
Abstract
Background
This study examined the relationships between a newly developed older person-specific non-preference-based quality of life (QoL) instrument (Older People’s Quality of Life brief questionnaire (OPQoL-brief)) and two generic preference-based instruments (the EQ-5D-3L Level (EQ-5D-3 L) and the Adult Social Care Outcomes Toolkit (ASCOT) in a community-dwelling population of Australian older people receiving aged care services.
Methods
We formulated hypotheses about the convergent validity between the instruments (examined by Wilcoxon-Mann Whitney, Kruskal Wallis and Spearman’s correlation tests) and levels of agreement (assessed using intra class correlation (ICC) and modified Bland-Altman plots based on normalized Z EQ-5D-3 L and ASCOT utilities and OPQoL-Brief summary scores).
Results
The utilities/summary scores for 87 participants (aged 65–93 years) were moderately but positively correlated. Moderate convergent validity was evident for a number of instrument dimensions with the strongest relationship (r = 0.57) between ‘enjoy life’ (OPQoL-Brief) and ‘social contact’ (ASCOT). The overall ICC was 0.54 and Bland-Altman scatter plots showed 3–6 % of normalized Z-scores were outside the 95 % limits of agreement suggesting moderate agreement between all three instruments (agreement highest between the OPQoL-Brief and the ASCOT).
Conclusions
Our results suggest that the OPQoL-Brief, the ASCOT and the EQ-5D_3L are suitable for measuring quality of life outcomes in community-dwelling populations of older people. Given the different constructs underpinning these instruments, we recommend that choice of instrument should be guided by the context in which the instruments are being applied. Currently, the OPQoL-Brief is not suitable for use in cost-utility analyses as it is not preference-based. Given their different perspectives, we recommend that both the ASCOT and the EQ-5D are applied simultaneously to capture broader aspects of quality of life and health status within cost-utility analyses within the aged care sector. Future research directed towards the development of a new single preference-based instrument that incorporates both health status and broader aspects of quality of life within quality adjusted life year calculations for older people would be beneficial.
Similar content being viewed by others

Background
Australia, like many other countries, has an ageing population with the proportion of those aged 65 or over set to increase from 14 % of the total population in 2014 to 22 % by 2061 [1, 2]. This has ramifications for the levels of health and aged care services required and the ways in which these services are provided [3, 4]. In particular, growing numbers of older people are associated with a higher demand for health and aged care services which increasingly puts pressure on public funds [5]. Economic evaluation is an important technique to help decision-makers determine the relative value for money of service innovations in health and aged care [6] and is recommended for use by decision-making bodies internationally including the Pharmaceutical Benefits Advisory Committee (PBAC) and the Medical Benefits Advisory Committee (MSAC) in Australia and the National Institute for Health and Clinical Excellence (NICE) in the United Kingdom [7–9]. Previous studies have shown that for economic evaluations conducted in the aged care sector, effectiveness is best determined through the measurement of outcomes or benefits that are broad in scope [10, 11] and which older people themselves view as most valuable [12]. Maximising the quality of life of older people is also seen as a basic human right [13, 14]. Robust quality of life measurement from the perspective of older people is therefore a key requirement for economic evaluations and a highly important aspect when considering their health and aged care needs [5, 10].
A number of generic, condition-specific and older-person-specific preference and non-preference-based instruments have been used to capture quality of life in older people [5, 15]. Within economic evaluation, preference-based instruments are appealing because their application facilitates the calculation of quality adjusted life years (QALYs) which provide a common currency for assessing the benefits gained from alternative interventions in terms of both quality of life and survival [6]. While generic instruments have the advantage of being applicable to a wide range of populations and conditions [16], condition-specific (instruments focused on one particular health condition or illness) or population-specific (e.g., older person-specific) may be more sensitive and therefore more suitable for use within particular patient groups or populations [16, 17]. However, it is not always clear whether a strong relationship exists between population-specific and the more widely used generic instruments and whether the latter are as valid as the former when used in specific populations or people living with a particular condition. This study explored the convergent validity (whether scores on one instrument correlate to scores on other instruments designed to assess the same construct [18]) and levels of agreement (measuring the consistency or homogeneity of scores [19]) between a newly developed older person-specific non-preference-based instrument (Older People’s Quality of Life brief questionnaire (OPQoL-Brief) [20]) and two generic preference-based quality of life instruments (the Adult Social Care Outcomes Toolkit (ASCOT) [21] and the EQ-5D-3L Level (EQ-5D-3 L) [22]) in a population of community-dwelling older people receiving aged care services. So far, no simultaneous head-to-head comparison between all three instruments has been conducted in the literature. The results of this study will help inform decisions concerning the appropriateness of applying these instruments in various contexts within research conducted on older people.
Methods
Sample
Potentially eligible participants were identified by five Australian aged care provider partner organisations according to the following eligibility criteria: age ≥ 65 years, receiving community aged care services, English speaking and cognitively intact as assessed by the Global Deterioration Scale (GDS) [23] (i.e., if a GDS score ≤ 2 where 1 = normal cognition to 7 = severe dementia). Potential participants who consented to receiving further information about the study from the research team were contacted after which formal consent to participate was obtained. The study involved two main components: (i) completion of three quality of life instruments (the OPQoL-Brief, the EQ-5D-3 L and the ASCOT) and a series of socio-demographic questions, reported upon in this paper and (ii) completion of a discrete choice experiment (DCE) to elicit older people’s preferences for alternative configurations of community aged care services, the details of which are reported elsewhere [24].
