
Abstract
Background
The ratio between non-high-density lipoprotein cholesterol and high-density lipoprotein cholesterol (NHHR) is a reliable marker for assessing the risk linked to lipid metabolism disorders. Sarcopenia, characterized by age-related loss of muscle mass and strength/function, includes the assessment of muscle mass, muscle strength, and muscle-specific strength. However, research into NHHR’s relationship with low muscle mass risk remains unexplored.
Methods
Our study utilized a cross-sectional approach, examining data derived from the National Health and Nutrition Examination Survey (NHANES) from 2011 to 2018. Through multivariable linear and logistic regression, we investigated the relationships of the NHHR with muscle mass and low muscle mass. We visualized the results using smoothing curves and assessed threshold effects. We also performed various subgroup and sensitivity analyses.
Results
This research encompassed 9,012 participants and demonstrated significant nonlinear associations between NHHR and ALMBMI or low muscle mass risk in a generalized additive model (GAM), pinpointing critical NHHR values (3.328 and 3.367) where changes in NHHR significantly impacted ALMBMI and low muscle mass risk.
Conclusions
The NHHR demonstrates a significant association with an increased risk of low muscle mass among middle-aged Americans. This ratio has potential as a predictive marker for low muscle mass. Further exploration of NHHR is expected to aid in advancing preventive and therapeutic measures for this condition.
Similar content being viewed by others


Introduction
Sarcopenia, characterized as a progressive and widespread disorder, predominantly impacts skeletal muscle, especially in the elderly population [1]. Previous definitions were continent- and region-specific. Recently, the Global Leadership Initiative in Sarcopenia (GLIS) has established the first global conceptual definition of sarcopenia, which includes muscle mass, strength, and muscle-specific strength as key components, through a rigorous and transparent International Delphi Consensus process involving experts from all major sarcopenia societies worldwide [2]. Globally, the estimated prevalence of sarcopenia within the general population ranges from 5–10% [3]. It affects daily functioning, increases the risk of falls, and reduces independence. Moreover, sarcopenia is linked to negative health consequences, such as fractures, osteoporosis, and cancer [4,5,6,7]. Dual-energy x-ray absorptiometry (DEXA) is a validated and commonly employed method for measuring skeletal muscle mass [8]. The appendicular lean mass to body mass index (ALMBMI) is acknowledged as a crucial indicator for evaluating muscle mass. The musculoskeletal system is essential for the human body to function normally. Therefore, having access to clinically relevant data is crucial for the early identification and prevention of sarcopenia. Several factors contribute to muscle mass reduction and the onset of sarcopenia, including aging, physical inactivity, neuromuscular dysfunction, energy intake, macronutrient and micronutrient intake, and changes in several hormones (insulin, sex hormones, thyroid hormones, glucocorticoids) [9,10,11,12].
Fatty acids and lipid metabolism intermediates play a vital role in the regulation of skeletal muscle mass and function [13]. The buildup of these lipids and their byproducts in muscle cells and surrounding spaces can induce lipid toxicity. Such accumulation triggers oxidative stress, impairs mitochondrial function, causes inflammation, and induces insulin resistance, all of which negatively impact muscle health [14]. Recent studies have recognized sarcopenia as a standalone risk factor for non-alcoholic fatty liver disease (NAFLD), which is often associated with various metabolic conditions, particularly dyslipidemia [15]. Patients with this condition often exhibit hypertriglyceridemia and reduced HDL cholesterol levels [16]. Elevated levels of LDL and homocysteine are recognized as risk factors for sarcopenia [17]. A prominent study conducted by Sunyoung Kang and colleagues in South Korea identified a strong inverse association between muscle strength and the prevalence of dyslipidemia and obesity; as muscle strength increased, the incidence of these conditions significantly declined [18]. Dyslipidemia may intensify the risk of sarcopenia via mechanisms that include insulin resistance, the inflammatory response, and oxidative stress. A recently discovered marker, the ratio of non-HDL to HDL cholesterol (NHHR), can independently predict the risk of NAFLD [19]. As an essential component of sarcopenia, low muscle mass can partially indicate the onset of this condition. Nevertheless, the connection between NHHR and low muscle mass remains unexplored, and the link between NHHR and muscle mass is yet to be determined. Consequently, we conducted a study utilizing NHANES data spanning from 2011 to 2018. We proposed that elevated NHHR levels would result in decreased muscle mass and a higher prevalence of low muscle mass. This study explored a newly identified area regarding the potential application of NHHR as a predictor for muscle mass.
