
Abstract
Background
The use of recombinant human follicle-stimulating hormone (r-hFSH) in ovarian stimulation protocols for infertility treatment in assisted reproductive technology (ART) clinical practice is well established. More recent advancements include the availability of biosimilar r-hFSH products, which expand the choices available to healthcare practitioners and patients. Better understanding of how such a product contributes to routine clinical practice is valuable to help prescribers make informed treatment choices. The objective of this study was to examine the effectiveness and safety of ovarian stimulation (OS) with follitropin alfa (Ovaleap®) for routine IVF or intracytoplasmic sperm injection treatment in gonadotropin-releasing hormone (GnRH) antagonist cycles in real-world ART clinical practice.
Methods
This non-interventional, multicenter, prospective study was initiated in 34 specialized reproductive medicine centers in Germany. Eligible women were 18–40 years old with a body mass index < 30 kg/m2, menstrual cycle 24–35 days and anti-Müllerian hormone ≥1 ng/mL, who were undergoing a first OS cycle exclusively with Ovaleap® during routine ART using a GnRH antagonist protocol. Primary effectiveness outcomes were number of retrieved oocytes after OS and clinical pregnancy rate (CPR). Secondary outcomes included fertilization rate, number of transferred embryos, live birth delivery rate, safety, and user satisfaction with the Ovaleap® pen.
Result(s)
Of 507 women screened, 463 received at least 1 dose of Ovaleap® and 439 had Visit 2 data (per protocol population; PPP). The mean(±SD) number of retrieved oocytes was 11.8 ± 7.2 (PPP). The CPR among women with documented embryo transfer was 41.3% (158/383), resulting in a live birth delivery rate of 31.6% (138/437) among PPP patients with available follow-up information. Overall, 8.6% (40/463) of women reported ≥1 adverse drug reaction. Ovarian hyperstimulation syndrome occurred in 23 (5.0%) patients, rated mild in 14 (3.0%), moderate in 8 (1.7%), and severe in 1 (0.2%). Patients reported high user satisfaction and high convenience with use of the Ovaleap® pen.
Conclusion
The effectiveness and safety of OS with Ovaleap® in a GnRH antagonist protocol were extended to real-world ART clinical practice for the first time.
Trial registration
Registered on 22 June 2016 (retrospectively registered) at ClinicalTrials.gov (NCT02809989).
Similar content being viewed by others


Background
Infertility treatment with assisted reproductive technology (ART) often includes ovarian stimulation (OS) with exogenous gonadotropins. Recombinant human follicle-stimulating hormone (r-hFSH) was developed as an alternative to urinary-derived FSH, allowing for greater availability, decreased variability, and possibly reduced risk of immunological reactions during infertility treatment [1,2,3]. Comparable effectiveness and safety of r-hFSH vs urinary gonadotropins have been demonstrated [4].
Ovaleap® (follitropin alfa, Theramex UK Ltd) is an r-hFSH developed as a biosimilar to Gonal-f®, administered subcutaneously by the use of a multidose, reusable, semi-automated pen injector and approved by the European Medicines Agency (EMA) in 2013 [5]. Ovaleap® is indicated for OS in women receiving ART, as well as for treatment of anovulation associated with polycystic ovary syndrome (PCOS) or hypogonadal hypogonadism and stimulation of spermatogenesis. To meet the requirements of a biosimilar [6, 7], similarity of Ovaleap® to Gonal-f® was demonstrated in comprehensive comparability studies of their physicochemical and biological characteristics, as well as efficacy, and safety [8,9,10]. These comparability studies demonstrate that a biosimilar r-hFSH and the corresponding reference biologic (Gonal-f®) share essentially the same active pharmaceutical ingredient (follitropin alfa) [9]. Ovaleap® demonstrated therapeutic equivalence to Gonal-f® for stimulating follicular development in a phase 3 multinational, multicenter, randomized, active-controlled, comparative study of infertile women using ART [11]. The study demonstrated that patients receiving Ovaleap® or Gonal-f® were equivalent in number of retrieved oocytes, the primary endpoint recommended by the EMA for evaluating clinical comparability [7], and showed comparable secondary efficacy and safety profiles following OS using a long GnRH agonist protocol. Safety and efficacy of Ovaleap® treatment were further demonstrated in an open-label, follow-up study of these patients with up to 2 additional Ovaleap® treatment cycles (in total 207 cycles) with a GnRH agonist [12].
