
Abstract
Purpose
This study aims to investigate the association between domain-specific physical activity (PA), sedentary behavior, subjective health perception, and health-related quality of life (HR-QoL) in Korean adults aged ≥ 65 years.
Methods
This cross-sectional study analyzed 6,004 older adults from the Korean National Health and Nutrition Examination Survey 2017–2020. PA and sedentary behavior were measured using a global PA questionnaire, and HR-QoL was assessed using the EuroQol-5 Dimension (EQ-5D, three-level version). Multiple logistic regression was used to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) after adjusting for confounding parameters.
Results
Older adults who were physically active at work showed a negative association with subjectively good health and HR-QoL, whereas those physically active in transport or leisure time showed a positive association with subjectively good health and HR-QoL. Older adults highly engaged in sedentary behavior showed a worse perception of health and HR-QoL. Compared to high sedentary behavior and physical activity during leisure time or transport, the EQ-5D index was higher than that of their counterparts.
Conclusion
Both domain-specific PA and sedentary behavior were significantly associated with older adults’ perception of health and HR-QoL. Interventions are needed to improve HR-QoL by reducing sedentary behavior and encouraging physical activity in transportation or leisure time among adults aged 65 years and above.
Similar content being viewed by others


Introduction
Advanced medicine and economic development have extended life expectancy and, along with a decrease in fertility rates, have increased the aging population worldwide [1]. Korea is also facing a huge challenge due to its aging population. In 2017, South Korea became an aged society, with more than 14% of people aged 65 years or older, and is predicted to become a super-aged society by 2025 [2]. An increasingly older population not only causes an increase in medical costs due to physical and psychological aging and disease but also raises the cost of social and economic support [3, 4]. Thus, improving quality of life, represented by the physical and psychological health of older adults, through active aging is becoming an increasingly prominent public health issue [5, 6].
Subjective health perception is one of the often-used tools in an overall measure of both physical and psychological health [7, 8]. Previous studies have reported that those with poor subjective health perception had a higher risk of mortality than those with good subjective health perception [9, 10]. It may be vital to improve subjective health perception to prolong the healthy lifespan of older adults.
Physical activity (PA), along with other lifestyle modifications, is one of the most effective ways to prevent aging-related non-communicable diseases [11,12,13]. A recent study on older people indicates that physical activity helps to maintain the functional capacities and health of older adults, leading to better life satisfaction [14]. In addition to insufficient PA, highly sedentary behavior may also pose a significant health risk [15, 16]. Increased activity and reduced sedentary behavior in older adults reportedly prevent cognitive and physical functional attenuation, alleviate diverse chronic conditions and symptoms related to aging, and might prevent or even reverse frailty [17,18,19]. This ultimately leads to improvements in the quality of life of older adults and encourages active aging.
However, most previous studies have focused on the total amount or intensity of PA. Thus, little is known about whether domain-specific PA, such as PA at work, during transportation, and during leisure time, is related to subjective health perception and health-related quality of life (HR-QoL) in older adults. Additionally, previous studies concluded that socio-environmental and contextual levels, such as gender, education, and income, may influence the motives and variables that affect PA level[20, 21]. However, there is still a lack of evidence regarding domain-specific PA. Furthermore, the joint association between domain-specific PA, sedentary behavior, subjective health, and HR-QoL in older adults has not been evaluated.
Therefore, the purpose of the current study was to investigate the association between domain-specific PA, sedentary behavior, subjective health perception, and HR-QoL among Korean individuals aged 65 years or above.
Methods
Study participants
The secondary data analysis was based on the Korean National Health and Nutrition Examination Survey (KNHANNES) data from 2017 to 2020. The KNHANNES is a nationwide cross-sectional survey conducted every year since 2007 in Korea [22]. Among 31,588 participants, 6,004 were included in the final analysis after excluding those younger than 65 years, with no data on PA, subjective health, and health-related quality of life (Fig. 1). All participants provided informed consent, and this study was approved by the Korea Centers for Disease Control and Prevention Institutional Review Board.