Materials and methods
Data source and study population
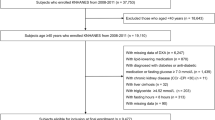
This research utilized data from the NHANES across four cycles from 2011 to 2018 to investigate the association between NHHR and muscle mass, along with the prevalence of low muscle mass. The methodology for selecting participants is depicted in Fig. 1. Initially, individuals lacking limb lean body mass data (n = 21,230) and those with incomplete NHHR records (n = 1,381) were excluded. Furthermore, participants under the age of 20 were not included in the study. An additional 2259 subjects missing other crucial variables were also excluded. The final analysis encompassed 9,012 adults who had a complete dataset. All participants underwent evaluations for their physical and medical status via health screenings performed at mobile facilities and standardized home interviews. The survey was overseen and implemented by the NCHS. The NCHS Research Ethics Review Board approved the ethical application of NHANES involving human subjects, and each participant provided informed consent.

Flowchart of participant selection
Assessment of NHHR
In the exposure assessment, NHHR was calculated as the dependent variable using the participants’ lipid profiles. The formula applied was NHHR = non-HDL-C/HDL-C, where non-HDL-C was derived by subtracting HDL-C from total cholesterol.
Assessment of appendix lean mass and low muscle mass
From 2011 to 2018, DEXA scans were administered to participants aged 20 to 59. Exclusion criteria included pregnancy, recent barium contrast imaging (within the last week), a body weight exceeding 450 pounds, or a height greater than 6 feet 5 inches. ALM for eligible participants was calculated by deducting bone mineral content from the total lean mass of the limbs. ALMBMI was subsequently computed by dividing ALM by the BMI. Following the criteria from the FNIH, low muscle mass was characterized by an ALMBMI of less than 0.789 kg for males and less than 0.512 kg for females.
Covariables
To mitigate potential confounding effects in the association between NHHR and ALMBMI, multivariable adjustment models were employed. Covariables included in the analysis were gender, age, race, hypertension, diabetes, PIR, cancer, sleep disorders, and education level. In addition, the parameters of interest in our study include daily intake measurements of energy, protein, carbohydrates, and fat, along with alcohol intake. Smoking is assessed through the measurement of cotinine levels in the blood (ng/ml). The methods for collecting these variables are extensively documented in the NHANES Survey Methods and Analysis.
Statistical analysis
For statistical analysis in this study, we utilized EmpowerStats 4.1 and R software (version 4.2.3). All analyses were conducted using the recommended weighting procedures for NHANES data to ensure representativeness. We used the Rao-Scott chi-square test for categorical variables and one-way ANOVA for continuous variables to account for the complex survey design. We established statistical significance at a p-value of less than 0.05. We divided the NHHR into four quartiles, ranging from the lowest (Q1) to the highest (Q4). Continuous variables were summarized using means and standard deviations (SDs), and categorical variables were presented as proportions. Multivariable linear and logistic regression analyses were conducted to explore the associations between NHHR and ALMBMI or low muscle mass using three progressive models. To assess the nonlinear relationship between NHHR and the outcomes, smoothed curves were fitted using the generalized additive model (GAM). In evaluating the model’s fit, the effective degrees of freedom (edf) for each predictor were carefully examined. An edf value closer to 1 suggests a nearly linear relationship, whereas higher values indicate increased nonlinearity and complexity in the relationship. Model 1 was unadjusted. Model 2 included adjustments for gender, age, and race. Model 3 further adjusted for educational attainment, hypertension, diabetes, cancer, and sleep disorders. Results were expressed as regression coefficients (β) and odds ratios (OR), both with 95% confidence intervals (CI). After adjusting for all confounders, we utilized smooth curve fitting and threshold effect analysis to assess the relationship between NHHR and ALMBMI, aiming to identify critical inflection points. Furthermore, subgroup analyses were executed to investigate the association between NHHR and ALMBMI or low muscle mass across various demographics and health statuses. Protein, fat, energy, and carbohydrate intakes were categorized into low and high groups, and we conducted interaction tests to examine the consistency of the associations across these subgroups.
