
Abstract
Objectives
To assess the amount spent on health and care workforce (HCW) remuneration in the African countries, its importance as a proportion of country expenditure on health, and government involvement as a funding source.
Methods
Calculations are based on country-produced disaggregated health accounts data from 33 low- and middle-income African countries, disaggregated wherever possible by income and subregional economic group.
Results
Per capita expenditure HCW remuneration averaged US$ 38, or 29% of country health expenditure, mainly coming from domestic public sources (three-fifths). Comparable were the contributions from domestic private sources and external aid, measured at around one-fifth each—23% and 17%, respectively. Spending on HCW remuneration was uneven across the 33 countries, spanning from US$ 3 per capita in Burundi to US$ 295 in South Africa. West African countries, particularly members of the West African Economic and Monetary Union (WAEMU), were lower spenders than countries in the Southern African Development Community (SADC), both in terms of the share of country health expenditure and in terms of government efforts/participation. By income group, HCW remuneration accounted for a quarter of country health expenditure in low-income countries, compared to a third in middle-income countries. Furthermore, an average 55% of government health expenditure is spent on HCW remuneration, across all countries. It was not possible to assess the impact of fragile and vulnerable countries, nor could we draw statistics by type of health occupation.
Conclusions
The results clearly show that the remuneration of the health and care workforce is an important part of government health spending, with half (55%) of government health spending on average devoted to it. Comparing HCW expenditure components allows for identifying stable sources, volatile sources, and their effects on HCW investments over time. Such stocktaking is important, so that countries, WHO, and other relevant agencies can inform necessary policy changes.
Résumé
Objectifs
Évaluer le montant dépensé pour la rémunération du personnel de santé et de soins dans les pays africains, son importance en tant que proportion de la dépense de santé des pays, et déterminer la contribution des sources de financement, en particulier du gouvernement.
Méthodes
Les calculs sont effectués à partir de données désagrégées des comptes de la santé produites par 33 pays africains à revenu faible et intermédiaire classés par groupe économique sous-régional lorsque possible.
Résultats
La rémunération du personnel de santé et de soins s'élevait en moyenne à 38 dollars par habitant, soit 29% de la dépense de santé des pays, et provenait principalement de sources publiques domestiques—à hauteur des trois-cinquièmes. La participation des sources privées domestiques et de l'aide extérieure était à peu près comparable—estimée à un-cinquième chacune, 23% et 17%, respectivement. Les dépenses consacrées à la rémunération du personnel de santé et de soins étaient inégales dans les 33 pays, allant de 3 dollars par habitant au Burundi à 295 dollars en Afrique du Sud. En fait, les pays d’Afrique de l’Ouest, et plus particulièrement ceux de l’Union économique et monétaire ouest africaine (UEMOA), ont dépensé moins que les pays de la Communauté de développement de l'Afrique australe (SADC), tant en termes de part de la dépense de santé des pays qu’en termes d’efforts/de la participation du gouvernement. Par groupe de revenu, la rémunération du personnel de santé et de soins représentait un quart de la dépense de santé des pays à faible revenu, contre un tiers de celles des pays à revenu intermédiaire. En outre, 55% en moyenne des dépenses publiques de santé, tous pays confondus, sont consacrées à la rémunération du personnel de santé et de soins. Il n'a pas été possible d'évaluer l'impact des pays fragiles et vulnérables, ni de dégager des tendances par type de personnel de santé.
Conclusions
Les résultats montrent clairement que la rémunération du personnel du santé et de soins représente une part importante des dépenses publiques de santé; la moitié en moyenne (55%), dans ce groupe de 33 pays africains à revenu faible et intermédiaire. La comparaison des différentes composantes de la dépense permettra au fil du temps d’identifier les sources stables, les sources volatiles et leurs effets éventuels sur les investissements. Ce type de données est important pour que les pays, l'OMS et les autres institutions intéressées, puissent apporter leur contribution aux réformes politiques qui pourraient s’avérer nécessaires.
Mots clés
Comptes de la santé, personnel de santé et de soins, rémunération, Afrique, UEMOA, CEDEAO, CEEAC, SADC, dépenses publiques de santé.
Similar content being viewed by others


Background
A health and care workforce (HCW) of adequate size and competence is critical to achieving the United Nations health-related Sustainable Development Goals (SDG3), Universal Health Coverage (UHC), and health security [1]. Yet globally, most countries face multiple challenges—shortages, suboptimal education and training, deployment, performance, productivity, working conditions, and retention—which, exacerbated by limited investment in health workforce education, affect the availability, accessibility, quality, and performance of national health systems and services, preventing a large majority of the population from accessing the appropriate health services they need. Hence, achieving SDG3 will require strengthening the education, training, recruitment, and equitable deployment of HCWs in a paradigm shift to make investments more efficient, effective, and relevant to country needs [2,3,4]. Advancing this objective will impact health expenditure, particularly HCW remuneration—which, along with pharmaceuticals, is a major component of countries’ health expenditure [5, 6]. Of particular bearing are low- and middle-income African countries, which are expected to account for half of the 10 million global shortage by 2030 [3, 7].
