
Abstract
Background
To describe the pathological distribution, imaging manifestations, and surgical managements and prognosis of large adrenal tumors (LATs) ≥ 5 cm
Methods
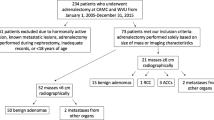
A total of 251 patients with LATs were analyzed on the basis of pathological or clinical diagnosis. Regarding surgery, open adrenalectomy was performed on 89 patients, and laparoscopic adrenalectomy was performed on 89 patients. Thirty-two patients with bilateral tumors were analyzed in terms of clinical characteristics. The survival rate was determined for 43 patients with adrenal metastases and 29 patients with primary adrenal malignancies. The CT characteristics including tumor diameter, shape, edge, heterogeneity, necrosis, calcification, pre-contrast attenuation, and contrast attenuation were analyzed for 117 patients.
Results
The majority of LATs were still benign, but they had a higher probability to be malignant. Benign LATs made up 68.13% of all cases, mainly adrenal cysts (19.52%), pheochromocytoma (18.73%), benign adenoma (16.73%), and myelolipoma (7.17%). Malignant LATs accounted for 28.69% of cases, mainly including adrenocortical carcinoma (8.76%) and metastases (17.13%). Laparoscopic surgery was found to involve less trauma than open surgery. It was also safer and postoperative recovery was faster, but it had drawbacks and could not completely replace open surgery. CT features had obvious specificity for the diagnosis of benign and malignant tumors. For example, benign adenomas had a smaller pre-contrast (< 10 Hu) whereas malignant adrenal tumors had, on the contrary, higher attenuation. Regarding adrenal malignant carcinoma, adrenal primary malignant tumors showed a better prognosis than adrenal metastases (mean survival of 19.17 months vs 9.49 months). Primary adrenal cortical carcinoma without metastasis had a better prognosis than primary adrenal cortical carcinoma metastasis (mean survival of 23.71 months vs 12.75 months), and adrenal solitary metastasis had a better prognosis than general multiple metastatic carcinoma (mean survival of 14.95 months vs 5.17 months).
Conclusion
LATs were more likely to be benign; however, they still had a high probability of being a malignant tumor. Understanding the clinicopathological characteristics of LATs can facilitate selection of more effective clinical treatment options.
Similar content being viewed by others


Background
With the development of imaging technology, there is an increasing number of adrenal incidentalomas discovered incidentally. However, large adrenal tumors (LATs) are considered uncommon, with an incidence ranging from 8.6 to 38.6% [1, 2]. The possibility of malignancy increases with the increasing tumor volume [3,4,5,6]. For LATs, accurate preoperative assessments of the nature and origin of the tumors are important to the choice of therapy [7,8,9].
By definition, LATs range in size from more than 5 to 10 cm in diameter, with a consensus of approximately 5 cm [3, 10]. LATs cover a spectrum of various pathologies, ranging from benign lesions to adrenocortical carcinoma or metastasis. Among 19 histopathological diagnoses, the most common was found to be adrenal cancer, followed by benign adenomas, pheochromocytomas, and metastasis [3]. The prognosis of different pathological types of LATs was found to differ. Patients with malignant tumors exhibited poor prognosis, especially those with adrenal metastasis [11]. Accurate diagnosis and functional evaluation of LATs and preoperative differentiation of benign and malignant tumors have great significance for the selection of appropriate treatment approaches. Functional adrenal tumors and local invading lesions require more preoperative preparation [3] and may even affect the choice of surgical approach [7]. Because the possibility of an uncomplete curative resection with the laparoscopic adrenalectomy, open adrenalectomy is indicated in some cases [12]. The clinical, imaging, and pathological features of LATs play an important role in preoperative judgment of the nature of each tumor and selection of the best treatment.
In the present study, the clinical data of 251 patients with LATs in our hospital during a 10-year period from 2009 to 2018, including the pathological distribution, imaging manifestations, and surgical managements and prognosis, were collected and analyzed to provide a basis for the treatment of LATs.