Results
Characteristics of participants
Table 1 displays the participant characteristics, sorted by NHHR quartiles. The quartile ranges for NHHR were 36.69 ± 11.84, 38.39 ± 11.82, 40.45 ± 11.24 and 41.10 ± 10.51. Significant age differences were noted among the groups (one-way ANOVA, p < 0.001) with average ages spanning from 36.69 to 41.10 years. Significant differences in gender distribution were also observed (Rao-Scott chi-square test, p < 0.001) with the percentage of males increasing from 32.49% in Q1 to 67.36% in Q4. The smoothed curves indicated a nonlinear relationship between NHHR and the outcomes. Therefore, we reported the results using NHHR quartiles instead of treating NHHR as a continuous variable. Marked racial and educational attainment disparities were observed (p < 0.001). Notably, the proportion of Mexican Americans rose from 10.74% in Q1 to 18.38% in Q4, while the percentage of participants with education beyond high school decreased from 68.53 to 55.09% over the same interval. Health status indicators also showed significant variation: the prevalence of hypertension increased from 16.42% in Q1 to 28.43% in Q4 (p < 0.001), and diabetes rates varied significantly (p < 0.001). No significant differences were observed in cancer prevalence (p = 0.557). Furthermore, significant increases in the PIR were noted from the first to the fourth quartile (p < 0.001). Notably, dietary intake metrics increased significantly; energy intake escalated from 2188.86 kcal in Q1 to 2333.88 kcal in Q4 (p < 0.001), protein intake increased from 84.43 g to 89.55 g (p < 0.001), and carbohydrate intake rose from 251.52 g to 284.14 g (p < 0.001). Although changes in fat intake were not statistically significant (p = 0.077), indicating stability, there was a substantial decrease in alcohol consumption, from 15.52 g in Q1 to 10.24 g in Q4 (p < 0.001). Additionally, cotinine levels increased from 53.62 ng/ml in Q1 to 80.26 ng/ml in Q4 (p < 0.001), reflecting potential changes in smoking behaviors or exposure. The prevalence of low muscle mass escalated significantly, from 4.39% in Q1 to 12.13% in Q4 (p < 0.001).
Relationship between NHHR and skeletal muscle mass
The results revealed a statistically significant negative association between elevated NHHR and ALMBMI. For sensitivity analysis, NHHR was categorized into quartiles; in the fully adjusted model (Model 3), the effect size for the fourth quartile was notably negative (β = -0.068, 95% CI: -0.074 to -0.061, P < 0.00001) compared to the first quartile. Concerning low muscle mass incidence, the study identified a positive relationship between an increase in NHHR and the likelihood of developing low muscle mass. Additionally, further analysis indicated that participants in the Q4 were at a 1.981-fold greater risk of developing low muscle mass compared to those in the Q1 in the fully-adjusted model (95% CI: 1.538 to 2.551, P < 0.00001), reinforcing the observed association between higher NHHR and increased low muscle mass risk. These findings highlight the impact of NHHR on ALMBMI and the risk of low muscle mass, emphasizing the importance of considering NHHR in clinical assessments and potential interventions aimed at mitigating these risks.