Within this context, a better understanding of government HCW expenditure is needed to support national policy-makers and relevant global agencies to develop more effective and sustainable investments over time. This paper seeks to better understand the scope of expenditure on HCW remuneration and its funding sources in Africa. The specific objectives are to:
-
(1)
assess the level of HCW remuneration expenditure and its relative size as part of countries’ overall health expenditure;
-
(2)
ascertain governments’ contribution compared to other funding sources; and
-
(3)
weigh in government HCW allocation as part of overall government health expenditure.
Furthermore, disaggregation by income group and relevant subregional economic entity is provided for benchmarking purposes and to inform decision-making.
Methods
The System of Health Accounts (SHA) and its boundaries measuring HCW expenditure
We use country-produced health accounts data to assess/discuss the magnitude of HCW expenditure in African countries [8]. In short, health accounts help countries trace each dollar spent on health—from source to use—by measuring the magnitude and flow of expenditure on health-defined services consumed by a country’s resident population over a specified period (generally a yearFootnote 1)—regardless of where the money originated (public, private, or external sourcesFootnote 2) or the location of service provision/consumption (hospitals/health centers). Thus, health accounts measure health expenditure associated with all activities that primarily promote, prevent, treat or rehabilitate people’s health status—e.g., disease prevention/cure in hospitals; home-based care for chronic conditions; or information/education/counseling campaigns in schools, prisons, or enterprises. They also measure expenditures on administering the health system at central and regional levels in decentralized countries.
The starting point for determining the boundaries of HCW expenditure is the System of Health Accounts (SHA), the international framework measuring country health expenditures [9]. It distinguishes between current-year consumption—i.e., recurrent spending—and spending for developing/acquiring health infrastructure consumed over years—i.e., capital/development spending. The former comprises current expenditure; and the latter, capital expenditure (Box 1). Key is understanding that pre-service education—provided to students prior to joining the HCW—is considered capital expenditure, whereas in-service training—namely, professional trainings, peer-learning activities, and/or guidance sessions on newly released/updated recommendations for treatment protocols—is considered current health expenditure. This paper only considers the latter.
Furthermore, HCW remuneration is considered in its entirety/complexity in various country contexts. On one hand, this entails wages and social contributions to salaried workers—including any benefits/allowances in cash or in kind, e.g., housing, fee waivers, etc. For the latter, the monetary equivalent of in-kind benefits is reported. On the other hand is the income of self-employed professionals (Box 2). This study follows the international standards defined as “all people engaged in actions whose primary intent is to enhance health” [10], a definition embracing anyone working—either in a publicly owned facility or as a private practitioner—towards promoting, restoring, or maintaining health. This includes management/support staff—part-time and full—located in health facilities or in communities, e.g., community health workers.
The baseline information was calculated in July 2022 for 2019, the year before the COVID-19 pandemic. Country health accounts reports, broken down by factor of provision (FP), can be retrieved from the Documentation Center of WHO’s Global Health Expenditure Database (GHED) (Box 3). The latest available data before 2019 were used when no data were available for 2019 (Appendix 1). Population size and income group data were extracted from GHED Data Explorer in July 2022 (2021 update) [11]. Four parameters of interest were examined:
-
(1)
The share of country health expenditure allocated to HCW remuneration; i.e., the sum of expenditure for compensating employees and paying self-employed professionals, over country health expenditure.
-
(2)
The main funding sources’ level of participation in HCW remuneration.
-
(3)
How much government health expenditure went to remunerating HCW.
-
(4)
Where respective government efforts stand in country comparisons.
Wherever possible, estimates were averaged across countries and by income group or subregional economic group [12,13,14,15] as some of them have common economic criteria to respect, which tends to some degree of harmonization in public spending, including spending on the HCW. This may have an impact on policy formulation, since they interact—e.g., within the WAEMU countries, the ratio of government wage bill to tax revenue cannot exceed 35% [16].
Averages are unweighted and all values are in US$, converted from national currency units using the GHED conversion rate expressed in real terms (2019). Country-specific gross domestic product deflators were used to convert current values to constant values.

WHO’s National Health Workforce Accounts (NHWA)
The National Health Workforce Accounts (NHWA), triggered by the 69th World Health Assembly, is a mechanism for collating/using a set of standardized indicators to generate reliable information/evidence on the health workforce. The objectives are to:
-
(a)
Enable planning, implementation, and monitoring of HCW policies geared towards UHC.
-
(b)
Improve comparability of HCW data both nationally and globally.
It is a system by which countries progressively improve the availability, quality, and use of HCW data by annually reporting a set of indicators to support achievement of UHC, SDGs, and other health objectives [17, 18].
The NHWA portal hosts a variety of HCW statistics relevant to measurement. We extracted country medical doctor (MD) density per 10,000 population for the latest year reported (2021 update) [19]. This information was then used gain perspective on countries’ HCW remuneration expenditure.
Results
General context: This paper analyzes current HCW remuneration expenditure in 33 African countries for which disaggregated information was available out of the 47 countries in the WHO African region, as of 30 July 2022. It represents 70% of the 47 countries, 75% of their population (824 million people out of 1 092 billion), 33% of their MDs (180,404), and 80% of their nurses (737,966). Of the world’s population, it comprises 11%, 1.4% of its MDs, and 2.6% of its nurses.