Reports from clinicians within an IVF-Worldwide web-based survey indicated that while 67.3% reported awareness of biosimilar r-hFSH products, only 25.6% had experience with biosimilar products and 92% indicated they would like more information on these products [13]. One clinically relevant approach to providing more information is the examination of effectiveness and safety within real-world, routine clinical practice. The real-world effectiveness of Ovaleap® has not previously been evaluated, nor the effectiveness and safety of Ovaleap® treatment used with a GnRH antagonist protocol. GnRH antagonist vs long agonist protocols for ART have been examined for efficacy and safety outcomes with support for lower incidence of ovarian hyperstimulation syndrome (OHSS) with GnRH antagonist protocols [14,15,16].
The objective of this current multicenter, prospective, non-interventional study was to examine effectiveness of OS with Ovaleap® for routine in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI) in real-world ART clinical practice using a GnRH antagonist protocol. The primary endpoints examined were number of retrieved oocytes and clinical pregnancy rate (CPR). Safety and user satisfaction with the Ovaleap® reusable semi-automated pen were also evaluated.
Methods
Study design and population
The study was a multicenter, prospective, open, non-interventional study that initially included 34 specialized reproductive medicine centers in Germany; the final number included in the present analysis was 33, due to one center not being able to participate. The study was conducted in accordance with Section 4 (paragraph 23, sentence 3) and Section 67 (paragraph 6) of the German Medicines Act (“Arzneimittelgesetz” – AMG) [17]. The protocol (XM17-WH-40103) was registered on ClinicalTrials.gov (ClinicalTrials.gov identifier: NCT02809989) and the publicly available register for non-interventional studies at the German Association of Research-Based Pharmaceutical Companies (Verband Forschender Arzneimittelhersteller e.V. [http://www.vfa.de/de/forschung/nisdb/]). It was reviewed by the appropriate ethics committees. Patients provided written informed consent prior to study participation and enrollment began March 2016 and ended May 2017.
To determine the number of patients to enroll, a sample size calculation was carried out based upon the estimated pregnancy rate from national data. It could be estimated that a study size of 400 women would be sufficient. This was carried out using PASS 11 software.
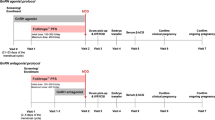
Study visits included information at screening and assessment at baseline (Visit 1), final maturation trigger, oocyte retrieval and embryo transfer (Visit 2), and the clinical pregnancy examination (Visit 3). Visit 2 involved multiple components, and patients who completed Visit 2 may not necessarily have had an embryo transfer. The observation period lasted approximately 6 to 8 weeks from the start of stimulation therapy. Patients with a sonographically verified intrauterine pregnancy (fetal heart and sac) were followed up until the end of the pregnancy or delivery of the baby/babies.
Patients eligible for inclusion were women undergoing IVF or ICSI following OS with Ovaleap® during routine ART and using a GnRH antagonist protocol. Duration of treatment was for one stimulation cycle. Inclusion criteria included patients age 18 to 40 years old, with body mass index (BMI) < 30 kg/m2, menstrual cycle duration 24 to 35 days, and anti-Müllerian hormone (AMH) ≥1 ng/mL (assessed within the previous 12 months), who were undergoing a first stimulation cycle for ART. Women with PCOS, endometriosis (American Fertility Society grades 3 and 4), uterine myoma (intramural > 4 cm, submucosal), or hydrosalpinx were excluded. Also excluded were women receiving combined application of IVF and ICSI or OS for fertility preservation.
Treatment
The decision to treat a patient with Ovaleap® was made separately from the decision to include the patient in the study. As a first step and prior to patient assessment, the participating physicians were free to choose the stimulation drug and the protocol according to their experiences and preferences. If a physician chose to treat her/his patient with Ovaleap® in an antagonist protocol she/he then screened the patient and checked for inclusion/exclusion criteria as a second step. If the patient fulfilled the criteria and was willing to participate, she was finally eligible to be included in the study. FSH treatment, administered subcutaneously daily, typically began on the second or third day of the menstrual cycle, with the duration and dosage at the discretion of the physician. Dosage was adjusted according to ovarian response and continued until sufficient development of follicles (as indicated by serum estrogen and/or ultrasound examination and local practice). Suppression of an endogenous LH surge was achieved by a GnRH antagonist. Type of GnRH antagonist and type of oocyte maturation trigger were at the discretion of the treating physician. For final oocyte maturation and timing of oocyte retrieval, a single dose of recombinant human chorionic gonadotropin (r-hCG), urinary hCG was administered, or alternatively a GnRH agonist.