The study was undertaken as a structured individual exercise completed within a group setting. Participants were asked to self-complete the three quality of life instruments independently with the research team available for the sole purpose of clarification of socio-demographic questions and/or questions within each instrument. The group setting was designed to accommodate a maximum of 20 participants with the same 3/4 researchers assisting. The groups were convened between June and December 2013 in central venues facilitated by the aged care research partners in South Australia and New South Wales [24].
Quality of life measurement
The OPQoL-Brief is an older-person-specific measure of quality of life and is a shorter version of the original 35-item OPQoL questionnaire (OPQoL-35) [20, 25]. The construct validity of the OPQoL-35 has been demonstrated in a population of multiethnic community-dwelling older people [25, 26]. The OPQoL is a non-preference-based instrument and it was not specifically developed for application in economic evaluation. Both the OPQoL-35 and the OPQoL-Brief include health-related and broader quality of life domains [27]. The OPQoL-Brief has 13 items relating to health, social relationships, independence, control over life, home and neighbourhood, psychological and emotional wellbeing, leisure and social activities, freedom and financial circumstances. Each item has a 5-point response scale coded 1–5 from ‘strongly disagree’ to ‘strongly agree’ (with higher codes representing better quality of life). The item scores can be summed up to give summary scores ranging from 13 to 65 with higher scores indicating better quality of life [20].
The ASCOT is a generic instrument designed to capture information about an individual’s social-care-related quality of life in community and institutional settings and is applicable to individuals aged ≥ 18 years [21]. Its construct validity when used in a population of older people has been demonstrated in the literature [28, 29]. The 4 level self-completion version (SCT4) has eight domains: control over daily life, personal cleanliness and comfort, food and drink, personal safety, social participation and involvement, occupation, accommodation cleanliness and comfort and dignity [21, 30]. Each domain has four levels (‘high needs’, ‘some needs’, ‘no needs’ and ‘ideal state’) coded 1–4 with higher codes representing better quality of life. As no Australian general population-specific algorithm for the ASCOT is currently available, preference weights from the UK general population, elicited using a Best-Worst Scaling approach (a form of DCE) [21], were used to calculate a utilities ranging from −0.17 to 1 with utilities less than ‘0’ representing states that are considered to be worse than death [21, 31].
The EQ-5D-3 L is a generic health-related quality of life measure with proven construct validity when used with populations of older people [32–35]. It has five domains: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each domain has three levels of impairment (‘no problems’, ‘some/moderate problems’ and ‘extreme’ problems) allowing the EQ-5D-3 L to distinguish between 243 states of health [36, 37]. Using the UK general population preference weights determined through the time trade off approach [36], utilities ranging from −0.59 to 1 can be attached to each of the health states with a higher utilities implying better quality of life. When the newly developed Australian general population specific scoring algorithm [38] is used, utilities ranging from −0.217 to 1 are obtained. The maximum utility of ‘1’ represents full health and a utility of ‘0’ represents dead. As with the ASCOT, utilities less than ‘0’ represent health states that are deemed to be worse than death [36, 39]. Similar to the ASCOT and for the sake of consistency, the UK-specific algorithm was applied to the EQ-5D-3 L in this study. The generic nature of the EQ-5D-3 L makes it applicable for the measurement and valuation of health related quality of life in populations of individuals aged ≥ 18 years [39, 40].
Statistical analysis
Descriptive statistics (means, standard deviations, medians, interquartile ranges and frequencies) were generated and normality was tested using the Shapiro–Francia test [41]. The distributions of the EQ-5D-3 L and ASCOT utilities and OPQoL-Brief summary scores were skewed (Shapiro–Francia test, p < 0.05). Consequently, non-parametric statistical tests of differences were applied (Wilcoxon-Mann Whitney, Kruskal Wallis and Spearman’s correlation tests) [42].
The convergent validity of the EQ-5D-3 L, ASCOT and OPQoL-Brief utilities or summary scores was explored using scatter plots and an assessment of the level of association (Spearman’s correlation) between individual dimensions from each of the three instruments and between these dimensions and utilities/summary scores of comparator instruments. We also examined the distribution of mean EQ-5D-3 L, ASCOT and OPQoL-Brief utilities/summary scores across all dimension levels of comparator instruments. Correlations between 0.4 and 0.6 were considered moderate and those ≥ 0.70 strong [43]. Differences in quality of life utilities/summary scores according to demographic and other participant characteristics were tested using Wilcoxon-Mann Whitney and Kruskal Wallis tests. Characteristics examined included age in years (65–74, 75–84 and ≥ 85), gender (female versus male), living arrangements (living alone or not), highest educational attainment (below or above secondary school) and whether the participant had an informal carer or not. The ability of each instrument to discriminate between 4 levels of self-assessed general health (defined as ‘excellent or very good’, ‘good’, ‘fair’ or ‘poor’) was also examined using the Kruskal Wallis test. Based on evidence from the literature [25, 44–46], we hypothesised a priori that strong correlations would exist between dimensions that measured similar constructs e.g., between the ‘Healthy to get out/about’ (OPQoL-Brief) and the ‘mobility’ (EQ-5D-3 L) dimensions. Overall, we also expected the OPQoL-Brief and ASCOT dimension and summary scores/utilities to be more strongly correlated to each other than to those of the EQ-5D-3 L as they both measure broader aspects of quality of life while the EQ-5D-3 L is more focused upon health-related quality of life [27, 47]. As such, we also expected the EQ-5D-3 L to be more strongly correlated than the broader measures of quality of life with self-assessed general health. Further, we postulated that lower OPQoL-Brief, EQ-5D-3 L and ASCOT mean utilities/summary scores respectively would be associated with correspondingly increasing levels of severity on the dimensions of comparator instruments. Finally, we hypothesised that all three instruments would discriminate between demographic and other participant characteristics in similar directions as they all measured the broad construct of quality of life. Specific hypotheses are presented in Tables 1 and 2.