Methods
From January 2009 to August 2018, among the patients admitted to the First Affiliated Hospital of Dalian Medical University, 1160 showed adrenal tumors in imaging reports. In this group, a total of 251 patients who had imaging manifestations showing that the size of adrenal tumors was larger than or equal to 5 cm were identified. Patient information (age, sex, survival time), laboratory work-up (blood cortisol, blood aldosterone, ACTH), tumor character (pathological diagnosis, imaging manifestations, lesion location, diameter), and information related to the operation (surgical methods, bleeding volume, blood transfusion volume, operation time, drainage time, hospitalization time) were collected. All patients with a preoperative diagnosis of pheochromocytoma received specific preparations to control hypertension and facilitate rehydration. Most of these preparations included α receptor blockers and equilibrium salt solution.
Among these patients, 178 underwent urological surgery. The typical surgical management plans were laparoscopic adrenalectomy and open adrenalectomy. Eighty-nine patients underwent open adrenalectomy. Laparoscopic adrenalectomy was performed in 89 patients. Seventy-three patients did not undergo surgery, and clinical doctors made clinical diagnoses based on thorough history, clinical evaluation, hormonal and biochemical workup, and imaging reports.
The survival rates of 43 patients with adrenal metastasis and 29 patients with primary adrenal malignancies were determined according to the follow-up by phone. Two-month, 6-month, 12-month, 24-month, and 30-month survival rates were analyzed.
CT images of 117 patients with benign adenoma, pheochromocytoma, cortical carcinoma, metastatic carcinoma, and gangliocytoma were collected. The CT characteristics including tumor diameter, shape, edge, heterogeneity, necrosis, calcification, pre-contrast attenuation, and contrast attenuation of the 117 patients were analyzed.
Statistical analysis
SPSS 21.0 software was used for statistical analysis. In case of skewed distribution and categorical data, rank sum test was used. A P value of < 0.05 was considered statistically significant for all tests.
Results
The pathological distribution of LATs and the characteristics of patients are shown in Table 1. Tumor size measured on histopathological examination or imaging measurement ranges from 50 to 200 mm. The five most common LATs, including adrenal cyst (19.52%), pheochromocytoma (18.73%), metastases (17.13%), benign adenoma (16.73%), and adrenal cortical cancer (8.76%), were responsible for 80.88% of cases in this study. Benign LATs, including adrenal cyst (19.52%), pheochromocytoma (18.73%), benign adenoma (16.73%), myelolipoma (7.17%), gangliocytoma (3.19%), schwannoma (0.8%), teratoma (1.20%), and hemangioma (0.80%), were responsible for 68.13%. Malignant LATs, mainly including metastases (17.13%), cortical carcinoma (8.76%), small cell carcinoma (1.20%), lymphoma (1.20%), and melanoma (0.4%), accounted for 28.69% of all cases.
Some obvious features in certain types of LATs were observed in the present study. The mean age of patients with lymphoma (66.67 years) and metastases (63.91 years) was higher than in other groups. In the case of metastases, the male/female ratio was 34/9, with a higher proportion of males than other groups. In patients with adrenal myelolipoma, most of the lesions were on the right side (R/L = 16:2).
Patients and tumor characteristics of bilateral LATs are shown in Table 2. Among the bilateral LATs, the most common diagnostic was malignant tumor (71.88%), followed by benign adenoma (15.63%), myelolipoma (6.25%), gangliocytoma (3.13%), and pheochromocytoma (3.13%). The most common type of malignant tumor was metastatic (50%), followed by cortical carcinoma (15.63%) and lymphoma (6.25%). Among adrenal metastases, lung cancer was the main source, accounting for 50% of all adrenal metastases. It was followed by kidney cancer (12.5%), intestinal malignancy (12.5%), and prostate cancer (6.26%).