Study assessments
The primary effectiveness endpoints included number of oocytes retrieved and CPR. Secondary effectiveness endpoints included total dose and administration duration of r-hFSH, serum estradiol level at the time of last examination prior to oocyte maturation trigger, endometrial thickness at the time of last sonography prior to trigger, drugs used for final oocyte maturation and timing oocyte retrieval, number of metaphase-II (MII) oocytes, percentage fertilization rate after IVF or ICSI, day of ovum pick-up (OPU), number of transferred embryos, and live birth delivery rate.
Safety and tolerability were examined by frequency and intensity (mild, moderate, severe) of adverse drug reactions (ADRs), defined as adverse events with an at least suspected relationship with Ovaleap®, including non-serious and serious ADRs. Frequency and intensity of OHSS were assessed at the discretion of the reporting physician.
Patient-reported outcomes for satisfaction with the Ovaleap® reusable semi-automated pen were evaluated with a previously described 7-question questionnaire [12, 18] after completion of FSH treatment (see Additional file 1; the document is available only in German language).
Data analysis
The total treated population (TTP) included all patients who received at least 1 administration of Ovaleap®. The per protocol population (PPP) included all patients who received at least 1 administration of Ovaleap®, completed through to embryo transfer day (although did not necessarily have embryo transfer) and adhered to all study documentation criteria. Patients in whom all fertilized or unfertilized oocytes were frozen after OPU were not evaluated further. The planned analyses assessed outcomes using descriptive statistics (e.g., mean ± SD, median, range, percentages). A multivariate general linear model (GLM) analysis was performed to examine the effect of age (< 35 vs ≥35 years old), AMH level (≤2.5 ng/mL vs > 2.5 ng/mL), FSH total stimulation dose (≤1500 IU vs > 1500 IU), and FSH treatment duration (≤9 days vs > 9 days) on number of retrieved oocytes in PPP patients. The safety analysis included TTP patients. SAS version 9.4 was used for all statistical analyses.
Results
Of the 507 women who were screened for enrollment in the study, 463 received at least 1 dose of FSH (TTP group) and 439 had Visit 2 data (PPP group) (Figure S1) (see Additional file 2). Among the PPP group, 56 women did not undergo an embryo transfer. Of these, the most frequent cause was a freeze-all intervention (24/56; 43%), followed by failed fertilization after either IVF/ICSI or degeneration of embryos (19/56; 34%), and no oocytes retrieved due to poor response or failed retrieval (13/56; 23%).
Demographic and baseline characteristics are shown in Table 1.
Effectiveness outcomes
Number of oocytes retrieved
Mean numbers of retrieved oocytes were 11.8 in PPP patients, 12.1 in the subset of women undergoing ICSI, and 11.5 in the subset of women receiving IVF (Table 2). As expected, the number of oocytes retrieved decreased with age (Fig. 1). The multivariate GLM analysis found age ≥ 35 years and AMH ≤2.5 ng/mL were significantly associated with fewer oocytes retrieved (P = .0285 and P < .0001, respectively) in PPP patients.

Number of retrieved oocytes by age in patients in the per protocol population
Clinical pregnancy
Overall, CPR per cycle was 35.6% (165/463) and 36.0% (158/439) in the TTP and PPP groups, respectively; CPR per embryo transfer was 41.4% (165/399) and 41.3% (158/383) in women with embryo transfer in the TTP and PPP groups, respectively (Table 2).
Secondary effectiveness outcomes
The mean number of MII oocytes was 9.2 (Table 2). Overall, fertilization rate was 68.3% (ICSI 69.6%; IVF 63.8%). The mean number of transferred embryos was 1.8. There were 138 live births in the PPP group who provided follow-up information (n = 437); thus, the live birth delivery rate was 31.6% (138/437) among patients with available follow-up information.
Safety and tolerability
The overall frequency of ADRs was low (Table 3). OHSS was the most frequently reported non-serious ADR (16/463; 3.5%) and OHSS (7/463, 1.5%) and miscarriage (10/463, 2.2%) were the most frequently reported serious ADRs. There was 1 ectopic pregnancy.
Overall, OHSS was classified as mild (14/463, 3.0%), moderate (8/463, 1.7%), or severe (1/463, 0.2%). No cases of life-threatening OHSS were reported. The majority of patients (17/23; 73.9%), experiencing OHSS had AMH levels > 3.5 ng/mL.
Patient-reported outcomes of pen use
Patients reported high levels of both user satisfaction and convenience with the Ovaleap® pen (full data not shown). In the PPP, 97.4% of patients reported they were sure or very sure about adjusting the daily dose of the drug, and 96.9% were sure or very sure that they had injected the correct dose. Instructional text was rated as easy or very easy to understand by 96.0% of women. Being satisfied or very satisfied with the Ovaleap® pen was reported by 99.8% of women, and the Ovaleap® pen was reported as convenient or very convenient to use by 99.0% of women.