Out of the 33 countries, 16 are low-income and 17 middle-income countries,Footnote 7 representing 76% of low-income and 71% of middle-income countries of the region, respectively (Table 1). By subregional economic group, eight countries are members of the Southern African Development Community (SADC)Footnote 8; six, the West African Economic and Monetary Union (WAEMU); seven, the Economic Community of West African States (ECOWAS) without being members of WAEMUFootnote 9; and seven, the Economic Community of Central African States (ECCAS). Five countries classified as “Other” do not belong to any of the above-mentioned sub-regional groups (Table 2).
Remuneration of the health and care workforce accounts for an average 29% of country health spending, with marked differences between countries
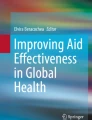
Per capita health expenditure in these 33 countries averaged US$ 109 in real terms, equivalent to 10% of the average global per capita health expenditure (US$ 1140) and 85% of the average per capita expenditure in the 47 African countries (US$ 128).Footnote 10 Average per capita HCW remuneration spending across these 33 countries amounted to US$ 38, 29% of health expenditure, from a minimal US$ 3 in Burundi to US$ 295 in South Africa—or one-sixth and one-half of overall health expenditure in these two countries, respectively. Furthermore, average HCW remuneration expenditure varies from one-quarter to one-third of health expenditure in the 16 low-income and 17 middle-income countries, respectively (Fig. 1a).

Health and care workforce remuneration as part of country health spending, by income and subregional economic group. Boxplots show the interquartile range (25th–75th percentile) of values. The vertical lines from the bars extend to the maximum and minimum values. The median is marked by the bar in the middle. The dot represents the average
There are also differences across subregional economic groups (Fig. 1b). Average per capita HCW expenditure by subregional economic group is estimated at US$ 11, US$ 18, and US$ 94 in WAEMU, ECOWAS,Footnote 11 and SADC countries, respectively (Appendix 2). On average HCW remuneration as a share of country health expenditure is the lowest in WAEMU countries, amounting to 23%—whereas for non-WAEMU ECOWAS countries and SADC countries this ratio is above 25%, averaging 27% and 30%, respectively. In ECCAS countries, HCW remuneration represents 35% of country health spending. Noteworthy is the higher variability in the SADC group compared to the other three (Fig. 1b).
Government biggest contributor to HCW remuneration
GovernmentFootnote 12 is the primary funding source for HCW remuneration, contributing to 60% on average. External aid and private sources contribute less, financing 17% and 23%, respectively. Nevertheless, by income group, contributions from each funding source vary significantly. In middle-income countries, governments fund 71%, compared to 49% in low-income countries. Conversely, external aid plays a critical role in in low-income countries, funding 27%—but in middle-income countries, it funds < 10%. Finally, private sources’ contributions are 24% and 21% in low- and middle-income countries, respectively (Fig. 2).

Funding sources for health and care workforce remuneration, across all countries and by income group. Boxplots show the interquartile range (25th–75th percentile) of values. The vertical lines from the bars extend to the maximum and minimum values. The median is marked by the bar in the middle. The dot represents the average
More than half of government health spending goes to HCW remuneration
Health and care workforce remuneration represents an average 55% of government spending on health. This is true for both low- and middle-income countries alike (Fig. 3a). However, there are marked differences between subregional economic groups. In ECOWAS and ECCAS countries, HCW remuneration accounts for 60% of government spending on health, compared with an average of 47% in WAEMU countries and 50% in SADC countries (Fig. 3b).

Government HCW remuneration as part of government health expenditure, by income and subregional economic group. Boxplots show the interquartile range (25th–75th percentile) of values. The vertical lines from the bars extend to the maximum and minimum values. The median is marked by the bar in the middle. The dot represents the average
Room for more government prioritization of HCW policies
Looking at governments’ efforts, the SADC countries as a group placed a relatively higher government priority on healthFootnote 13 (see the red dots on the right side of Fig. 4). All but Comoros devoted to health more than the average 7% of general government spending calculated across the 33 countries, rising to 15% for South Africa. Moreover, in three countries—South Africa, Zambia, and Zimbabwe—government spending on HCW (see upper-right quadrant) is above-average; in these three countries, HCW remuneration accounts for > 55% of government health expenditure (above the horizontal line in Fig. 4). Whereas, in the other SADC countries, government spending on HCW remuneration was < 55%, below the average calculated across the 33 countries.

Government priority to health and part of government health spending on health and care workforce remuneration. Government priority to health refers to government expenditure on health as a share of government expenditure. The lines represent the average, across the 33 countries, of government priority to health (vertical line) and government remuneration of the health and care workforce as a share of government expenditure on health (horizontal line). Bubble size represents medical doctor density per 10,000 population
West African countries (greenFootnote 14 dots in Fig. 4), in contrast, spent less on health as a share of general government expenditure; all but fourFootnote 15 spent < 7%—the average of government spending on health calculated for the 33 countries (left side of Fig. 4)—but with varying levels of HCW remuneration spending as a share of government health spending. Some contributed > 55%, the average (upper-left quadrant); while in others like Mali, this figure is as low as 28% (lower-left quadrant). ECCAS countries showed no clear-cut pattern.