Flow diagram
Measurements
PA level was assessed using the Global Physical Activity Questionnaire (GPAQ). The GPAQ consists of 16 items that collect information about the amount of PA in three domains (leisure time, transport, and work) as well as sedentary behavior. PA in leisure time and work captures intensity (i.e., vigorous, moderate), frequency, and duration. The transport-related PA asked participants to respond to frequency and duration in a typical week. Total PA was calculated by summing the minutes spent per week in each domain. Sedentary behavior consisted of one question: ‘How much do you usually spend sitting or reclining on a typical day?’ and responded to hours and minutes. The validity and reliability of the Korean GPAQ have been evaluated previously [23].
The subjective health state was measured using a single item asking respondents to rate ‘How do you feel about your health in daily life?’. The participants responded on a five-point Likert scale (1 = very healthy to 5 = very unhealthy). Dichotomous variables were defined for a subjective health index as positive vs. neutral/non-positive. HR-QoL was measured using the three-level version of the five-dimension EroQol scale questionnaire (EQ-5D-3L). The EQ-5D-3L comprises the following five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The response options were scaled to three levels: no problems, some problems, and extreme [24]. We defined dichotomous variables for each EQ-5D-3L dimension according to the presence or absence of any grade of problems (i.e., no problem vs. some/extreme problems).
Covariates
In the adjusted model, we included covariates such as age, sex, household income, education levels, material status, and prevalence of chronic diseases (e.g., hypertension, diabetes mellitus, hyperlipidemia, arthritis, and osteoporosis). Anthropometry was used to measure the weight, height, and body mass index. Household income was categorized into quartiles (low, middle-low, middle-high, and high). Education level was classified as elementary school, middle school, high school, or college graduate or higher. Marital status included married/living together, married/living separately, spouse died, divorced, and not married. Participants were identified as having diabetes when their fasting glucose level was ≥ 126 mg/dL, HbA1c ≥ 6.5%, or use of medication [25]. Hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg, diastolic blood pressure (DBP) ≥ 90 mmHg, or using anti-hypertensive medications [25]. Hypertension was classified based on SBP ≥ 140 mmHg/DBP ≥ 90 mmHg or using anti-hypertensive medications [26]. Other chronic diseases were defined as having been diagnosed by a doctor or currently taking medicine.
Data analysis
Participants’ characteristics were presented using descriptive analyses. To compare the differences in characteristics, we performed an independent t-test for continuous variables and a chi-squared (χ2-test) for categorical variables. Each domain-specific PA was categorized into two groups (no PA vs. any PA) based on the amount of PA. Based on the median value, sedentary behavior was divided into < 7 h/day and ≥ 7 h/day.
Multivariable-adjusted logistic regression was performed to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) of the association with domain-specific PA, sedentary behavior, subjective health, and HR-QoL. Additionally, the joint association between domain-specific PA, sedentary behavior, subjective health, and HR-QoL was investigated using multiple-adjusted logistic regression. We included covariates such as age, sex, household income, education level, material status, and diseases to adjust for potential confounders. After adjusting for confounding factors, an analysis of covariance (ANCOVA) was performed to investigate the relationship between domain-specific PA, sedentary behavior, and the EQ-5D index.
To assess the robustness of our findings, we also conducted a subgroup analysis to explore whether the association of domain-specific PA, sedentary behavior, subjective health, and HR-QoL differed according to sociodemographic parameters. All analyses were conducted using SPSS software for Windows (version 26.0; IBM Corp., Armonk, NY), and statistical tests were 2-tailed, and p values < 0.05 were considered significant.
Results
Demographical characteristics of participants
Participants were grouped by sex; their characteristics are presented in Table 1. The mean age was 73.05 ± 5.12 years (male:72.91 ± 5.06 years, female:73.16 ± 5.17 years) and the body mass index was 24.09 ± 3.17 kg/m2 (male:23.76 ± 2.95 kg/m2, female:24.34 ± 3.31 kg/m2). Hypertension was the most common disease in both males (57%) and females (64%). Only 29.1% of the elderly met the aerobic PA guideline, and 17.9% were engaged in sufficient resistance exercise.
Association of domain-specific PA, subjective health, and HR-QoL
When we analyzed the sum of all domains’ PA, older persons who participated in PA showed a positive correlation with subjective health and HR-QoL parameters (Table 2). Individuals with any PA per week perceived themselves as healthier (OR = 1.36, 95% CI 1.18–1.58) and reported being less likely to have problems with HR-QoL parameters from 27% (OR = 0.73, 95% CI 0.63–0.86) to 40% (OR = 0.60, 95% CI 0.49–0.73) compared to those who did not do physical activity per week.