Generally, the prognosis of adrenal malignant tumors was poor (Table 3). Lung cancer was the most common primary carcinoma of adrenal metastasis, of which 41.67% of cases were solitary adrenal metastasis and 58.33% were systemic multiple metastases including adrenal metastasis. The 2-, 6-, 12-, 24-, and 30-month survival rates of patients with lung cancer were 96%, 58%, 33%, 8%, and 4%, respectively. Adrenal cortical carcinoma accounted for 75.86% of the primary adrenal malignancy, 40.91% of which appeared distant metastatic at the time of initial diagnosis. The 2-, 6-, 12-, 24-, and 30-month survival rates of patients with primary adrenal cortical carcinoma were 91%, 64%, 45%, 23%, and 14%, respectively. In this cohort, the mean survival time of primary adrenal malignant tumors was 19.17 months and that of metastatic adrenal tumors was 9.49 months. In general, the prognosis of patients with primary adrenal carcinoma without metastases was relatively good (Figs. 1, 2, 3, and 4).

The survival time of the adrenal malignancy

The survival time of adrenal metastasis of lung cancer and adrenal cortical carcinoma

The survival graphs for adrenal metastases vs primary adrenal carcinoma

The survival graphs for adrenal metastases vs primary adrenal carcinoma without vs with metastases
There was no significant difference between open adrenalectomy and laparoscopic adrenalectomy with respect to gender, age, or tumor location (Table 4). However, tumor diameter was larger in the open adrenalectomy group than in the laparoscopic adrenalectomy group (P < 0.05). There were more benign and nonfunctional LATs in the laparoscopic adrenalectomy group than in the open adrenalectomy group (P < 0.05). Finally, there were significant differences in intraoperative bleeding (251.8 > 63.09 ml), blood transfusion (202.25 > 8.99 ml), operation time (2.35 > 1.96 h), hospitalization time (20.36 > 14.72 days), and postoperative drainage time (5.58 > 3.75 days) between the two groups.
CT features were compared among five types of LATs: benign adenomas, pheochromocytomas, cortical carcinomas, metastatic carcinomas, and gangliocytomas. As shown in Table 5, cortical carcinomas and gangliocytomas had a larger diameter. In terms of tumor shape, a large proportion of benign adenomas and pheochromocytomas were round (94.12%), while metastasis was more common in lobulated tumors (47.06%). Among the infiltrative tumors, there was a high proportion of cortical carcinomas (50%). Benign adenomas (97.06%), pheochromocytomas (94.29%), and gangliocytomas (85.71) were mostly circumscribed, while cortical carcinomas mostly presented ill-defined tumor margins (47.83%). Pheochromocytomas (94.29%), cortical carcinomas (88.89%), and metastatic carcinomas (95.65%) were mostly heterogeneous. However, the majority of gangliocytomas were homogeneous. Ninety-four percent of the pheochromocytomas were accompanied by necrosis, while most of the gangliocytomas had no necrosis. Tumors with calcification were more likely to be benign adenomas, whereas metastatic carcinomas and gangliocytomas had no calcification. CT features had readily visible specificity for the diagnosis of benign and malignant tumors; for example, benign adenomas had a smaller pre-contrast (< 10 Hu) which attenuation of other types of adrenal tumors did not have, whereas the contrast attenuation was more pronounced in pheochromocytoma than in other groups.
Discussion
Adrenal tumors are occasionally found in patients undergoing abdominal radiology, and the prevalence of such findings increased with increasing age [13, 14]. Generally, the larger the tumor, the greater possibility of adrenal cancer [3,4,5,6]; therefore, it was even recommended that a tumor size greater than 5 cm should be considered an additional criterion for surgical treatment of adrenal incidental tumors [15]. For this reason, we decided to analyze tumors of this size to provide experience and basis for preoperative differentiation and selection of appropriate treatment approaches of LATs.
LATs covered a wide range of pathological types. In other studies, benign LATs accounted for 62.59%, and malignant LATs accounted for 37.41% [3]. This is similar to our present study. Thus, in clinical diagnosis of LATs, the possibility of benign tumors should be considered first. However, a LAT still had a high probability of being a malignant tumor.
