
Abstract
Background
A conceptual model approach to clarify the elements of health-related quality of life (HRQL), their determinants and causal pathways is needed to aid researchers, health practitioners and policy makers in their bid to improve HRQL outcomes in patients. The aim of this systematic review was to appraise empirical evidence on the performance of the Wilson and Cleary Model of HRQL.
Methods
We conducted a search of MEDLINE, Science Direct, PsyARTICLES and CINAHL databases to identify articles that used Wilson and Cleary model to examine HRQL in chronic diseases. A narrative synthesis was employed in the review of the articles.
Results
Evidence supports linkages between adjacent concepts and between non-adjacent concepts of the Wilson and Cleary model indicating that in practice there is a need to examine relationships among constructs - or to consider interventions in terms of - both with and without mediators. Symptoms status has the highest magnitude of relative impact on health-related quality of life.
Conclusion
The Wilson and Cleary model demonstrated good features suitable for evaluating health-related quality of life in chronic diseases.
Similar content being viewed by others


Background
Health-related quality of life (HRQL) is an important outcome measure in clinical trials and health research. The concept includes measures of patient and social perspectives regarding the impact of illness in order to improve treatment efficacy, safety and shared decision-making [1,2,3]. Examining the construct of HRQL has become important because it focuses on components of well-being, which are affected by progressive changes in health status, health care and social support [4].
Patients living with chronic illnesses such as sickle cell disease, HIV/AIDs, chronic obstructive pulmonary disease, arthritis and obesity have been found to have impaired HRQL [5]. HRQL has thus become an important construct in the evaluation of the effect of a disease and its management. However, there has been lack of agreement on the definitions and dimensions of HRQL which could guide standard measurements and research that could lead to a more detailed understanding of the concept. Nonetheless, there are three identified areas of consensus, that first, HRQL is a multidimensional construct encompassing symptoms of diseases, treatment side effects, general perception of health status and life satisfaction [6]; second, the assessment of HRQL is subjective based on self-report termed patient-reported outcomes (PROs) [3, 7] and third, research on HRQL should be based on conceptual models [8, 9]. Such models would enhance the understanding of the relationships and linkages among dimensions of HRQL which in turn could facilitate the design of protocols for optimal care.
Wilson and Cleary [10] have proposed a conceptual model to integrate clinical and psychosocial approaches to health care. Their model links the biological and physiological (objective health) variables to the measure of HRQL or subjective health constructs. This link was made to move research on HRQL from the traditional descriptive methods to models, so that causal relationships among the components could be investigated and clarified. Knowing the proximate causes of HRQL in a disease population would help target rather than just monitor the improvement of HRQL in clinical trials.
The Wilson and Cleary model is the most widely cited conceptual framework of HRQL [8, 9, 11]. In a systematic review of health-related quality of life models, Bakas and colleagues [8] showed that the Wilson and Cleary model was unique to HRQL, adequate, clear and consistent and could be applied to all individuals irrespective of age, health and disease conditions as well as culture. They further showed that the Wilson and Cleary model could generate hypotheses to provide clinicians with a broader view of HRQL beyond just biological factors and symptoms, and that the model ‘makes sense’ for real world application. The model focusses on relationships among different domains of health by proposing a linear sequence of causal links along a causal pathway which begins with the bio-physiological level moving along the causal pathway outward to the subjective level and the interaction of the individual as a social being.
The Wilson and Cleary model presents a taxonomy of patient outcomes categorised into five underlying health concepts and proposes specific causal links between these health concepts. Their underlying assumptions are that understanding relationships among these concepts will inform the design of optimally effective clinical interventions ([9] The five health concepts described in the model are biological and physiological factors, symptoms status, functioning, general health perceptions and overall quality of life.