Finally, irrespective of their subregional economic group, countries on the right side of Fig. 4 presented a higher density HCW—as measured by the number of MDs per 10,000 inhabitants (see bubble size in Fig. 4). Nigeria, in the upper-left quadrant,Footnote 16 is a noticeable exception.
Discussion
Findings
To our knowledge, this is the first attempt to provide a comparable HCW remuneration measurement for such a large number of African countries [20]. The estimates presented/discussed in this paper are based on country-produced data, not derived from modeling or a special data-collection effort but from actual data produced by country health accounts teams. Notably, 30 + African countries could produce data disaggregated enough using the international health spending measurement framework, despite the challenges/limitations of their respective underlying health information systems.
In terms of representativeness, all WAEMU countries but two—Benin and Guinea Bissau—are represented; the ECOWAS countries that are not WAEMU members are all included. This brings the total number of ECOWAS countries to 13 out of 15 (87%); and 50% of the SADC countries on the other hand.
Findings show that HCW remuneration spending is around 30% of country health expenditure. Governments are the main source of funding for HCW remuneration, contributing 60% on average. Furthermore, 55% of government health expenditure is spent on HCW remuneration, underscoring the complexity of the trade-offs to be made considering funding other inputs, e.g., pharmaceuticals. These results are difficult to compare with the only previous publication,Footnote 17 which reported that HCW on average absorbs > 33% of government health expenditure, because our study does not include “capital” types of expenditure—namely, pre-service education, and does not include any high-income country [21].
The highest HCW spenders were those putting higher priority on health, mostly SADC countries—although this subregional economic group bore the highest heterogeneity, probably because of Comoros, and after excluding the Democratic Republic of the Congo, the two SADC countries with below-average priority on health. In fact, Comoros displayed below-average government spending on HCW remuneration, mirroring the West African countries’ spending pattern. A combination of different macroeconomic contexts as well different levels of HCW investment prioritization are likely to play a crucial role in explaining the different levels of spending for remuneration among countries.
Our results highlight the importance of government spending in funding HCW remuneration. The world economic outlook is currently uncertain, predicting a possible slowdown or weak economic growth. Within this context, maintaining or increasing the levels of public spending, and especially the one on HCW might become more of a challenge [22, 23]. Countries relying more on external sources could also face challenges, as it could generally be harder to maintain already-declining donor funding to low- and lower-middle-income countries’ health systems: external aid for health actually peaked in 2014 and has plateaued since [24]. It should be recognized, however, that lower levels of spending on HCW are likely to increase inequalities in access to service and may also be detrimental to the quality of care. Ten years ago, already, analyses determined a need for improved coordination between donor agencies and called for a paradigm shift towards investment in human resources, helping countries develop strategies reflecting specific domestic contexts and international best practices [4, 25]. Thus, mobilizing domestic resources and prioritizing HCW remuneration funding will be key, alongside policies aimed at investing in effective/efficient HCW policies [26].
Limitations
While the current data set allows for general analysis of HCW remuneration, detailed analyses are not currently possible—e.g., comparison between health worker categories, gender pay gap, etc. It was not possible to assess the extent to which expenditures went to MDs, nurses, or other HCW, nor to determine the composition of their remuneration—salaries versus benefits, or policies like “pay for performance”—because the data set does not provide further breakdown by type of remuneration/payment. In addition, because there are currently no statistics that aggregate health workers into a single category, the results are expressed as a share of the country's health expenditure, not per health worker. Collecting systematic information on the private sector is also a serious challenge for several countries [27]. This is particularly the case for countries that do not have a national registry of health facility, which covers all private facilities, ideally by listing all facilities by level of care, from very peripheral first-contact health centers to high-end specialized hospitals, and including independent laboratories/pharmacies [28, 29].
When differentiating countries by risk/vulnerability status to further explore the potential impact on HCW remuneration, we noticed that two-thirds of the countries—11 fragile and 12 warningFootnote 18—were in a “precarious” situation [30]. This impeded differentiating a pattern in levels spent on HCW remuneration. Finally, data availability and quality issues were also a limiting factor,Footnote 19 and later we may have more countries as health accounts quality continues to improve [31, 32].
Conclusions
The results clearly show that the remuneration of the health and care workforce is an important part of government health spending, with an average of 55% of government health spending devoted to it—with some countries well below or above the average. Health prioritization and the macroeconomic context are certainly two elements that play a key role in explaining differences between countries, and would need to be better integrated in further analysis of HCW remuneration spending, especially when considering an increase in the health and care workforce and its impact on remuneration-related expenditures. This is particularly relevant as the 10-million shortage by 2030 will be concentrated in Africa. WHO has called upon governments and partners in countries with greatest health workforce shortages—majority of which part of our study—to take action to double their workforce by 2030. While HCW remuneration accounts for half government health spending, doubling the health and care workforce will require significant increases in government health spending. It will be important to consider options within the fiscal space to allow a sustainable financial growth for the education and employment of health workers, alongside the optimization of the health and care workforce and a focus on efficiencies.
