
Abstract
Objective
To investigate whether seasonal variations and meteorological factors influence pregnancy outcomes in women undergoing in vitro fertilization-embryo transfer (IVF-ET) treatment.
Design
Retrospective cohort study.
Setting
University-affiliated reproductive medical center.
Subjects
Women aged < 35 years undergoing IVF from June 1, 2015, to June 1, 2019.
Interventions
Cycles were divided into four groups according to the date of the beginning of ovulation induction: spring (659 cycles), summer (578 cycles), autumn (519 cycles), and winter (534 cycles).
Results
The high-quality embryo rate was higher in autumn and winter than in cycles in which ovulation induction occurred in spring and summer (58.70% vs. 58.78% vs. 62.67% vs. 63.42%; P < 0.001). The results of linear regression analysis showed that the high-quality embryo rate was significantly correlated with the daily average temperature of ovulation induction (P = 0.037). The clinical pregnancy rates of cycles starting ovulation induction in spring, summer, and autumn were significantly higher than those starting in winter (70.71% vs. 73.18% vs. 70.13% vs. 65.17%; P = 0.031), while the biochemical pregnancy rate, early abortion rate, and live birth rate were not significantly different (P > 0.050). Multivariate logistic regression analysis showed significant seasonal variation in clinical pregnancy (OR = 1.643, 95% CI = 1.203–2.243; P = 0.002), and that a higher daily average temperature at the time of ovulation induction increased the clinical pregnancy rate (OR = 1.012, 95% CI = 1.001–1.022; P = 0.031).
Conclusions
In women younger than 35 years who undergo IVF treatment, the season and ambient temperature on the date of the beginning of ovulation induction may have an impact on embryo development and clinical pregnancy.
Similar content being viewed by others


Introduction
Spontaneous conception has seasonal variations, and multiple pregnancies, ectopic pregnancy, spontaneous abortion, stillbirth, and live birth are all thought to be impacted by seasonal variations [1,2,3]. Studies have found that among naturally conceived pregnancies in the USA, birth rates are higher in summer and early autumn (July to September) than in spring (April and May), whereas in Northern Europe, birth rates are highest in spring (March and April) and lowest in autumn (October and November) [4]. Natural conception may be influenced by a number of factors, including cultural and sociological factors, as well as environmental factors.
Assisted reproductive technology (ART) provides a good model for investigating the effects of meteorological changes on a woman's conception process, because the patient's physiological status and meteorological factors can be more easily determined [5]. Although many studies of seasonal variation and meteorological factors on pregnancy outcomes in women who underwent in vitro fertilization (IVF) treatment have been conducted in identical climatic conditions, their results are varied [5,6,7,8]. A study conducted in Jerusalem showed that the quality of the embryo and fertilization rates were affected by seasonal variation during ART treatment [5], whereas another study found that pregnancy outcomes of ART did not follow any specific seasonal variation [6]. Omsk, Russia, and Alberta, Canada, have a similar humid continental climate; however, studies from Omsk identified higher pregnancy rates in summer and autumn [7], whereas studies from Alberta found no significant seasonal variation in pregnancy outcomes [8]. The differences in the results may be contributed to the differences in the study population and the geographical environment in which the study population is located, and the criteria for assigning patients to the corresponding seasons are inconsistent in various studies (e.g., according to the day of stimulation, oocyte retrieval, or embryo transfer).
Therefore, we conducted a large cohort study of more than 2000 IVF cycles at a reproductive medical center to investigate the effects of seasonal and meteorological factors on the date of the beginning of ovulation induction on embryo development and pregnancy outcomes in women who had undergone IVF treatment. Multivariate logistic regression analysis was performed to understand the seasonal factors that are associated with IVF pregnancy outcomes for improved clinical application.
Materials and methods
Study design
We conducted a retrospective cohort study of women who underwent IVF for the first time at the Reproductive Medicine Center of the First Affiliated Hospital of Zhengzhou University from June 1, 2015, to June 1, 2019. All patients were treated using the follicular phase long-acting long protocol. And only 2290 women had a successful first fresh embryo transfer cycle that met the inclusion and exclusion criteria. Henan Province has a warm temperate subtropical monsoon climate. All cycles were divided into spring (March–May), summer (June–August), autumn (September–November), and winter (December–February) according to the date of the beginning of ovulation induction.