Discussion
This prospective, multicenter, non-interventional study extends the knowledge of the effectiveness of Ovaleap®, to a broader population of women, undergoing routine IVF/ICSI treatment, with a GnRH antagonist protocol. In the 2017 German IVF-Registry (DIR) annual report, 64.2% of patients received GnRH antagonist therapy, compared to 18.5% who received long GnRH agonist treatment overall [19]. Compared to long-term treatment with GnRH agonists, GnRH antagonist treatment is shorter, requires less FSH stimulation and fewer injections [14, 15], and is associated with a decreased risk of OHSS [16]. In poor responders and patients with PCOS, GnRH antagonist therapy has been proposed to be the first treatment protocol option [20]; however, a recent review article has also stated that a long GnRH agonist protocol is still applicable for poor responders [21].
The patient population studied here, based on mean age, is representative of the 30–34 year age range reported in 2018 DIR annual report, the most recent comprehensive analysis of trends in German IVF practice. This age range accounts for 30% of all oocyte retrievals done in Germany [22]. Amongst those patients aged 30–34 years in the 2018 report, the mean number of oocytes retrieved (IVF, 10.5; ICSI, 11.1) and CPR after embryo transfer (IVF, 40.0%; ICSI, 39.6%) are comparable to the findings presented here [22].
Additionally, in this non-interventional study of GnRH antagonist treatment, the primary endpoints of number of oocytes retrieved and CPR compared favorably with previous studies using a GnRH agonist protocol and in women of < 35 years old [11]. Other secondary endpoints associated with FSH drug usage were also similar [11]. OHSS was also comparable among the current non-interventional and the prior phase 3 comparative and open-label follow-up Ovaleap® studies [11]. Additionally, large multicenter studies of women with a similar age range as here, such as the Menopur in GnRH Antagonist Cycles with Single Embryo Transfer (MEGASET) study [23] using follitropin beta, reported 1.6% early-onset moderate/severe OHSS compared to here overall 1.9% moderate/severe OHSS with Ovaleap®, and in the recent Evidence-based Stimulation Trial with Human rFSH in Europe and Rest of World (ESTHER-1), utilizing follitropin delta and comparing to follitropin alfa in a GnRH antagonist protocol, the overall incidence of moderate/severe OHSS for follitropin alfa was 2.9% [24].
The primary endpoints in the current study are also comparable to previous randomized comparative r-hFSH studies examining follitropin alfa (Gonal-f®) [25,26,27,28,29], follitropin beta (Puregon®) [30] and more recent trials evaluating another biosimilar follitropin alfa [31] as well as follitropin delta [24]. In the analysis of the MEGASET study, follitropin beta was found to have comparable pregnancy and cumulative live birth rates when compared to menotropin (27% vs 30 and 38% vs 40%, respectively) [23]. Similarly, a study of 1050 Danish women found that treatment with GnRH antagonist or a GnRH agonist regimen resulted in comparable cumulative live birth rates, despite more oocytes being retrieved with the GnRH agonist protocol [32].
Comparison of the current non-interventional study’s number of retrieved oocytes (mean, 11.8) and CPRs among patients with embryo transfer (41.3%) with those of an observational, non-interventional study evaluating dosing regimens of follitropin alfa (Gonal-f®) in routine clinical practice demonstrated similar number of oocytes retrieved (11.4 ± 6.7) and CPRs (39.5%) [33]. Altogether, across study comparisons, the effectiveness of follitropin alfa (Ovaleap®) for OS during routine clinical practice using a GnRH antagonist protocol is supported.
Number of retrieved oocytes is a valuable primary endpoint as it has been associated with live birth rate [34, 35] and is not influenced by factors outside of r-hFSH stimulation in the manner that live birth rate may be influenced by other ART treatment factors (such as laboratory procedures, type of embryo transfer, regional policies of embryo transfer, differences in luteal phase support) [36]. The association with ongoing pregnancy and live birth rates is due to the availability of more oocytes rather than differences in oocyte quality [37, 38]. Notably, the live birth delivery rate achieved with Ovaleap® reported in our patient group of women with good prognostic factors (31.6% of the PPP among patients with available follow-up information) corresponds well to the birth rate in an “ideal” patient group (i.e. age < 36 years, at least 4 fertilized oocytes, fresh transfer on day 5, first or second IVF/ICSI cycle) receiving 2 embryos after IVF or ICSI in Germany from the 2016 DIR registry (32.0%) [19].
