0%) in 2013 to 3.8% (2.2%) in 2023, and to 8.8% (5.5%) in 2060. The prevalence of former smokers using NVPs (those switching from smoking to vaping after age 35) increases from 0% (0%) in 2013 to 1.5% (1.0%) in 2023, then increases to 1.6% (1.0%) in 2060. Compared with females, greater reduction in smoking and increase in NVP use in males is due to higher levels of switching to NVPs at younger ages among males. SVADs and LYLs cumulate to 11.3 million and 112.8 million during 2013–2060 for males and to 4.5 million and 43.9 million for females.
Under the NVP Scenario, approximately 1.8 million (1.3 million males, 0.5 million females) SVADs are averted, a 10.4% relative reduction compared with the No-NVP Scenario, and 38.9 million (28.7 million males, 10.1 million females) LYLs are averted, a 19.9% relative reduction.
Sensitivity to NVP transition parameters
Sensitivity analyses are shown in Table 5 for smoking-attributable and vaping-attributable deaths (SVADs) and in Table 6 for life-years lost (LYLs). While holding the NVP relative risk multiplier (RiskNVP) constant at 5% (columns 2 and 3 in both tables), we examine the individual impact of variations in transition rates on SVADs and LYLs averted relative to the initial levels in the NVP Scenario. Each of five transition multipliers was varied for (1) NVP switching, (2) smoking initiation, (3) NVP initiation, (4) smoking cessation, and (5) NVP cessation.
If the baseline NVP switching rate parameter is reduced by 50% with 0% annual decay, NVP replacement of smoking is less in the NVP Scenario. Compared with the baseline NVP Scenario, averted SVADs decline in relative terms by 39% from 1.8 million to 1.1 million; averted LYLs decline by 37% from 38.9 million to 24.6 million. A doubling of the NVP switching rates from their initial levels yields a 50% relative increase in averted SVADs to 2.8 million and a 47% relative increase in averted LYLs to 57 million. Using the initial NVP switching rates but with a 10% decay rate reduces averted SVADs by 40% to 1.1 million and reduces averted LYLs by 38% to 24.0 million. Using the initial NVP switching rates but with a 5% annual increase rate in the first five years (2018–2022) increases averted SVADs by 11.0% to 2.0 million and increases averted LYLs by 10% to 42.9 million.
Increasing the smoking initiation multiplier from its baseline level primarily increases youth and young adult use at first, leading to more SVADs and LYLs later in life. An increase from 75 to 125% reduces averted SVADs by 5% and averted LYLs by 7.6%, and a reduction from 75 to 25%, increases averted SVADs by 6% and averted LYLs by 8%. Increasing or decreasing the NVP initiation multiplier yields a smaller relative change in averted SVADs and LYLs. Increasing the NVP initiation multiplier from 50% to 75% yields a relative reduction of 0.1% in averted SVADs and of 0.1% in averted LYLs. A reduction in the NVP initiation multiplier to 25% increases averted SVADs and averted LYLs by 0.2% or less.
Compared with changes in the initiation parameters, changes in cessation multipliers lead to a more immediate impact on SVADs, since cessation generally occurs later in life when mortality risk is highest. Increasing the smoking cessation multiplier from 100% to 150% of cessation in the No-NVP Scenario yields a 59% relative increase to 2.9 million averted SVADs and a 42% relative increase to 55.3 million averted LYLs. Reducing the smoking cessation multiplier from 100 to 50% yields a 100% relative reduction to 224 averted SVADs and a 64.6% relative reduction to 13.8 million averted LYLs. Comparable change in the NVP cessation multipliers yields less change. Increasing the NVP cessation multiplier from 100 to 150%, averted SVADs increased by 1.7% and LYLs increased by 1.4%. Reducing the NVP cessation multiplier to 50%, averted SVADs and LYLs decline by 2.8% and 2.1%, respectively.
Since the NVP risk is substantially lower than the smoking risk in the above analyses, the relative changes in averted SVADs and LYLs by varying the NVP initiation or cessation multipliers are less than the relative changes by varying the smoking initiation or cessation multipliers within comparable ranges.
Sensitivity to NVP relative risks
Tables 5 and 6 also provide estimates of averted SVADs and LYLs with an NVP relative risk multiplier (RiskNVP) of 40% (columns 4 and 5) under the different NVP transition parameter ranges. With all other parameters at their baseline levels in the NVP Scenario, averted SVADs decrease in relative terms by 42% from 1.8 million with 5% NVP risks to 1.1 million with 40% NVP risks, and averted LYLs decrease by 42% from 38.9 million to 22.6 million.
By setting RiskNVP at 40%, reducing the NVP switching rates by 50% yields a 39% relative reduction in averted LYLs, while increasing the NVP switching rates by 100% (from 100 to 200%) yields a 49% relative increase. Annually reducing the switching rates by 10% yields a 41% relative reduction in averted LYLs, while annually increasing the switching rates by 5% only in the first 5 years (2018–2022) yields an 11% relative increase in averted LYLs. Reducing the smoking initiation multiplier from 75 to 25% yields a 21% relative increase in LYLs, while an increase to 125% yields a 19% relative reduction compared with baseline. Reducing the NVP initiation multiplier from 50% to 25% yields 6% additional averted LYLs, while an increase to 75% yields 6% fewer averted LYLs. Reducing the smoking cessation multiplier from 100 to 50% yields 122% fewer averted LYLs, while an increase to 150% yields 81% additional averted LYLs. Reducing the NVP cessation rate multiplier from 100 to 50% yields 28% fewer averted LYLs, while increasing to 150% yields 19% additional averted LYLs.