The inclusion criteria were as follows: 1) age 20–35 years, to eliminate the effect of advanced age on pregnancy outcomes, 2) normal ovarian function (antral follicle count [AFC] > 7, anti-Mullerian hormone [AMH] > 1.1 ng/mL), 3) first fresh IVF cycle using the follicular phase long-term protocol for ovulation induction, and 4) fresh embryo transfer after oocyte retrieval. The exclusion criteria were as follows: 1) cycle cancellation of fresh embryo transfer due to liver or kidney dysfunction, pre-implantation genetic diagnosis/pre-implantation genetic screening, or personal reasons; 2) a history of endometriosis, adenomyosis, uterine malformation, endometrial polyps, uterine fibroids, scarred uterus, pelvic tuberculosis, cervical insufficiency, cervical conization, severe hydrosalpinx, polycystic ovary syndrome, repeated implantation failure, recurrent miscarriages, or endocrine diseases; 3) chromosomal abnormalities (for either the woman or man, or both); and 4) severe oligozoospermia or teratozoospermia in the male partner.
This study was approved by the Ethics Committee for Scientific Research and Clinical Trials of the First Affiliated Hospital of Zhengzhou University. Written informed consent for participation was not required for this study, in accordance with the national legislation and institutional requirements.
Meteorological data
The meteorological data for June 1, 2015, to June 1, 2019, for Zhengzhou City, Henan Province, China were downloaded from the China Meteorological Data Network (http://data.cma.cn/). The data included daily average temperature, daily average humidity, and sunshine duration.
IVF protocol
Downregulation regimen
On day 2–3 of the menstrual cycle, patients were given 3.75 mg of a long-acting gonadotropin (Gn)-releasing hormone agonist (Diphereline, 3.75 mg; Beaufour-Ipsen, Dreux, France), by subcutaneous injection, to achieve pituitary downregulation. After 30–42 days, vaginal ultrasound and serum follicle stimulating hormone (FSH), luteinizing hormone (LH), estrogen (E2), and progesterone (P) levels were used to assess pituitary downregulation, and to ensure that the downregulating standard was reached (no functional cyst with diameter > 10 mm, a serum FSH level < 5 IU/L, and LH level < 3 IU/L); controlled ovarian hyperstimulation was subsequently performed.
Ovulation induction and oocyte retrieval
The dosage of Gn (GONAL-f; Merck Serono, Darmstadt, Germany) was individualized based on the patient's age, AMH level, AFC, body mass index (BMI), and serum basal FSH level. The dosage of Gn and the addition of human menopausal Gn (LeBold, Zhuhai Livzon Pharmaceutical, China) was considered based on the follicle size and hormone levels. When one dominant follicle was ≥ 20 mm in diameter and at least three dominant follicles were ≥ 17 mm in diameter, we administered 250 mg of Azer (Merck Serono, Italy) and 2000 IU of human chorionic Gn (hCG) (Zhuhai Livzon Pharmaceutical, China). Oocyte retrieval was performed under vaginal ultrasound guidance 36–37 h after the trigger injection.
Embryo culture and transfer
Fertilization was observed on the first day after oocyte retrieval; double pronucleus (2PN) was considered to identify normal zygotes, and these were transferred into cleavage fluid to continue culture. Cleavage and development of embryos were observed on the third day; embryo quality was assessed according to the number, diameter, morphology, and developmental rate of blastomeres. Fresh embryo transfer was performed according to embryo quality, endometrial status, and patient conditions.