However, different relationships were observed in the analyses of domain-specific PA. Leisure time and transport PA were significantly positively correlated with subjective good health and HR-QoL. In contrast, work PA was significantly inversely associated with the odds of subjective good health and HR-QoL (Table 2). Individuals who participated in leisure or transportation PA were more likely to be identified as healthy by 73% (OR = 1.73, 95% CI 1.44–2.07) and 21% (OR = 1.21, 95% CI 1.05–1.39), respectively, compared with those who did not participate in these activities. In addition, for every 60 min per week of leisure- or transportation-related PA, the subjective health awareness OR increased by 9% (OR = 1.09, 95% CI 1.05–1.13) and 4% (OR = 1.04, 95% CI 1.01–1.07), respectively. Each leisure- and transportation-related activity also showed a dose-response relationship with the HR-QoL variables, as well as the EQ-5D index. A similar trend was observed when we conducted a sensitivity analysis by sex, age, BMI, education level, income status, and chronic disease status (Supplementary Table 1).
In contrast, older adults who engaged in work-related PA were 40% (OR = 0.60, 95% CI 0.37–0.97) were less likely to be identified as healthy than those with no work-related PA. In addition, individuals who have work-related PA were 1.33 times (OR = 1.33, 95% CI 0.84–2.11) to 2.38 times (OR = 2.38, 95% CI 1.59–3.56; p < 0.05) more likely to have problems with each HR-QoL dimensions compared to those who did not engage in work-related activity. The EQ-5D index was also significantly lower in older persons with work-related PA than in those without PA (0.84 ± 0.17 vs. 0.89 ± 0.15; p < 0.001).
Association of sedentary behavior, subjective health, and HR-QoL
Sedentary time showed a significant negative association with the odds of subjectively positive health and HR-QoL parameters (Table 3). Compared to the older adults who spent < 7 h per day sedentary behavior (low sedentary), those who spent ≥ 7 h/day sedentary (high sedentary) were 14% (OR = 0.86, 95% CI 0.74–0.99) less likely to self-report as healthy. Furthermore, for every 60 min of increased sedentary behavior per day, the subjective health awareness OR decreased by 3% (OR = 0.97, 95% CI 0.94–0.99). In terms of the dose-response relationship, sedentary behavior declined in HR-QoL and EQ-5D index. Compared to individuals on a low sedentary trajectory, those who were highly sedentary reported higher odds of having mobility problems (OR = 1.44, 95% CI 1.26–1.65), self-care problems (OR = 1.47, 95% CI 1.17–1.86), usual care problems (OR = 1.83, 95% CI 1.53–2.20), and pain and discomfort (OR = 1.57, 95% CI 1.38–1.80). Particularly, highly sedentary individuals had a significantly lower EQ-5D index than those with low sedentary behavior (0.88 ± 0.16 vs. 0.92 ± 0.12; p < 0.001). These trends were observed in the subgroup analysis by sex, age, body mass index, education level, income level, and chronic disease status (Supplementary Table 1).
Joint association between domain-specific PA, sedentary behavior with HR-QoL
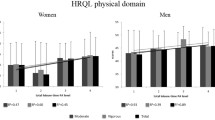
The joint associations of domain-specific PA, sedentary behavior, subjective health, and HR-QoL are shown in Table 4; Fig. 2. When analyzing total PA, older people with more physically active or less sedentary behavior had higher odds of subjective good health and lower odds of having problems with HR-QoL variables. Additionally, older adults who were physically active and had less sitting time showed a significantly higher EQ-5D index compared to those who were physically inactive and had high sitting time (0.93 ± 0.11 vs. 0.85 ± 0.18; p < 0.05).

