
Abstract
Background
Evidence on the social determinants of mental health conditions and violence among people who inject or use drugs (PWUD) is limited, particularly in conflict-affected countries. We estimated the prevalence of symptoms of anxiety or depression and experience of emotional or physical violence among PWUD in Kachin State in Myanmar and examined their association with structural determinants, focusing on types of past migration (migration for any reason, economic or forced displacement).
Materials
A cross-sectional survey was conducted among PWUD attending a harm reduction centre between July and November 2021 in Kachin State, Myanmar. We used logistic regression models to measure associations between past migration, economic migration and forced displacement on two outcomes (1) symptoms of anxiety or depression (Patient Health Questionnaire-4) and (2) physical or emotional violence (last 12 months), adjusted for key confounders.
Results
A total of 406, predominantly male (96.8%), PWUD were recruited. The median age (IQR) was 30 (25, 37) years, most injected drugs (81.5%) and more commonly opioid substances such as heroin or opium (85%). Symptoms of anxiety or depression (PHQ4 ≥ 6) were high (32.8%) as was physical or emotional violence in the last 12 months (61.8%). Almost one-third (28.3%) had not lived in Waingmaw for their whole life (migration for any reason), 77.9% had left home for work at some point (economic migration) and 19.5% had been forced to leave home due to war or armed conflict (forced displacement). A third were in unstable housing in the last 3 months (30.1%) and reported going hungry in the last 12 months (27.7%). Only forced displacement was associated with symptoms of anxiety or depression [adjusted odds ratio, aOR 2.33 (95% confidence interval, CI 1.32–4.11)] and recent experience of violence [aOR 2.18 (95% CI 1.15–4.15)].
Conclusion
Findings highlight the importance of mental health services integrated into existing harm reduction services to address high levels of anxiety or depression among PWUD, particularly among those who have been displaced through armed conflict or war. Findings reinforce the need to address broader social determinants, in the form of food poverty, unstable housing and stigma, in order to reduce mental health and violence.
Similar content being viewed by others


Background
In 2020, an estimated 275 million people globally used drugs for non-medical purposes [1]. Greater use is reported in countries with higher levels of drug production, such as Afghanistan, Mexico and Myanmar, which share 95% of the global opium production [1]. Myanmar is also one of the world's leading amphetamine-type stimulants (ATS) producers. Methamphetamine is the most popular type of ATS in the market, and the use is in increasing trend [2].
Within Myanmar, drug production areas such as Kachin State, Northern Shan State and the Sagaing Region have the highest prevalence of drug use among the population [2, 3]. Elevated drug use in these contexts is thought to be attributable to increased availability of drugs and consequent changes in social norms. Increased drug use is thought to be a coping mechanism in response to increasing psychological distress and poor economic prospects as a result of historically decades of prolonged conflict between ethnic armed groups and state actors and forced displacement [4,5,6,7,8,9]. Evidence from Myanmar also shows a link between working in mining industries and opium, heroin or stimulant use, with drugs used as a way of coping with difficult working conditions [10]. For example, estimates of injecting drug use within Kachin State, where jade and gold mines are a common industry, are 5% among 15–49-year-old men compared to the national prevalence of 0.3% (15–64 years) [11,12,13].
There are also 912,000 internally displaced persons (IDPs) in Myanmar due to decades of conflict and violence, with the largest population in Kachin, Chin, Shan and Rakhine States [14]. This forced displacement can detrimentally affect health, creating disparities in social, economic and cultural opportunities, resulting in discrimination and racism, as well as reduced access to quality health care [15]. These factors are all linked with an increased risk of developing poor mental health and poorer outcomes [9, 16,17,18]. A meta-analysis reported that the prevalence of depression among displaced people, such as refugees, migrants, asylum seekers and IDPs, was 26.4%, and one-fourth of migrants suffer from depression globally [19].
Poor mental health conditions are a major source of mortality and morbidity globally [20]. People who use drugs can be more vulnerable to poor mental health due to homelessness, ill health and unemployment, compounded by stigma and the criminalised nature of drug use in most contexts [21, 22]. A global systematic review reported a high prevalence of severe depressive symptoms (42.0%), depression diagnosis (28.7%) and suicidal attempts (22.1%) among people who inject drugs (PWID) [23]. Evidence suggests that poor mental health can exacerbate drug-related outcomes, including increased risk of overdose, injecting-related injuries, injecting risk behaviours and acquiring HIV in people who use or inject drugs (PWUD) [23,24,25].
Studies have also documented heightened exposure to physical violence among people who use drugs across various settings [26, 27]. Aside from physical injury, violence can lead to poorer mental health, including post-traumatic stress disorder and anxiety, avoidance of health services and engagement in behaviours that can increase the risk of HIV acquisition [27,28,29]. Despite the documented need and the clear interplay between mental health, violence and HIV risk, screening and treatment of psychological conditions or violence have not been prioritised in the comprehensive harm reduction package recommended by the World Health Organization (WHO) and the implementation of mental health services in harm reduction interventions is limited [30]. Consequently, the experience of violence is neither routinely assessed nor documented, leading to missed opportunities for treatment and support.