Outcome measures
The primary outcomes were clinical pregnancy and live birth, and the secondary outcomes were biochemical pregnancy and early abortion. Clinical pregnancy was defined as a pregnancy diagnosed by ultrasonographic visualization of one or more gestational sacs or definitive clinical signs of pregnancy. Live birth was defined as the complete expulsion or extraction from its mother of a product of fertilization, irrespective of the duration of the pregnancy which, after such separation, breathes or shows any other evidence of life, such as heart beat, umbilical cord pulsation, or definite movement of voluntary muscles, irrespective of whether the umbilical cord has been cut or the placenta is attached. Biochemical pregnancy was defined as a pregnancy diagnosed only by the detection of hCG in serum or urine and that does not develop into a clinical pregnancy. Early abortion was defined as the spontaneous loss of a clinical pregnancy occurring before 12 completed weeks of gestational age [9].
Evaluation measures were as follows: 1) ovarian response indicators: total dosage of Gn used, length of Gn used, and number of oocytes retrieved; 2) embryo quality indicators: number of 2PN fertilization, 2PN fertilization rate (number of 2PN fertilization/number of oocytes retrieved × 100), number of 2PN cleavage, 2PN cleavage rate (number of 2PN cleavage/number of 2PN fertilization × 100), number of high-quality embryos, high-quality embryo rate (number of high-quality embryos/number of 2PN cleavage × 100), and number of transferred embryos; 3) pregnancy outcomes: biochemical pregnancy rate (number of hCG positive cycles/number of transplant cycles × 100), clinical pregnancy rate (number of clinical pregnancy cycles/number of transplant cycles × 100), early abortion rate (number of cycles with early abortion/number of cycles with clinical pregnancy × 100), and live birth rate (number of deliveries that resulted in at least one live born baby/number of transplant cycles × 100).
Statistical analysis
SPSS 22.0 (IBM Corporation, Armonk, NY, USA) was used for data processing and analysis. Measurement data were suggested to meet the normal distribution using the Shapiro–Wilk test; therefore, the measurement data were expressed as mean ± standard deviation. For comparison of continuous variables between multiple groups and when the variance was homogeneous among groups, one-way ANOVA was used. The LSD-t test was used for paired comparisons of continuous variables within the groups. Enumeration data are expressed as the constituent ratio or rate (%). The chi-square test was used to compare differences between categorical variables, and Bonferroni correction was used to account for multiple testing. Linear regression analysis was used for continuous variables, and multivariate logistic regression analysis was used for dichotomous variables. Analysis items with P < 0.050 was considered statistically significant.
Sensitivity analysis
We conducted sensitivity analyses stratified by the day of embryo transfer to verify the stability of our findings. At our center, most fresh embryo transfers occurred at the cleavage stage on Day 3. Day 3 and Day 5 embryo transfers were analyzed separately to assess whether the potential effects of seasonal variation and meteorological factors remained consistent across studies.
Results
Patients’ general characteristics
According to the inclusion and exclusion criteria, 2290 patients (2290 fresh IVF cycles) were included in this study. We divided the patients into four groups according to the seasons: 659 cycles in the spring group, 578 cycles in the summer group, 519 cycles in the autumn group, and 534 cycles in the winter group. The results showed that there were no significant differences in age, type of infertility, duration of infertility, infertility factor, BMI, basal E2 level, basal FSH level, basal LH level, basal AMH level, or AFC among patients in different seasons (P > 0.050; Table 1).
Laboratory results and pregnancy outcomes
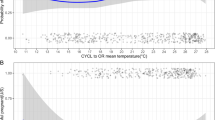
There were no statistically significant differences in the total dosage of Gn used, length of Gn used, number of oocytes retrieved, number of 2PN fertilization, 2PN fertilization rate, number of 2PN cleavage, 2PN cleavage rate, number of high-quality embryos, and number of transferred embryos in each season (P > 0.050). The high-quality embryo rate in the autumn and winter groups was significantly higher than that in the spring and summer groups (62.67% vs. 63.42% vs. 58.70% vs. 58.78%; P < 0.001). In addition, the clinical pregnancy rate was higher in the spring and summer groups than that in the winter group (70.71% vs. 73.18% vs. 70.13% vs. 65.17%; P = 0.031). The biochemical pregnancy rate, early abortion rate, and live birth rate in the winter group were lower than those in the other three groups, but the differences were not statistically significant (P > 0.050; Table 2 and Fig. 1).