The presence of bilateral masses accounts for about 15% of the incidental adrenal tumors [16, 17]. In our study, except for malignant lesions, bilateral adrenal adenoma and lymphoma were the most common diagnoses. Metastatic or invasive neoplasms, congenital adrenal cortical hyperplasia, bilateral adrenal cortical adenomas, and ACTH-independent macronodular adrenal hyperplasia were described by certain authors as the most likely diagnosis. Others did not find a difference in the frequency of malignant lesions between patients with bilateral adrenal tumors and unilateral ones [17]. In our group, however, the malignant rate of bilateral adrenal tumor was higher (71.88% vs 22.83%). This difference was caused by the high proportion of metastatic carcinomas. In this way, bilateral LATs should be suspected of malignancy, and further examination should be performed to exclude metastases.
Imaging diagnosis is of great value in estimating the nature of LATs. CT, MRI, and FDG-PET/CT can be used in clinical diagnosis of LATs. We compared the imaging features of the following five common LATs: (1) cortical carcinoma: larger diameter, infiltrative, ill-defined tumor margin, heterogeneous; (2) metastatic carcinoma: lobulated tumors, heterogeneous, few calcifications; (3) benign adenomas: round, circumscribed, calcification; (4) gangliocytoma: larger diameter, circumscribed, homogeneous, no necrosis, few calcifications; and (5) pheochromocytoma: round, circumscribed, heterogeneous, necrosis, higher contrast attenuation.
Other authors described the presence of fat and a pre-contrast attenuation under 10 Hounsfield units have been found to be correlated with benignity [18, 19]. This is in accordance with our present study of LATs where benign adenomas had a pre-contrast attenuation (< 10 Hu) while other types of LATs did not have. Some scholars even thought that lesions with a pre-contrast attenuation of less than 10 Hu may be considered benign regardless of size [20]. However, in patients with adrenal metastases, 7% of cases with noncontrast HU ≤ 10 turned out to be malignant [21]. In our series, metastases had no calcification, which was similar to other studies except one [22]. This shows that CT cannot completely determine the nature of the tumor, and more comprehensive imaging examination was needed. In this case, contrast-enhanced washout CT was able to provide further information, showing that adenomas took up intravenous CT contrast rapidly and had a rapid loss of contrast, whereas malignant adrenal lesions usually became enhanced rapidly but had a slower loss of contrast [23, 24].
Other imaging methods, such as MRI and PET/CT, can further differentiate the benign and malignant adrenal tumors [25, 26]. PET/CT especially might be effective in finding the extra-adrenal malignancies with low uptake [27, 28].
Laparoscopic adrenalectomy is widely used in the world, and it is the first choice for small adrenal benign tumors, on account of its advantages, including reduced postoperative pain, shorter hospitalization and recovery times, reduced complication rates, and better cosmetic results [29]. These advantages of laparoscopic surgery may be related to the small tumor volume and greater number of benign tumors in this group. More prospective clinical studies are needed to compare the safety and efficacy of laparoscopic versus open surgery in the treatment of LATs. With the development of laparoscopic surgery and robotic surgery [30], tumor diameter has ceased to be a limiting factor in the surgical management of adrenal benign tumors. Laparoscopic adrenalectomy is preferred for benign LATs regardless of size or for LATs with radiological findings suspicious of malignancies and a relatively small diameter (according to the experience of the surgeon) but no evidence of local invasion. For malignant LATs, especially those with local invasion, open surgery might be a more reasonable choice. Thus, the selection of surgical method should be evaluated comprehensively according to the experience of the surgeon and the characteristics of the tumor.
Systemic imaging examination before LAT surgery and screening malignant lesions in other parts and selecting suitable treatment for patients were of great significance. Among adrenal malignant tumors, 59.72% were metastatic and 40.28% were primary. Among metastases, 55.81% were accompanied by multiple systemic metastases. At the time of diagnosis of primary adrenal carcinomas, 41.38% of patients had distant metastasis. From our results, both cases of primary adrenal cancer and adrenal metastasis, once accompanied by metastases in other parts of the body, showed poor prognosis. In this case, surgical treatment was not the most appropriate method. In other studies, adrenocortical carcinoma patients had a very poor prognosis with a 5-year overall survival below 30% in most series [31]. Age, tumor property, general health, comorbidities, and patient preference should be taken into account in order to maximize the benefits to patients.