Joint associations between domain-specific physical activity and sedentary behavior with EQ5D index in Korean older adults
Abbreviation: physical activity; PA, sedentary behavior; SB, *p < 0.05 with Sedentary behavior ≥ 7 h/day & No PA/week group, #p < 0.05 with Sedentary behavior ≥ 7 h/day & any PA/week group. a=adjust for age, gender, income, material status, education level, disease (hypertension, diabetes, hyperlipidemia, arthritis, osteoporosis)
However, subjective health and HR-QoL results according to domain-specific PA and sedentary time differed from total PA. In the case of leisure or transportation-related PA, individuals who were physically active or had less sitting time showed increased odds of subjectively good health and declined odds of responding to problems with HR-QoL components compared to those who had no PA or highly sedentary behavior. Compared to low sitting/active older adults, those who had high sitting time or were inactive in leisure or transportation PA significantly increased the odds of having problems in HR-QoL variables (Supplementary Table 2). Older adults who were physically active/have less sitting time also showed higher EQ-5D index than those who were the opposite (EQ-5D index in leisure 0.95 ± 0.09 vs. 0.87 ± 0.16; p < 0.05, in transportations 0.93 ± 0.11 vs. 0.85 ± 0.18; p < 0.05).
In contrast, work-related PA showed opposite results to leisure-or transportation-related PA. In terms of work-related PA, individuals who were physically active or had high sitting times tended to have lower odds of being healthy and higher odds of having HR-QoL problems. Even though sitting time was < 7 h/day, participants who did not perform work-related PA showed significantly lower odds of worse HR-QoL parameters than active individuals (Supplementary Table 2).
Discussion
The main goal of the current study was to evaluate the association between domain-specific PA, sedentary behavior, subjective health perception, and HR-QoL in older adults. In our study, physically active older adults showed different associations with subjective health perception and HR-QoL, according to the PA domain. Additionally, older adults who engaged in sitting time or work-related PA showed an inverse association with subjective health perception and HR-QoL.
Unlike our results, Scarabottolo et al. [27] and Choi and Bum [28] reported that high activity in work or leisure PA benefitted functional capacity and general health perception. There are two main reasons for the difference between the results of prior studies and those of this study. First, this study used a different tool, the GPAQ, to measure PA levels. The amount of PA was calculated using the number of days and frequency of moderate and vigorous PA in each domain. However, in the case of Scarabottolo [27], work, sports, and leisure activities were divided into never, rarely, sometimes, often, and always. In addition, Choi’s [28] study was divided only by whether or not there was PA in work and leisure. In addition to the PA domain, the PA amount is closely related to quality-of-life parameters. Thus, additional research is needed to investigate the effects of quality of life and PA by measuring the exact amount of PA in each domain of the older population. Second, there are mixed meanings for PA at work. Work-related PA may imply both a physically healthy state in which one can continue working [29] and a state in which one has to work because of vulnerable sociodemographic characteristics [30,31,32]. Cunningham et al. [29] reported that PA levels in older adults are closely related to their activities of daily living (ADL). Therefore, older adults who continue working are more likely to be physically and potentially mentally healthy due to more social relationships. In contrast, Ryu et al. [30] reported an increase of 2.28 times the stress and depression in the case of moderate to vigorous PA at work. In particular, for every 100 metabolic equivalents (METs) increase in PA in simple blue-collar jobs, the risk of depression increased by 29% and 30% for men and women, respectively. Other jobs, such as white-collar jobs, showed no significant association between work-related PA and depression. In addition, the amount of PA associated with work is closely related to sociodemographic factors that may affect health and quality of life [31,32,33]. Therefore, it is necessary to understand these effects and consider the social and environmental factors affecting the quality of life when investigating the amount of work PA.
In this study, leisure time and transportation PA showed a positive correlation between subjectively good health and HR-QoL. Considering that transport-related PA is the most frequent domain of PA, follow-up research investigating the effect of transport-related PA is necessary [30, 34, 35]. PA is known to affect various determinant parameters such as income, level of education, and walking environment [32, 33, 36]. Thus, it is necessary to provide laws and systems to promote PA in older adults as social support.
Sedentary behavior was negatively correlated with mental health and HR-QoL. This study also confirmed that sedentary behavior was negatively associated with subjective health and HR-QoL perception. Additionally, we observed that older adults with high sitting time, who were also highly engaged in transportation or leisure PA, had less severe subjective health and HR-QoL scores. Tully et al. [37] supported these results in terms of sedentary behavior and PA’s relationship with physical and mental health.
