
Abstract
Background
This study aimed to explore the associations between triglyceride glucose (TyG) index-related obesity indices and periodontitis within the American population.
Methods
This cross-sectional investigation utilized data from the National Health and Nutrition Examination Survey (NHANES) for 2009–2014. The association between the TyG–waist-to-height ratio (TyG-WHtR), TyG–weight-adjusted-waist index (TyG-WWI), TyG–waist circumference (TyG-WC), or TyG–body mass index (TyG-BMI) and periodontitis was investigated utilizing multivariable logistic regression model, subgroup, and dose-response curve analyses.
Results
This study enrolled 4,808 adult participants. Except for TyG-BMI, which did not exhibit a relationship with periodontitis, TyG-WHtR, [odds ratio (OR) (95% confidence interval (CI))] = 2.83 [1.58–5.10], P = 0.002], TyG-WWI [OR (95% CI) = 7.50 (3.06–18.34), P < 0.001], and TyG-WC [OR (95% CI) = 2.12 (1.23–3.64), P = 0.011] were all associated with periodontitis. Participants in the highest quartile displayed an elevated risk of periodontitis relative to their counterparts in the lowest quartile, as evidenced for TyG-WWI [OR (95% CI) = 1.72 (1.26–2.33), P = 0.001] and TyG-WC [OR (95% CI) = 1.50 (1.13–1.99), P = 0.009] in the full adjustment model. Subgroup analyses suggested more pronounced positive associations between these indices and periodontitis in participants who were < 60 years old, had a BMI ≥ 25, and did not have diabetes. The dose-response curve indicated linear responses in these associations.
Conclusions
This investigation identified a significant and stable association between TyG-WHtR, TyG-WWI, or TyG-WC and periodontitis, which implies a robust correlation between high insulin resistance and susceptibility to periodontitis in the American population.
Similar content being viewed by others
Background
Periodontitis, a chronic inflammatory condition characterised by the progressive destruction of periodontal support tissues, exhibits a prevalence of up to 42% in adults in the United States and 11.2% globally for severe cases [1], making it the sixth most widespread human disease [2]. Periodontitis has been one of the primary contributors to tooth loss in adults [3], which not only impacts nutrition and quality of life but also aggravates global disease burden [4].
Remarkably, the systemic impact of periodontitis is of greater concern than its localized effects on oral health. For instance, periodontitis is related to an increased risk of metabolic syndrome, diabetes, and other chronic diseases [5,6,7]. Insulin resistance (IR) may assume a dominant part in this relationship. Thouvenot et al. [8] revealed that obesity promotes inflammatory factor secretion and inhibits insulin sensitivity, further exacerbating periodontal dysbiosis. Therefore, an extensive understanding of the link between obesity-related IR and periodontitis is essential in disease management.
Given the complexity of traditional IR index measurements, simpler assessment tools have been developed, such as the triglyceride glucose (TyG) index, which estimates insulin sensitivity from triglyceride (TG) and fasting glucose levels, and shows considerable clinical potential [9, 10]. Meanwhile, based on TyG, several new indices have been proposed combining obesity-related anthropological parameters to more accurately assess the severity of IR. For instance, the body mass index (BMI) is a widely accepted and standard tool for evaluating overall obesity and general health, and waist-to-height ratio (WHtR) is commonly utilized as an index for assessing abdominal obesity and its associated metabolic risks, as is the waist circumference (WC) [11, 12]. Furthermore, the weight-adjusted-waist index (WWI), a novel anthropometric measurement, has been suggested to be a superior index of central obesity compared to traditional BMI [13]. Given the significant correlation between an elevated TyG index and heightened risk of periodontitis, it was hypothesised that a novel composite index, incorporating TyG and obesity indices, may serve as a promising index for estimating periodontitis risk in individuals with IR. Notably, the composite metrics TyG-WHtR, TyG-WC, and TyG-BMI have shown a strong correlation with metabolic syndrome, diabetes, and other diseases and more accurately reflected diseases risk compared to TyG alone [14,15,16]. Furthermore, integrating TyG with obesity indices provides a more comprehensive assessment of the influence of IR severity resulting from diverse fat distributions on periodontitis. Nevertheless, no studies have assessed the correlations between these indices and periodontitis in the American population, which underscores the essential need for further confirmation of their correlations.
Therefore, by surveying the National Health and Nutrition Examination Survey (NHANES) database, the study analysed different TyG-related indices to explore the association between obesity-related IR and periodontitis risk.
Methods
Study design and participant selection
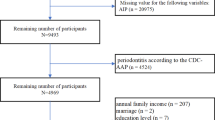
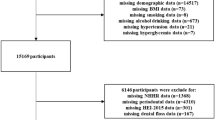
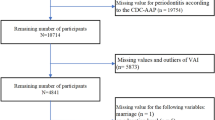
This study extracted data of 30,468 individuals from the NHANES database for the period 2009–2014. The NHANES utilizes a multistage stratified probability sampling strategy to collect extensive data on the health, lifestyle, and nutrition of the US citizens [17]. The full dataset comprised three pooled NHANES cycles for 2009–2010, 2011–2012, and 2013–2014, and strictly adhered to the following exclusion criteria: (1) participants aged < 30 years; (2) individuals with missing data on periodontitis; (3) edentulous adults; (4) incomplete data on TyG index (5) incomplete data on body measurement parameters; and (6) pregnant women. Ultimately, the study enrolled a total of 4,808 participants. The general data selection process is outlined in Fig. 1.