Our research had some specific limitations. The number of cases in our single center was limited, and there were only a few tumors of rare pathology. There may be a large bias in the evaluation of clinical features and survival prognosis of these patients; for some patients with adrenal metastases, the diagnosis mainly depended on clinical diagnosis, without any confirmation from pathological diagnosis. In some patients with bilateral tumors, pathology was only performed on one side of the body, which may also affect the statistical results of pathological distribution in this group of cases.
Conclusion
LATs were here affirmed to be a group of complex diseases with diverse sources. Understanding the clinicopathological characteristics of LATs was found to be of great significance for accurately evaluating LATs and selecting the most suitable treatment.
Availability of data and materials
The data came from our hospital’s data system.
Abbreviations
- LATs:
-
Large adrenal tumors
References
Zografos GN, Farfaras A, Vasiliadis G, et al. Laparoscopic resection of large adrenal tumors. JSLS. 2010;14(3):364–8.
Parnaby CN, Chong PS, Chisholm L, et al. The role of laparoscopic adrenalectomy for adrenal tumours of 6 cm or greater. Surg Endosc. 2008;22(3):617–21.
Cichocki A, Samsel R, Papierska L, et al. Adrenal tumour bigger than 5 cm — what could it be? An analysis of 139 cases. Endokrynol Pol. 2017;68(4):411–5.
Henneman D, Chang Y, Hodin RA, et al. Effect of laparoscopy on the indications for adrenalectomy. Arch Surg. 2009;144(3):255–9.
Mccauley LR, Nguyen MM. Laparoscopic radical adrenalectomy for cancer: long-term outcomes. Curr Opin Urol. 2008;18(2):134–8.
Porpiglia F, Fiori C, Daffara F, et al. Retrospective evaluation of the outcome of open versus laparoscopic adrenalectomy for stage I and II adrenocortical cancer. Eur Urol. 2010;57(5):873–8.
Chen W, Liang Y, Lin W, et al. Surgical management of large adrenal tumors: impact of different laparoscopic approaches and resection methods on perioperative and long-term outcomes. BMC Urol. 2018;18(1):31.
Macgillivray DC, Whalen GF, Malchoff CD, et al. Laparoscopic resection of large adrenal tumors. Ann Surg Oncol. 2002;9(5):480–5.
Naya Y, Suzuki H, Komiya A, et al. Laparoscopic adrenalectomy in patients with large adrenal tumors. Int J Urol. 2005;12(2):134–9.
Liao CH, Chueh SC, Lai MK, et al. Laparoscopic adrenalectomy for potentially malignant adrenal tumors greater than 5 centimeters. J Clin Endocrinol Metab. 2006;91(8):3080–3.
Mege D, Taieb D, Lowery A, et al. Contemporary review of large adrenal tumors in a tertiary referral center. Anticancer Res. 2014;34(5):2581–8.
Taffurelli G, Ricci C, Casadei R, Selva S, Minni F, et al. Open adrenalectomy in the era of laparoscopic surgery: a review. Updates Surg. 2017;69(2):135–43.
Young WF. Management approaches to adrenal incidentalomas: a view from Rochester, Minnesota. Endocrinol Metab Clin North Am. 2009;29:159–85.
Kloos RT, Gross MD, Francis IR. Incidentally discovered adrenal masses. Endocr Rev. 1995;16(4):460–84. https://doi.org/10.1210/edrv-16-4-460.
Bednarczuk T, Bolanowski M, Sworczak K, et al. Adrenal incidentaloma in adults - management recommendations by the Polish Society of Endocrinology. Endokrynol Pol. 2016;67(2):234–58.
Morelli V, Palmieri S, Salcuni AS, et al. Bilateral and unilateral adrenal incidentalomas: biochemical and clinical characteristics. Eur J Endocrinol. 2013;168(2):235–41.