The biological and physiological factors focus on the functioning of cells, organs and organ systems. The clinical factors include factors that generally affected health but are mediated by changes in cells, organs or organ systems functions. The next point on the continuum is symptoms status which has been described as a patient’s perception of an abnormal physical, emotional or cognitive state [10]. The complexity of relationship between biological and physiological factors and symptoms is underlined by the fact that some physiological abnormality may not immediately produce symptoms while some symptoms such as depression may not be clinically traceable to physiologic abnormality [10]. Following symptoms is functional status which is reflected in the ability of the individual to perform specific tasks such as climbing the stairs. The next link is the general health perceptions, a subjective rating that integrates all the previously mentioned health concepts and others such as mental health and is followed by the overall or global health-related quality of life at the end of the continuum [10]. Arrows in the model depict dominant causal associations. Reciprocal relationships are implied but not shown. The possibility of bidirectional relationship has also been suggested [10] but not indicated.
Empirical evidence from studies that have used the Wilson and Cleary model is needed to establish patterns of relationship and their consistency. Integrating results of empirical studies onto the model will reveal the features and performance of the model and enhance our understanding of patterns of relationships and effects of mediators thereby increasing the information available to health researchers and practitioners. Furthermore, understanding the relative importance of each of the concepts with respect to their effects on the overall quality of life may be useful in future research. This paper reports a systematic review of literature on the application of Wilson and Cleary’s model in chronic diseases to examine the paths and pattern of relationships of the concepts as well as determine their relative importance. We aimed to answer three important research questions:
-
1.
Does empirical evidence show the causal relationship of the dominant concepts as proposed in the Wilson and Cleary model?
-
2.
Does the Wilson and Cleary model follow a strictly linear unidirectional path?
-
3.
What is the relative effect of each latent factor?
Methods
This study followed the format of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement [12]. The electronic databases searched consisted of Science Direct, MEDLINE, CINAHL and PsyARTICLES. The search term used was “Wilson and Cleary” (free text). Further related search terms such as, “Wilson and Cleary model”, “Wilson and Cleary conceptual model”, “(Health-related quality of life OR HRQL OR HRQOL) AND (Wilson and Cleary OR Wilson and Cleary model)”, were also used, but did not yield any additional studies. The search covered a period from 1995 (when the model was published) to December 2016.
Inclusion criteria:
-
Chronic disease
-
Articles published in English language
-
HRQL measured with validated instruments
-
Empirical study
-
Wilson and Cleary model was used or tested
-
Peer-reviewed articles with full-text accessible.
Exclusion criteria:
-
Articles based on instrument development
-
Articles that did not apply the model
The titles and abstracts of retrieved articles were reviewed by AO for eligibility and selected based on the inclusion criteria. The selection was validated by JL. Full-texts of articles were reviewed for inclusion by AO, JL and YG validated these and also agreed on the five articles that were hand-searched for inclusion in the study.
Quality assessment of selected articles
The Quality Assessment Tool for Quantitative Studies designed by the Effective Public Health Practice Project (EPHPP) was used to evaluate the quality of included articles [13]. The EPHPP tool was designed to assess quality of observational and clinical studies. The tool was used to rate each article on a three-point scale (strong, moderate and weak) in six components: selection bias, study design, confounders, blinding, data collection methods, and withdrawal and drop-outs. A global rating was allocated to each study.
Data extraction, synthesis and analysis
Standardised data extraction form was used to extract data from the included studies by AOO, these were reviewed independently by YG and JL. Information extracted from each article included author, year of publication disease, study design, measures of latent factors, study aim, outcome of study and percentage of variance explained by the model. Articles selected had the primary objective of testing or applying the Wilson and Cleary model in the disease population. Most of the study designs were cross sectional (77%), heterogeneity was not formally calculated as meta-analysis was not performed.
Three research questions proposed for this study were to evaluate linearity and non-linearity of relationships and the effects of predictor variables on HRQL. Linearity was evaluated based on direct causal links between the concepts along the path of continuum proposed by Wilson and Cleary [10]. Non-linearity was evaluated based on significance of paths between non-adjacent variables - that is we establish that there is non-linearity if the effects between non-adjacent variables were significant so that paths between adjacent and non-adjacent variables were allowed [14]. The magnitude of the influence of each of the variables was also examined to evaluate their relative effects on HRQL.