The risk environment concept developed to understand drug-related harms examines how different types (physical, social, economic and political) and levels (macro and micro) of environmental influence shape health among people who use drugs, in line with broader efforts to address structural determinants of health [31]. Epidemiological evidence shows structural factors (e.g. law, housing, economic insecurity, stigma, displacement), community factors (e.g. policing practices, access to services) and individual behaviours (e.g. sharing needles/syringes) increase vulnerability to HIV and hepatitis C infection among PWID [31,32,33,34]. There is a growing body of evidence documenting the epidemiology of HIV among PWID in Myanmar, showing a high prevalence (35%) nationally and higher in Kachin State (54%) [12]. However, there has been little consideration of their structural determinants and a lack of evidence on the experience of violence or mental health conditions [35].
There is an urgent need to better understand the broader health and welfare of PWUD in Myanmar and their determinants to inform integrated prevention and intervention strategies. Drawing on data from a cross-sectional survey of PWUD in Kachin State, Myanmar, we estimate the prevalence of symptoms of depression or anxiety and experience of emotional or physical violence in the last 12 months. We examine their association with structural determinants, focusing on types of past migration (migration for any reason, economic or forced displacement).
Methods
Study design and setting
Kachin State has one of the largest populations of IDPs in Myanmar as well as migrants moving to work in gold and jade mines [36, 37]. United Nations agencies, international and local non-governmental organisations (NGOs) in collaboration with ethnic health organisations and faith-based organisations deliver services to IDPs, including the provision of shelter, non-food items, protection, health, education, nutrition, livelihoods, and access to clean water, sanitation and good hygiene practices. In contrast, services for migrant workers are limited. Harm reduction services are also provided by international and local NGOs in Kachin, and project sites are systematically divided among implementers to avoid services overlapping.
Since 2003, the Asian Harm Reduction Network (AHRN) has been implementing a comprehensive “one-stop-shop” harm reduction cascade of services in Kachin State and progressively expanded to Shan State and Sagaing Region. There are now 35 service delivery sites in three states and regions in Myanmar [38]. The Waingmaw centre was selected for this cross-sectional study because of high levels of drug use, including both injecting heroin and increased use of amphetamine and associated high prevalence of HIV (54%), HCV (85%) and other health needs among PWUD. There is also a sizeable mobile population and historically frequent outbreaks of conflict likely to produce particular health needs among the population, but which have not yet been researched [12]. Harm reduction services at Waingmaw service centre include psychosocial counselling, social support, health education, distribution of needles and syringes, condoms, facilitating access to methadone maintenance therapy (MMT), provision of HIV, TB and viral hepatitis prevention, diagnostics and treatment, overdose management, and other medical services through drop-in centres, key population service centres, mobile medical teams, outreach and community-based activities [39].
In Myanmar key population service centres are targeted towards men who have sex with men, PWID and sex workers and other vulnerable population including people who (non-injecting) use drugs and sexual partner of PWUD. They contain dedicated spaces for recreational activities and provide medical care such as primary health care, standard infectious and non-infectious disease screening, diagnosis and treatment. Screening and treatment services for most common psychological disorders such as depression and psychosis were first introduced to the key population service centre model in 2016 using the Mental Health Gap Action Programme (mhGAP), and it was expanded to many harm reduction facilities after 2017 [40]. Yet, mental health treatment options are limited, and some psychological disorders require referral to specialist care facilities. In Myanmar, public hospitals are the main sources of mental health services and drug treatment provision [2].
Study population and sampling design
We conducted a clinic-based cross-sectional study using structured questionnaires in Waingmaw, Kachin State, Myanmar. The study was a collaboration between the AHRN and the London School of Hygiene and Tropical Medicine. PWUD, routinely identified by the clinic centre staff, who visited the clinic during the survey period between 16th July and 2nd November 2021, were invited to participate in the survey by AHRN's centre staff or a research interviewer. All available clients were invited to participate, and informed consent was obtained if they were eligible, interested, and had time to complete the questionnaire. Participants were eligible if they had: (i) used drugs (heroin or amphetamines) at least once in the last 3 months; (ii) were 14 years or older, and (iii) able to give consent. After completing the questionnaire, participants received 5000 MMK (~ 2.7 USD) in recognition for their time.
Questionnaire and data collection
Following informed consent, interviews were conducted by four interviewers trained in research ethics, data collection procedures, and COVID-19 infection control measures in a private space at the centre. Interviewers administered a structured questionnaire in Burmese using a tablet (Open Data Kit V.1 28.4). Data were collected on demographics, health and service use, mental and physical health, drug use characteristics, violence and sexual practices, and stigma. Indicators were drawn from validated measures and other surveys among PWUD [41, 42]. The questionnaires were translated into Burmese by KWKY. We extracted HIV and HCV status from patient records in the clinic where available. If no test had been conducted or they had not been tested in the past 6 months, and their last test was negative, participants were offered to test and referred to the AHRN's on-site counsellor and laboratory technician.
Outcomes
Our primary outcome was symptoms of anxiety or depression over the last 2 weeks measured through a validated composite measure (Patient Health Questionnaire-4, PHQ4) comprising two items from the Public Health Questionnaire focusing on depressed mood and loss of interest and two items from Generalised Anxiety Disorder scale (feeling anxious or inability to control worrying) [43]. The reliability of the PHQ4 with the study population was assessed using Cronbach's alpha, and it was 0.79, indicating an acceptable/strong level of internal reliability. We took the sum of the four items and made a binary outcome variable (Score 0–5 and ≥ 6) which has been validated as a reliable brief measure of depression or anxiety in other contexts [43].