To assess the level of agreement between the instruments, we estimated the intra-class correlation coefficients (ICC) at an individual level based on a two-way mixed-effect model where the individual effect was random and the effect of the instrument was fixed [48]. An ICC below 0.75 implies poor to moderate agreement and one above 0.75 good agreement [43]. To further study the limits of agreement between the three instruments, modified Bland-Altman plots were used. As the instruments use different rating scales leading to marked differences in the magnitude of the scores (i.e., OPQoL-Brief scores can be up to 13 times larger than those for the ASCOT and EQ-5D-3 L), Z scores of utilities/summary scores were calculated for the modified plots as recommended in the literature [49–51]. Utilities and summary scores were transformed (by squaring them) to follow a normal distribution before calculating Z scores. Of the three instruments, we hypothesised that the OPQoL-Brief and ASCOT would have the highest level of agreement given that they both incorporate broader aspects of quality of life than the EQ-5D-3 L which is more narrowly focused upon health status.
A significance level threshold of 5 % was assumed as the criterion for determining statistical significance in all analyses [52]. To account for the multiple comparisons conducted within this study, Šidák-Holm adjusted p-values were used for statistical tests of difference [53]. All analyses were conducted in Stata version 13.1 [48].
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical approval was obtained from the Flinders University Social and Behavioural and the University of Sydney Human Research Ethics Committees.
Consent
Informed consent was obtained from all individual participants included in the study.
Results
Demographic and other participant characteristics
Participant characteristics are presented in Table 1. Of the 380 potential participants initially identified as eligible for this study, 106 individuals (28 %) consented to participate and 87 individuals (82 % of those who consented to participate) provided data for this study. The mean (median) age of participants was 80 (81) years (age range was 65–93 years) and the majority (66 %) were female. The majority of participants (56 %) were born in Australia while 17 % were born in the UK; 59 % lived alone and 28 % lived with a spouse or with other family members; and 51 % had obtained a secondary school level of education or lower. The majority of participants (56 %) had an informal carer and indicated that their general health was excellent, very good or good (67 %). All study participants were receiving community support services and therefore required some assistance with activities of day to day living.
Quality of life scores
Table 1 presents quality of life utilities (EQ-5D and ASCOT) and summary scores (OPQol-Brief) according to demographic and other participant characteristics. The mean (standard deviation) for the OPQoL-Brief scores and EQ-5D-3 L and ASCOT utilities were 53.931 (6.685), 0.515 (0.287) and 0.852 (0.141), respectively. When these results were transformed into Z scores, the mean scores for all three instruments were similar (range from −0.016 to −0.000) suggesting unsubstantial variation between the instruments. The ICC between the three instruments showed moderate level of agreement overall (0.54) (results available from authors on request). Generally, and in line with our hypothesis, the direction of the relationships between the utilities/summary scores of all three quality of life instruments and participant characteristics where statistical significance could be established was similar (Table 1). Some deviations from hypothesized directions were evident (Table 1) but these were not statistically significantly different across all three instruments. There were statistically significant differences in EQ-5D-3 L utilities (Kruskal Wallis test, p < 0.05) according to age group (with mean utilities increasing with age) and according to gender (mean utilities higher for males) suggesting that the EQ-5D-3 L was sensitive to age and gender differentiation. In addition, there was a statistically significant relationship between the quality of life utilities/summary scores from all three instruments and self-assessed general health indicating that all instruments discriminated well according to self-assessed general health (Kruskal Wallis test, p value < 0.01).
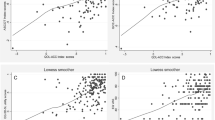
Figures 1a, b and c present scatter plots comparing utilities/summary scores between the OPQoL-Brief and EQ-5D-3 L, OPQoL-Brief and ASCOT and between the EQ-5D-3 L and ASCOT, respectively. All plots show a moderate but statistically significant positive association between the utilities/summary scores (Spearman’s correlation, p value < 0.001): r = 0.53 for OPQoL-Brief versus EQ-5D-3 L, r = 0.58 for OPQoL-Brief versus ASCOT and r = 0.50 for EQ-5D-3 L versus ASCOT. Our hypothesis that the highest level of agreement would be seen between the OPQoL-Brief and ASCOT was accepted. The plots also show that more individuals reported themselves to be in the best state (according to the descriptive systems of each respective instrument) for the EQ-5D-3 L (15 %) compared to the OPQoL-Brief (7 %) and the ASCOT (6 %).