Results
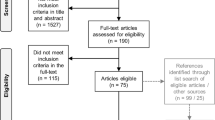
The initial search yielded a total of 2018 full text peer reviewed articles (Fig. 1). Duplicates were removed and articles were screened on titles and abstracts. The full-texts of the selected 78 articles were screened. Of these, 59 articles were excluded: 14 because they were based on instrument development, 18 did not apply the model, 14 were not empirical studies and 11 could not be categorised as focusing on chronic disease. Five additional articles were added through searching of reference lists of the selected studies. The total number of articles reviewed was 26 [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. The flow chart of the included studies is displayed in Fig. 1.

Flow chart of study selection procedure
Characteristics of studies reviewed
The 26 studies took place in 15 countries with one study based across four countries in Sub-Saharan Africa (Botswana, Lesotho, South Africa and Swaziland) (Table 1). The other countries were: USA (n = 9), Norway (n = 3), Canada (n = 2), Netherlands (n = 3), Thailand (n = 2), UK (n = 1), France (n = 1), Austria (n = 1), Sweden (n = 1), Brazil (n = 1) and Hong Kong (n = 1).
Thirteen different types of disease were studied: heart failure/surgery (n = 5), HIV/AIDS (n = 6), coronary artery disease (n = 3), oral health disease (n = 2), obesity (n = 2), chronic obstructive pulmonary disease (n = 2) and asthma, diabetes, Hodgkin’s lymphoma, kidney, Pompe disease, generalised anxiety disorder and stroke (all n = 1). Study designs were either cross sectional (n = 20) or longitudinal (n = 6). The total number of participants was 11,849, with a mean age of 50.5 years; 43.7% were female.
Quality assessment
Six studies were rated as strong (23%), 19 studies had moderate rating (73%) and one study had a weak rating (Table 1).
Measures
Generic instruments
The most widely used instrument was the Medical Outcome Survey (MOS) Short Form 36 (SF-36) [41], in both the full form SF-36 (n = 10) and the shorter form 12 [42], SF-12 (n = 2). Components of the instrument were used to measure symptoms status (n = 3), functional status (n = 7), general health perceptions (n = 9) and global HRQL (n = 2). Other generic instruments used were the Sickness Impact Scale (SIS), Patient Health Questionnaire (PHQ-9) [43] to measure depression, Beck’s Depression Index (BDI) [44] and the Hospital Anxiety and Depression Scale (HADS) [45].
Disease-specific instruments for HRQL
Disease-specific HRQL instruments used in the studies included the MacNew Heart Disease Quality of Life [24], Minnesota Living with Heart Failure Questionnaire (MLFHQ) and the New York Heart Association (NYHA) classification to measure the global HRQL in heart failure [23, 26, 38]. The HIV/AIDS-Targeted Quality of Life (HAT-QoL) instrument [29,30,31] for HIV/AIDs populations while the Quality of Life, Obesity and Dietetics (QOLOD) [18], Oral Health Impact Profile (OHIP-14) [17, 33] were used in diabetes and oral health populations respectively.
Analytical tools
In modelling the data (Table 2), different analytical tools were used: stepwise/hierarchical regression (n = 3), linear mixed model/multiple regression (n = 4), logistic regression and/or partial correlation (4). Structural Equation Modelling (SEM)/path modelling was used in most of the studies (n = 15), with 67% of those who used SEM/path analysis reporting the fit of the model. SEM has been found to exhibit superior properties compared to regression analysis in overcoming the limitations of regression by decomposing the sources of correlation among independent variables [21] and make it possible for each variable in a path model to be treated simultaneously as both a predictor and as an outcome.
Research question 1: Does empirical evidence show the causal relationship of the dominant concepts as proposed in Wilson and Cleary’s model?
Adjacent linkages and mediators
Wilson and Cleary [10] hypothesised that there existed direct causal links between biological and physiological factors, symptoms, functional status, general health perceptions and HRQL. Symptoms mediate between physiological factors and functional status, while functional status mediates between symptoms and general health perceptions, and general health perceptions mediates between functional status and overall HRQL. Eleven studies supported the direct causal link proposition between biological and physiological factors and symptoms (Fig. 2). Markers of biological and physiological variables were found to associate with worse symptoms in the patients with HIV/AIDs, xerostomia, coronary artery disease, Hodgkins lymphoma and generalised anxiety disorder [17, 37, 38, 40, 46]. The next level of the model associates symptoms with functioning and mediates between functioning and biological/physiological variables. This has been established in 20 studies (e.g., [16, 22, 29]). More symptoms predicted a greater impact on everyday functioning, with symptoms status explaining 49% of functional health in HIV/AIDs patients [37]. Functional status was found to have direct links to general health perception and mediated between general health perception and symptoms in 16 studies. Worse functioning indicated low perceived health. For example, worse functioning was associated with lower global oral health perception in Hodgkin’s lymphoma [46]. More symptoms and less functional health may lead to a perceived decrease in perceived general health. The hypothesised effect of general health perception on overall HRQL was established in 12 studies (Fig. 2).