Tables 5 and 6 (last row) also provide the change in SVADs and LYL with RiskNVP at 40% compared with RiskNVP = 5%. In all cases, the public health benefits in terms of averted SVADs and averted LYLs are reduced, with relative reductions of at least 23% associated with the NVP initiation and cessation rates as well as the smoking initiation and cessation rates. Thus, increasing NVP risks leads to greater sensitivity of LYLs to changes in switching, NVP initiation, and NVP cessation parameters.
Discussion
The SAVM is the first simulation model incorporating vaping that was subjected to validation. SAVM projections of US smoking prevalence were generally close to estimates from 2013–2018 NHIS, except at younger ages where the relative reductions in smoking prevalence from surveys were greater than those predicted by the model. NVP use projections from SAVM were generally consistent with those of the 2018 NHIS.
While not discussed above, we also conducted validations of smoking prevalence against two other major national surveys: the Tobacco Use Supplement to the Current Population Survey (TUS-CPS) and the National Survey on Drug Use and Health (NSDUH) (See Supplement 3). The relative reductions in SAVM estimates were generally closer to 18–24-year-old estimates from these two surveys than to NHIS estimates, but they performed slightly less well overall. However, the prevalence estimates from TUS-CPS and NSDUH differ substantially from those of the NHIS both in terms of levels and trends over 2013–2018, which is consistent with previous studies [58, 81]. Thus, validation results may depend on the survey used to validate the model.
Using our baseline estimates of NVP relative mortality risks, switching rates, smoking and NVP initiation rates, and smoking and NVP cessation rates, the SAVM projects that NVP use in the population will translate to 1.8 million premature smoking-attributable and vaping-attributable deaths avoided and 38.9 million life-years gained from 2013–2060. However, these estimates are based on a specific set of parameters and should be carefully considered in the context of sensitivity analyses which show the influence of each parameter on public health outcomes. While the validation results increase confidence in the model, predictions for the future depend on the stability of its underlying transition behaviors and are subject to much greater uncertainty when considering longer time horizons.
The NVP relative risk relative to smoking was initially set to 5% [64, 75], but when increased to 40%, the associated public health gains were substantially reduced. This finding is particularly important in light of the uncertainty and controversy surrounding the relative risks of NVP use compared with smoking [25]. In addition, with the NVP relative risk at 5%, public health gains were more sensitive to the level of switching and smoking cessation rates and to a lesser extent smoking or NVP initiation rates. However, with NVP relative risks raised to 40%, public health impacts became much more sensitive to all parameters except for the NVP initiation rate.
Our analysis is subject to limitations. While our No-NVP Scenario is based on trends informed by data through 2013, future trends are subject to uncertainty and depend on tobacco control policies and other environmental changes that would have occurred if NVPs had not come onto the US market. The NVP relative risk, switching, initiation, and cessation parameters applied in the NVP Scenario are also subject to considerable uncertainty. Compared with smoking, NVPs are new products with less empirical evidence on their long-term health effects and usage/transition patterns [27, 37]. In addition, patterns of future NVP use are difficult to predict. NVP use is still relatively new and use patterns can be expected to change as a result of the “disruptive” nature of the product [1, 56]. Future NVP use will depend on product innovations and industry structure [56, 59, 60] and regulations surrounding NVP content, marketing, and use [51, 52]. In particular, NVP risks may be reduced with prudent FDA regulations that ban or limit the presence of known toxicants in e-liquids. In addition, public health benefits can be amplified with stronger policies directed at reducing smoking initiation and increasing smoking cessation.
Limitations to the model were identified in the 2013–2018 validation. In particular, the model underestimates the reduction in smoking among 18–24-year-olds observed in the NHIS, thereby overestimating future smoking prevalence. Because the No-NVP Scenario is based on age, period, and cohort effects through 2013, before NVPs became more widespread, some divergence is expected: more young adult smokers may be switching to NVP use or not initiating smoking than our model captures. Our sensitivity analyses indicated that public health impacts were particularly sensitive to the rate of switching from smoking to NVPs by 18–24-year-olds and smoking initiation in the NVP Scenario. In particular, downward trends in youth and young adult smoking have increased since 2017, when vaping devices such as JUUL became more widely used [15, 46, 63, 96]. The 2019 Monitoring the Future survey [66] indicates past 30-day smoking rates as low as 5.8% and daily smoking rates as low as 2%. Recent studies [2, 19, 58, 71, 97] also indicate that NVP use among US young adult smokers may be higher than indicated by our NVP initiation rates.
The validation of NVP use is sensitive to how regular NVP use is defined. Unlike cigarette smoking where regular use is generally defined in terms of having smoked at least 100 cigarettes during one’s lifetime, there is no accepted measure of regular NVP use. While we defined regular use by 10+ days in the last month, we also considered 1+ day and 20+ days measures based on PATH in 2013–2017. The 20+ days measure yielded levels similar to our 10+ days measure of NVP use, while the 1+ day measure yielded much higher estimates. Still, there is currently considerable uncertainty about NVP initiation, especially regarding initiation into more regular use [40, 67,68,69]. Although youth NVP rates increased substantially in 2019 [31, 100], they fell in 2020 [31], highlighting the challenges inherent in predicting future NVP use, even in the short-term. Nevertheless, like earlier simulation results [14, 73, 103], public health impacts were found to be relatively insensitive to the NVP initiation parameter.