a Scatter plot between OPQoL-Brief and EQ-5D-3 L. b Scatter plot between OPQoL-Brief and ASCOT. c Scatter plot between EQ-5D-3 L and ASCOT
The relationships between individual dimensions of all instruments and between individual dimensions of one instrument relative to utilities/summary scores for each of the comparator instruments are summarised in Table 2. The strongest evidence of convergent validity between dimensions (r = 0.57) was seen in the comparison between ‘enjoy life’ (OPQoL-Brief) and ‘social contact’ (ASCOT). Evidence of moderate convergent validity was seen between other similar dimensions of the OPQoL-Brief and ASCOT such as ‘enjoy life’ (OPQol-Brief) and ‘control over daily life’ (ASCOT) and between ‘healthy to be independent’ (OPQoL-Brief) and ‘occupation/spend time’ (ASCOT). In the comparison between OPQoL-Brief and EQ-5D-3 L dimensions, evidence of moderate convergent validity was also seen between the ‘healthy to get out and about’ (OPQoL-Brief) and the ‘mobility’ and ‘usual activities’ dimensions of the EQ-5D-3 L. Some apparently similar dimensions had low correlation such as ‘healthy to be independent’ (OPQoL-Brief) and ‘mobility’ (EQ-5D-3 L). Low correlation (r ≤ 0.35) was seen between all EQ-5D-3 L and ASCOT dimensions. Overall, the lowest correlations (r < 0.01) were seen between ‘keeping clean and presentable’ on the ASCOT and two dimensions: ‘stay involved with things’ (OPQoL-Brief) and ‘anxiety/depression’ (EQ-5D-3 L). These results show that correlations between all of the dimensions measuring similar constructs were in the direction that was hypothesised but the level of correlation was low or moderate rather than strong. Table 2 also shows that in general, higher correlations were evident between dimensions of particular instruments and utilities/summary scores of comparator instruments than those observed between individual dimensions of comparator instruments.
Tables 3, 4 and 5 present the distribution of EQ-5D-3 L, ASCOT and OPQoL-Brief utilities/summary scores across all dimension levels of comparator instruments. The majority of participants reported themselves having a good quality of life according to the classification systems of all instruments i.e., 69–93 % agreed or strongly agreed with each of the 13 statements in the OPQoL-Brief, 72–100 % reported themselves as living in the best state or had no needs on the ASCOT and 79–98 % had no or some problems on the EQ-5D-3 L dimensions. In general, and in line with our hypothesis, lower OPQoL-Brief, EQ-5D-3 L and ASCOT mean utilities/summary scores were associated with correspondingly increasing levels of severity on the dimensions of comparator instruments. Exceptions were seen for dimensions where the number of participants that chose particular responses within these dimensions was low e.g., for four OPQoL-Brief dimensions (‘I am healthy enough to have my independence’, ‘I have social/leisure activities that I enjoy doing’, ‘I try to stay involved with things’ and ‘I feel lucky compared to most people’). In terms of the ceiling effect for all instruments, the highest proportion reporting ‘strongly agree’ for the OPQoL-Brief was for the ‘I feel safe where I live’ dimension (57 %) and ranged from 22 to 53 % for the other dimensions. For the EQ-5D-3 L, 63 and 52 % reported no problems on the ‘usual activities’ and ‘anxiety/depression’ dimensions, respectively (range for other dimensions was from 15 to 23 %), while at least 70 % reported being in the ‘ideal state’ in relation to four ASCOT dimensions (‘personal cleanliness’, ‘food and drink’, ‘safety’ and ‘dignity’). The range for the percentage reporting being in the ‘ideal state’ on other dimensions was 29–63 %.
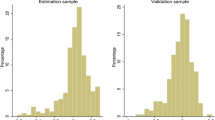
The modified Bland-Altman scatter plots in Fig. 2 show the limits of agreement between the three instruments. The plots suggest moderate agreement between all three instruments with only 3–6 % of Z scores outside the 95 % limits of agreement. As anticipated, the highest agreement (narrower limits of agreement) was between the OPQoL-Brief and the ASCOT (−1.828–1.860), then the OPQoL–Brief and the EQ-5D-3 L (−2.023–2.048) and lastly the EQ-5D-3 L and the ASCOT (−2.067–2.075) though overall the differences between the spans of the limits were marginal.

Modified Bland and Altman Plots. a OPQoL-Brief Z scores vs EQ-5D-3 L Z scores. b OPQoL-Brief Z scores vs ASCOT Z scores. c EQ-5D-3 L Z scores vs ASCOT Z scores
Discussion
While the EQ-5D-3 L and ASCOT have been compared previously [28, 29, 47], this is the first study to directly compare the convergent validity and levels of agreement between the OPQoL-Brief, EQ-5D-3 L and ASCOT in a sample of community-dwelling older people receiving aged care services. As there were moderate levels of agreement between these instruments, our results support the applicability of all three instruments for measuring quality of life outcomes in populations of older people in a community setting. In general, the EQ-5D-3 L focuses more on health related quality of life while the ASCOT and the OPQoL-Brief consider broader aspects of quality of life. The findings from this study indicate that there was more agreement between the OPQoL-Brief and the ASCOT than there was between the OPQoL-Brief and EQ-5D-3 L or between the EQ-5D-3 L and the ASCOT. These findings are consistent with other studies that have shown that the ASCOT is more strongly correlated to instruments that measure broader quality of life than the EQ-5D-3 L [47].