Nonlinear association between the NHHR and skeletal muscle mass
These results investigated the nonlinear associations between NHHR and ALMBMI and the risk of sarcopenia, as illustrated in Figs. 2 and 3. The majority of the samples in this study are concentrated within the 0–10 range of the NHHR (Figs. 2B and 3B). A significant edf of 5.6482 indicates a non-linear fit between NHHR and ALMBMI, and an edf of 4.6307 indicates a non-linear relationship with the occurrence of low muscle mass (Table S1). Detailed analyses of smooth curves demonstrated a nonlinear relationship between ALMBMI and NHHR (Fig. 2A). Similarly, nonlinear patterns were observed in the analyses concerning the risk of developing low muscle mass (Fig. 2B). The association between NHHR and ALMBMI and the risk of sarcopenia was statistically significant, with p < 0.00001.
Utilizing a biphasic linear model and recursive algorithms, the research identified critical turning points at NHHR values of 3.328 and 3.367 (Tables 4 and 5). Below an NHHR of 3.328, each unit increase in NHHR was linked to a decrease of 0.036 in ALMBMI (β = -0.036, 95% CI: -0.039 to -0.032). No significant changes were noted in ALMBMI above this NHHR value. Moreover, when NHHR was less than 3.367, each unit increase resulted in a 45.3% increase in the odds of low muscle mass onset (OR: 1.453, 95% CI: 1.281 to 1.649). Conversely, above an NHHR of 3.367, the relative risk of low muscle mass remained unchanged, indicating a plateau in effect at higher NHHR levels.

The dose-response relationship between NHHR and ALMBMI (A) and Concentration of Samples (B)

The dose-response relationship between NHHR and low muscle mass (A) and Concentration of Samples (B)
Subgroup analysis
The detailed subgroup analysis in the data reveals distinct patterns across various demographic and health-related variables. Gender-specific results indicate a beta coefficient of -0.015 (95% CI: -0.017, -0.013) for males and − 0.012 (95% CI: -0.014, -0.009) for females. Age analysis suggests stronger associations in individuals aged 40 and above (-0.019; 95% CI: -0.022, -0.017) than those below 40 (-0.010; 95% CI:-0.012,-0.007). Educational attainment also demonstrates variations, with the most significant effect observed in those above high school (-0.017; 95% CI:-0.019,-0.015). The PIR analysis yields no significant interactions, with coefficients remaining relatively stable across categories. Health conditions such as hypertension, diabetes, and sleep disorders also influence the outcomes. Additionally, dietary intake variables like energy, protein, carbohydrate, and fat intake exhibit slight variations in their associations with the studied outcomes.
The stability of the link between NHHR and low muscle mass was examined via subgroup analysis, detailed in Table 6. Despite comprehensive scrutiny, the p-values for interactions (P > 0.05), except in the diabetes subgroup, showed no significant association, indicating that factors such as age, gender, race, education level, family PIR, hypertension, cancer status, and sleep disorders did not markedly affect this connection between NHHR and the occurrence of low muscle mass. The findings indicate that this association remains consistent across various demographic groups.
Discussion
This cross-sectional study involved 9,012 participants. A negative association between NHHR and ALMBMI was observed. It appears that an increase in NHHR may elevate low muscle mass risk. Further analyses using smoothed curve fitting and threshold effects revealed a nonlinear association between NHHR and muscle mass. These findings imply that managing NHHR, a widely accessible clinical measure, could enhance muscle mass and decrease low muscle mass incidence. In our study of the relationship between NHHR and low muscle mass, we identified significant discrepancies in the definitions and diagnostic criteria for sarcopenia. These discrepancies have a considerable impact on research outcomes. Most definitions of sarcopenia focus on the loss of muscle strength, muscle mass, and function. However, there is a lack of consensus on the exact diagnostic criteria for sarcopenia. Clinically, there are various methods to measure sarcopenia, including bioelectrical impedance analysis (BIA), DEXA, and computed tomography (CT). Each of these methods has its own diagnostic criteria and effectively assesses muscle mass and strength. Additionally, grip strength and timed up-and-go tests are used to assess muscle functionality to determine the impact of sarcopenia. Depending on the method, criteria, and population used, the results may vary significantly. During our research period, these standards were updated. The GLIS has recently developed a unified global conceptual definition of sarcopenia, which includes muscle mass, muscle strength, and muscle-specific strength as key components [20]. This new definition aims to harmonize the various existing definitions and improve the comparability of research findings across different studies.