The study’s limitations include: First, it was a cross-sectional study, making it difficult to explain the causal relationship between PA, sedentary behavior, perception of subjective health, and HR-QoL. Second, the study participants comprised Korean senior citizens aged 65 years or older; therefore, caution is required when compared with other races and cultures. Despite these limitations, this study is meaningful because it is the first to investigate the importance of domain-specific PA in older adults, and its relationship with sedentary behavior and HR-QoL using national data, which is a large sample size. In the future, a large-scale cohort study that considers various socio-environmental variables that affect the PA and HR-QoL of the elderly is needed. Also it is necessary to continuously examine policy support in order to improve older people’s HR-QoL, by first investigating inequality factors (within the elderly) from various angles.
Conclusion
This study is the first to confirm the importance of reducing sedentary behavior, along with improving transportation and leisure-time related PA, to improve the HR-QoL of older adults. Considering the worldwide trend of aging populations, it is necessary to care for the physical and mental health of older adults. Continuous research on PA and reducing sedentary behavior is required to achieve this.
Data Availability
Not applicable.
Abbreviations
- PA:
-
Physical activity
- HR-QoL:
-
Health-related quality of life
References
World Health Organization. World report on ageing and health. World Health Organization; 2015.
Kim KW, Kim OS. Super aging in South Korea unstoppable but mitigatable: a sub-national scale population projection for best policy planning. Spat Demography. 2020;8(2):155–73. https://doi.org/10.1007/s40980-020-00061-8.
Chang AY, Skirbekk VF, Tyrovolas S, Kassebaum NJ, Dieleman JL. Measuring population ageing: an analysis of the global burden of Disease Study 2017. Lancet Public Health. 2019;4(3):e159–67. https://doi.org/10.1016/S2468-2667(19)30019-2.
Mahal A, McPake B. Health systems for aging societies in Asia and the pacific. Health Syst Reform. 2017;3(3):149–53. https://doi.org/10.1080/23288604.2017.1356429.
Boehlen FH, Maatouk I, Friederich HC, Schoettker B, Brenner H, Wild B. Loneliness as a gender-specific predictor of physical and mental health-related quality of life in older adults. Qual Life Research: Int J Qual Life Aspects Treat Care Rehabilitation. 2022;31(7):2023–33. https://doi.org/10.1007/s11136-021-03055-1.
Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020;139:6–11. https://doi.org/10.1016/j.maturitas.2020.05.018.
Tanaka S, Muraki S, Inoue Y, Miura K, Imai E. The association between subjective health perception and lifestyle factors in Shiga Prefecture, Japan: a cross-sectional study. BMC Public Health. 2020;20(1):1786. https://doi.org/10.1186/s12889-020-09911-y:ARTN.
Dong WH, Pan XF, Yu CQ, Lv J, Guo Y, Bian Z, Yang L, Chen YP, Wu TC, Chen ZM, Pan A, Li LM, China Kadoorie Biobank Collaborative Group. Self-rated health status and risk of incident stroke in 0.5 million chinese adults: the China Kadoorie biobank study. J Stroke. 2018;20(2):247–57. https://doi.org/10.5853/jos.2017.01732.
Bopp M, Braun J, Gutzwiller F, Faeh D. (2012) Health Risk or Resource? Gradual and Independent Association between Self-Rated Health and Mortality Persists Over 30 Years. PLOS ONE, 7(2). https://doi.org/:ARTN e3079510.1371/journal.pone.0030795.
Wuorela M, Lavonius S, Salminen M, Vahlberg T, Viitanen M, Viikari L. Self-rated health and objective health status as predictors of all-cause mortality among older people: a prospective study with a 5-, 10-, and 27-year follow-up. BMC Geriatr. 2020;20(1):120. https://doi.org/10.1186/s12877-020-01516-9.
Geidl W, Abu-Omar K, Messing S, Hartung V, Rütten A, Pfeifer K. National recommendations for physical activity and physical activity promotion: older adults and adults with non-communicable diseases. Aktuelle Ernahrungsmedizin. 2019;44(2):99–104. https://doi.org/10.1055/a-0836-5862.
Katzmarzyk PT, Friedenreich C, Shiroma EJ, Lee IM. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br J Sports Med. 2022;56(2):101–6. https://doi.org/10.1136/bjsports-2020-103640.
Palmer K, Monaco A, Kivipelto M, Onder G, Maggi S, Michel JP, Prieto R, Sykara G, Donde S. The potential long-term impact of the COVID-19 outbreak on patients with non-communicable diseases in Europe: consequences for healthy ageing. Aging Clin Exp Res. 2020;32(7):1189–94. https://doi.org/10.1007/s40520-020-01601-4.