Our NVP cessation multiplier baseline value of 100% implies that cessation from both smoking and NVPs is at the identical rate that of smoking cessation in the No-NVP Scenario. This transition implicitly includes cessation from both smoking and vaping. While this complete cessation from smoking may increase with the availability of NVPs, some smokers may instead switch to NVPs. In our model, the public health impact regarding smoking depends on the number who quit smoking through both complete cessation and switching in the NVP Scenario compares to the number of smokers who would otherwise quit in the absence of NVPs (the No-NVP Scenario). In addition, some recent evidence indicates that NVPs may be less addictive than smoking [7, 61, 62, 72, 87], implying a value greater than 100% and that those smokers switching to vaping may be more likely to quit vaping in future years than smokers in the No-NVP Scenario.
The NVP Scenario in SAVM applies simplifying assumptions so that the model is user-friendly. A never smoker who experiments with NVPs and does not transition to smoking is considered a non-user. Because transitions to and from dual use are often particularly unstable [4, 8, 18, 78], we have chosen not to distinguish dual from exclusive cigarette use in the NVP Scenario. In addition, consistent with previous CISNET models [43,44,45], SAVM does not consider relapse, with transitions to former smokers or former NVP users treated as permanent. Except for the switching parameter, we have assumed that the NVP relative risk and other transition parameters are age and time invariant to simplify the analysis. However, other key parameters, such as the smoking cessation and initiation parameters could shift over time. Intertemporal and age patterns will depend on technological advances in NVPs and regulatory policies. It will be important to update key parameters to reflect new evidence as it becomes available.
Finally, although other categories of nicotine delivery products are available on the market, including cigars, smokeless tobacco, and heated tobacco products [21], we only consider two categories of products, cigarettes, and NVPs, to keep the model tractable. As a substitute for NVPs, heated tobacco products in particular may affect NVP as well as cigarette use.
While subject to limitations, the SAVM model can be easily modified. The model is developed in Excel both for transparency and to ensure its accessibility to non-technical audiences. More experienced users can modify the model’s underlying assumptions and structure as described in the SAVM User Guide, thereby providing the user flexibility. The model and an accompanying user guide are available at https://tcors.umich.edu/Resources_Download.php?FileType=SAV_Model.
The SAVM can also be easily applied to other contexts and policy scenarios. The requisite data on smoking prevalence and population by age and gender are generally available by state and for most countries. Further, the model can be used to consider the impact of different policies by comparing the NVP Scenario under current conditions to a scenario with user-specified policy parameters. However, the results will depend on the user’s knowledge of the impact of the policy both on cigarette and NVP use and any age- or cohort-related variations in these parameters, so that sensitivity analysis is strongly encouraged.
In conclusion, the SAVM was developed as a user-friendly tool to examine the potential public health impact of NVP use on smoking behaviors and to show how public health outcomes vary across different assumptions related to NVP health risks and the initiation and cessation of NVP use and smoking. Using readily available data, SAVM can be applied by policymakers, researchers, and other stakeholders in other countries to help understand the role of NVPs vis-à-vis smoking and the impact that those products have on public health.
Availability of data and materials
The model, data used therein, and a 100-page user manual will be made available to all requestors, and we have made the model available on our (University of Michigan) FDA Tobacco Center of Regulatory Science (TCORS) website at https://tcors.umich.edu/Resources_Download.php?FileType=SAV_Model.
Abbreviations
- NVP:
-
Nicotine vaping product
- SAVM:
-
Smoking and Vaping Model
- SADs:
-
Smoking-attributable deaths
- LYLs:
-
Life years lost
References
Abrams DB. Promise and peril of e-cigarettes: can disruptive technology make cigarettes obsolete? JAMA. 2014;311(2):135–6. https://doi.org/10.1001/jama.2013.285347.
Al Rifai M, Merchant AT, Nambi V, Jia X, Gulati M, Valero-Elizondo J, et al. Temporal trends in e-cigarette use among U.S. adults: behavioral risk factor surveillance system, 2016 to 2018. Am J Med. 2020;133(9):e508–11. https://doi.org/10.1016/j.amjmed.2019.12.020.
Amato MS, Boyle RG, Levy D. How to define e-cigarette prevalence? Finding clues in the use frequency distribution. Tob Control. 2016;25(e1):e24–9. https://doi.org/10.1136/tobaccocontrol-2015-052236.
Azagba S, Shan L, Latham K. Adolescent dual use classification and its association with nicotine dependence and quit intentions. J Adolesc Health. 2019;65(2):195–201. https://doi.org/10.1016/j.jadohealth.2019.04.009.
Azagba S, Qeadan F, Shan L, Latham K, Wolfson M. E-cigarette use and transition in adult smoking frequency: a longitudinal study. Am J Prev Med. 2020;59(3):367–76. https://doi.org/10.1016/j.amepre.2020.02.024.
Bachand AM, Sulsky SI, Curtin GM. Assessing the likelihood and magnitude of a population health benefit following the market introduction of a modified-risk tobacco product: enhancements to the dynamic population modeler, Dpm(+1). Risk Anal. 2018;38(1):151–62. https://doi.org/10.1111/risa.12819.
Bold KW, Sussman S, O'Malley SS, Grana R, Foulds J, Fishbein H, et al. Measuring e-cigarette dependence: initial guidance. Addict Behav. 2018;79:213–8. https://doi.org/10.1016/j.addbeh.2017.11.015.
Borland R, Murray K, Gravely S, Fong GT, Thompson ME, McNeill A, et al. A new classification system for describing concurrent use of nicotine vaping products alongside cigarettes (so-called ʻdual useʼ): findings from the Itc-4 Country Smoking and Vaping Wave 1 Survey. Addiction. 2019;114(S1):24–34. https://doi.org/10.1111/add.14570.