Adjacent and non-adjacent linkages of concepts
Research question 2: Does the Wilson and Cleary model strictly follow a linear unidirectional path?
Linkages between non-adjacent concepts
We examined the links between non-adjacent variables to establish whether empirical data show that the model allows non-linear, indirect paths.
Biological and physiological variables were directly associated with functional status, general health perception and overall HRQL in nine, two and three studies respectively (Fig. 2). For example, Kanters et al. [25] showed that enzyme activity, a biological marker, was significantly associated with HRQL in adult Pompe disease. Direct links were established between symptom status and, general health perception and HRQL in nine and seven studies respectively. Furthermore, functional status was associated directly with overall HRQL in seven studies. In coronary artery disease, physical functioning showed high positive significant effect on HRQL (β = 0.36) indicating that a reduction in functional health may reduce HRQL [24]. The studies assumed non-reciprocal relationships except Mathisen et al. [27] who attempted to model reciprocal relationship between general health perception and HRQL. This did not take into consideration possible effects between other concepts. Hence, we could not establish the possibilities of bidirectional relationships between the abstract concepts in this study.
Research question 3: What is the relative effect of each variable?
The relative effects of the variables were measured in terms of the magnitude of their influence on HRQL (Fig. 3). The causal links were labelled 0 M, 1 M, 2 M and 3 M to signify the number of mediators between constructs that were bypassed. 0 M was a direct link between the concepts with the proposed mediating variable signifying that no mediator was bypassed in the link, 1 M was an indirect link with one mediator bypassed, 2 M with two mediators bypassed and 3 M with three mediators bypassed. 0 M, 1 M and 2 M revealed symptoms status as a consistently important factor that affected HRQL, followed by functional status. In 0 M all four concepts; biological and physiological, symptom status, functioning status and general health perception were compared with respect to the effect of each on the adjacent variable. Clinical variables had the lowest magnitude of effect followed by general health perception, function status and symptoms status in order of increasing magnitude. Clinical factor was however on the same level with functional status when only the immediate mediator was bypassed.

Bar chart of observed magnitudes of effects
Discussion
Brief summary
The findings of this systematic review support the model of HRQL as proposed by Wilson and Cleary [10] and establish the conceptualised relationships and mediation. Of the articles reviewed, 74% found symptom status a significant predictor and critical mediator making it the most important predictor of HRQL by indirect effects through functional status and general health perceptions and by direct effects. More symptoms implied impaired functioning with consequently worse general health perception and lower HRQL. Most of the studies (73%) were of moderate quality; this was because the quality assessment criteria [13] gives low ratings to study designs that are not experimental or longitudinal in nature.
Comparison with previous studies
Both symptoms and general health perception were found to account for 38.2% of variance in global HRQL [26] and studies also showed that general health perception alone mediated the relationship between symptom status and HRQL [16, 28, 35, 37, 38]. One of the most important symptoms was depression which strongly associated with physical functioning (β = −0.32) and general health perceptions [24]. Two studies found no association between the clinical factors, and any of the health constructs in heart failure and diabetes [23, 35]. This may be due to other profound non-clinical factors that responsible for impaired HRQL in these populations. The non-adjacent links among the health concepts showed that the model was non-linear also the effects of the variable were not fully mediated by their proposed mediators. For example, the direct link between symptom status and overall HRQL indicated that both functional status and general health perception did not fully mediate the effects of symptom burden on HRQL.