Furthermore, while the results provide some insight into the magnitude of HCW remuneration, more work and research is needed to obtain a more disaggregated and detailed picture, particularly with regard to remuneration across health occupations, between genders, and between the public and private sectors—e.g., private sources’ size would need confirmation in the future. At present, however, HCW remuneration expenditure—albeit part of country-produced health accounts—has not made into the GHED, as harmonization of concepts, collaboration with national counterparts, and integration of feedback require more time/resources. It is a work in progress, and this type of expenditure will eventually make it to publication in the coming years. This is part of a sustained effort by WHO and its partners to provide by-topic detailed thematic guidance, in-country technical assistance, and data-quality assurance to Member States. For example, for a subset of countries, disaggregated data on diseases and health programs—e.g., spending on family planning and primary health care—have been published for the past 5 years.
Capturing trends in the amounts spent on HCW remuneration, including by source of funding, will provide better insights for developing policies related to the funding of HCW remuneration, thereby helping to shape the supply for health workers. Systematically comparing the components of HCW expenditure across countries will allow better identification of different funding sources—either stable or volatile in nature—and their impact on HCW investment over time. Such stocktaking is important for countries, WHO, and other relevant agencies to inform necessary policy changes. Moreover, beyond country comparisons, such as ours, countries interested in further analysis could conduct deep dive analysis, looking at specific variables, to track policy questions of interest—e.g., on recruitment/retention and/or assessing government spending on HCW relative to total government spending on human resource from general government spending.
Data availability
The data sets analyzed during the current study are available from https://www.dropbox.com/s/grdu990bqimhxwq/hwf_data_final_20230220.xlsx?dl=0.
Notes
All of the values in this paper are per year. This can be either calendar or fiscal, depending on the country's context.
“Public” means government-owned resources (collected through taxation) and mandatory contributions to social health insurance schemes, when existing. “Private” refers to out-of-pocket payments and contributions to voluntary health insurance, i.a. “External” refers to funds from abroad (e.g., foreign countries, multilateral agencies).
World Health Organization (WHO). The Global Health Expenditure Database [Internet]. Geneva: WHO; 2023. Available from: https://apps.who.int/nha/database/Home/Index/en (accessed 26 Sep 2023).
World Health Organization (WHO). Methodology for the update of the global health expenditure database 2020–2022: technical note [Internet]. Geneva: WHO; 2023. Available from: https://iris.who.int/handle/10665/365909 (accessed 26 Sep 2023).
World Health Organization (WHO). Global spending on health 2020: Weathering the storm [Internet]. Geneva: WHO; 2020. Available from: https://apps.who.int/iris/handle/10665/337859 (accessed 26 Sep 2023).
World Health Organization (WHO). Global spending on health: rising to the pandemic’s challenges [Internet]. Geneva: WHO; 2022. Available from: https://www.who.int/publications/i/item/9789240064911 (accessed 26 Sep 2023).
Middle-income countries include lower-middle and upper-middle–income countries, as per the World Bank 2019 classification of income groups. A 34th country, Seychelles, is not included as it was the only high-income country with available disaggregated spending amounts on HCW expenditure.
The Democratic Republic of the Congo, which is a member of both ECCAS and SADC, is counted as ECCAS.
Throughout the article, unless otherwise indicated, ECOWAS excludes WAEMU member countries.
The reference year for global and regional average per capita health expenditure is 2019, using the 2021 GHED update.
US$ 15 across the 13 ECOWAS countries with disaggregated data available; WAEMU countries included.
“Government” includes funding sources from government resources (general taxation) and contributions to mandatory health insurance schemes. “External aid” refers to development partner funds handled by non-profit entities or channeled through governments. “Private sources” refer to domestic funds, e.g., out-of-pocket payments and contributions to voluntary health insurance schemes, i.a.
Proxied by government expenditure on health as a share of general government expenditure, as on the x axis of Fig. 4.
Dark and light green, respectively, for ECOWAS and WAEMU countries.
Burkina Faso, Cabo Verde, Ghana, and Niger.
High expenditure on HCW remuneration as a share of government expenditure on health, but with relatively lower government priority on health (government expenditure on health as a share of general government expenditure).
Though, in their paper “Paying for needed health workers for the SDGs: an analysis of fiscal and financial space” In: Health employment and economic growth: an evidence base. Geneva: World Health Organization, 2017, also available, Lauer et al. made a crude attempt to express wage bill as a proportion of public spending on health for 136 countries, and their estimate was 57%.
Stable countries: Botswana, Cabo Verde, Gabon, Ghana, and Namibia. Warning countries: Côte d’Ivoire, Comoros, Gambia, Eswatini, Liberia, Malawi, São Tomé and Príncipe, Senegal, Sierra Leone, South Africa, Togo, and Zambia. Alert countries: Burkina Faso, Burundi, Chad, Central African Republic, Democratic Republic of the Congo, Guinea, Mali, Niger, Nigeria, and Zimbabwe. Five other countries remain unclassified.
One country with available HCW-disaggregated expenditure data could not be included here because more than 30% of its health expenditure was “unclassified:” for > 30% of this country’s expenditure, it was unclear whether it was on HCW, pharmaceuticals, or other type of inputs—potentially underestimating the HCW amounts reported.