As a secondary outcome, we measured experience of recent (last 12 months) either physical or emotional violence. The violence questions were developed based on the operational definition and questionnaire used in WHO multi-country study on women's health and domestic violence against women [42]. Physical violence was defined as being pushed, shoved, slapped, kicked, punched, choked, dragged, burnt, had a weapon against him/her, thrown something at him/her, or beaten him/her up. Emotional violence was defined as being called in a derogatory term (for example, opium-eater). A participant was classified as being subject to recent violence if they affirmed any of the violence questions.
Co-variables
Our three key explanatory variables were defined as: (i) being a migrant (not living in Waingmaw township for the whole life); (ii) economic migration (ever left the home community for work); and (iii) forced displacement as an IDP (ever left the home community because of war or armed conflict). We considered stigma related to drug use and other structural factors for their hypothesised relationships with mental health and violence. 'Enacted Stigma' related to drug use was measured using the substance-use stigma mechanisms scale (SU-SMS) and concerned the experience of stigma within families and among health care workers [44]. The responses were given on a Likert scale of 1–5, with higher scores indicating greater endorsement of substance-use stigma. Average scores for sub-scales of enacted stigma for family members and health care workers were calculated, and stigma level was categorised using median scores.
Other factors considered included ethnicity (Kachin, Shan, Pa'O, Bamar, other), education (no school, primary, middle, high school, college), main source of income in the last 3 months (casual labourer, farming, office job, government job, army, shop or market worker, from parents/other relatives, from spouse, lover or friend's income, sex for money, no money to live on), housing status in the last 3 months (stable housing including own place, parents' house, rented private room and unstable housing including someone else's house, an IDP camp, sleeping on somebody's sofa/floor, squatting, having no fixed address, drug treatment institution, drug rehabilitation centre, jail or prison, and work-provided accommodation), and food insufficiency in the last 12 months (defined as being hungry and did not eat because you could not afford to buy enough food).
Patterns of drug use variables included type of drug use in the last 3 months (amphetamine-type stimulants (ATS) with or without opioid substance, opioid substances without ATS), mode (injecting, non-injecting) and location of drug use in the last 3 months (private place such as home and public places including places where they bought drugs, on the street, around the bushes, shooting galleries, public toilets, and workplace). Health care accessibility variables included type of current treatment (religious-based psyche-social support, government rehabilitation programme with overnight stay/ as day visit, private doctor, self-help/community support, methadone maintenance, counselling, NGO clinic), having outreach workers' visits in the last 12 months (yes/no).
Statistical analyses
We examined univariable associations using logistic regression in separate models for each explanatory variable and each outcome. Variables significantly associated with outcomes (P < 0.05) in univariable analysis, and a priori confounders were included in multivariable models. For multivariable models, we adjusted for the following confounders for their association with migration and mental health and violence: age, housing, main income from farming in the last 3 months and type of drug used. We considered the presence of anxiety or depression symptoms and location of drug use variables as additional a priori confounders for the outcome of recent exposure to physical or emotional violence. We present crude odds ratio (OR) and adjusted odds ratio (aOR) with the 95% confidence interval (CI) produced from the models. All the analyses were done in Stata version 17.0 (Stata Corp, US).
Results
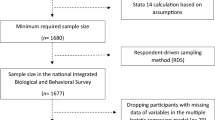
Of the 1,237 unique PWUD who attended the service in Waingmaw during the recruitment period, some 417/1237 (33.8%) were screened and eligible for the study, while the remainder (n = 820, 66.2%) were not screened as they had then left clinics before meeting the interviewers. The comparative table presenting the characteristics of PWUD by screening status has been reported as Additional file 1. Of those who were screened, 406/417 (97.1%) clients provided consent. Ten of eleven recruits who declined consent reported time limitation as a reason, and one client said they were afraid of identifying as a drug user.
Characteristics of study participants are presented in Table 1. The median age of participants was 30 (IQR 25, 37) years. The majority were male (96.8%), 69.7% were of Kachin ethnicity, and a quarter (25.6%) had no school or primary school level education. The median age of first drug use was 20 (IQR 18–25) years, 81.5% had ever injected drugs, and over half (56.2%) injected drugs daily in the last 4 weeks. Heroin or opium was the main drug used (85.0%), but 15.0% used ATS with or without opioid substances in the last 3 months). Casual labour was the main source of income for 48.0% of participants, and 7.4% of respondents had no money in the last 3 months. One-third (28.1%) had ever had suicidal thoughts, and 13.2% had ever attempted suicide. Overall, 64.4% had antibodies to HIV and 78.7% had antibodies to HCV.
Other social determinants
Approximately a third of participants (27.7%) had felt hungry in the last 12 months or lived in unstable housing (30.1%) in the last 3 months. Within the previous 12 months of the survey, 26.8% were stopped by police or anti-drugs squad, and 7.6% were detained. The most common reason for the arrest was drug possession or drug use (38.3%), followed by theft or robbery (36.2%). The median average stigma score experienced within families was 2 (IQR 1–3), while for experience from health care workers was 1 (IQR 1–1). More than half (54.3%) of respondents had ever taken any treatment to modify or reduce or stop drug use, and 35.5% were on treatment at the time of the survey, with 51.3% (40/78) on methadone. In the last 12 months prior to the survey, 20.9% had outreach workers' visits, 74.0% had ever had an HIV test, and 57.3% had ever had an HCV test. HIV, HCV and dual infections positivity were 64.4%, 78.7% and 55.6%.