Sarcopenia represents a significant public health issue, incurring substantial healthcare costs and adding to the annual disease burden. The combination of resistance exercise and adequate protein intake as a clinical intervention effectively prevents the development of sarcopenia [21]. Recent studies indicate that changes in lipid metabolism and fatty infiltration in muscle tissues are key characteristics of sarcopenia and aging [22]. These alterations contribute to muscle insulin resistance and ceramide accumulation [23]. During aging, oxidative damage and the accumulation of intracellular lipid droplets in muscle tissue impair mitochondrial oxidative phosphorylation. This impairment leads to muscle metabolic disorders and adversely affects muscle function [24]. The research examined the connection between NHHR, muscle mass, and the likelihood of low muscle mass development. Notably, appropriate inflection points were identified at NHHR values of 3.328 and 3.367. It is important to highlight that when NHHR was below 3.367, each unit increase in NHHR resulted in a 45.3% increase in the likelihood of developing sarcopenia. Increasing evidence suggests that NHHR accurately predicts the risk of lipid metabolism-related disorders [19, 25]. Despite the absence of direct studies investigating the link between sarcopenia and NHHR, numerous studies on lipid metabolism have identified associations between low muscle mass and various lipid-related factors. Several meta-analyses have confirmed that serum triglyceride levels are positively associated with the development of sarcopenia, whereas HDL-C levels are negatively associated. Additionally, these associations are influenced by factors such as gender and age [26, 27]. Moreover, numerous studies involving middle-aged and older adults in China and Korea have identified a negative association between the TG/HDL-C ratio and sarcopenia [28,29,30]. This ratio also exhibits a negative association with grip strength [31]. Furthermore, research involving older adults has indicated that sarcopenia development is linked to lipid metabolism disorders, especially those involving VLDL and RLP-C [32]. Dyslipidemia may elevate the risk of developing sarcopenia through pathways including insulin resistance, inflammation, and oxidative stress. Research has shown that in sarcopenia patients, increased oxidative stress and higher plasma levels of 7-ketocholesterol and 7β-hydroxycholesterol correlate with elevated secretion of inflammatory indicators such as TNF-α and IL-8 [33]. Our study demonstrated a significant association between elevated NHHR and low muscle mass, a key component of sarcopenia. The NHHR was initially developed to assess the extent of atherosclerosis, going beyond conventional lipid parameters [34]. It has been strongly associated with insulin resistance [35], NAFLD [36], metabolic syndrome [37], and both the occurrence and recurrence of kidney stones [38], showcasing its superior predictive capabilities. Given that blood biochemistry tests are a standard procedure in clinical practice, NHHR is both accessible and cost-effective, making it highly beneficial for widespread application.
Strengths and limitations
The main strength of our research lies in its focus on the nonlinear relationship between NHHR and low muscle mass, with our findings gaining credibility and representativeness from substantial sample size and meticulous adjustment for covariables. Additionally, the diagnosis of myasthenia gravis and the acquisition of NHHR data were based on DEXA scans and laboratory tests, minimizing subjectivity and avoiding recall bias. Nonetheless, our study faces several limitations. The cross-sectional nature of our study limits the ability to determine causality, highlighting the need for prospective studies for further clarification. Moreover, despite adjusting for numerous confounders, as suggested by prior research and clinical practice, the influence of unmeasured or unknown variables on our results cannot be fully excluded.