It was found that all three instruments were able to discriminate between groups with known differences based on self-reported ratings of general health with higher mean quality of life utilities and summary scores generally reported for individuals in better general health. Unlike the ASCOT and the OPQOL-Brief, the EQ-5D-3 L was additionally able to discriminate between age groups and gender (females and males). This may suggest that age and gender are stronger predictors of health related quality of life than they are of broader quality of life. Overall, mean EQ-5D-3 L utilities increased with age in our study. This is an unexpected finding and in contrast to a number of other studies from different countries [39, 54, 55]. Further research is recommended before strong conclusions can be drawn about this relationship.
While there was statistically significant correlations in the anticipated direction between dimensions of the three instruments measuring the same constructs, this correlation was at best moderate. Further, comparisons of the utilities and summary scores also showed moderate levels of agreement overall across all instruments with the Z scores showing that the normalized mean scores were all within one standard deviation of each other. At least five reasons may help explain why the level of agreement across all instruments was not stronger. Firstly, there were differences in the ceiling effect amongst the instruments (greater for the EQ-5D-3 L compared to the ASCOT and OPQoL-Brief). Therefore, more individuals reported themselves to have been in full health on the EQ-5D-3 L than on the other two instruments. This result has also been demonstrated in other studies [37, 56] and may be due to the lower number of levels for the EQ-5D-3 L dimensions (i.e., three) compared to other instruments (five for the OPQoL-Brief and four for the ASCOT). The recent development of the new five-level version of the EQ-5D-3 L may minimize this ceiling effect [57]. Secondly, there were only small variations in responses on the dimensions of each of the instruments with most respondents (at least 85 %) classifying themselves within the top two response categories for instrument dimensions . A third explanation, linked to the developmental origins of each instrument, is that there are differences in the descriptive systems of the three instruments with the OPQoL-Brief and ASCOT having more dimensions measuring the same construct than between any other instrument comparisons. Fourthly, it is possible that other factors external to the dimensions of the instruments may have confounded some of the hypothesised relationships. For instance, it is possible that ‘mobility’ (EQ-5D-3 L) is not only dependent on being ‘healthy enough to get out/about’ (OPQoL-Brief) but may be dependent on other factors such as having the financial freedom to be mobile, feeling safe to move around or having activities to go to. Consequently and as also shown elsewhere [58], the associations between dimensions hypothesised to measure the same construct may not be as strong due to confounding relationships not being accounted for. Finally, some of the findings may also be an artefact of the relatively small sample size for this study resulting in small numbers for some of the response categories and therefore potentially exaggerated correlations [59].
Despite both low and moderate correlations being evident between individual dimensions of the three instruments, correlations between the overall utilities and summary scores were all moderate reflecting a level of correlation deemed adequate by previous studies for the purposes of determining that such instruments are interchangeable [47, 58, 60–66]. Indeed what matters to an analyst in the context of an economic evaluation is the mean value of the overall utilities/summary scores and not that of the item responses [67, 68]. We therefore conclude that given this context, all three instruments are applicable for measuring quality of life outcomes in populations of older people in a community setting.
Considering the low conceptual overlap between them, the choice of instrument may be guided by the quality of life measurement-perspective deemed to be the most appropriate in the context within which the instruments are being applied. In circumstances where quality of life needs to reflect changes in health status, the EQ-5D-3 L may be considered to be the most appropriate choice. Where an instrument is needed to measure broader quality of life (i.e., in assessing how the changes in health, aged and social care services received impact on overall quality of life), then the ASCOT should be considered if a utility-based outcome is required (i.e., in the context of cost-utility analysis) or the OPQoL-Brief if a non-preference based outcome is desired.
Study limitations include that participants in this study were essentially a self-selected group who were cognitively intact, fairly healthy and chose to participate in this research. Further, these participants represented just over a fifth of potential study participants initially identified. This therefore meant that our sample may not have been entirely representative of older people receiving consumer aged care services in Australia and that these results will need to be interpreted with this in mind. Nevertheless, we did achieve wide representation across both metropolitan and non-metropolitan areas of two Australian states and the participants exhibited a range of socio-demographic characteristics. There was also no statistically significant difference between responders and non-responders. Secondly, the comparisons made in our study focused on three instruments administered at a single time point. Further research should also be directed at longitudinal assessment to evaluate the performance of instruments in assessing change over time. Additionally, future research could consider extending the comparisons to other instruments designed for application with older people that focus on aspects of quality of life other than those captured by this study such as the ICEpop CAPability measure for Older people (ICECAP-O) [10] and the control, autonomy, self-realisation, and pleasure (CASP) measure of quality of life [69]. Finally, utility algorithms based on the UK general population were used to score the ASCOT and the EQ-5D-3 L. While an Australian general population specific scoring algorithm is available for the EQ-5D-3 L, no such algorithm is available for the ASCOT or the OPQOL-Brief. For consistency, only UK-based algorithms were used for the main analysis. However, similar findings were observed in a secondary analysis when Australian general population EQ-5D-3 L weights were used instead of the UK general population EQ-5D-3 L weights (results available from authors upon request).