Laboratory results and pregnancy outcomes. Note: * Bonferroni correction, P < 0.050
Logistic regression assessment of pregnancy outcomes
We performed univariate logistic regression analysis on pregnancy outcome indicators (biochemical pregnancy, clinical pregnancy, early abortion, and live birth), in which statistically significant indicators were included in the multivariate logistic regression analysis. After correction for confounding factors, the results showed that the clinical pregnancy rates were 1.253-fold, 1.643-fold, and 1.190-fold higher in the spring, summer, and autumn groups, respectively, compared to the winter group. In addition, we found a significant correlation between the daily average temperature of ovulation induction and clinical pregnancy (odds ratio [OR] = 1.012, 95% CI = 1.001–1.022; P = 0.031; Table 3).
Linear regression assessment of high-quality embryo rate
There was a significant difference in the high-quality embryo rate among the seasons, and linear regression analysis of the relationship between the high-quality embryo rate and meteorological factors showed that the high-quality embryo rate was significantly correlated with the daily average temperature at ovulation induction (P = 0.037; Table 4).
Sensitivity analyses
In the sensitivity analyses restricted to Day 3 fresh embryo transfers (1888 cycles), the association between seasonal parameters and clinical pregnancy was consistent with the results described in our overall analysis. The clinical pregnancy rate was 52.1% higher (OR = 1.521, 95% CI = 1.064–2.174; P = 0.021) in summer compared with cycles starting ovulation induction in winter, and increased with the daily average temperature at ovulation induction (OR = 1.014, 95% CI = 1.001–1.029; P = 0.042; Table 5). In cycles with fresh embryo transfer on Day 5 (402 cycles), the ORs for seasonal parameters and clinical pregnancy varied more because of the small sample size.
Discussion
Due to many factors, such as environment, lifestyle, and age at the time of reproduction, the incidence of infertility shows a continuous increasing trend. The emergence of ART has brought hope for fertility to many infertile families [10]. The aim of this study was to investigate whether seasonal variations and meteorological factors affect embryo development and pregnancy outcomes in women undergoing IVF for the first time. Our findings suggest that season and environmental temperature on the date of the beginning of ovulation induction was an important factor affecting embryo development and clinical pregnancy. The clinical pregnancy rate was significantly higher in seasons with higher daily mean temperatures (spring, summer, and autumn) than in winter, which has a lower daily mean temperature, while other environmental factors such as humidity and sunshine duration had no effect on pregnancy outcomes.
There are many controversies about whether seasonal variation and environmental factors are related to pregnancy outcomes in women undergoing IVF treatment. The conclusions drawn from this study are in agreement with previous findings [11, 12]. A study conducted at the University of Arizona, USA, showed that the implantation rate, clinical pregnancy rate, and live birth rate were higher in women who obtained oocytes for ART in summer than in other seasons [11]. A study conducted in Hong Kong, China, also concluded that daily temperature is the most important factor affecting pregnancy outcomes, whereas humidity, sunlight duration, and solar radiation had no effect on pregnancy outcomes [12]. In addition, there are many inconsistent conclusions that pregnancy outcomes in women undergoing IVF treatment are not affected by seasonal variations [6, 8, 13]. On the one hand, it may be because of differences in the geographical environment in which the study populations were located, as well as the use of controlled ovarian hyperstimulation protocols. On the other hand, the time nodes of included patients are also inconsistent. Some studies are based on the date of the beginning of ovulation induction, while others are based on the date of oocyte retrieval or embryo transfer. The conclusions drawn from different study settings are not comparable.