Conclusions
In conclusion, the results of this study indicate a negative association between NHHR and muscle mass, as well as a positive association with the increased prevalence of low muscle mass. This implies that NHHR could function as a new predictor of low muscle mass which is a key component of sarcopenia. Clinicians could utilize the NHHR to identify individuals at risk for low muscle mass and to implement appropriate interventions as needed. Further research, including prospective studies and randomized controlled trials, is necessary to substantiate these conclusions. Furthermore, additional research is necessary to clarify the underlying mechanisms.
Data availability
The NHANES data utilized in this study are accessible to the public and can be obtained from the following link: https://www.cdc.gov/nchs/nhanes.
Abbreviations
- non-HDL-C:
-
Non-high-density lipoprotein cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- NHHR:
-
Non-HDL-C and HDL-C ratio
- PIR:
-
Poverty-to-income ratio
- BMI:
-
Body mass index
- TC:
-
Total Cholesterol
- NCHS:
-
National Center for Health Statistics
- FNIH:
-
Foundation for the National Institutes of Health
- RLP-C:
-
Remnant Lipoprotein Cholesterol
- VLDL:
-
Very Low-Density Lipoprotein
- LDL:
-
Low-Density Lipoprotein
- PIR:
-
Poverty income ratio
- TNF-α:
-
Tumor Necrosis Factor-alpha
- IL-8:
-
Interleukin-8
- ALM:
-
Appendicular lean mass
References
Sayer AA, Cruz-Jentoft A. Sarcopenia definition, diagnosis, and treatment: consensus is growing. Age Ageing. 2022;51(10).
Kirk B, Cawthon PM, Arai H, Ávila-Funes JA, Barazzoni R, Bhasin S et al. The conceptual definition of Sarcopenia: Delphi Consensus from the Global Leadership Initiative in Sarcopenia (GLIS). Age Ageing. 2024;53(3).
Golabi P, Gerber L, Paik JM, Deshpande R, de Avila L, Younossi ZM. Contribution of Sarcopenia and physical inactivity to mortality in people with non-alcoholic fatty liver disease. JHEP Reports: Innov Hepatol. 2020;2(6):100171.
Wiedmer P, Jung T, Castro JP, Pomatto LCD, Sun PY, Davies KJA, et al. Sarcopenia - Molecular mechanisms and open questions. Ageing Res Rev. 2021;65:101200.
Papadopoulou SK, Papadimitriou K, Voulgaridou G, Georgaki E, Tsotidou E, Zantidou O et al. Exercise and Nutrition Impact on osteoporosis and Sarcopenia-the incidence of Osteosarcopenia: a narrative review. Nutrients. 2021;13(12).
Xiang S, Li Y, Li Y, Zhang J, Pan W, Lu Y, et al. Increased Dietary Niacin Intake improves muscle strength, Quality, and glucose homeostasis in adults over 40 years of age. J Nutr Health Aging. 2023;27(9):709–18.
Qiao YS, Chai YH, Gong HJ, Zhuldyz Z, Stehouwer CDA, Zhou JB, et al. The Association between Diabetes Mellitus and Risk of Sarcopenia: accumulated evidences from Observational studies. Front Endocrinol. 2021;12:782391.
Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. The journals of gerontology Series A, Biological sciences and medical sciences. 2014;69(5):547 – 58.
Kim D, Wijarnpreecha K, Sandhu KK, Cholankeril G, Ahmed A. Sarcopenia in nonalcoholic fatty liver disease and all-cause and cause-specific mortality in the United States. Liver International: Official J Int Association Study Liver. 2021;41(8):1832–40.