Migration
Overall, 28.3% of participants were identified as migrants (defined as those who had not been living in Waingmaw for their whole life), 77.9% reported economic migration (defined as those who had ever left the home community for work), and 19.5% had ever experienced forced displacement (defined as those who had ever left the home community because of war or armed conflict).
Violence and mental health
Overall, 61.0% of participants (n = 246/403) had experienced recent emotional violence. The most common perpetrators were family members (n = 131, 33.5%), strangers (n = 96, 24.6%) and friends (n = 91, 23.3%). Twenty-five participants (6.4%) reported intimate partner as perpetrator of emotion violence. Less than 10% of study participants experienced recent physical violence (n = 37/404, 9.2%). The most common perpetrators were strangers (n = 9, 23.1%), family members (n = 8, 20.5%), friends (n = 7, 18.0%) and police (n = 6, 15.4%). There was no participant who reported intimate partner as the perpetrator of physical violence. Almost two-thirds (n = 251, 61.8%) of respondents reported recent experience of physical or emotional violence. More than two-thirds (67.2%) of respondents had symptoms of anxiety or depression (PHQ4 score 6 or more).
Effect of migration on symptoms of anxiety or depression
We found no evidence that past migration was associated with symptoms of anxiety or depression [aOR 2.1 (95% CI 0.86–5.11)]. Among other social determinants, there was evidence that people who had experiencing stigma within families (≥ 2 average stigma score) had 1.7 times higher odds of symptoms of anxiety or depression [aOR 1.67 (95% CI 1.02–2.72)], relative to those who had experiences less stigma.
We found no evidence that economic migration was associated with symptoms of anxiety or depression [aOR 0.95 (95% CI 0.53–1.71)]. There was some evidence that experiencing emotional violence in the last 12 months was associated with increased odds of symptoms of anxiety or depression [aOR 1.70 (95% CI 1.01–2.84)].
We found evidence that people who had experienced forced displacement had 2.3 times higher odds of symptoms of anxiety or depression [aOR 2.33 (95% CI 1.32–4.11)], relative to those who had not experienced forced displacement. Participants experiencing higher stigma within families had higher odds of having symptoms of anxiety or depression [aOR 1.73 (95% CI 1.05–2.83)].
In all three models, there was evidence that going hungry in the last 12 months was associated with increased odds of symptoms of anxiety or depression, whereas participants reporting farming as a main source of income in the last 3 months had lower odds of symptoms of anxiety or depression than those whose income was from other sources (mining, logging, driving vehicles, skilled works and selling) (Table 2). The separate analysis of depression and anxiety is presented in Additional file 1: Tables S1, S2 and S3.
Effect of migration on physical or emotional violence
We found no evidence that past migration was associated with recent physical or emotional violence [aOR 0.89 (95% CI 0.53–1.48)]. However, there was evidence that the presence of symptoms of anxiety or depression [aOR 1.77 (95% CI 1.07–2.94)] was associated with increased odds of physical or emotional violence.
We found no evidence that economic migration was associated with recent physical or emotional violence [aOR 1.21 (95% CI 0.70–2.07)]. There was evidence that those who had symptoms of anxiety or depression had greater odds of recent physical or emotional violence [aOR 1.87 (95% 1.12–3.12)].
There was evidence that forced displacement was associated with higher odds of exposure to physical or emotional violence [aOR 2.18 (95% CI 1.15–4.15)]. In all three models, participants reporting high stigma scores within families had higher odds of physical or emotional violence, while being on methadone was associated with reduced odds of physical or emotional violence (Table 3).
Discussion
To the best of our knowledge, this is the first study reporting mental health and recent physical or emotional violence among PWUD and their association with migration and other social determinants in Myanmar. We observed a high prevalence of symptoms of anxiety or depression (32.8%). One in ten PWUD had experienced physical violence in the last year, and six in ten had experienced emotional violence in the form of verbal abuse. In an examination of the effect of different forms of migration on mental health and violence, only forced displacement was associated with increased odds of both symptoms of depression or anxiety and experience of physical or emotional violence. We also found evidence that experiencing stigma from family members was associated with both symptoms of anxiety or depression and physical and emotional violence in all models.
One-third of participants reported symptoms of anxiety or depression in our study, almost a third had ever had suicidal thoughts, and 13% had ever attempted suicide. Prevalence of symptoms of anxiety or depression is in line with other evidence from a systematic review, reporting the presence of severe depression symptoms in 42.0% of PWID, and Ukraine's study on PWID living with HIV, showing poor mental health conditions among PWID and highlights the imperative to include mental health services within the harm reduction cascade of service delivery [23, 45]. Besides, the link between mental health conditions and substance use disorder was reported elsewhere [46, 47]. Findings also highlight the precarious conditions in which PWUD live in Kachin, a third of whom had the experience of unstable housing in the last 3 months and food insecurity in the last 12 months and a quarter of whom have been stopped by the police or anti-drugs squad in the last 12 months, indicators of extreme marginalisation linked to poor mental health in other settings [21, 48].