Bullen C, Howe C, Laugesen M, McRobbie H, Parag V, Williman J, et al. Electronic cigarettes for smoking cessation: a randomised controlled trial. Lancet. 2013;382(9905):1629–37. https://doi.org/10.1016/S0140-6736(13)61842-5.
Caraballo RS, Shafer PR, Patel D, Davis KC, McAfee TA. Quit methods used by US adult cigarette smokers, 2014-2016. Prev Chronic Dis. 2017;14:E32. https://doi.org/10.5888/pcd14.160600.
Carter BD, Abnet CC, Feskanich D, Freedman ND, Hartge P, Lewis CE, et al. Smoking and mortality--beyond established causes. N Engl J Med. 2015;372(7):631–40. https://doi.org/10.1056/NEJMsa1407211.
Centers for Disease Control and Prevention. 2019a, "US population and mortality data". Retrieved November 1, 2019.
Centers for Disease Control and Prevention. National health interview survey, vol. 2019; 2019b.
Cherng ST, Tam J, Christine PJ, Meza R. Modeling the effects of e-cigarettes on smoking behavior: implications for future adult smoking prevalence. Epidemiology. 2016;27(6):819–26. https://doi.org/10.1097/EDE.0000000000000497.
Chu KH, Colditz JB, Primack BA, Shensa A, Allem JP, Miller E, et al. Juul: spreading online and offline. J Adolesc Health. 2018;63(5):582–6. https://doi.org/10.1016/j.jadohealth.2018.08.002.
CISNET. 2016, "Smoking Histories". Retrieved December 20, 2019 (https://resources.cisnet.cancer.gov/projects/).
Cobb CO, Villanti AC, Graham AL, Pearson JL, Glasser AM, Rath JM, et al. Markov modeling to estimate the population impact of emerging tobacco products: a proof-of-concept study. Tob Regul Sci. 2015;1(2):129–41. https://doi.org/10.18001/TRS.1.2.3.
Coleman B, Rostron B, Johnson SE, Persoskie A, Pearson J, Stanton C, et al. Transitions in electronic cigarette use among adults in the Population Assessment of Tobacco and Health (PATH) Study, Waves 1 and 2 (2013-2015). Tob Control. 2018. https://doi.org/10.1136/tobaccocontrol-2017-054174.
Creamer MR, Wang TW, Babb S, Cullen KA, Day H, Willis G, et al. Tobacco product use and cessation indicators among adults - United States, 2018. MMWR Morb Mortal Wkly Rep. 2019;68(45):1013–9. https://doi.org/10.15585/mmwr.mm6845a2.
Cullen KA, Gentzke AS, Sawdey MD, Chang JT, Anic GM, Wang TW, et al. E-cigarette use among youth in the United States, 2019. JAMA. 2019;322(21):2095. https://doi.org/10.1001/jama.2019.18387.
Czoli CD, White CM, Reid JL, O’Connor RJ, Hammond D. Awareness and interest in iqos heated tobacco products among youth in Canada, England and the USA. Tob Control. 2020;29(1):89–95. https://doi.org/10.1136/tobaccocontrol-2018-054654.
Dai H, Leventhal AM. Association of electronic cigarette vaping and subsequent smoking relapse among former smokers. Drug Alcohol Depend. 2019;199:10–7. https://doi.org/10.1016/j.drugalcdep.2019.01.043.
de Groot PM, Wu CC, Carter BW, Munden RF. The epidemiology of lung cancer. Transl Lung Cancer Res. 2018;7(3):220–33. https://doi.org/10.21037/tlcr.2018.05.06.
DeVito EE, Krishnan-Sarin S. E-cigarettes: impact of e-liquid components and device characteristics on nicotine exposure. Curr Neuropharmacol. 2018;16(4):438–59. https://doi.org/10.2174/1570159X15666171016164430.
Eissenberg T, Bhatnagar A, Chapman S, Jordt SE, Shihadeh A, Soule EK. Invalidity of an oft-cited estimate of the relative harms of electronic cigarettes. Am J Public Health. 2020;110(2):161–2. https://doi.org/10.2105/AJPH.2019.305424.
Etter JF. Throat hit in users of the electronic cigarette: an exploratory study. Psychol Addict Behav. 2016;30(1):93–100. https://doi.org/10.1037/adb0000137.
Fairchild AL, Bayer R, Lee JS. The e-cigarette debate: what counts as evidence? Am J Public Health. 2019;109(7):1000–6. https://doi.org/10.2105/AJPH.2019.305107.
Farsalinos KE, Spyrou A, Tsimopoulou K, Stefopoulos C, Romagna G, Voudris V. Nicotine absorption from electronic cigarette use: comparison between first and new-generation devices. Sci Rep. 2014;4(1):4133. https://doi.org/10.1038/srep04133.
Federal Register, 2014, " Deeming tobacco products to be subject to the Federal Food, Drug, and Cosmetic Act, as Amended by the Family Smoking Prevention and Tobacco Control Act; regulations on the sale and distribution of tobacco products and required warning statements for tobacco products". (https://www.federalregister.gov/articles/2014/04/25/2014-09491/deeming-tobacco-products-to-be-subject-to-the-federal-food-drug-and-cosmetic-act-as-amended-by-the#h-39).
Filippidis FT, Laverty AA, Gerovasili V, Vardavas CI. Two-Year trends and predictors of e-cigarette use in 27 European Union member states. Tob Control. 2017;26(1):98–104. https://doi.org/10.1136/tobaccocontrol-2015-052771.
Gentzke AS, Wang TW, Jamal A, Park-Lee E, Ren C, Cullen KA, et al. Tobacco product use among middle and high school students - United States, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(50):1881–8. https://doi.org/10.15585/mmwr.mm6950a1.