Kasperlik-załuska AA, Słowińska-srzednicka J, Rosłonowska E, et al. Bilateral, incidentally found adrenal tumours — results of observation of 1790 patients registered at a single endocrinological centre. Endocrynol Pol. 2010;61(1):69–73 PMID:20205107.
Thomas AJ, Habra MA, Bhosale PR, et al. Interobserver agreement in distinguishing large adrenal adenomas and adrenocortical carcinomas on computed tomography. Abdom Radiol. 2018;43(11):3101–8.
Terzolo M, Stigliano A, Chiodini I, et al. AME Position Statement on adrenal incidentaloma. Eur J Endocrinol. 2011;164(6):851–70.
Mayo-Smith WW, Song JH, et al. Management of incidental adrenal masses: a white paper of the ACR Incidental Findings Committee. J Am Coll Radiol. 2017;14(8):1038–44.
Fassnacht M, Arlt W, Bancos I, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016;175(2):G1–G34.
Twersky J, Levin DC. Metastatic melanoma of the adrenal: an unusual cause of adrenal calcification. Radiology. 1975;116:627–8.
Pena CS, Boland GW, Hahn PF, et al. Characterization of indeterminate (lipid-poor) adrenal masses: use of washout characteristics at contrast-enhanced CT. Radiology. 2000;217:798–802.
Young WF Jr. Conventional imaging in adrenocortical carcinoma: update and perspectives. Hormones Cancer. 2011;2:341–7.
McNicholas MM, Lee MJ, Mayo-Smith WW, et al. An imaging algorithm for the differential diagnosis of adrenal adenomas and metastases. Am J Roentgenol. 1995;165:1453–9.
Haider MA, Ghai S, Jhaveri K, et al. Chemical shift MR imaging of hyperattenuating (>10 HU) adrenal masses: does it still have a role? Radiology. 2004;231:711–6.
Tsukamoto N, Kojima M, Hasegawa M, et al. The usefulness of (18)F-fluorodeoxyglucose positron emission tomography ((18)F-FDG-PET) and a comparison of (18)F-FDG-pet with (67)gallium scintigraphy in the evaluation of lymphoma: relation to histologic subtypes based on the World Health Organization classification. Cancer. 2007;110:652–9.
Ansquer C, Scigliano S, Mirallie E, et al. 18F-FDG PET/CT in the characterization and surgical decision concerning adrenal masses: a prospective multicentre evaluation. Eur J Nucl Med Mol Imaging. 2010;37:1669–78.
Palazzo FF, Sebag F, Sierra M, et al. Long-term outcome following laparoscopic adrenalectomy for large solid adrenal cortex tumors. World J Surg Endos. 2006;30(5):893–8. https://doi.org/10.1007/s00268-005-0288-2.
Agcaoglu O, Aliyev S, Karabulut K, et al. Robotic versus laparoscopic resection of large adrenal tumors. Ann Surg Oncol. 2012;19(7):2288–94.
Almeida MQ, Bezerra-Neto JE, Mendonca BB, et al. Primary malignant tumors of the adrenal glands. Clinics. 2018;73(suppl 1):e756s.
Acknowledgements
We thank LetPub (www.letpub.com) for its linguistic assistance during the preparation of this manuscript.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
Article topic design was contributed by DY and JW. Data processing was performed by ZZ, LW, JC, XL, DL, TC, XY, HH, XW, and XS. JW and DY are the corresponding authors. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The name of the ethics committee: Ethics Committee of First Affiliated Hospital of Dalian Medical University.
Ethics References No: YJ-KY-FB-2018-59.
Consent for publication
We simply extracted data and did not involve the private information of patients.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zhang, Z., Wang, L., Chen, J. et al. Clinical analysis of adrenal lesions larger than 5 cm in diameter (an analysis of 251 cases). World J Surg Onc 17, 220 (2019). https://doi.org/10.1186/s12957-019-1765-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-019-1765-7