The link between poor mental health and conflict has been well established. A global review estimated the prevalence of depression to be 10.8% and any anxiety disorder at 21.7% among people affected by conflict; among our sample 1 in three participants reported symptoms of anxiety or depression, and prevalence and odds were higher among those who had been displaced due to armed conflict or war [16]. Due to the cross-sectional design of the study, it is impossible to establish the temporal sequencing between displacement, initiation into drug use and the onset of poor mental health. However, findings suggest that the already high levels of poor mental health conditions among people who use drugs are attenuated among those displaced as a result of armed conflict and war. Evidence from other regions shows that drug use among people living in or displaced from conflict-affected countries is more frequent due to increased drug availability, changing social norms or structure, lacking economic opportunities, and coping with trauma [4]. Mental health services should be made available widely in harm reduction settings, and health facilities providing care to PWUD in conflict-affected areas should be person-tailored to individual needs of internally displaced persons, including psychological support, income generation, facilitating social integration process and referral mechanisms for coping with ongoing stressors and improving access to essential health care [49].
We failed to find any evidence to support or refute our hypothesis that past experience of migration (for any reason) or migration for work was associated with poor mental health or experience of emotional or physical violence. This may be related to the imprecision of the question that failed to capture specific aspects of vulnerability faced by these types of migration and heterogeneous nature of characteristics among them [50]. Evidence shows a complex relationship between migration and health, with health outcomes confounded by pre-migration experiences, socio-economic status, the availability and agency of host communities for migrants that could possibly lead to healthier conditions and reduced isolation [51]. In contrast with those forcibly displaced who are more likely to live in temporary housing or emergency accommodation in often overcrowded conditions and less able to integrate with host communities or access to health services [15, 19]. Further research in Myanmar is needed to understand the additional vulnerabilities that forced displacement as opposed to economic migration, has for PWUD.
The findings add to growing evidence of the interplay between stigma, mental health, and violence [7, 52, 53]. More than half of the participants had experienced physical or emotional violence in the last 12 months, and this was associated with symptoms of anxiety or depression. Our finding of more stigma experienced within families than in healthcare settings is possibly a consequence of our sampling strategy that focused on a harm reduction service where staff are likely to be more sensitised to drug use. We found evidence that experiencing stigma from family members was associated with both symptoms of anxiety and depression and recent violence. Family members' behaviours toward PWUD, who were found to be the most common perpetrators of emotional violence in our study, could also be linked to social stigma and the considerable psychological distress they experience [54]. It also may reflect stigma toward drug use in society more broadly, where widespread poverty intersects with long-standing conflict, drug production and drug use, creating conditions where poor health thrives, as is most clearly evident in the large-scale epidemics of HIV linked to drug injecting [12].
The gross domestic product per capita income of a quarter of the Myanmar population was below the poverty line. Besides, food insecurity is high in conflict-affected border states, including Kachin state, due to increasing market prices of rice and cooking oil and compromised life and livelihoods of the population [55, 56]. Other evidence shows a clear relationship between drug use-related stigma and mental health conditions linked with the experience of violence, which can increase vulnerability to violence, particularly among women [53, 57], while stigma also negatively affects overall health and the uptake of health services [58, 59].
Addressing widespread stigma towards people who use drugs is complicated and requires substantial cultural changes within communities and society more broadly. Efforts should be undertaken include raising awareness about the availability and effectiveness of drug treatment services, the promotion of alternatives to imprisonment for drug offences in recognition of the negative social and health consequences for PWUD, their families and communities, as well as reducing the negative portrayal of drug use alongside violence and crime in social and mainstream media [54, 60]. Longer-term initiatives are also required, such as addressing poverty and homelessness that increase stigma towards PWUD as well as perpetuating drug use [61].
We found evidence of an association between methadone and reduced odds of physical and emotional violence. While we are unable to elucidate the pathways between methadone and emotional or physical violence, evidence from a linked qualitative study among PWUD in Bhamo and Waingmaw in Kachin State suggests that the provision of methadone plays an important role in relieving economic pressure, affording people opportunities to work rather than finding and paying for their own methadone or other drugs and exacerbating already precarious livelihoods [62].
The study had several limitations. The study was cross-sectional in nature and cannot determine the temporal relationship or causality. The use of convenience sampling of clinic attendance in place of the planned respondent-driven sampling was necessary due to security constraints but limits the inferences we can make on the representativeness of findings to other PWUD in Kachin state, particularly to the large population living in rural areas who will have reduced access to clinics in townships. Findings are also drawn from self-reports which may be subject to reporting bias, particularly given the sensitive nature of questions in relation to mental health and violence.
Our study focused on measuring three forms of migration experience as a primary exposure, and models adjust for confounders associated with these exposures and our outcomes. We report the effect estimates for confounders and other covariates associated with the outcomes but note the limitations of this approach and that other unmeasured factors may confound these estimates [63]. These are reported here given the exploratory nature of the analysis and in the absence of research to inform interventions among a highly marginalised group but should be interpreted with caution.