Jyväkorpi SK, Urtamo A, Kivimäki M, Strandberg TE. Macronutrient composition and sarcopenia in the oldest-old men: the Helsinki businessmen Study (HBS). Clinical nutrition (Edinburgh. Scotland). 2020;39(12):3839–41.
Bossi P, Delrio P, Mascheroni A, Zanetti M. The Spectrum of Malnutrition/Cachexia/Sarcopenia in Oncology according to different Cancer types and settings: a narrative review. Nutrients. 2021;13(6).
Dhillon RJ, Hasni S. Pathogenesis and management of Sarcopenia. Clin Geriatr Med. 2017;33(1):17–26.
Lipina C, Hundal HS. Lipid modulation of skeletal muscle mass and function. J cachexia Sarcopenia Muscle. 2017;8(2):190–201.
Sousa-Victor P, García-Prat L, Muñoz-Cánoves P. Control of satellite cell function in muscle regeneration and its disruption in ageing. Nat Rev Mol Cell Biol. 2022;23(3):204–26.
Li AA, Kim D, Ahmed A. Association of Sarcopenia and NAFLD: an overview. Clin Liver Disease. 2020;16(2):73–6.
Zhai Y, Xiao Q. The common mechanisms of Sarcopenia and NAFLD. Biomed Res Int. 2017;2017:6297651.
Jiang Y, Xu B, Zhang K, Zhu W, Lian X, Xu Y, et al. The association of lipid metabolism and sarcopenia among older patients: a cross-sectional study. Sci Rep. 2023;13(1):17538.
Kang S, Moon MK, Kim W, Koo BK. Association between muscle strength and advanced fibrosis in non-alcoholic fatty liver disease: a Korean nationwide survey. J cachexia Sarcopenia Muscle. 2020;11(5):1232–41.
Yang S, Zhong J, Ye M, Miao L, Lu G, Xu C, et al. Association between the non-HDL-cholesterol to HDL-cholesterol ratio and non-alcoholic fatty liver disease in Chinese children and adolescents: a large single-center cross-sectional study. Lipids Health Dis. 2020;19(1):242.
Kirk B, Cawthon PM, Cruz-Jentoft AJ. Global consensus for Sarcopenia. Aging. 2024;16(11):9306–8.
Kirk B, Mooney K, Vogrin S, Jackson M, Duque G, Khaiyat O, et al. Leucine-enriched whey protein supplementation, resistance-based exercise, and cardiometabolic health in older adults: a randomized controlled trial. J cachexia Sarcopenia Muscle. 2021;12(6):2022–33.
Hirschfeld HP, Kinsella R, Duque G. Osteosarcopenia: where bone, muscle, and fat collide. Osteoporosis international: a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2017;28(10):2781–90.
Al Saedi A, Debruin DA, Hayes A, Hamrick M. Lipid metabolism in Sarcopenia. Bone. 2022;164:116539.
Kadoguchi T, Shimada K, Miyazaki T, Kitamura K, Kunimoto M, Aikawa T, et al. Promotion of oxidative stress is associated with mitochondrial dysfunction and muscle atrophy in aging mice. Geriatr Gerontol Int. 2020;20(1):78–84.
Iannuzzi A, Giallauria F, Gentile M, Rubba P, Covetti G, Bresciani A et al. Association between Non-HDL-C/HDL-C ratio and carotid intima-media thickness in Post-menopausal Women. J Clin Med. 2021;11(1).
Du Y, Oh C, No J. Associations between Sarcopenia and metabolic risk factors: a systematic review and Meta-analysis. J Obes Metabolic Syndrome. 2018;27(3):175–85.
Bi B, Dong X, Yan M, Zhao Z, Liu R, Li S, et al. Dyslipidemia is associated with sarcopenia of the elderly: a meta-analysis. BMC Geriatr. 2024;24(1):181.
Lin Y, Zhong S, Sun Z. Association between serum triglyceride to high-density lipoprotein cholesterol ratio and sarcopenia among elderly patients with diabetes: a secondary data analysis of the China Health and Retirement Longitudinal Study. BMJ open. 2023;13(8):e075311.