Possible explanations and implication
The findings of Sullivan et al. [14] in coronary artery disease patients supported our findings of a direct link between biological and physiological variables, and functional status. Further studies of a longitudinal nature will be required to establish possible bidirectional relationships among the concepts and whether the factors exert reciprocal influence on each other. For example, while the symptoms of pain may reduce functioning in patients with sickle cell disease, the inability to function as expected may lead to depression which may further limit functioning and lower HRQL. Our study is the first to synthesize results of studies on Wilson and Cleary’s model and to establish the relative importance of the constructs in determining the quality of life of patients in chronic diseases.
Limitations
We identified some potential limitations to this study. The study focused on several chronic diseases which have different clinical statuses, prognoses and levels of disability, which restricts our ability to generalise based on the lack of homogeneity of symptom status and functional status of the patients. There is also the potential limitation due to publication bias as only published articles were used in this study. In addition, different instruments were used to measure HRQL in the included studies; while some are generic, some are disease-specific [47]. As there is no instrument that is a “gold standard”, researchers often select instruments sensitive to the health state they are investigating ([48] rather than a general measure of HRQL. Moreover, there are also variations in clinically important differences across groups of patients defined by diseases, conditions, severity level, socio-economic status and nationality [49].
Conclusion
Our findings show that the Wilson and Cleary model demonstrates a good fit and proved useful in identifying relationships among the health constructs, and predictors of HRQL in the studied disease populations. The model explained between 22.9% and 72% of the variance in overall quality of life indicating that, in some cases, the model may require modification to capture factors not specified in the model but that may be important determinants of overall quality of life.
The findings supported the robustness of the Wilson and Cleary model as a conceptual framework to characterise predictors of HRQL in chronic diseases and to aid understanding of the relationship between clinical and psychological outcomes for patients with chronic illness. Our understanding of specific directions of influence will aid healthcare practitioners and researchers to develop appropriate care protocols that will address psychosocial variables alongside clinical factors in chronic disease management. This study has demonstrated that symptoms are a major determinant of HRQL in patients with chronic disease, thus a clinical approach to reduce symptoms may help improve HRQL. Furthermore, in treating patients with chronic diseases, clinicians and healthcare practitioners should be alert for signs of depression because this study has highlighted depression as a major issue in HRQL.
Further work is needed to examine bidirectional relationships. Studies so far have focused on an assumption of no reciprocal relationship but low health perception or low HRQL might also worsen disease conditions and responses to treatment. Further studies on evaluation of the Wilson and Cleary model should be compared to the findings of this study.
Abbreviations
- HRQL:
-
Health-related quality of life.
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis
- SEM:
-
Structural Equation Modelling
References
Anderson KL, Burckhardt CS. Conceptualization and measurement of quality of life as an outcome variable for health care intervention and research. J Adv Nurs. 1999;29:298–306.
Hall T, Krahn GL, Horner-Johnson W, Lamb G. Examining functional content in widely used health-related quality of life scales. Rehabil Psychol. 2011;56:94–9.
Panepinto JA. Health-related quality of life in patients with hemoglobinopathies. Hematology Am Soc Hematol Educ Program. 2012;2012:284–9.
Zubritsky C, Abbott KM, Hirschman KB, Bowles KH, Foust JB, Naylor MD. Health-related Quality of Life : Expanding a 2013;53:205–210.
Anie KA, Egunjobi FE, Akinyanju OO. Psychosocial impact of sickle cell disorder: perspectives from a Nigerian setting. Glob Health. 2010;6:2.
Cella D, Stone AA. Health-related quality of life measurement in oncology: advances and opportunities. Am Psychol. 2015;70:175–85.
Post M. Definitions of quality of life: what has happened and how to move on. Top Spinal Cord Inj Rehabil. 2014;20:167–80.
Bakas T, McLennon SM, Carpenter JS, Buelow JM, Otte JL, Hanna KM, et al. Systematic review of health-related quality of life models. Heal {&} Qual Life Outcomes. 2012;10:134–45.
Ferrans CE, Zerwic JJ, Wilbur JE, Larson JL. Conceptual model of health-related quality of life. J Nurs Scholarsh. 2005;37:336–42.
Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA. 1995;273:59–65.