Giovenco DP, Delnevo CD. Prevalence of population smoking cessation by electronic cigarette use status in a national sample of recent smokers. Addict Behav. 2018;76:129–34. https://doi.org/10.1016/j.addbeh.2017.08.002.
Glasser AM, Collins L, Pearson JL, Abudayyeh H, Niaura RS, Abrams DB, et al. Overview of electronic nicotine delivery systems: a systematic review. Am J Prev Med. 2016;52(2):e33–66. https://doi.org/10.1016/j.amepre.2016.10.036.
Goldenson NI, Kirkpatrick MG, Barrington-Trimis JL, Pang RD, McBeth JF, Pentz MA, et al. Effects of sweet flavorings and nicotine on the appeal and sensory properties of e-cigarettes among young adult vapers: application of a novel methodology. Drug Alcohol Depend. 2016;168:176–80. https://doi.org/10.1016/j.drugalcdep.2016.09.014.
Goniewicz ML, Knysak J, Gawron M, Kosmider L, Sobczak A, Kurek J, et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob Control. 2014;23(2):133–9. https://doi.org/10.1136/tobaccocontrol-2012-050859.
Goniewicz ML, Gawron M, Smith DM, Peng M, Jacob P 3rd, Benowitz NL. Exposure to nicotine and selected toxicants in cigarette smokers who switched to electronic cigarettes: a longitudinal within-subjects observational study. Nicotine Tob Res. 2017;19(2):160–7. https://doi.org/10.1093/ntr/ntw160.
Green SH, Bayer R, Fairchild AL. Evidence, policy, and e-cigarettes. N Engl J Med. 2016;375(5):e6. https://doi.org/10.1056/NEJMc1606395.
Hajek P, Przulj D, Phillips-Waller A, Anderson R, McRobbie H. Initial ratings of different types of e-cigarettes and relationships between product appeal and nicotine delivery. Psychopharmacology. 2018;235(4):1083–92. https://doi.org/10.1007/s00213-017-4826-z.
Hajek P, Phillips-Waller A, Przulj D, Pesola F, Myers Smith K, Bisal N, et al. A randomized trial of e-cigarettes versus nicotine-replacement therapy. N Engl J Med. 2019;380(7):629–37. https://doi.org/10.1056/NEJMoa1808779.
Hammond D, Reid JL, Rynard VL, Fong GT, Cummings KM, McNeill A, et al. Prevalence of vaping and smoking among Adolescents in Canada, England, and the United States: repeat national cross sectional surveys. BMJ. 2019;365:l2219. https://doi.org/10.1136/bmj.l2219.
Hecht SS, Carmella SG, Kotandeniya D, Pillsbury ME, Chen M, Ransom BW, et al. Evaluation of toxicant and carcinogen metabolites in the urine of e-cigarette users versus cigarette smokers. Nicotine Tob Res. 2014;17(6):704–9. https://doi.org/10.1093/ntr/ntu218.
Hill A, Camacho OM. A System dynamics modelling approach to assess the impact of launching a new nicotine product on population health outcomes. Regul Toxicol Pharmacol. 2017;86:265–78. https://doi.org/10.1016/j.yrtph.2017.03.012.
Holford TR, Levy DT, McKay LA, Clarke L, Racine B, Meza R, et al. Patterns of Birth Cohort-Specific Smoking Histories, 1965-2009. Am J Prev Med. 2014a;46(2):e31–7. https://doi.org/10.1016/j.amepre.2013.10.022.
Holford TR, Meza R, Warner KE, Meernik C, Jeon J, Moolgavkar SH, et al. Tobacco control and the reduction in smoking-related premature deaths in the United States, 1964-2012. JAMA. 2014b;311(2):164–71. https://doi.org/10.1001/jama.2013.285112.
Holford TR, Levy DT, Meza R. Comparison of smoking history patterns among African American and White cohorts in the United States born 1890 to 1990. Nicotine Tob Res. 2016;18(Suppl 1):S16–29. https://doi.org/10.1093/ntr/ntv274.
Jackler RK, Ramamurthi D. Nicotine Arms Race: Juul and the high-nicotine product market. Tob Control. 2019;28(6):623–8. https://doi.org/10.1136/tobaccocontrol-2018-054796.
Jeon J, Holford TR, Levy DT, Feuer EJ, Cao P, Tam J, et al. Smoking and lung cancer mortality in the United States from 2015 to 2065: a comparative modeling approach. Ann Intern Med. 2018;169(10):684–93. https://doi.org/10.7326/M18-1250.
Jha P, Ramasundarahettige C, Landsman V, Rostron B, Thun M, Anderson RN, et al. 21st-century hazards of smoking and benefits of cessation in the United States. N Engl J Med. 2013;368(4):341–50. https://doi.org/10.1056/NEJMsa1211128.
Kalkhoran S, Glantz SA. Modeling the health effects of expanding e-cigarette sales in the United States and United Kingdom: a Monte Carlo analysis. JAMA Intern Med. 2015;175(10):1671–80. https://doi.org/10.1001/jamainternmed.2015.4209.
Levy DT, Meza R, Zhang Y, Holford TR. Gauging the effect of U.S. Tobacco control policies from 1965 through 2014 using Simsmoke. Am J Prev Med. 2016;50(4):535–42. https://doi.org/10.1016/j.amepre.2015.10.001.
Levy DT, Cummings KM, Villanti AC, Niaura R, Abrams DB, Fong GT, et al. A framework for evaluating the public health impact of e-cigarettes and other vaporized nicotine products. Addiction. 2017a;112(1):8–17. https://doi.org/10.1111/add.13394.