Abbreviations
- COVID-19:
-
Severe acute respiratory syndrome-related coronavirus 2, or SARS-CoV-2
- ECCAS:
-
Economic Community of Central African States
- ECOWAS:
-
Economic Community of West African States
- FP:
-
Factor of provision
- GHED:
-
WHO’s Global Health Expenditure Database
- HCW:
-
Health and care workforce
- MD:
-
Medical doctor
- NHWA:
-
WHO’s National Health Workforce Accounts database
- SADC:
-
Southern African Development Community
- SDG:
-
United Nations Sustainable Development Goal
- SHA:
-
System of health accounts
- THE:
-
Total health expenditure
- UHC:
-
Universal health coverage
- WAEMU:
-
West African Economic and Monetary Union
- WHO:
-
World Health Organization
References
United Nations, Department of Economic and Social Affairs, Statistics Division (UNSD). SDG indicators [Internet]. New York: UNSD; 2017. Available from: https://unstats.un.org/sdgs/indicators/indicators-list. Accessed 26 Sep 2023.
United Nations, Statistics Division (UNSTATS). Indicator 3.c.1. E-handbook on SDG indicators [Internet]. New York: UNSTATS; 2021. Available from: https://unstats.un.org/wiki/display/SDGeHandbook/Indicator+3.c.1. Accessed 26 Sep 2023.
World Health Organization (WHO). Global strategy on human resources for health: workforce 2030 [Internet]. Geneva: WHO; 2016. Available from: https://www.who.int/publications/i/item/9789241511131. Accessed 26 Sep 2023.
Zhao F, Squires N, Weakliam D, et al. Investing in human resources for health: the need for a paradigm shift. Bull World Health Organ. 2013;91(11):799-799A. https://doi.org/10.2471/BLT.13.118687.
Tichy EM, Hoffman JM, Suda KJ, Rim MH, Tadrous M, Cuellar S, et al. National trends in prescription drug expenditures and projections for 2022. Am J Health Syst Pharm. 2022;79(14):1158–72. https://doi.org/10.1093/ajhp/zxac102.
Martin AB, Hartman M, Lassman D, Catlin A. National Health Expenditure Accounts Team. National health care spending in 2019: steady growth for the fourth consecutive year. Health Aff Millwood. 2021;40(1):14–24. https://doi.org/10.1377/hlthaff.2020.02022.
Boniol M, Kunjumen T, Nair TS, et al. The global health workforce stock and distribution in 2020 and 2030: a threat to equity and ‘universal’ health coverage? BMJ Glob Health. 2022;7:e009316. https://doi.org/10.1136/bmjgh-2022-009316.
World Health Organization, Regional Office for Africa (WHO/AFRO). All countries. Brazzaville: WHO/AFRO; 2021. Available from: https://www.afro.who.int/countries. Accessed 26 Sept 2023.
Organisation for Economic Co-operation and Development (OECD), European Union (EU), World Health Organization (WHO). A System of Health Accounts 2011: Revised edition. Geneva: WHO; 2017. Available from: https://www.who.int/publications/i/item/9789240042551. Accessed 26 Sep 2023.
World Health Organization (WHO). The world health report: 2006: working together for health. Geneva: WHO; 2016. Available from: https://apps.who.int/iris/handle/10665/43432. Accessed 26 Sep 2023.
World Health Organization (WHO). The Global Health Expenditure Database. Geneva: WHO; 2023. Available from: https://apps.who.int/nha/database/Home/Index/en. Accessed 26 Sep 2023.
The Economic Community of West African States (ECOWAS). Member States. Abuja: ECOWAS; 2023. Available from: https://ecowas.int/member-states/. Accessed 26 Sep 2023.
The West African Economic and Monetary Union (WAEMU). Member States. Lomé: WAEMU; 2023. Available from: http://www.uemoa.int/en/. Accessed 26 Sep 2023.
The Economic Community of Central African States (ECCAS). Member Countries. Libreville: ECCAS; 2023. Available from: https://ceeac-eccas.org/en/#structure. Accessed 26 Sep 2023.
The Southern African Development Community (SADC). Homepage. Gaborone: SADC; 2023. Available from: https://www.sadc.int/member-states. Accessed 26 Sep 2023.
International Monetary Fund (IMF). IMF Country Reports No 19/91, West African Economic and Monetary Union (WAEMU): Selected Issues. Washington, DC: IMF; 2019. Available from: https://www.elibrary.imf.org/downloadpdf/journals/002/2019/091/002.2019.issue-091-en.xml. Accessed 26 Sep 2023.
World Health Organization (WHO). National Health Workforce Accounts: a Handbook. Geneva: WHO; 2017. Available from: https://apps.who.int/iris/bitstream/handle/10665/259360/9789241513111-eng.pdf. Accessed 26 Sep 2023.
World Health Organization (WHO). Strengthening the collection, analysis and use of health workforce data and information: a handbook. Geneva: WHO; 2022. Available from: https://apps.who.int/iris/handle/10665/365680 (accessed 26 Sep 2023).
World Health Organization (WHO). The National Health Workforce Accounts Data Portal. Geneva: WHO; 2023. Available from: https://apps.who.int/nhwaportal/Home/Index. Accessed 26 Sep 2023.
Bertone MP, Lurton G, Mutombo PB. Investigating the remuneration of health workers in the DR Congo: implications for the health workforce and the health system in a fragile setting. Health Policy Plan. 2016;31(9):1143–51. https://doi.org/10.1093/heapol/czv131.