In view of the estimated global need for ART (≥1500 cycles/million population per year) [39], there is substantial need for infertility treatment options that are convenient, have high satisfaction and reduced burden, and possibly lower financial burden through expanded availability and healthcare options. In particular, the convenience, satisfaction, confidence in accurate dosing, and ease of use of the controlled OS device for treatment administration may play an important role in reducing ART treatment burden, which may improve patient treatment continuation [40,41,42]. Consistent with previous patient reports of the usability of the Ovaleap® pen [11, 12], almost all patients in the current study of Ovaleap® treatment during routine clinical practice rated the Ovaleap® pen with high satisfaction and high convenience, ease of use, and confidence in accuracy of dosing. These characteristics are consistent with expressed patient preferences during infertility treatment and may be helpful in reducing psychological stress and possibly improving treatment outcomes [43, 44].
Limitations of the current study are those associated with observational, non-interventional studies, including lack of randomization or controlled comparison, possible selection bias in the treated patients, and dependence on accurate reporting from the treating physicians. Strengths of the current study include the large patient sample, inclusion of a broader population of infertile women who may be more representative of the general population seeking ART treatment compared with the highly selected participants in randomized controlled trials, and greater representation of routine clinical practice in which treatment decisions are at the discretion of the treating physician. This approach has been advocated in order to provide clinical insights on newly introduced stimulation agents [45]. Altogether, the study findings of effectiveness, safety, and patient satisfaction with Ovaleap® treatment support Ovaleap® as a treatment option for women undergoing controlled OS for ART in routine clinical practice.
Conclusions
Effectiveness, safety, and high user satisfaction with controlled OS with the Ovaleap® pen were extended to real-world ART clinical practice, including IVF and ICSI treatment, using a GnRH antagonist protocol. The real-world outcomes of this multicenter, prospective, open-label, non-interventional study are consistent with those previously reported in randomized controlled clinical trials.
Availability of data and materials
The study was registered on 22 June 2016 (retrospectively registered) at ClinicalTrials.gov (NCT02809989), https://clinicaltrials.gov/ct2/show/NCT02809989. Study documents and individual participant data have not been shared.
Abbreviations
- ADR:
-
Adverse drug reaction
- AMH:
-
Anti-Müllerian hormone
- ART:
-
Assisted reproductive technology
- BMI:
-
Body mass index
- CPR:
-
Clinical pregnancy rate
- EMA:
-
European Medicines Agency
- GLM:
-
General linear model
- GnRH:
-
Gonadotropin releasing hormone
- ICSI:
-
Intracytoplasmic sperm injection
- IVF:
-
in vitro fertilization
- MII:
-
Metaphase-II
- OHSS:
-
Ovarian hyperstimulation syndrome
- OPU:
-
Ovum pick-up
- OS:
-
Ovarian stimulation
- PCOS:
-
Polycystic ovary syndrome
- PPP:
-
Per protocol population
- r-hCG:
-
recombinant human chorionic gonadotropin
- r-hFSH:
-
Recombinant human follicle-stimulating hormone
- TTP:
-
Total treated population
References
Howles CM. Recombinant gonadotrophins in reproductive medicine: the gold standard of today. Reprod BioMed Online. 2006;12:11–3.
Howles CM. Genetic engineering of human FSH (Gonal-F®). Hum Reprod Update. 1996;2:172–91.
Harrison S, Wolf T, Abuzeid MI. Administration of recombinant follicle stimulating hormone in a woman with allergic reaction to menotropin: a case report. Gynecol Endocrinol. 2000;14:149–52.
van Wely M, Kwan I, Burt AL, Thomas J, Vail A, Van der Veen F, Al-Inany HG. Recombinant versus urinary gonadotrophin for ovarian stimulation in assisted reproductive technology cycles. Cochrane Database Syst Rev. 2011;2:cd005354.
European Medicines Agency. Ovaleap (follitropin alfa) [assessment report]. 31 July 2013. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002608/WC500152908.pdf. Accessed 31 Jan 2020.
Weise M, Bielsky MC, De Smet K, Ehmann F, Ekman N, Narayanan G, Heim HK, Heinonen E, Ho K, Thorpe R, et al. Biosimilars-why terminology matters. Nat Biotechnol. 2011;29:690–3.
European Medicines Agency Committee for Medical Products for Human Use. Guideline on non-clinical and clinical development of similar biological medicinal products containing recombinant human follicle stimulating hormone (r-hFSH). 21 February 2013. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2013/03/WC500139624.pdf. Accessed 31 Jan 2020.