Reports of physical violence were lower than anticipated (9.2%), given the context of conflict. Further research is needed to corroborate and understand the experience of violence. Measures used for assessing mental health outcomes reported on symptoms, and they are not diagnostic. They have also not been psychometrically tested and validated in Myanmar; however, they have been used across different settings, and findings suggest high internal reliability in our study (Cronbach's α = 0.79) [64, 65]. We could not recruit many women into the study, reflecting the gender profile of PWUD attending the centre, who are predominantly male and the highly stigmatised and hidden nature of drug use among women [66]. There is an urgent need for more research to understand the health needs among women who use or inject drugs in the region to inform appropriate services, especially in relation to violence [67].
Conclusions
The high prevalence of symptoms of anxiety or depression and physical or emotional violence in Kachin State supports the need to integrate harm reduction services with interventions to address mental health and violence. Findings point to the need for expanded mental health services in Myanmar among PWUD, particularly with internally displaced persons. There is a need for longer-term policy and social changes to address broader determinants of the marginalisation of PWUD, including addressing poverty, stigma and forced displacement. In the short term, our findings highlight opportunities to address the immediate health needs of PWUD in relation to mental health and violence within harm reduction services to improve the health and well-being of this highly marginalised population.
Availability of data and materials
The data sets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AHRN:
-
Asian Harm Reduction Network
- aOR:
-
Adjusted odds ratio
- ATS:
-
Amphetamine-type stimulants
- CI:
-
Confidence interval
- col:
-
Column
- HCV:
-
Hepatitis C virus
- HIV:
-
Human Immunodeficiency virus
- IDP:
-
Internally displaced person
- IQR:
-
Interquartile range
- mhGAP:
-
Mental Health Gap Action Programme
- MMT:
-
Methadone maintenance therapy
- n:
-
Number
- NGO:
-
Non-governmental organisation
- OR:
-
Unadjusted odds ratio
- ORW:
-
Outreach worker
- PHQ-4:
-
Patient Health Questionnaire-4
- PWID:
-
People who inject drugs
- PWUD:
-
People who use or inject drugs
- ref:
-
Reference
- UK:
-
United Kingdom
- USD:
-
United States Dollar
- WHO:
-
World Health Organization
References
UNODC. World drug report 2021: global overview: drug demand and drug supply. United Nations Office on Drugs and Crime; 2021.
Ministry of Health and Sports. National Strategic framework for health and drugs. Nay Pyi Taw: Ministry of Health and Sports; 2020.
UNODC. World drug report 2021: executive summary, policy implications. United Nations Office on Drugs and Crime; 2021.
Jack H, Reese Masterson A, Khoshnood K. Violent conflict and opiate use in low and middle-income countries: a systematic review. Int J Drug Policy. 2014;25(2):196–203.
Guarino H, Ruggles KV, Mateu-Gelabert P, Quinn K, Syckes C, Friedman SR. Adverse childhood experiences predict early initiation of opioid use behaviors. Front Sociol. 2021;6:620395.
Huang C, Yuan Q, Zhang L, Wang L, Cui S, Zhang K, et al. Associations between childhood trauma and the age of first-time drug use in methamphetamine-dependent patients. Front Sociol. 2021;12:658205.
Sagram J, Lee W, Choi J, Milloy M-J, Hayashi K, DeBeck K, et al. Childhood physical abuse and subsequent violent victimization among people who use illegal drugs in Vancouver, Canada. PLOS ONE. 2021;16(8):e0255875.
Prangnell A, Imtiaz S, Karamouzian M, Hayashi K. Childhood abuse as a risk factor for injection drug use: a systematic review of observational studies. Drug Alcohol Rev. 2020;39(1):71–82.
World Health Organization. Mental health and forced displacement 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-and-forced-displacement.
Bouchon M, Quétie M. Perceptions about drug use and harm reduction in Kachin, Myanmar MDM; 2018.
Department of population. Census atlas Myanmar: the 2014 Myanmar population and housing census. Ministry of Labour, Immigration and Population 2014.
National AIDS Program. Myanmar integrated biological and behavioural surveilliance survey & population size estimates among people who inject drugs (2017–2018). Nay Pyi Taw: Ministry of Health and Sports; 2019.
National AIDS Program. 2016 HIV estimates & projections (National & Sub-National Levels). Nay Pyi Taw: Ministry of Health and Sports; 2018 March, 2018.
UNOCHA. Myanmar humanitarian update no. 17. United Nations Office for the Coordination of Humanitarian Affairs; 2022 19/04/2022.
Cantor D, Swartz J, Roberts B, Abbara A, Ager A, Bhutta ZA, et al. Understanding the health needs of internally displaced persons: a scoping review. J Migr Health. 2021;4:100071.
Charlson F, Van Ommeren M, Flaxman A, Cornett J, Whiteford H, Saxena S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet. 2019;394(10194):240–8.
Porter M, Haslam N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons. JAMA. 2005;294(5):602.
Meyer SR, Lasater M, Tol WA. Migration and mental health in low- and middle-income countries: a systematic review. Psychiatry. 2017;80(4):374–81.
Bedaso A, Duko B. Epidemiology of depression among displaced people: a systematic review and meta-analysis. Psychiatry Res. 2022; 114493.
Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. 2016;3(2):171–8.
Degenhardt L, Peacock A, Colledge S, Leung J, Grebely J, Vickerman P, et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: a multistage systematic review. Lancet Glob Health. 2017;5(12):e1192–207.