In summary, we found that the OPQoL-Brief, the ASCOT and the EQ-5D_3L instruments are suitable for measuring quality of life outcomes in community-dwelling populations of older people. The results of this study support the use of both the OPQoL-Brief and ASCOT as outcome measures in economic evaluations of health and social care interventions targeted at community-dwelling older people who are cognitively intact. In this context both instruments have the attraction of considering broader aspects of quality of life beyond those incorporated within the EQ-5D-3 L which is more narrowly focused upon health status. However, because the OPQoL-Brief is currently not preference-based, its use within economic evaluation is limited.
Given their different perspectives we recommend that both the ASCOT and the EQ-5D are applied simultaneously to capture broader aspects of quality of life and health status within economic evaluations in the aged care sector. Future research to investigate the potential for the incorporation of both health status and broader aspects of quality of life within a single preference based instrument for the calculation of quality adjusted life years within economic evaluations targeted for older people would be beneficial.
References
Australian Bureau of Statistics. Population projections, Australia, 2012 (base) to 2101. Canberra: Australian Bureau of Statistics; 2013.
Australian Bureau of Statistics. 3101.0-Australian demographic statistics, Jun 2014. Canberra: Australian Bureau of Statistics; 2014.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380:37–43.
Muir G. Evidence-based health care and public health: how to make decisions about health services and public health. 3rd ed. London: Churchil Livingstone Elsevier; 2009.
Makai P, Brouwer WB, Koopmanschap MA, Stolk EA, Nieboer AP. Quality of life instruments for economic evaluations in health and social care for older people: a systematic review. Soc Sci Med. 2014;102:83–93.
Drummond MF, Sculpher M, O’Brien B, Stoddart GL, Torrance GW. Methods for the economic evaluation of health care programmes. Oxford: Oxford University Press; 2005.
Harris A, Bulfone L. In: Jost TS, McGraw-Hill International, editors. Health care coverage determinations: an international comparative study. Maidenhead: Open University Press; 2004.
National Institute for Clinical Excellence. Guide to the methods of technology appraisal. London: NICE; 2004.
Ontario Ministry of Health and Long-Term Care. Ontario guidelines for economic analysis of pharmaceutical products. Ontario: Ontario Ministry of Health and Long-Term Care; 1994.
Coast J, Flynn TN, Natarajan L, Sproston K, Lewis J, Louviere JJ, et al. Valuing the ICECAP capability index for older people. Soc Sci Med. 2008;67:874–82.
Ratcliffe J, Laver K, Couzner L, Cameron ID, Gray L, Crotty M. Not just about costs: the role of health economics in facilitating decision making in aged care. Age Ageing. 2010;39:426–9.
Brazier J, Ratcliffe J, Salomon J, Tsuchiya A. Measuring and valuing health benefits for economic evaluation. Oxford: Oxford University Press; 2007.
Browning C, Heine C, Thomas S. Promoting ageing well: psychological contributions. In: Ricciardelli L, Caltabiano M, editors. Applied topics in health psychology. Chichester: Wiley-Blackwell; 2013. p. 57–71.
Australian Human Rights Commission. Human rights approach to ageing and health: respect and choice. Sydney: Australian Human Rights Commission; 2012
Haywood KL, Garratt AM, Fitzpatrick R. Older people specific health status and quality of life: a structured review of self-assessed instruments. J Eval Clin Pract. 2005;11:315–27.
Brazier J, Deverill M, Green C, Harper R, Booth A. A review of the use of health status measures in economic evaluation. Health Technol Assess. 1999;3(9):1–164.
Froberg DG, Kane RL. Methodology for measuring health-state preferences-I: Measurement strategies. J Clin Epidemiol. 1989;42:345–54.
Campbell DT, Fiske DW. Convergent and discriminant validation by the multitrait-multimethod matrix. Psychol Bull. 1959;56:81–105.
Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86:420–8.
Bowling A, Hankins M, Windle G, Bilotta C, Grant R. A short measure of quality of life in older age: the performance of the brief older People’s quality of life questionnaire (OPQOL-brief). Arch Gerontol Geriatr. 2013;56:181–7.
Netten A, Burge P, Malley J, Potoglou D, Towers AM, Brazier J, et al. Outcomes of social care for adults: developing a preference-weighted measure. Health Technol Assess. 2012;16:1–166.
Dolan P, Roberts J. Modelling valuations for Eq-5d health states: an alternative model using differences in valuations. Med Care. 2002;40:442–6.
Reisberg B, Ferris SH, de Leon MJ, Crook T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am J Psychiatry. 1982;139:1136–9.
Kaambwa B, Lancsar E, McCaffrey N, Chen G, Gill L, Cameron ID, et al. Investigating consumers‘and informal carers’ views and preferences for consumer directed care: a discrete choice experiment. Soc Sci Med. 2015;140:81–94.
Bowling A, Stenner P. Which measure of quality of life performs best in older age? a comparison of the OPQOL, CASP-19 and WHOQOL-OLD. J Epidemiol Community Health. 2011;65:273–80.
Bowling A. The psychometric properties of the older People’s quality of life questionnaire compared with the CASP-19 and the WHOQOL-OLD. Curr Gerontol Geriatr Res. 2009.