Levy DT, Yuan Z, Li Y. The prevalence and characteristics of e-cigarette users in the U.S. Int J Environ Res Public Health. 2017b;14(10). https://doi.org/10.3390/ijerph14101200.
Levy DT, Borland R, Lindblom EN, Goniewicz ML, Meza R, Holford TR, et al. Potential deaths averted in USA by replacing cigarettes with e-cigarettes. Tob Control. 2018a;27(1):18–25. https://doi.org/10.1136/tobaccocontrol-2017-053759.
Levy DT, Tam J, Kuo C, Fong GT, Chaloupka F. The Impact of implementing tobacco control policies: the 2017 Tobacco Control Policy Scorecard. J Public Health Manag Pract. 2018b;24(5):448–57. https://doi.org/10.1097/PHH.0000000000000780.
Levy DT, Yuan Z, Luo Y, Abrams DB. The Relationship of e-cigarette use to cigarette quit attempts and cessation: insights from a large, nationally representative U.S. survey. Nicotine Tob Res. 2018c;20(8):931–9. https://doi.org/10.1093/ntr/ntx166.
Levy DT, Lindblom EN, Sweanor DT, Chaloupka F, OʼConnor RJ, Shang C, et al. An Economic analysis of the pre-deeming US market for nicotine vaping products. Tob Regul Sci. 2019a;5(2):169–81. https://doi.org/10.18001/trs.5.2.8.
Levy DT, Warner KE, Cummings KM, Hammond D, Kuo C, Fong GT, et al. Examining the relationship of vaping to smoking initiation among us youth and young adults: a reality check. Tob Control. 2019b;28(6):629–35. https://doi.org/10.1136/tobaccocontrol-2018-054446.
Levy DT, Yuan Z, Li Y, Mays D, Sanchez-Romero LM. An Examination of the variation in estimates of e-cigarette prevalence among U.S. adults. Int J Environ Res Public Health. 2019c;16(17). https://doi.org/10.3390/ijerph16173164.
Levy, D. T., C. E. Douglas, L. M. Sanchez-Romero, K. M. Cummings and D. T. Sweanor. 2020a. "An analysis of the FTCʼS attempt to stop the Altria-Juul Labs deal." Tob Regul Sci 6(4):302-05. doi: 10.18001/TRS.6.4.7.
Levy DT, Sweanor D, Sanchez-Romero LM, OʼConnor R, Goniewicz ML, Borland R. Altria-Juul Labs deal: why did it occur and what does it mean for the US nicotine delivery product market. Tob Control. 2020b;29(e1):e171–e74. https://doi.org/10.1136/tobaccocontrol-2019-055081.
Liu G, Wasserman E, Kong L, Foulds J. A comparison of nicotine dependence among exclusive e-cigarette and cigarette users in the PATH study. Prev Med. 2017;104:86–91. https://doi.org/10.1016/j.ypmed.2017.04.001.
Martinez U, Martinez-Loredo V, Simmons VN, Meltzer LR, Drobes DJ, Brandon KO, et al. How does smoking and nicotine dependence change after onset of vaping? A Retrospective Analysis of Dual Users. Nicotine Tob Res. 2019;22(5):764–70. https://doi.org/10.1093/ntr/ntz043.
McKeganey N, Russell C. Prevalence of awareness and use of Juul e-cigarettes in a national probability sample of adolescents in the United States. Am J Health Behav. 2019;43(3):591–605. https://doi.org/10.5993/AJHB.43.3.13.
McNeill A, Brose LS, Calder R, Bauld L, and Robson D. Vaping in England: an evidence update including mental health and pregnancy, March 2020: a report commissioned by Public Health England. London: Public Health England. Retrieved April 3, 2020; 2020. (https://www.gov.uk/government/publications/vaping-in-england-evidence-update-march-2020/vaping-in-england-2020-evidence-updatesummary).
Mendez D, Warner KE. A magic bullet? The potential impact of e-cigarettes on the toll of cigarette smoking. Nicotine Tob Res. 2020;23(4):654–61. https://doi.org/10.1093/ntr/ntaa160.
Meza R, Jimenez-Mendoza E, Levy DT. Trends in tobacco use among adolescents by grade, sex, and race, 1991-2019. JAMA Netw Open. 2020;3(12):e2027465. https://doi.org/10.1001/jamanetworkopen.2020.27465.
Miech R, Johnston LD, OʼMalley PM, Terry-McElrath YM. The national prevalence of adolescent nicotine use in 2017: estimates taking into account student reports of substances vaped. Addict Behav Rep. 2019a;9:100159. https://doi.org/10.1016/j.abrep.2019.100159.
Miech R, Johnston L, OʼMalley PM, Bachman JG, Patrick ME. Trends in adolescent vaping, 2017-2019. N Engl J Med. 2019b;381(15):1490–1. https://doi.org/10.1056/NEJMc1910739.
Miech R, Johnston L, OʼMalley PM, Bachman JG, Patrick ME. Adolescent vaping and nicotine use in 2017-2018 - U.S. National Estimates. N Engl J Med. 2019c;380(2):192–3. https://doi.org/10.1056/NEJMc1814130.
Miller CR, Smith DM, Goniewicz ML. Changes in nicotine product use among dual users of tobacco and electronic cigarettes: findings from the Population Assessment of Tobacco and Health (PATH) Study, 2013-2015. Subst Use Misuse. 2020;55(6):909–13. https://doi.org/10.1080/10826084.2019.1710211.