Hernández-Peña P, Poullier JP, Van Mosseveld CJ, Van de Maele N, Cherilova V, Indikadahena C, et al. Health worker remuneration in WHO Member States. Bull World Health Organ. 2013;91(11):808–15. https://doi.org/10.2471/BLT.13.120840.
World Health Organization (WHO). Global spending on health: rising to the pandemic’s challenges. Geneva: WHO; 2022. Available from: https://www.who.int/publications/i/item/9789240064911. Accessed 26 Sep 2023.
Glassman A, Madan Keller J, Smitham E. The future of global health spending amidst multiple crises. Washington, DC: Center for Global Development; 2023. Available from: https://www.cgdev.org/publication/future-global-health-spending-amidst-multiple-crises. Accessed 26 Sep 2023.
World Health Organization (WHO). Global spending on health 2020: Weathering the storm. Geneva: WHO; 2020. Available from: https://apps.who.int/iris/handle/10665/337859. Accessed 26 Sep 2023).
Vujicic M, Weber SE, Nicolic IA, Atun R, Kumar R. An analysis of GAVI, the Global Fund and World Bank support for human resources for health in developing countries. Health Policy Planning. 2012;27(8):649–57.
Asamani JA, Kigozi J, Sikapande B, et al. Investing in the health workforce: fiscal space analysis of 20 countries in East and Southern Africa, 2021–2026. BMJ Glob Health. 2022;7:e008416.
World Health Organization (WHO). Private sector landscape in mixed health systems. Geneva: WHO; 2020. Available from: https://www.who.int/publications/i/item/9789240018303. Accessed 26 Sep 2023.
Nigeria, Federal Ministry of Health. Nigeria Health Facility Registry (HFR). Abuja: Federal Ministry of Health; 2019. Available from: https://hfr.health.gov.ng/. Accessed 26 Sep 2023.
World Health Organization (WHO). Geolocated Health Facilities Data Initiative [Internet]. Geneva: WHO; 2022. Available from: https://www.who.int/data/GIS/GHFD. Accessed 26 Sep 2023.
The Fund for Peace. Fragile States Index [Internet]. Washington, DC: The Fund for Peace; 2018. Available from: https://fragilestatesindex.org/. Accessed 26 Sep 2023.
van Mosseveld C, Hernández-Peña P, Arán D, Cherilova V, Mataria A. How to ensure quality of health accounts. Health Policy. 2016;120(5):544–51. https://doi.org/10.1016/j.healthpol.2016.03.009.
World Health Organization (WHO). Quality control of SHA-based health accounts data. Geneva: WHO; 2023. Forthcoming.
Acknowledgements
The authors are deeply indebted to the country teams that prepared the data. By alphabetical order of country name, the list below acknowledges the WHO Country Office colleagues and Country Focal Points: Botswana: Juliet Evelyn Bataringaya, Tebogo Madidimalo, and Onkemetse Mathala. Burkina Faso: Fatimata Zampaligre, Tchichihouenichidah (Simon) Nassa, and Soumaila Traoré. Burundi: Joseph Nzambimana, Jacqueline Niyungeko, and Ignace Ngabonziza. Cabo Verde: Edith Pereira, Maria Rosário Lopes Correia, and Aryana Germana de Sousa Gomes. Central African Republic: Regis Antoine Mbary Daba, Arlette Valerie Tete, and Jean Chrysostome Kette. Chad: Kadai Oumar Abatcha and Noural Houda Mahamat Boukhari. Comoros: Ahamada Msa Mliva, Koulthoume Maoulana, and Zahara Abdallah. Congo: Dieudonné Bakala, Saturnin Brice Roch Massana, and Gilbert Bruno Ernest Mokongo Amotona. Côte d'Ivoire: Tania Bissouma Ledjou, Christelle Gbayoro, and Séka Christophe Aguia. Democratic Republic of the Congo: Amédée Prosper Djiguimde, Gérard Eloko Eya Matangelo, and Eddy Mongani Mpotongwe. Eswatini: Khosi R. Mthethwa. Ethiopia: Indrajit Hazarika, Samuel Abera, and Ermias Dessie. Gabon: Aboubacar Inoua, Ange Mibindzou Mouelet, and Murielle Ovili. Gambia: Momodou Ceesay, Gibril Jarju, and Haddy Badjie. Ghana: Kingsley Addai Frimpong, Kwakye Kontor, and Ben Bempah. Guinea: Abdoulaye Kaba, Souleymane Diakite, and Ousmane Diakite. Kenya: Brendan Kwesiga, Elkana Ong'uti, and David Njuguna. Liberia: Gebrekidan Mesfin Zbelo, Ernest Gonyon, and Roland Kessely. Malawi: Solome Nampewo, Robert Mwanamanga, and Tasira Mwaupighu. Mali: Nayé Bah, Issa Traoré, and Alpha Mahamoud Touré. Mauritania: Aminata Sakho Kelly, Aly Cheibany, Med Mahmoud Khatry, and Houda Ely. Namibia: Mary Nana Ama Brantuo, Bertha Katjivena, and Thomas Mbeeli. Niger: Moussa Bizo and Sakina Habou Ocquet. Nigeria: Francis Nwachukwu Ukwuije and Nneka Orji. São Tome and Príncipe: José Manuel da Costa dos Prazeres, Anya Major Pires dos Santos, and Paulo Jorge