Milte CM, Walker R, Luszcz MA, Lancsar E, Kaambwa B, Ratcliffe J. How important is health status in defining quality of life for older people? An exploratory study of the views of older South Australians. Appl Health Econ Health Policy. 2014;12:73–84.
Malley J, Towers A-M, Netten A, Brazier J, Forder J, Flynn T. An assessment of the construct validity of the ASCOT measure of social care-related quality of life with older people. Health Qual Life Outcomes. 2012;10:21.
Forder J, Caiels J. Measuring the outcomes of long-term care. Soc Sci Med. 2011;73:1766–74.
Netten A, Beadle-Brown J, Caiels J, Forder J, Malley J, Smith N, et al. Adult social care outcomes toolkit: main guidance v2.1-PSSRU discussion paper 2716/3. Kent: PSSRU; 2011.
Netten A, Forder J, Malley J, Smith N, Towers A. Adult Social Care Outcomes Toolkit-Additional guidance: Scoring ASCOT v2.1. Kent: PSSRU; 2011.
Coast J, Peters TJ, Richards SH, Gunnell DJ. Use of the EuroQoL among elderly acute care patients. Qual Life Res. 1998;7:1–10.
Brazier JE, Walters SJ, Nicholl JP, Kohler B. Using the SF-36 and euroqol on an elderly population. Qual Life Res. 1996;5:195–204.
Lyons RA, Crome P, Monaghan S, Killalea D, Daley JA. Health status and disability among elderly people in three UK districts. Age Ageing. 1997;26:203–9.
van den Bos GA, Triemstra AH. Quality of life as an instrument for need assessment and outcome assessment of health care in chronic patients. Qual Health Care. 1999;8:247–52.
Dolan P. Modeling valuations for EuroQol health states. Med Care. 1997;35:1095–108.
Brazier J, Roberts J, Tsuchiya A, Busschbach J. A comparison of the EQ-5D and SF-6D across seven patient groups. Health Econ. 2004;13:873–84.
Viney R, Norman R, Brazier J, Cronin P, King MT, Ratcliffe J, et al. An Australian discrete choice experiment to value eq-5d health states. Health Econ. 2014;23:729–42.
Kind P, Hardman G, Macran S. UK population norms for EQ-5D: discussion paper 172, Centre for health economics discussion paper series. York: University of York: Centre for Health Economics; 1999.
Kind P, Dolan P, Gudex C, Williams A. Variations in population health status: results from a United Kingdom national questionnaire survey. Bmj. 1998;316:736–41.
Shapiro SS, Wilk MB. An analysis of variance test for normality (complete samples). Biometrika. 1965;52:591–611.
Altman DG. Practical statistics for medical research. London: Chapman & Hall/CRC; 1991.
Dancey C, Reidy J. Statistics without maths for psychology: using SPSS for windows. London: Prentice-Hall; 2004.
Allen J, Inder K, Lewin T, Attia J, Kelly B. Construct validity of the assessment of quality of life-6D (AQoL-6D) in community samples. Health Qual Life Outcomes. 2013;11:61.
Mulhern B, Meadows K. The construct validity and responsiveness of the EQ-5D, SF-6D and Diabetes Health Profile-18 in type 2 diabetes. Health Qual Life Outcomes. 2014;12:42.
Peters LL, Boter H, Slaets JP, Buskens E. Development and measurement properties of the self assessment version of the INTERMED for the elderly to assess case complexity. J Psychosom Res. 2013;74:518–22.
van Leeuwen KM, Bosmans JE, Jansen APD, Hoogendijk EO, van Tulder MW, van der Horst HE, et al. Comparing measurement properties of the EQ-5D-3 L, ICECAP-O, and ASCOT in frail older adults. Value in Health. 2015;18:35–43.
StataCorp LP. Intercooled Stata 13.1 for Windows, College station. Texas: StataCorp, L.P; 2014.
Harrison WW, Bearse Jr MA, Ng JS, Barez S, Schneck ME, Adams AJ. Reproducibility of the mfERG between instruments. Doc Ophthalmol. 2009;119:67–78.
Petreca DR, Benedetti TRB, Silva DAS. Validation of the flexibility component of the AAHPERD functional fitness assessment in Brazilian older adults. Revista Brasileira de Cineantropometria Desempenho Humano. 2011;13:455–60.
van Hateren KJ, Alkhalaf A, Kleefstra N, Groenier KH, de Jong PE, de Zeeuw D, et al. Comparison of midregional pro-A-type natriuretic peptide and the N-terminal pro-B-type natriuretic peptide for predicting mortality and cardiovascular events. Clin Chem. 2012;58:293–7.
Bross IDJ. Critical levels, statistical language and scientific inference. In: Godambe VP, Sprott DA, editors. Foundations of statistical inference. Toronto: Holt, Rinehart & Winston of Canada, Ltd; 1971.
Abdi H. The bonferonni and šidák corrections for multiple comparisons. In: Salkind NJ, editor. Encyclopedia of measurement and statistics. Sage: Thousand Oaks; 2007. p. 103–7.
Burstrom K, Johannesson M, Diderichsen F. Swedish population health-related quality of life results using the EQ-5D. Qual Life Res. 2001;10:621–35.
Luo N, Johnson JA, Shaw JW, Feeny D, Coons SJ. Self-reported health status of the general adult U.S. population as assessed by the EQ-5D and Health Utilities Index. Med Care. 2005;43:1078–86.