Mirbolouk M, Charkhchi P, Kianoush S, Uddin SMI, Orimoloye OA, Jaber R, et al. Prevalence and distribution of e-cigarette use among U.S. adults: behavioral risk factor surveillance system, 2016. Ann Intern Med. 2018;169(7):429–38. https://doi.org/10.7326/M17-3440.
Morean M, Krishnan-Sarin S, OʼMalley SS. Comparing cigarette and e-cigarette dependence and predicting frequency of smoking and e-cigarette use in dual-users of cigarettes and e-cigarettes. Addict Behav. 2018;87:92–6. https://doi.org/10.1016/j.addbeh.2018.06.027.
National Academy of Sciences, Engineering and Medicine. 2018. Public Health Consequences of E-CigarettesCongress.
Nelluri B, Murphy K, Mookadam F, Mookadam M. The current literature regarding the cardiovascular effects of electronic cigarettes. Futur Cardiol. 2016;12(2):167–79. https://doi.org/10.2217/fca.15.83.
Nutt DJ, Phillips LD, Balfour D, Curran HV, Dockrell M, Foulds J, et al. E-cigarettes are less harmful than smoking. Lancet. 2016;387(10024):1160–2. https://doi.org/10.1016/S0140-6736(15)00253-6.
Poland B, Teischinger F. Population Modeling of modified risk tobacco products accounting for smoking reduction and gradual transitions of relative risk. Nicotine Tob Res. 2017;19(11):1277–83. https://doi.org/10.1093/ntr/ntx070.
Ratajczak A, Feleszko W, Smith DM, Goniewicz M. How Close are we to definitively identifying the respiratory health effects of e-cigarettes? Expert Rev Respir Med. 2018;12(7):549–56. https://doi.org/10.1080/17476348.2018.1483724.
Robertson L, Hoek J, Blank ML, Richards R, Ling P, Popova L. Dual use of electronic nicotine delivery systems (ENDS) and smoked tobacco: a qualitative analysis. Tob Control. 2019;28(1):13–9. https://doi.org/10.1136/tobaccocontrol-2017-054070.
Rosenberg MA, Feuer EJ, Yu B, Sun J, Henley SJ, Shanks TG, et al. Chapter 3: Cohort life tables by smoking status, removing lung cancer as a cause of death. Risk Anal. 2012;32(Suppl 1):S25–38. https://doi.org/10.1111/j.1539-6924.2011.01662.x.
Royal College of Physicians. Nicotine without smoke: tobacco harm reduction. London: RCP; 2016.
Ryan H, Trosclair A, Gfroerer J. Adult Current smoking: differences in definitions and prevalence estimates--Nhis and Nsduh, 2008. J Environ Public Health. 2012;2012:918368–11. https://doi.org/10.1155/2012/918368.
Shahab L, Goniewicz ML, Blount BC, Brown J, McNeill A, Alwis KU, et al. Nicotine, carcinogen, and toxin exposure in long-term e-cigarette and nicotine replacement therapy users: a cross-sectional study. Ann Intern Med. 2017a;166(6):390–400. https://doi.org/10.7326/M16-1107.
Shahab L, Goniewicz ML, Blount BC, Brown J, West R. E-cigarettes and toxin exposure. Ann Intern Med. 2017b;167(7):525–6. https://doi.org/10.7326/L17-0315.
Soneji S, Barrington-Trimis JL, Wills TA, Leventhal AM, Unger JB, Gibson LA, et al. Association between Initial use of e-cigarettes and subsequent cigarette smoking among adolescents and young adults: a systematic review and meta-analysis. JAMA Pediatr. 2017;171(8):788–97. https://doi.org/10.1001/jamapediatrics.2017.1488.
Soneji SS, Sung HY, Primack BA, Pierce JP, Sargent JD. Quantifying population-level health benefits and harms of e-cigarette use in the United States. PLoS One. 2018;13(3):e0193328. https://doi.org/10.1371/journal.pone.0193328.
Stanton CA, Sharma E, Edwards KC, Halenar MJ, Taylor KA, Kasza KA, et al. Longitudinal transitions of exclusive and polytobacco electronic nicotine delivery systems (ENDS) use among youth, young adults and adults in the USA: findings from the path study waves 1-3 (2013-2016). Tob Control. 2020;29(Suppl 3):s147–s54. https://doi.org/10.1136/tobaccocontrol-2019-055574.
Strong DR, Pearson J, Ehlke S, Kirchner T, Abrams D, Taylor K, et al. Indicators of dependence for different types of tobacco product users: descriptive findings from wave 1 (2013-2014) of the Population Assessment of Tobacco and Health (PATH) Study. Drug Alcohol Depend. 2017;178:257–66. https://doi.org/10.1016/j.drugalcdep.2017.05.010.
Tam J, Levy DT, Jeon J, Clarke J, Gilkeson S, Hall T, et al. Projecting the effects of tobacco control policies in the USA through microsimulation: a study protocol. BMJ Open. 2018;8(3):e019169. https://doi.org/10.1136/bmjopen-2017-019169.
Taylor KA, Sharma E, Edwards KC, Halenar MJ, Kissin W, Kasza KA, et al. Longitudinal pathways of exclusive and polytobacco cigarette use among youth, young adults and adults in the USA: findings from the path study waves 1-3 (2013-2016). Tob Control. 2020;29(Suppl 3):s139–s46. https://doi.org/10.1136/tobaccocontrol-2020-055630.
Tegin G, Mekala HM, Sarai SK, Lippmann S. E-Cigarette Toxicity? South Med J. 2018;111(1):35–8. https://doi.org/10.14423/SMJ.0000000000000749.