In this study, there was no significant difference in the total dosage of Gn used, length of Gn used, or number of oocytes retrieved among seasons, which is consistent with the results of Wunder et al. [14], indicating that seasonal variations do not affect the ovarian response. The present study showed that the high-quality embryo rate was significantly higher in autumn and winter than in spring and summer, which is consistent with the conclusions of Stolwijk et al. [15], but in contrast to the conclusions of Rojansky et al. [5]. The effect of seasonal variations on human fertility mainly occurs through seasonal variations in daily temperature and light intensity [16]. Photoperiodism is the main environmental factor that causes seasonal variations in mammalian reproduction [17]. Melatonin secretion from the pineal gland is affected by periodic changes in light intensity due to seasonal variations, changing the secretion rhythm of Gn-releasing hormone, which affects multiple aspects such as Gn secretion and follicular development [18]. Melatonin has been shown to improve pregnancy outcomes in IVF by increasing the number of mature oocytes, fertilization rate, and the number of high-quality embryos [10, 19]. The duration of sunshine in autumn and winter can lead to increased melatonin secretion [20, 21], which is capable of improving egg quality. Dragojevic et al. found that melatonin receptors are present in both the central nervous system and peripheral tissues where they play a physiological role [22]. In the present study, all patients used Gn-releasing hormone agonists for hypothalamic and pituitary down-regulation; thus, the effect of light on the hypothalamus and pituitary was diminished and melatonin may act mainly through peripheral tissues.
Although the high-quality embryo rate in autumn and winter was higher than that in spring and summer, our study results showed that the clinical pregnancy rate in winter was lower than that in the other three seasons, which may be related to the vitamin D content in the body. While diet contributes to circulating vitamin D levels, the majority is derived from sun exposure [23]. Vitamin D deficiency and secondary hyperparathyroidism are more likely to occur in winter than in summer [24]. Some studies have shown no association between vitamin D levels and clinical outcomes of IVF [25,26,27]. Howover, a meta-analysis of 11 published cohort studies concluded that adequate vitamin D levels are associated with higher clinical pregnancy and live birth rates among women undergoing ART [28]. In addition, factors other than season, temperature, and vitamin D levels may also be involved. For example, lifestyle changes associated with diet and activity in warm months may lead to better clinical outcomes during these months [29]. Future research should consider including the personal factors of couples that may be influenced by seasonal factors.
It is noteworthy that this study has many strengths. First, to reduce the effect of age on pregnancy outcomes, the included sample was limited to women aged < 35 years. Second, Zhengzhou City, Henan Province belongs to a continental monsoon climate with moderate cold and warm temperatures and four clear seasons, which provides favorable environmental conditions for studying the effects of seasonal factors on pregnancy outcomes. Furthermore, this study is the first to focus on a population undergoing ovulation induction using the follicular phase long-acting long protocol, and IVF cycles were divided into four seasons according to the date of the beginning of ovulation induction, which can better assess the impact of seasonal factors on ovarian response, embryo development, and pregnancy outcomes. In addition, the present study is the first to investigate the effects of seasonal variation and environmental temperature on high-quality embryo rate. However, this study also inevitably has several limitations. First, we collected retrospective data from a single center, the First Affiliated Hospital of Zhengzhou University, Henan Province; therefore, the findings cannot be applied to other regions with different climates. Additionally, indoor heating is common in some areas of Henan Province, which may have affected the study results; nevertheless, all patients were inevitably affected by the external environment. Temperature has been shown to be associated with male fertility [30,31,32,33]. In this study, we have excluded men with severe oligozoospermia or teratozoospermia, but still cannot completely rule out the effects of seasonal variation and ambient temperature on semen quality. As in previous studies, we selected the season and meteorological factors related to a specific date in the IVF process to serve as proxy for the overall environment during treatment, which may have introduced bias in the study results.
Conclusions
This study suggests that season and ambient temperature on the date of the beginning of ovulation induction may affect embryo development and clinical pregnancy during IVF treatment. However, a multicenter study with a large sample size is required to verify the conclusion.
Availability of data and materials
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
References
Hughes MM, Katz J, Mullany LC, Khatry SK, LeClerq SC, Darmstadt GL, Tielsch JM. Seasonality of birth outcomes in rural Sarlahi District, Nepal: a population-based prospective cohort. BMC Pregnancy Childbirth. 2014;6(14):310.
Smits LJ, Van Poppel FW, Verduin JA, Jongbloet PH, Straatman H, Zielhuis GA. Is fecundability associated with month of birth? An analysis of 19th and early 20th century family reconstitution data from The Netherlands. Hum Reprod. 1997;12(11):2572–8.
Rojansky N, Brzezinski A, Schenker JG. Seasonality in human reproduction: an update. Hum Reprod. 1992;7(6):735–45.