do Rosário Afonso. Senegal: Farba Lamine Sall, Thiané Gueye Diaw, and Alioune Badara Sadia Sonko. Sierra Leone: Selassi A. d'Almeida, Michael Amara, and Nathaniel Soloku. South Africa: Rajesh Narwal and Mongi Jokozela. South Sudan: Joy Luba Lomole Waya, and Kediende Chong. Togo: Kiswendsida Romain Hilaire Ouedraogo, Aboubakar Issa, and Kwami Ezunyuie Komedza. Uganda: Christabel Abewe, Susan Najjuko, and Sarah Byakika. Zambia: Solomon Sitinadziwe Kagulura, Henry Kansembe, and Patrick Banda. Zimbabwe: Stanley Munyaradzi Midzi, Heather Machamire, and Gwati Gwati. The authors are also grateful to Jean-Edouard Doamba, Ezrah Rwakinanga, and the participants of the data review workshops in Lomé, Togo, on September 23–27, 2019 and in Harare, Zimbabwe on October 15–17, 2019 for the fruitful discussions and active revision of the data. Finally, the authors would like to thank James Asamani, Mathieu Boniol, James Campbell, Ogochukwu Chukwujekwu, Giorgio Cometto, Julien Dupuy, Natalja Eigo, and Ke Xu for reviewing the draft manuscript and providing helpful feedback.
Funding
The WHO health accounts team receives funding from the Bill & Melinda Gates Foundation; Gavi the Vaccine Alliance; the Global Fund to Fight AIDS, Tuberculosis and Malaria; and the United States Agency for International Development. None participated in the analysis and interpretation of the findings.
Author information
Authors and Affiliations
Contributions
HT wrote the first draft. MA ran the analysis, prepared the figures and tables, and wrote sections of the paper. Both HT and MA interpreted the preliminary findings. JPB and PZ wrote sections of the paper and provided an HCW perspective. SC and BN managed the implementation strategy. All authors reviewed the paper and agreed on its conclusions.
Disclaimer
The authors are staff members of the World Health Organization. The authors alone are responsible for the views expressed in this article and they do not necessarily represent the dec AQ isions, policy or views of the World Health Organization.
Corresponding author
Ethics declarations
Competing interest
The authors declare no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1: Country list
Country name | Country code | Income groupa | Subregional economic group | Latest available year |
|---|---|---|---|---|
Botswana | BWA | Middle-income | SADC | 2017 |
Burkina Faso | BFA | Low-income | WAEMU | 2019 |
Burundi | BDI | Low-income | ECCAS | 2018 |
Cabo Verde, Republic of | CPV | Middle-income | ECOWAS | 2016 |
Central African Republic | CAF | Low-income | ECCAS | 2018 |
Chad | TCD | Low-income | ECCAS | 2018 |
Comoros | COM | Middle-income | SADC | 2019 |
Congo | COG | Middle-income | ECCAS | 2018 |
Côte d'Ivoire | CIV | Middle-income | WAEMU | 2018 |
Democratic Republic of the Congo | COD | Low-income | ECCAS | 2019 |
Eswatini | SWZ | Middle-income | SADC | 2017 |
Ethiopia | ETH | Low-income | Other | 2017 |
Gabon | GAB | Middle-income | ECCAS | 2019 |
Gambia | GMB | Low-income | ECOWAS | 2015 |
Ghana | GHA | Middle-income | ECOWAS | 2015 |
Guinea | GIN | Low-income | ECOWAS | 2019 |
Kenya | KEN | Middle-income | Other | 2019 |
Liberia | LBR | Low-income | ECOWAS | 2019 |
Malawi | MWI | Low-income | SADC | 2018 |
Mali | MLI | Low-income | WAEMU | 2018 |
Mauritania | MRT | Middle-income | Other | 2017 |
Namibia | NAM | Middle-income | SADC | 2016 |
Niger | NER | Low-income | WAEMU | 2019 |
Nigeria | NGA | Middle-income | ECOWAS | 2019 |
Sao Tome and Principe | STP | Middle-income | ECCAS | 2017 |
Senegal | SEN | Middle-income | WAEMU | 2016 |
Sierra Leone | SLE | Low-income | ECOWAS | 2018 |
South Africa | ZAF | Middle-income | SADC | 2016 |
South Sudan | SSD | Low-income | Other | 2017 |
Togo | TGO | Low-income | WAEMU | 2019 |
Uganda | UGA | Low-income | Other | 2019 |
Zambia | ZMB | Middle-income | SADC | 2016 |
Zimbabwe | ZWE | Middle-income | SADC | 2018 |
Appendix 2: Expenditure on the health and care workforce remuneration
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Toure, H., Aranguren Garcia, M., Bustamante Izquierdo, J.P. et al. Health expenditure: how much is spent on health and care worker remuneration? An analysis of 33 low- and middle-income African countries. Hum Resour Health 21, 96 (2023). https://doi.org/10.1186/s12960-023-00872-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12960-023-00872-y