Larney S, Peacock A, Mathers BM, Hickman M, Degenhardt L. A systematic review of injecting-related injury and disease among people who inject drugs. Drug Alcohol Depend. 2017;171:39–49.
Colledge S, Larney S, Peacock A, Leung J, Hickman M, Grebely J, et al. Depression, post-traumatic stress disorder, suicidality and self-harm among people who inject drugs: a systematic review and meta-analysis. Drug Alcohol Depend. 2020;207:107793.
Tomko C, Schneider KE, Rouhani S, Urquhart GJ, Park JN, Morris M, et al. Identifying pathways to recent non-fatal overdose among people who use opioids non-medically: How do psychological pain and unmet mental health need contribute to overdose risk? Addict Behav. 2022;127:1–7.
Remiena RH, Stirrattb MJ, Nguyena N, Robbinsa RN, Palaa AN, Mellinsa CA. Mental health and HIV/AIDS: the need for an integrated response. AIDS. 2019;33:1411–20.
Kennedy MC, Hayashi K, Milloy MJ, Boyd J, Wood E, Kerr T. Supervised injection facility use and exposure to violence among a cohort of people who inject drugs: a gender-based analysis. Int J Drug Policy. 2020;78:102692.
Braitstein P, Li K, Tyndall M, Spittal P, O'Shaughnessy MV, Schilder A, et al. Sexual violence among a cohort of injection drug users: University of British Columbia; 2001.
Daigre C, Rodriguez-Cintas L, Tarifa N, Rodriguez-Martos L, Grau-Lopez L, Berenguer M, et al. History of sexual, emotional or physical abuse and psychiatric comorbidity in substance-dependent patients. Psychiatry Res. 2015;229(3):743–9.
Schneider R, Cronkite R, Timko C. Lifetime physical and sexual abuse and substance use treatment outcomes in men. J Subst Abuse Treat. 2008;35(4):353–61.
United Nations Office on Drugs and Crime. Implementing comprehensive HIV and HCV programmes with people who inject drugs, practical guidance for collaborative interventions; 2017.
Rhodes T. Risk environments and drug harms: a social science for harm reduction approach. Int J Drug Policy. 2009;20:193–201.
Myers B, Petersen Z, Pithey A, Pasche S, Dada S. Barriers to antiretroviral therapy use among people who inject drugs: a systematic review. Alcohol and Drug Abuse Research Unit, South African Medical Research Council; 2012.
Debeck K, Cheng T, Montaner JS, Beyrer C, Elliott R, Sherman S, et al. HIV and the criminalisation of drug use among people who inject drugs: a systematic review. Lancet HIV. 2017;4(8):e357–74.
Marmot M. Social determinants of health inequalities. Lancet. 2005;365:1099–104.
O’Brien S, Jaramillo MM, Roberts B, Platt L. Determinants of health among people who use illicit drugs in the conflict-affected countries of Afghanistan, Colombia and Myanmar: a systematic review of epidemiological evidence. Confl Heal. 2022;16(1):1–20.
Gupta S. Leveraging migration for development: a review of literature on patterns and movements in Myanmar (working paper). UNOPS; 2016.
UNOCHA. Myanmar humanitarian update No. 23. United Nations Office for the Coordination of Humanitarian Affairs; 2022 31/10/2022.
Asian Harm Reduction Network—Myanmar: Yangon, Myanmar; Available from: https://ahrnmyanmar.org/about-ahrn/overview/.
Shwe Yee N, Naing AY, Cuesta JG, Das M, Dave K. Gaps in hepatitis B vaccination completion and sero-protection for people who inject drugs in Hpakant, Myanmar, 2015–2018. Trop Med Infect Dis. 2020;5(77):1–11.
World Health Organization. mhGAP intervention guide for mental, neurological and substance use disorders in non-specialized health settings (Version 2.0). Geneva: World Health Organization; 2016.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13.
García-Moreno C, Jansen HAFM, Ellsberg M, Heise L, Watts C. WHO multi-country study on women’s health and domestic violence against women. Geneva: World Health Organization; 2005.
Löwe B, Wahl I, Rose M, Spitzer C, Glaesmer H, Wingenfeld K, et al. A 4-item measure of depression and anxiety: validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord. 2010;122:86–95.
Smitha LR, Earnshawb VA, Copenhaverc MM, Cunninghamd CO. Substance use stigma: reliability and validity of a theory-based scale for substance-using populations. Drug Alcohol Depend. 2017;162:34–43.
Vasylyev M, Davtyan H, Denisiuk O, Chadwick Jayaraj J, Koval T, Piddubna A, et al. Anxiety, depression, and quality of life among HIV positive injection drug users in Ukraine, 2017. J Infect Dev Ctries. 2019;13(7S):111S-S117.
Ross S, Peselow E. Co-occurring psychotic and addictive disorders. Clin Neuropharmacol. 2012;35(5):235.
National Institute of Mental Health. Substance use and co-occurring mental disorders 2021 updated March 2021. Available from: https://www.nimh.nih.gov/health/topics/substance-use-and-mental-health.
Arum C, Fraser H, Artenie AA, Bivegete S, Trickey A, Alary M, et al. Homelessness, unstable housing, and risk of HIV and hepatitis C virus acquisition among people who inject drugs: a systematic review and meta-analysis. Lancet. 2021;6:e309–23.