Winstel R, Wieland J, Gertz B, Mueller A, Allgaier H. Manufacturing of recombinant human follicle-stimulating hormone Ovaleap® (XM17), comparability with Gonal-f®, and performance/consistency. Drugs R D. 2017;17:305–12.
de Mora F, Fauser B. Biosimilars to recombinant human FSH medicines: comparable efficacy and safety to the original biologic. Reprod BioMed Online. 2017;35:81–6.
Bosch E, Howles C. No difference in clinical outcomes using follitropin alfa (biosimilar) compared to follitropin alfa or follitropin beta for controlled ovarian stimulation (cos) in oocyte donation-recipient cycles [abstract]. Fertil Steril. 2018;110(4 suppl):e336.
Strowitzki T, Kuczynski W, Mueller A, Bias P. Randomized, active-controlled, comparative phase 3 efficacy and safety equivalence trial of Ovaleap® (recombinant human follicle-stimulating hormone) in infertile women using assisted reproduction technology (ART). Reprod Biol Endocrinol. 2016;14:1.
Strowitzki T, Kuczynski W, Mueller A, Bias P. Safety and efficacy of Ovaleap® (recombinant human follicle-stimulating hormone) for up to 3 cycles in infertile women using assisted reproductive technology: a phase 3 open-label follow-up to main study. Reprod Biol Endocrinol. 2016;14:31.
Christianson MS, Shoham G, Tobler KJ, Zhao Y, Monseur B, Leong M, Shoham Z. Use of various gonadotropin and biosimilar formulations for in vitro fertilization cycles: results of a worldwide web-based survey. J Assist Reprod Genet. 2017;34:1059–66.
Al-Inany HG, Youssef MA, Ayeleke RO, Brown J, Lam WS, Broekmans FJ. Gonadotrophin-releasing hormone antagonists for assisted reproductive technology. Cochrane Database Syst Rev. 2016;4:CD001750.
Wang R, Lin S, Wang Y, Qian W, Zhou L. Comparisons of GnRH antagonist protocol versus GnRH agonist long protocol in patients with normal ovarian reserve: a systematic review and meta-analysis. PLoS One. 2017;12:e0175985.
Toftager M, Bogstad J, Bryndorf T, Lossl K, Roskaer J, Holland T, Praetorius L, Zedeler A, Nilas L, Pinborg A. Risk of severe ovarian hyperstimulation syndrome in GnRH antagonist versus GnRH agonist protocol: RCT including 1050 first IVF/ICSI cycles. Hum Reprod. 2016;31:1253–64.
German Federal Ministry of Justice and Consumer Protection. Medicinal Products Act (Arzneimittelgesetz – AMG), 12 December 2005. Federal Law Gazette Part I, p.3394. Updated 4 April 2016 (Federal Law Gazette I p. 569). Available at: https://www.gesetze-im-internet.de/englisch_amg/englisch_amg.html. Accessed 31 Jan 2020.
Somkuti SG, Schertz JC, Moore M, Ferrande L, Kelly E. Gonal-F prefilled pen in OI study 24785 group. Patient experience with follitropin alfa prefilled pen versus previously used injectable gonadotropins for ovulation induction in oligoanovulatory women. Curr Med Res Opin. 2006;22:1981–96.
Blumenauer V, Czeromin U, Fehr D, Fiedler K, Gnoth C, Krussel JS, Kupka MS, Ott A, Tandler-Schneider A. Deutsches IVF Register (DIR) Annual 2017. J Reproduktionsmed Endokrinol. 2018;15:216–49 Available at: https://www.deutsches-ivf-register.de/perch/resources/dir-annual-2017-english-final-190320.pdf and https://www.deutsches-ivf-register.de/perch/resources/dir-jahrbuch-2017-deutsch-final-4.pdf.
Lambalk CB, Banga FR, Huirne JA, Toftager M, Pinborg A, Homburg R, van der Veen F, van Wely M. GnRH antagonist versus long agonist protocols in IVF: a systematic review and meta-analysis accounting for patient type. Hum Reprod Update. 2017;23:560–79.
Haahr T, Dosouto C, Alviggi C, Esteves SC, Humaidan P, et al. Front Endocrinol (Lausanne). 2019;10:614.
D·I·R Deutsches IVF-Register (D·I·R). Kurz und knapp – Die Jahre 2017 und 2018 im Deutschen IVF-Register (D·I·R) [Article in German]. J Reproduktionsmed Endokrinol. 2019;16(6) Available at: https://www.deutsches-ivf-register.de/jahrbuch.php. Accessed 31 Jan 2020.