Wang N, Chen M, Fang D. Relationship between serum triglyceride to high-density lipoprotein cholesterol ratio and sarcopenia occurrence rate in community-dwelling Chinese adults. Lipids Health Dis. 2020;19(1):248.
Chung TH, Kwon YJ, Shim JY, Lee YJ. Association between serum triglyceride to high-density lipoprotein cholesterol ratio and sarcopenia in elderly Korean males: The Korean National Health and Nutrition Examination Survey. Clinica chimica acta; international journal of clinical chemistry. 2016;463:165-8.
Huang Y, Liao J, Liu Y. Triglyceride to high-density lipoprotein cholesterol ratio was negatively associated with relative grip strength in older adults: a cross-sectional study of the NHANES database. Front Public Health. 2023;11:1222636.
Gong H, Liu Y, Lyu X, Dong L, Zhang X. Lipoprotein subfractions in patients with Sarcopenia and their relevance to skeletal muscle mass and function. Exp Gerontol. 2022;159:111668.
Ghzaiel I, Zarrouk A, Pires V, de Barros JP, Hammami S, Ksila M, et al. 7β-Hydroxycholesterol and 7-ketocholesterol: New oxidative stress biomarkers of Sarcopenia inducing cytotoxic effects on myoblasts and myotubes. J Steroid Biochem Mol Biol. 2023;232:106345.
Zhao W, Gong W, Wu N, Li Y, Ye K, Lu B, et al. Association of lipid profiles and the ratios with arterial stiffness in middle-aged and elderly Chinese. Lipids Health Dis. 2014;13:37.
Lin D, Qi Y, Huang C, Wu M, Wang C, Li F, et al. Associations of lipid parameters with insulin resistance and diabetes: a population-based study. Clin Nutr. 2018;37(4):1423–9.
Kwok RM, Torres DM, Harrison SA. Vitamin D and nonalcoholic fatty liver disease (NAFLD): is it more than just an association? Hepatology (Baltimore. Md). 2013;58(3):1166–74.
Kim SW, Jee JH, Kim HJ, Jin SM, Suh S, Bae JC, et al. Non-HDL-cholesterol/HDL-cholesterol is a better predictor of metabolic syndrome and insulin resistance than apolipoprotein B/apolipoprotein A1. Int J Cardiol. 2013;168(3):2678–83.
Hong H, He Y, Gong Z, Feng J, Qu Y. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and kidney stones: a cross-sectional study. Lipids Health Dis. 2024;23(1):102.
Acknowledgements
We express our gratitude to the personnel at the National Center for Health Statistics of the Centers for Disease Control for their efforts in designing, collecting, and compiling the NHANES data, as well as for establishing the public database.
Funding
This research was supported by the Key Research Projects of the Department of Science and Technology of Sichuan Province, China, under Grant NO.2022YFS0164,2023YFS0176.
Author information
Authors and Affiliations
Contributions
J.-Q.H. and F.-J.H. collected the data. J.-W.Z and Y.-J.Z. analyzed and interpreted. J.-Q.H and S.-Y.H. wrote the main manuscript text. J.-Q.H., Z.-X.Z, and R.W. designed the study. M.-J.W. and W.Z. critically reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Institutional review board statement
The study adhered to the principles outlined in the Declaration of Helsinki and received approval from the Institutional Review Board of the National Centre for Health Statistics.
Informed consent
All participants provided informed consent before enrollment.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hao, Jq., Zhuang, Zx., Hu, Sy. et al. The association between non‑high‑density lipoprotein cholesterol to high‑density lipoprotein cholesterol ratio (NHHR) and low muscle mass in adults aged 20–59: a population-based study in the United States. Lipids Health Dis 23, 274 (2024). https://doi.org/10.1186/s12944-024-02243-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02243-5