Lam DA, Miron JA. Global patterns of seasonal variation in human fertility. Ann N Y Acad Sci. 1994;18(709):9–28.
Rojansky N, Benshushan A, Meirsdorf S, Lewin A, Laufer N, Safran A. Seasonal variability in fertilization and embryo quality rates in women undergoing IVF. Fertil Steril. 2000;74(3):476–81.
Gindes L, Yoeli R, Orvieto R, Shelef M, Ben-Rafael Z, Bar-Hava I. Pregnancy rate fluctuations during routine work in an assisted reproduction technology unit. Hum Reprod. 2003;18(11):2485–8.
Medyannikova IV, Klinyshkova TV. Efficiency of Treatment Cycles for In vitro Fertilization at Climatic Conditions of Siberian Region (Omsk, Russia)[J]. Global Veterinaria. 2012;9(4):388–95.
Dunphy BC, Anderson-Sykes S, Brant R, Pattinson HA, Greene CA. Human embryo implantation following in-vitro fertilization: is there a seasonal variation? Hum Reprod. 1995;10(7):1825–7.
Zegers-Hochschild F, Adamson GD, de Mouzon J, Ishihara O, Mansour R, Nygren K, Sullivan E, Vanderpoel S, International Committee for Monitoring Assisted Reproductive Technology, World Health Organization. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril. 2009;92(5):1520–4.
Yong W, Ma H, Na M, Gao T, Zhang Y, Hao L, Yu H, Yang H, Deng X. Roles of melatonin in the field of reproductive medicine. Biomed Pharmacother. 2021;144:112001.
Farland LV, Correia KFB, Missmer SA, Racowsky C. Seasonal variation, temperature, day length, and IVF outcomes from fresh cycles. J Assist Reprod Genet. 2020;37(10):2427–33.
Zhao M, Zhang H, Waters THB, Chung JPW, Li TC, Chan DYL. The effects of daily meteorological perturbation on pregnancy outcome: follow-up of a cohort of young women undergoing IVF treatment. Environ Health. 2019;18(1):103.
Liu X, Bai H, Mol BW, Shi W, Gao M, Shi J. Seasonal variability does not impact in vitro fertilization success. Sci Rep. 2019;9(1):17185.
Wunder DM, Limoni C, Birkhäuser MH, Swiss FIVNAT-Group. Lack of seasonal variations in fertilization, pregnancy and implantation rates in women undergoing IVF. Hum Reprod. 2005;20(11):3122–9.
Stolwijk AM, Reuvers MJ, Hamilton CJ, Jongbloet PH, Hollanders JM, Zielhuis GA. Seasonality in the results of in-vitro fertilization. Hum Reprod. 1994;9(12):2300–5.
Revelli A, La Sala GB, Gennarelli G, Scatigna L, Racca C, Massobrio M. Seasonality and human in vitro fertilization outcome. Gynecol Endocrinol. 2005;21(1):12–7.
Wood S, Quinn A, Troupe S, Kingsland C, Lewis-Jones I. Seasonal variation in assisted conception cycles and the influence of photoperiodism on outcome in in vitro fertilization cycles. Hum Fertil (Camb). 2006;9(4):223–9.
Eryilmaz OG, Devran A, Sarikaya E, Aksakal FN, Mollamahmutoğlu L, Cicek N. Melatonin improves the oocyte and the embryo in IVF patients with sleep disturbances, but does not improve the sleeping problems. J Assist Reprod Genet. 2011;28(9):815–20.
Tamura H, Nakamura Y, Korkmaz A, Manchester LC, Tan DX, Sugino N, Reiter RJ. Melatonin and the ovary: physiological and pathophysiological implications. Fertil Steril. 2009;92(1):328–43.
Yie SM, Brown GM, Liu GY, Collins JA, Daya S, Hughes EG, Foster WG, Younglai EV. Melatonin and steroids in human pre-ovulatory follicular fluid: seasonal variations and granulosa cell steroid production. Hum Reprod. 1995;10(1):50–5.