Devroey P, Pellicer A, Nyboe Andersen A, Arce JC, Menopur in GnRH Antagonist Cycles with Single Embryo Transfer Trial Group. A randomized assessor-blind trial comparing highly purified hMG and recombinant FSH in a GnRH antagonist cycle with compulsory single-blastocyst transfer. Fertil Steril. 2012;97:561–71.
Nyboe Andersen A, Nelson SM, Fauser BC, Garcia-Velasco JA, Klein BM, Arce JC. Individualized versus conventional ovarian stimulation for in vitro fertilization: a multicenter, randomized, controlled, assessor-blinded, phase 3 noninferiority trial. Fertil Steril. 2017;107:387–96 e4.
Andersen AN, Devroey P, Arce JC. Clinical outcome following stimulation with highly purified hMG or recombinant FSH in patients undergoing IVF: a randomized assessor-blind controlled trial. Hum Reprod. 2006;21:3217–27.
European and Israeli Study Group on Highly Purified Menotropin versus Recombinant Follicle-Stimulating Hormone. Efficacy and safety of highly purified menotropin versus recombinant follicle-stimulating hormone in in vitro fertilization/intracytoplasmic sperm injection cycles: a randomized, comparative trial. Fertil Steril. 2002;78:520–8.
Frydman R, Howles CM, Truong F. A double-blind, randomized study to compare recombinant human follicle stimulating hormone (FSH; Gonal-F) with highly purified urinary FSH (Metrodin HP) in women undergoing assisted reproductive techniques including intracytoplasmic sperm injection. The French Multicentre Trialists. Hum Reprod. 2000;15:520–5.
Schats R, Sutter PD, Bassil S, Kremer JA, Tournaye H, Donnez J. Ovarian stimulation during assisted reproduction treatment: a comparison of recombinant and highly purified urinary human FSH. On behalf of the Feronia and Apis study group. Hum Reprod. 2000;15:1691–7.
Westergaard LG, Erb K, Laursen SB, Rex S, Rasmussen PE. Human menopausal gonadotropin versus recombinant follicle-stimulating hormone in normogonadotropic women down-regulated with a gonadotropin-releasing hormone agonist who were undergoing in vitro fertilization and intracytoplasmic sperm injection: a prospective randomized study. Fertil Steril. 2001;76:543–9.
The Latin-American Puregon IVF Study Group. A double-blind clinical trial comparing a fixed daily dose of 150 and 250 IU of recombinant follicle-stimulating hormone in women undergoing in vitro fertilization. Fertil Steril. 2001;76:950–6.
Rettenbacher M, Andersen AN, Garcia-Velasco JA, Sator M, Barri P, Lindenberg S, van der Ven K, Khalaf Y, Bentin-Ley U, Obruca A, et al. A multi-Centre phase 3 study comparing efficacy and safety of Bemfola® versus Gonal-f® in women undergoing ovarian stimulation for IVF. Reprod BioMed Online. 2015;30:504–13.
Toftager M, Bogstad J, Lossl K, Praetorius L, Zedeler A, Bryndorf T, Nilas L, Pinborg A. Cumulative live birth rates after one ART cycle including all subsequent frozen-thaw cycles in 1050 women: secondary outcome of an RCT comparing GnRH-antagonist and GnRH-agonist protocols. Hum Reprod. 2017;32:556–67.
Naether OG, Tandler-Schneider A, Bilger W. Individualized recombinant human follicle-stimulating hormone dosing using the CONSORT calculator in assisted reproductive technology: a large, multicenter, observational study of routine clinical practice. Drug Healthc Patient Saf. 2015;7:69–76.
Polyzos NP, Drakopoulos P, Parra J, Pellicer A, Santos-Ribeiro S, Tournaye H, Bosch E, Garcia-Velasco J. Cumulative live birth rates according to the number of oocytes retrieved after the first ovarian stimulation for in vitro fertilization/intracytoplasmic sperm injection: a multicenter multinational analysis including approximately 15,000 women. Fertil Steril. 2018;110:661–70 e1.
Drakopoulos P, Blockeel C, Stoop D, Camus M, de Vos M, Tournaye H, Polyzos NP. Conventional ovarian stimulation and single embryo transfer for IVF/ICSI. How many oocytes do we need to maximize cumulative live birth rates after utilization of all fresh and frozen embryos? Hum Reprod. 2016;31:370–6.
Howles CM. The development of ovarian stimulation for IVF. In: Kovacs G, Brinsden PR, DeCherney AH, editors. In-vitro fertilization: the pioneers' history (Chapter 25). Cambridge: Cambridge University Press; 2018. p. 202–7.