Miller KE, Rasmussen A. The mental health of civilians displaced by armed conflict: an ecological model of refugee distress. Epidemiol Psychiatr Sci. 2017;26(2):129–38.
Foo S, Tam W, Ho C, Tran B, Nguyen L, McIntyre R, et al. Prevalence of depression among migrants: a systematic review and meta-analysis. Int J Environ Res Public Health. 2018;15(9):1986.
Fernández-Reino M. The health of migrants in the UK 2020 updated 21/08/2020.
World Health Organziation. World report on violence and health. Geneva: World Health Organization; 2002.
Keyser-Marcus L, Alvanzo A, Rieckmann T, Thacker L, Sepulveda A, Forcehimes A, et al. Trauma, gender, and mental health symptoms in individuals with substance use disorders. J Interpers Violence. 2015;30(1):3–24.
Thein KZK, Herberholz C, Sandar WP. Caring for persons with drug use disorders in the Yangon Region, Myanmar: Socioeconomic and psychological burden, coping strategies and barriers to coping. PLOS ONE. 2021;16(10):e0258183.
World Food Program. WFP Myanmar country brief. World Food Program; 2020.
World Food Program. Myanmar: analysis of the economic fallout and food insecurity in wake of the takeover. World Food Program; 2021.
Couto e Cruz C, Salom CL, Dietze P, Burns L, Alati R. The association between experiencing discrimination and physical and mental health among people who inject drugs. Int J Drug Policy. 2019;65:24–30.
Wolfe D, Luhmann N, Harris M, Momenghalibaf A, Albers E, Byrne J, et al. Human rights and access to hepatitis C treatment for people who inject drugs. Int J Drug Policy. 2015;26(11):1072–80.
Reid G, Sharma M, Higgs P. The long winding road of opioid substitution therapy implementation in South-East Asia: challenges to scale up. J Public Health Res. 2014;3(1):jphr2014.
Central Committee for Drug Abuse Control. National drug control policy. Central Committee for Drug Abuse Control; 2018.
National Academies of Sciences Engineering and Medicine. Ending discrimination against people with mental and substance use disorders: the evidence for stigma change. In: Understanding stigma of mental and substance use disorders. US: National Academies Press (US); 2016.
Rhodes T, Kyaw KWY, Harris M. Precarious lives, precarious treatments: making drug treatment work in Northern Myanmar. Med Anthropol. 2022;1–18.
Westreich D, Greenland S. The table 2 fallacy: presenting and interpreting confounder and modifier coefficients. Am J Epidemiol. 2013;177(4):292–8.
Kriengtuntiwong T, Zaw YH, Taneepanichskul N. Brain-derived neurotrophic factor (BDNF) depression and subjective sleep quality in the first trimester of pregnancy among migrant workers in Thailand. J Multidiscip Healthc. 2021;14:2549–56.
Theingi P, Kamiya Y, Myat Moe M, Cho San C, Cox SE. Depression and its associated factors among people with multidrug-resistant tuberculosis in Myanmar. Tropical Med Int Health. 2021;26(9):1117–26.
Meyers SA, Earnshaw VA, D’Ambrosio B, Courchesne N, Werb D, Smith LR. The intersection of gender and drug use-related stigma: a mixed methods systematic review and synthesis of the literature. Drug Alcohol Depend. 2021;223: 108706.
UNFPA Asia and the Pacific Regional Office. kNOwVAWdata Phase I Report. 2021.
Acknowledgements
We acknowledge the AHRN's service users, the respondents who participated in this survey, the field staff who collected data, the AHRN staff and all stakeholders who supported the smooth implementation of the survey.
Funding
This work is supported by the ESRC, Drugs and (dis)order: Building sustainable peacetime economies in the aftermath of war, UKRI Award no. ES/P011543/1, 2017–2021, as part of the Global Challenges Research Fund. The funder had no role in the design of the study, collection, analysis, interpretation of data and writing of the manuscript.
Author information
Authors and Affiliations
Contributions
KWYK, LP, BR and SDR contributed to conception, design, acquisition and analysis. KWYK, LP, BR, SDR, MB and AYN interpreted the data, drafted or substantively revised the manuscript. KWYK, LP, MB, AYN, SDR and BR approved the submitted version. KWYK, LP, MB, AYN, SDR and BR are personally accountable for the author's own contributions, ensuring that questions are related to the accuracy or integrity of any part of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained for participating in the survey and linking HIV/HCV testing data with AHRN's centre records before the interview. Ethics approval was obtained from the ethics board of the London School of Hygiene and Tropical Medicine, UK, and the Institutional review board of the Department of Medical Research, Ministry of Health and Sports, Myanmar.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1
Characteristics of PWUD who were screened and not screened during their visit to the Waingmaw AHRN clinic during the survey period. Table S2 Factors associated with symptoms of depression among survey clients (n = 406). Table S3 Factors associated with symptoms of anxiety among survey clients (n = 406)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kyaw, K.W.Y., Platt, L., Bijl, M. et al. The effect of different types of migration on symptoms of anxiety or depression and experience of violence among people who use or inject drugs in Kachin State, Myanmar. Harm Reduct J 20, 45 (2023). https://doi.org/10.1186/s12954-023-00766-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12954-023-00766-1