Wu J, Han Y, Zhao F-L, Zhou J, Chen Z, Sun H. Validation and comparison of EuroQoL-5 dimension (EQ-5D) and Short Form-6 dimension (SF-6D) among stable angina patients. Health Qual Life Outcomes. 2014;12:156.
Janssen MF, Birnie E, Bonsel GJ. Quantification of the level descriptors for the standard EQ-5D three-level system and a five-level version according to two methods. Qual Life Res. 2008;17:463–73.
Coast J, Peters T, Natarajan L, Sproston K, Flynn T. An assessment of the construct validity of the descriptive system for the ICECAP capability measure for older people. Qual Life Res. 2008;17:967–76.
Fisher RA. On the probable error of a coefficient of correlation deduced from a small sample. Metron. 1921;1:3–32.
Chen G, Flynn T, Stevens K, Brazier J, Huynh E, Sawyer M, et al. Assessing the health-related quality of life of Australian adolescents: an empirical comparison of the child health utility 9D and EQ-5D-Y instruments. Value Health. 2015;18:432–8.
Ratcliffe J, Stevens K, Flynn T, Brazier J, Sawyer M. An assessment of the construct validity of the CHU9D in the Australian adolescent general population. Qual Life Res. 2012;21:717–25.
Stockler MR, Osoba D, Corey P, Goodwin PJ, Tannock IF. Convergent discriminitive, and predictive validity of the prostate cancer specific quality of life instrument (PROSQOLI) assessment and comparison with analogous scales from the EORTC QLQ-C30 and a trial-specific module. J Clin Epidemiol. 1999;52:653–66.
Chren M-M, Lasek RJ, Quinn LM, Covinsky KE. Convergent and discriminant validity of a generic and a disease-specific instrument to measure quality of life in patients with skin disease. J Investig Dermatol. 1997;108:103–7.
Mehta T, Venkata Subramaniam A, Chetter I, McCollum P. Assessing the validity and responsiveness of disease-specific quality of life instruments in intermittent claudication. Eur J Vasc Endovasc Surg. 2006;31:46–52.
Hughes TE, Kaplan RM, Coons SJ, Draugalis JR, Johnson JA, Patterson TL. Construct validities of the Quality of Well-Being Scale and the MOS-HIV-34 Health Survey for HIV-infected patients. Med Decis Making. 1997;17:439–46.
Rockwood TH, Church JM, Fleshman JW, Kane RL, Mavrantonis C, Thorson AG, et al. Fecal incontinence quality of life scale: quality of life instrument for patients with fecal incontinence. Dis Colon Rectum. 2000;43:9–16. discussion 16–17.
Kaambwa B, Billingham L, Bryan S. Mapping utility scores from the Barthel index. Eur J Health Econ. 2011.
Sengupta N, Nichol MB, Wu J, Globe D. Mapping the SF-12 to the HUI3 and VAS in a managed care population. Med Care. 2004;42:927–37.
Sexton E, King-Kallimanis BL, Conroy RM, Hickey A. Psychometric evaluation of the CASP-19 quality of life scale in an older Irish cohort. Qual Life Res. 2013;22:2549–59.
Hoi L, Chuc N, Lindholm L. Health-related quality of life, and its determinants, among older people in rural Vietnam. BMC Public Health. 2010;10:549.
Yohannes AM, Tampubolon G. Determinants of quality of life in older people from the english longitudinal study of ageing. European Psychiatry. 2012;27:1.
Gott M, Barnes S, Parker C, Payne S, Seamark D, Gariballa S, et al. Predictors of the quality of life of older people with heart failure recruited from primary care. Age Ageing. 2006;35:172–7.
Lubetkin E, Jia H, Franks P, Gold M. Relationship among sociodemographic factors, clinical conditions, and health-related quality of life: Examining the EQ-5D in the U.S. general population. Qual Life Res. 2005;14:2187–96.
Hellström Y, Hallberg IR. Perspectives of elderly people receiving home help on health, care and quality of life. Health Soc Care Community. 2001;9:61–71.
Konig HH, Bernert S, Angermeyer MC, Matschinger H, Martinez M, Vilagut G, et al. Comparison of population health status in six european countries: results of a representative survey using the EQ-5D questionnaire. Med Care. 2009;47:255–61.
Acknowledgments
This work was supported through an Australian Research Council Linkage Project (grant number LP110200079). Additional financial contributions were received from the following aged care organisations: ACH Group, Catholic Community Services, Hammondcare, Helping Hand and Resthaven.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
All authors declare that they have no competing of interest.
Authors’ contributions
JR, EL, IDC, MC and LG contributed to the study inception and writing of the Australian Research Council (ARC) linkage grant application. BK & JR analysed the data, interpreted the results and wrote the first draft of the manuscript. LG and NM made revisions to the first draft. All authors contributed to the interpretation of results and revision of the manuscript. All authors have read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kaambwa, B., Gill, L., McCaffrey, N. et al. An empirical comparison of the OPQoL-Brief, EQ-5D-3 L and ASCOT in a community dwelling population of older people. Health Qual Life Outcomes 13, 164 (2015). https://doi.org/10.1186/s12955-015-0357-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-015-0357-7