Reichman DE, Goldschlag D, Rosenwaks Z. Value of antimullerian hormone as a prognostic indicator of in vitro fertilization outcome. Fertil Steril. 2014;101:1012–8 e1.
Arce JC, La Marca A, Mirner Klein B, Nyboe Andersen A, Fleming R. Antimullerian hormone in gonadotropin releasing-hormone antagonist cycles: prediction of ovarian response and cumulative treatment outcome in good-prognosis patients. Fertil Steril. 2013;99:1644–53.
European Society of Human Reproduction and Embryology. ART fact sheet. Last updated: 18 February 2018. Available at: https://www.eshre.eu/Press-Room/Resources.aspx. Accessed 31 Jan 2020.
Boivin J, Domar AD, Shapiro DB, Wischmann TH, Fauser BC, Verhaak C. Tackling burden in ART: an integrated approach for medical staff. Hum Reprod. 2012;27:941–50.
Brandes M, van der Steen JO, Bokdam SB, Hamilton CJ, de Bruin JP, Nelen WL, Kremer JA. When and why do subfertile couples discontinue their fertility care? A longitudinal cohort study in a secondary care subfertility population. Hum Reprod. 2009;24:3127–35.
Verberg MF, Eijkemans MJ, Heijnen EM, Broekmans FJ, de Klerk C, Fauser BC, Macklon NS. Why do couples drop-out from IVF treatment? A prospective cohort study. Hum Reprod. 2008;23:2050–5.
Buhler K. Managing infertility with the follitropin alfa prefilled pen injector - patient considerations. Ther Clin Risk Manag. 2015;11:995–1001.
Landfeldt E, Jablonowska B, Norlander E, Persdotter-Eberg K, Thurin-Kjellberg A, Wramsby M, Strom O. Patient preferences for characteristics differentiating ovarian stimulation treatments. Hum Reprod. 2012;27:760–9.
Bühler K, Naether O. A 2:1 formulation of follitropin alfa and lutropin alfa in routine clinical practice: a large, multicentre, observational study. Gynecol Endocrinol. 2011;27:650–4.
Acknowledgements
The authors thank Lynanne McGuire, PhD, CMPP, and Meghan Sullivan, PhD, of MedVal Scientific Information Services, LLC, Princeton, NJ, and Colin M Howles PhD, ARIES Consulting, Geneva Switzerland for providing medical writing and editorial assistance. This manuscript was prepared according to the International Society for Medical Publication Professionals’ “Good Publication Practice for Communicating Company-Sponsored Medical Research: the GPP3 Guidelines”.
Funding
This study was supported by Teva GmbH Germany. Medical writing assistance was funded by Teva GmbH Germany, Teva Branded Pharmaceutical Products R&D, Inc. (Frazer, PA) and Theramex HQ UK Ltd. Teva and Theramex provided a full review of the article.
Author information
Authors and Affiliations
Contributions
All authors contributed to the preparation of the manuscript and meet ICMJE Uniform Requirements for manuscripts submitted to biomedical journals. PS, CK, KP and IW contributed to the study design, and PS and IW treated patients in the study. NG was responsible for study implementation and data collection. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was reviewed by the appropriate ethics committees. Patients provided written informed consent prior to study participation.
Consent for publication
Not applicable.
Competing interests
PS: Received honoraria for consultancy, presentations, and involvement in clinical studies from Teva, Merck, and Ferring.
NG: Received personal fees from Pharmalog Institut für klinische Forschung GmbH, subcontracted service CRO of Teva GmbH Germany for this non-interventional study.
KP: Received honoraria for consultancy, presentations and involvement in clinical studies from Teva GmbH Germany/Pharmalog Institut für klinische Forschung GmbH.
CK: Received honoraria for consultancy and presentations from Teva GmbH Germany, Kade, Gedeon Richter, Exeltis, Merck Serono, Theramex.
IW: Received honoraria for consultancy, presentations, and involvement in clinical studies from Teva, Merck, Ferring, Theramex, MSD, Pharmalog.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Patient satisfaction questionnaire.
Additional file 2.
Patient disposition.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sydow, P., Gmeinwieser, N., Pribbernow, K. et al. Effectiveness and safety of follitropin alfa (Ovaleap®) for ovarian stimulation using a GnRH antagonist protocol in real-world clinical practice: a multicenter, prospective, open, non-interventional assisted reproductive technology study. Reprod Biol Endocrinol 18, 54 (2020). https://doi.org/10.1186/s12958-020-00610-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12958-020-00610-2