Thun MJ, Lopez AD, Hartge P. Smoking-related mortality in the United States. N Engl J Med. 2013;368(18):1753–4. https://doi.org/10.1056/NEJMc1302783.
U.S. Department of Health and Human Services. The health consequences of smoking—50 years of progress: a report of the Surgeon General. Atlanta: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014.
U.S. Food and Drug Administration, Center for Tobacco Products. 2020, "Rules and Regulations". Retrieved May 22, 2020 (https://www.fda.gov/tobacco-products/rules-regulations-and-guidance/rules-and-regulations).
U.S. Food and Drug Administration, Center for Tobacco Products, National Institutes of Health and National Institute on Drug Abuse. Population Assessment of Tobacco and Health (PATH) Study. Washington: Food and Drug Administration (https://pathstudyinfo.gov); 2019.
Unger M, Unger DW. E-Cigarettes/Electronic Nicotine Delivery Systems: A Word of Caution on Health and New Product Development. J Thorac Dis. 2018;10(Suppl 22):S2588–S92. https://doi.org/10.21037/jtd.2018.07.99.
Vallone DM, Bennett M, Xiao H, Pitzer L, Hair EC. Prevalence and correlates of Juul use among a national sample of youth and young adults. Tob Control. 2018;28(6):603–9. https://doi.org/10.1136/tobaccocontrol-2018-054693.
Vallone DM, Cuccia AF, Briggs J, Xiao H, Schillo BA, Hair EC. Electronic cigarette and Juul use among adolescents and young adults. JAMA Pediatr. 2020;174(3):277–86. https://doi.org/10.1001/jamapediatrics.2019.5436.
Voos N, Kaiser L, Mahoney MC, Bradizza CM, Kozlowski LT, Benowitz NL, et al. Randomized within-subject trial to evaluate smokersʼ initial perceptions, subjective effects and nicotine delivery across six vaporized nicotine products. Addiction. 2019;114(7):1236–48. https://doi.org/10.1111/add.14602.
Wagener TL, Floyd EL, Stepanov I, Driskill LM, Frank SG, Meier E, et al. Have combustible cigarettes met their match? The nicotine delivery profiles and harmful constituent exposures of second-generation and third-generation electronic cigarette users. Tob Control. 2016;26(e1):e23–8. https://doi.org/10.1136/tobaccocontrol-2016-053041.
Wang TW, Gentzke AS, Creamer MR, Cullen KA, Holder-Hayes E, Sawdey MD, et al. Tobacco product use and associated factors among middle and high school students - United States, 2019. MMWR Surveill Summ. 2019;68(12):1–22. https://doi.org/10.15585/mmwr.ss6812a1.
Warner KE. Tobacco control policies and their impacts. past, present, and future. Ann Am Thorac Soc. 2014;11(2):227–30. https://doi.org/10.1513/AnnalsATS.201307-244PS.
Warner KE, Sexton DW, Gillespie BW, Levy DT, Chaloupka FJ. Impact of tobacco control on adult per capita cigarette consumption in the United States. Am J Public Health. 2014;104(1):83–9. https://doi.org/10.2105/AJPH.2013.301591.
Warner KE, Mendez D. E-cigarettes: comparing the possible risks of increasing smoking initiation with the potential benefits of increasing smoking cessation. Nicotine Tob Res. 2019;21(1):41–7. https://doi.org/10.1093/ntr/nty062.
Watkins SL, Glantz SA, Chaffee BW. Association of noncigarette tobacco product use with future cigarette smoking among youth in the Population Assessment Of Tobacco And Health (PATH) study, 2013-2015. JAMA Pediatr. 2018;172(2):181–7. https://doi.org/10.1001/jamapediatrics.2017.4173.
Weitkunat R, Lee PN, Baker G, Sponsiello-Wang Z, Gonzalez-Zuloeta Ladd AM, Ludicke F. A novel approach to assess the population health impact of introducing a modified risk tobacco product. Regul Toxicol Pharmacol. 2015;72(1):87–93. https://doi.org/10.1016/j.yrtph.2015.03.011.
Yingst JM, Foulds J, Veldheer S, Hrabovsky S, Trushin N, Eissenberg TT, et al. Nicotine Absorption during electronic cigarette use among regular users. PLoS One. 2019;14(7):e0220300. https://doi.org/10.1371/journal.pone.0220300.
Zhu SH, Zhuang YL, Wong S, Cummins SE, Tedeschi GJ. E-cigarette use and associated changes in population smoking cessation: evidence from US current population surveys. BMJ. 2017;358:j3262. https://doi.org/10.1136/bmj.j3262.
Acknowledgements
We would like to thank Ted Holford for comments on an earlier draft of the paper.
Funding
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health (NIH) and FDA Center for Tobacco Products (CTP) under award number U54CA229974. Support was also received for Dr. Levy from the National Cancer Institute under award number P01CA200512. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the Food and Drug Administration.
Author information
Authors and Affiliations
Contributions
DTL wrote the original draft. ZY and YL did the initial modeling and helped write the original methods section. All authors contributed to the development of the model and have contributed to the writing of the paper. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All original data are publicly available.
Consent for publication
All authors have approved the manuscript for submission.
Competing interests
We have no conflicts of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplement 1.
Mathematical formulation of the SAVM model. Supplement 2. Estimation of the Switch Rate from Cigarette to NVP Use. Supplement 3. Further validation of the model.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Levy, D.T., Tam, J., Sanchez-Romero, L.M. et al. Public health implications of vaping in the USA: the smoking and vaping simulation model. Popul Health Metrics 19, 19 (2021). https://doi.org/10.1186/s12963-021-00250-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12963-021-00250-7