Villalonga-Olives E, Kawachi I, Almansa J, Witte C, Lange B, Kiese-Himmel C, et al. Pediatric health-related quality of life: a structural equation modeling approach. PLoS One. 2014;9
Moher D, Liberati A, Tetzlaff J, Altman DG, Grp P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement (reprinted from annals of internal medicine). Phys Ther. 2009;89:873–80.
Effective Public Health Practice Project. Quality assessment tool for quantitative studies. Eff Public Heal Pract Proj. 2010:2–5.
Sullivan MD, Kempen GI, Van Sonderen E, Ormel J. Models of health-related quality of life in a population of community- dwelling Dutch elderly. Qual Life Res. 2000;9:801–10.
Ade-Oshifogun JB. Model of functional performance in obese elderly people with chronic obstructive pulmonary disease. J Nurs Scholarsh. 2012;44:232–41.
Arnold R, Ranchor AV, Koëter GH, de Jongste MJL, Sanderman R. Consequences of chronic obstructive pulmonary disease and chronic heart failure: the relationship between objective and subjective health. Soc Sci {&} Med. 2005;61:2144–54.
Baker SR, Pankhurst CL, Robinson PG. Testing relationships between clinical and non-clinical variables in xerostomia: a structural equation model of oral health-related quality of life. Qual Life Res. 2007;16:297–308.
Brunault P, Frammery J, Couet C, Delbachian I, Bourbao-Tournois C, Objois M, et al. Predictors of changes in physical, psychosocial, sexual quality of life, and comfort with food after obesity surgery: a 12-month follow-up study. Qual Life Res. 2014:493–501.
Carlson B, Pozehl B, Hertzog M, Zimmerman L, Riegel B. Predictors of overall perceived health in patients with heart failure. J Cardiovasc Nurs. 2014;28:206–15.
Cosby C, Holzemer WL, Henry SB, Portillo CJ. Hematological complications and quality of life in hospitalized AIDS patients. AIDS Patient Care STDs. 2000;14:269–79.
Eilayyan O, Gogovor A, Mayo N, Ernst P, Ahmed S. Predictors of perceived asthma control among patients managed in primary care clinics. Qual Life Res. 2015;24:55–65.
Halvorsrud L, Kirkevold M, Diseth A, Kalfoss M. Quality of life model: predictors of quality of life among sick older adults. Res Theory Nurs Pract. 2010;24:241–59.
Heo S, Moser DK, Riegel B, Hall LA, Christman N. Clinical investigation: testing a published model of health-related quality of life in heart failure. J Card Fail. 2005;11:372–9.
Hofer S, Benzer W, Alber H, Ruttmann E, Kopp M, Sch Ssler G, et al. Determinants of health-related quality of life in coronary artery disease patients: a prospective study generating a structural equation model. Psychosomatics. 2005;46:212–23.
Kanters TA, Redekop WK, Rutten-Van Mölken MPMH, Kruijshaar ME, Güngör D, Van Der Ploeg AT, et al. Evidence for decline in the incidence of cystic fibrosis: a 35-year observational study in Brittany, France. 2012.
Krethong P, Jirapaet V, Jitpanya C, Sloan RA. Causal model of health-related quality of life in Thai patients with heart-failure. J Nurs Scholarsh. 2008;40:254–60.
Mathisen L, Andersen MH, Veenstra M, Wahl AK, Hanestad BR, Fosse E. Quality of life can both influence and be an outcome of general health perceptions after heart surgery. Health Qual Life Outcomes. 2007;5:27.
Mayo NE, Scott SC, Bayley M, Cheung A, Garland J, Jutai J, et al. Modeling health-related quality of life in people recovering from stroke. Qual Life Res. 2015;24:41–53.
Nokes KM, Coleman CL, Hamilton MJ, Corless IB, Sefcik E, Kirksey KM, et al. Age-related effects on symptom status and health-related quality of life in persons with HIV/AIDS. Appl Nurs Res. 2011;24:10–6.
Phaladze NA, Human S, Dlamini SB, Hulela EB, Hadebe IM, Sukati NA, et al. Quality of life and the concept of ‘ living well ’ with HIV/AIDS in sub-Saharan Africa. J Nurs Schorlarsh. 2005;37:120–6.