Zapata-Lamana R, Poblete-Valderrama F, Ledezma-Dames A, Pavón-León P, Leiva AM, Fuentes-Alvarez MT, Cigarroa I, Parra-Rizo MA. Health, functional ability, and environmental quality as predictors of life satisfaction in physically active older adults. Social Sci. 2022;11(6):265. https://doi.org/10.3390/socsci11060265.
Gaskin C, Keesman K, Rogerson M, Salmon J, Orellana L. Physical activity and sedentary behavior among older adults with non-communicable diseases. Eur J Pub Health. 2017;27(suppl3). https://doi.org/10.1093/eurpub/ckx187.244.
Gilchrist SC, Howard VJ, Akinyemiju T, Judd SE, Cushman M, Hooker SP, Diaz KM. Association of sedentary behavior with cancer mortality in middle-aged and older US adults. JAMA Oncol. 2020;6(8):1210–7. https://doi.org/10.1001/jamaoncol.2020.2045.
Amaral Gomes ES, Ramsey KA, Rojer AGM, Reijnierse EM, Maier AB. The association of objectively measured physical activity and sedentary behavior with (instrumental) activities of Daily Living in community-dwelling older adults: a systematic review. Clin Interv Aging. 2021;16:1877–915. https://doi.org/10.2147/CIA.S326686.
Gerten S, Engeroff T, Fleckenstein J, Füzéki E, Matura S, Pilatus U, Vogt L, Pantel J, Banzer W. Deducing the impact of physical activity, sedentary behavior, and physical performance on cognitive function in healthy older adults. Front Aging Neurosci. 2021;13:777490. https://doi.org/10.3389/fnagi.2021.777490.
Zhaoyang R, Martire LM, Darnall BD. Daily pain catastrophizing predicts less physical activity and more sedentary behavior in older adults with osteoarthritis. Pain. 2020;161(11):2603–10. https://doi.org/10.1097/j.pain.0000000000001959.
Zapata-Lamana R, Poblete-Valderrama F, Cigarroa I, Parra-Rizo MA. The practice of vigorous physical activity is related to a higher educational level and income in older women. Int J Environ Res Public Health. 2021;18(20):10815. https://doi.org/10.3390/ijerph182010815.
Parra-Rizo MA, Vásquez-Gómez J, Álvarez C, Diaz-Martínez X, Troncoso C, Leiva-Ordoñez AM…, Cigarroa I. Predictors of the level of physical activity in physically active older people. Behav Sci. 2022;12(9):331. https://doi.org/10.3390/bs12090331.
Kweon S, Kim Y, Jang MJ, Kim Y, Kim K, Choi S, Chun C, Khang YH, Oh K. Data resource profile: the Korea National Health and Nutrition Examination Survey (KNHANES). Int J Epidemiol. 2014;43(1):69–77. https://doi.org/10.1093/ije/dyt228.
Lee J, Lee C, Min J, Kang DW, Kim JY, Yang HI, Park J, Lee MK, Lee MY, Park I, Jae SY, Jekal Y, Jee SH, Jeon JY. Development of the Korean Global Physical Activity Questionnaire: reliability and validity study. Global Health Promotion. 2020;27(3):44–55. https://doi.org/10.1177/1757975919854301.
Lee YK, Nam HS, Chuang LH, Kim KY, Yang HK, Kwon IS, Kind P, Kweon SS, Kim YT. South korean time trade-off values for EQ-5D health states: modeling with observed values for 101 health states. Value in Health: the Journal of the International Society for Pharmacoeconomics and Outcomes Research. 2009;12(8):1187–93. https://doi.org/10.1111/j.1524-4733.2009.00579.x.
Elliott TL, Pfotenhauer KM. Classification and diagnosis of diabetes. Prim Care. 2022;49(2):191–200. https://doi.org/10.1016/j.pop.2021.11.011.
Williams B, Mancia G, Spiering W, Rosei EA, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Lip GYH, McManus R, Narkiewicz K, Ruschitzka F, Schmieder RE, Shlyakhto E, Tsioufis C, Aboyans V, Desormais I. [2018 ESC/ESH guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH)]. G Ital Cardiol. 2018;19(11):3S–73S. https://doi.org/10.1714/3026.30245.