Wehr TA. Photoperiodism in humans and other primates: evidence and implications. J Biol Rhythms. 2001;16(4):348–64.
DragojevicDikic S, Jovanovic AM, Dikic S, Jovanovic T, Jurisic A, Dobrosavljevic A. Melatonin: a “Higgs boson” in human reproduction. Gynecol Endocrinol. 2015;31(2):92–101.
Wirz-Justice A, Skene DJ, Münch M. The relevance of daylight for humans. Biochem Pharmacol. 2021;191:114304.
Kroll MH, Bi C, Garber CC, Kaufman HW, Liu D, Caston-Balderrama A, Zhang K, Clarke N, Xie M, Reitz RE, Suffin SC, Holick MF. Temporal relationship between vitamin D status and parathyroid hormone in the United States. PLoS ONE. 2015;10(3):e0118108.
Rudick B, Ingles S, Chung K, Stanczyk F, Paulson R, Bendikson K. Characterizing the influence of vitamin D levels on IVF outcomes. Hum Reprod. 2012;27(11):3321–7.
Xuemei Liu, Zhang Wei Xu, Yanping, et al. Effect of vitamin D status on normal fertilization rate following in vitro fertilization. [J]. Reprod Biol Endocrinol. 2019;17:59.
Alberta Fabris, Alberto Pacheco, María Cruz, et al. Impact of circulating levels of total and bioavailable serum vitamin D on pregnancy rate in egg donation recipients. [J]. Fertil Steril. 2014;102:1608–12.
Justin Chu, Ioannis Gallos, Aurelio Tobias, et al. Vitamin D and assisted reproductive treatment outcome: a systematic review and meta-analysis. [J]. Hum Reprod. 2018;33:65–80.
Correia Katharine FB, Farland Leslie V, Missmer Stacey A, et al. The association between season, day length, and temperature on clinical outcomes after cryopreserved embryo transfer.[J]. Fertil Steril. 2022;117:539–47.
Levitas E, Lunenfeld E, Weisz N, Friger M, Har-Vardi I. Seasonal variations of human sperm cells among 6455 semen samples: a plausible explanation of a seasonal birth pattern. Am J Obstet Gynecol. 2013;208(5):406.e1-6.
Kabukçu C, Çil N, Turan T, Özlülerden Y, Çabuş Ü, Abban MG. Do seasonal variations in ambient temperature, humidity and daylight duration affect semen parameters? A retrospective analysis over eight years. Andrologia. 2020;52(10):e13777.
Zhou Y, Meng T, Wu L, Duan Y, Li G, Shi C, Zhang H, Peng Z, Fan C, Ma J, Xiong C, Bao W, Liu Y. Association between ambient temperature and semen quality: A longitudinal study of 10 802 men in China. Environ Int. 2020;135:105364.
Wang X, Tian X, Ye B, et al. The association between ambient temperature and sperm quality in Wuhan, China.[J]. Environ Health. 2020;19:44.
Acknowledgements
We would like to thank the medical staff and patients of the First Affiliated Hospital of Zhengzhou University for recording the data and cooperating with the treatment. Thanks to Dr. Qiwei Yu for his assistance in statistical analyses and revising the manuscript.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82071649) and the Key Scientific Research Projects of Higher Education Institutions in Henan Province (Grant No. 22A320025).
Author information
Authors and Affiliations
Contributions
JZ contributed to the conception of this study. TC was responsible for the study design, statistical analyses, and manuscript writing. DW contributed to revising the manuscript. TY contributed to data collection. All authors contributed to the manuscript and approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study design was reviewed and approved by the Ethics Committee for Scientific Research and Clinical Trials of the First Affiliated Hospital of Zhengzhou University. Written informed consent for participation was not required due to the retrospective nature of this study, in accordance with the national legislation and institutional requirements.
Consent for publication
Not applicable.
Competing of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chu, T., Wang, D., Yu, T. et al. Effects of seasonal variations and meteorological factors on IVF pregnancy outcomes: a cohort study from Henan Province, China. Reprod Biol Endocrinol 20, 113 (2022). https://doi.org/10.1186/s12958-022-00986-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12958-022-00986-3