Portillo CJ, Mendez MR, Holzemer WL, Corless IB, Nicholas PK, Coleman C. Quality of life of ethnic minority persons living with HIV/AIDS. J Multicult Nurs Heal. 2005;11:31–8.
Saengsiri. A-O, Thanasilp S, Preechawong S. Factors predicting quality of life for coronary artery disease patients after percutaneous coronary intervention. Asian Biomed. 2014;8:31–42.
Dos Santos CM, Celeste RK, Hilgert JB, Hugo FN. Testing the applicability of a model of oral health-related quality of life. Cad Saude Publica. 2015;31:1871–80.
Schulz T, Niesing J, Stewart RE, Westerhuis R, Hagedoorn M, Ploeg RJ, et al. The role of personal characteristics in the relationship between health and psychological distress among kidney transplant recipients. Soc Sci {&} Med. 2012;75:1547.
Shiu ATY, Choi KC, Lee DTF, DSF Y, Man Ng W. Application of a health-related quality of life conceptual model in community-dwelling older Chinese people with diabetes to understand the relationships among clinical and psychological outcomes. J Diabetes Investig. 2014;5:677–86.
Sousa KH, Holzemer WL, Henry SB, Slaughter R. Dimensions of health-related quality of life in persons living with HIV disease. J Adv Nurs. 1999;29:178–87.
Sousa KH, Kwok O-M. Putting Wilson and Cleary to the Test: Analysis of a HRQOL Conceptual Model Using Structural Equation Modeling. Qual Life Res VO - 15. 2006;:725.
Ulvik B, Nygard O, Hanestad BR, Wentzel-Larsen T, Wahl AK. Associations between disease severity, coping and dimensions of health-related quality of life in patients admitted for elective coronary angiography - a cross sectional study. Health Qual Life Outcomes. 2008;6:38.
Wettergren L, Björkholm M, Axdorph U, Langius-Eklöf A. Determinants of health-related quality of life in long-term survivors of Hodgkin’s lymphoma. Qual Life Res. 2004;13:1369–79.
Wyrwich KW, Harnam N, Locklear JC, Svedsäter H, Revicki DA. Understanding the relationships between health outcomes in generalized anxiety disorder clinical trials. Qual Life Res. 2011;20:255–62.
Ware Jr JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med Care. 1992:473–83.
Ware Jr JE, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34:220–33.
Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. 2002;32:509–15.
Beck AT, Steer RA. Internal consistencies of the original and revised Beck depression inventory. J Clin Psychol. 1984;40:1365–7.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–70.
Wettergren L, Bjo M. Determinants of health-related quality of life in long-term survivors of Hodgkin ’ s. lymphoma. 2004:1369–79.
Ware Jr JE. The status of health assessment 1994. Annu Rev Public Health. 1995;16:327–54.
Hawthorne G, Richardson J, Day NAA. Comparison of the assessment of quality of life (AQoL) with four other generic utility instruments. Ann Med. 2001;33:358–70.
Samsa G, Edelman D, Rothman ML, Williams GR, Lipscomb J, Matchar D. Determining clinically important differences in health status measures. PharmacoEconomics. 1999;15:141–55.
Acknowledgements
Not applicable.
Ethical approval and consent to participate
Not applicable.
Funding
Authors received no direct funding for this work. However, AOO received financial support from the University of Ibadan for his PhD. CH was, and JL is, partially funded as a staff member of Fuse, the Centre for Translational Research in Public Health, a UKCRC Public Health Research Centre of Excellence. Funding for Fuse from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, the National Institute for Health Research, under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged.
Availability of data and materials
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
Author information
Authors and Affiliations
Contributions
AOO conceived the study, led the design of the review and drafted the manuscript. YG helped to draft the manuscript. CH helped to draft the manuscript. JL participated in the design of the review and helped to draft the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Ojelabi, A.O., Graham, Y., Haighton, C. et al. A systematic review of the application of Wilson and Cleary health-related quality of life model in chronic diseases. Health Qual Life Outcomes 15, 241 (2017). https://doi.org/10.1186/s12955-017-0818-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-017-0818-2