Scarabottolo CC, Cyrino ES, Nakamura PM, Tebar WR, Canhin DDS, Gobbo LA, Christofaro DGD. Relationship of different domains of physical activity practice with health-related quality of life among community-dwelling older people: a cross-sectional study. BMJ Open. 2019;9(6):e027751. https://doi.org/10.1136/bmjopen-2018-027751.
Choi C, Bum C-H. Physical leisure activity and work for quality of life in the elderly. J Phys Educ Sport. 2019;19(2):1230–5.
Cunningham C, O’ Sullivan R, Caserotti P, Tully MA. Consequences of physical inactivity in older adults: a systematic review of reviews and meta-analyses. Scand J Med Sci Sports. 2020;30(5):816–27. https://doi.org/10.1111/sms.13616.
Ryu J, Jeong A, Min JH, Lee DH, Lee J, Song IH, Jeon JY. The relationship between domain-specific physical activity and depressive symptoms in korean adults: analysis of the Korea National Health and Nutrition Examination Survey. J Affect Disord. 2022;302:428–34. https://doi.org/10.1016/j.jad.2022.01.097.
Talarska D, Tobis S, Kotkowiak M, Strugała M, Stanisławska J, Wieczorowska-Tobis K. Determinants of quality of life and the need for support for the elderly with good physical and mental functioning. Med Sci Monitor: Int Med J Experimental Clin Res. 2018;24:1604–13. https://doi.org/10.12659/msm.907032.
Meijer EP, Goris AHC, Wouters L, Westerterp KR. Physical inactivity as a determinant of the physical activity level in the elderly. Int J Obes Relat Metabolic Disorders: J Int Association Study Obes. 2001;25(7):935–9. https://doi.org/10.1038/sj.ijo.0801644.
Zhang Y, Su D, Chen Y, Tan M, Chen X. Effect of socioeconomic status on the physical and mental health of the elderly: the mediating effect of social participation. BMC Public Health. 2022;22(1):605. https://doi.org/10.1186/s12889-022-13062-7.
Lee J, Min J, Lee DH, Kang DW, Jeon JY. Intensity- and domain-specific physical activity levels between cancer survivors and non-cancer diagnosis individuals: a propensity score matching analysis. Support Care Cancer. 2021;29(2):661–8. https://doi.org/10.1007/s00520-020-05514-w.
Lee EB, Hong S, Min J, Park DH, Cho W, Suh SH, Lee HD, Lee HJ, Kimm H, Jee SH, Kang ES, Lee DH, Jeon JY. (2021) Association between domain-specific physical activity and diabetes in Korean adults. Sci Rep-Uk 11 (1). https://doi.org/10.1038/s41598-021-92560-x.
Jun HG, Chang YY, Dan BJ, Jo BR, Min BH, Yang H, Song WK, Kim J. Walking and sit-to-stand support system for elderly and disabled. Int C Rehab Robot. 2011. https://doi.org/10.1109/ICORR.2011.5975365.
Tully MA, McMullan I, Blackburn NE, Wilson JJ, Bunting B, Smith L, Kee F, Deidda M, Giné-Garriga M, Coll-Planas L, Dallmeier D, Denkinger M, Rothenbacher D, Caserotti P. Sedentary behavior, physical activity, and mental health in older adults: an isotemporal substitution model. Scand J Med Sci Sports. 2020;30(10):1957–65. https://doi.org/10.1111/sms.13762.
Acknowledgements
Not applicable.
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
All the authors contributed to the conception and design of the study. Material preparation, data collection, and analysis were performed by Jihee Min, Jae Seung Chang, and In-Deok Kong. The first draft of the manuscript was written by Jihee Min, and all the authors commented on the previous versions of the manuscript. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and Consent to participate
This study was conducted per the principles of the Declaration of Helsinki. Approval was granted by the Korea Centers for Disease Control and Prevention Institutional Review Board (No. 2018-01-03-P-A; 2018-01-03-C-A; 2018-01-03-2 C-A).
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Min, J., Chang, J.S. & Kong, I.D. Domain-specific physical activity, sedentary behavior, subjective health, and health-related quality of life among older adults. Health Qual Life Outcomes 21, 52 (2023). https://doi.org/10.1186/s12955-023-02136-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-023-02136-8