Flowchart of participants in this study
Definitions and calculations of TyG-related obesity indices
The exposure variables TyG-WHtR, TyG-WWI, TyG-WC, and TyG-BMI were derived from the analysis of fasting glucose, TG, and certain body parameters. Baseline blood samples were gathered to measure fasting glucose and TG levels while anthropometric measurements were obtained by healthcare professionals with specialized training. The TyG index was calculated as TyG = ln [(TG levels × fasting glucose levels) / 2]. This index was then used to calculate the combined indices as previously described [18]: (1) WHtR = WC / Height; (2) \(WWI=\frac{WC}{\sqrt{Weight}}\) ; (3) TyG-WHtR = TyG × WHtR; (4) TyG-WWI = TyG × WWI; (5) TyG-WC = TyG × WC; (6) TyG-BMI = TyG × BMI.
Clinical periodontal assessment and definition
A comprehensive dental examination (excluding the third molars) was conducted by trained professionals. Measurements were performed at six sites for each tooth. The diagnostic assessment of the periodontal condition strictly adhered to the Centers for Disease Control and Prevention and American Academy of Periodontics definitions for the clinical attachment loss and probing pocket depth values at the four interproximal sites of each tooth [19]. Following a series of assessments, individuals diagnosed with mild, moderate, or severe periodontitis were assigned to the periodontitis group, whereas those without periodontitis were assigned to the non-periodontitis group.
Assessment of covariates
A number of factors were incorporated as covariates, including gender, race, age, physical activity, educational level, BMI, alcohol consumption, smoking, income-to-poverty ratio (PIR), diabetes mellitus, hypertension, dental flossing frequency and dentition status. Gender was specifically classified as male or female. Age was divided into two groups with a threshold of 60. The PIR was grouped into two levels: “<1” and “≥1”. A BMI “<25” was considered within the normal weight range, while a BMI “≥25” was defined as overweight/obese. Alcohol consumption and smoking status were categorized as yes/no. Diabetes diagnosis was based on HbA1c levels of ≥ 6.5%, ≥ 126 mg/dL for fasting glucose level, ≥ 200 mg/dL for plasma glucose concentrations after an oral glucose tolerance test, physician confirmation, or self-reported use of insulin or diabetes drugs. Confirmation of a hypertension diagnosis occurred when any of the following criteria were satisfied: systolic blood pressure ≥ 40 mmHg (average of three consecutive readings), diastolic blood pressure ≥ 90 mmHg (average of three consecutive measurements), or individuals reporting a history of hypertension or utilizing antihypertensive medications. If dental floss was not used on any day during a week, the frequency of dental floss usage was marked as ‘No’ [20]. The assessment of dentition status depended on the presence of functional teeth: having 20 or more natural permanent teeth was considered functional dentition, whereas 19 or fewer indicated non-functional dentition [21].
Statistical analyses
Considering the sophisticated multistage probability sampling design adopted in the NHANES, attention was given to the potential effects of sample weights, stratification, and clustering in the dataset. Consequently, the study grouped the TyG-WHtR, TyG-WWI, TyG-WC, and TyG-BMI estimates into quartiles and applied a weighted multivariable logistic regression model to analyse the associations of the TyG-related obesity indices with periodontitis. To ensure a comprehensive analysis, three adjustment models were formulated. Model 1 remained unadjusted; model 2 was subjected to adjustments for the demographic variables of age, gender, and race; and model 3 was adjusted for all potential confounders: age, gender, race, education level, PIR, BMI, physical activity, alcohol, smoking, hypertension, diabetes, dental floss and dentition status.
Given the right-skewed distribution of the data, a natural logarithm (ln) transformation was employed for continuous variables. Additionally, subgroup analyses based on the full adjustment model was applied to observe the associations between the TyG-related obesity indices and periodontitis in distinct subgroups of BMI, age, gender hypertension, and diabetes. The interaction test results were further analysed to identify the heterogeneity in the relationships within each subgroup. Finally, dose-response curves were used to identify possible connections between TyG-related obesity indices and periodontitis in the three models. The execution of statistical analyses involved R Studio (version 4.3.1) and Empower Stats (version 4.1), and statistical significance was set at P < 0.05.
Results
Baseline features of the study cohort
The essential traits of the participant characteristics are outlined in Table 1. The 4,808 individuals in the cohort showed an overall periodontitis prevalence of 50.12%. Participants aged < 60 years accounted for 73.3%, while those aged ≥ 60 years accounted for 26.7%. The cohort comprised 49.6% males and 50.4% females in gender distribution. As for race, the cohort included 8.1% Mexican Americans, 69.5% non-Hispanic whites, 9.7% non-Hispanic blacks, 5.6% with other Hispanic backgrounds, and 7.0% of other ethnicities.
In contrast to the non-periodontitis group, the periodontitis group exhibited several distinguishing features: They were notably older, had a larger WC, higher smoking rates, a greater proportion of males, increased prevalence of diabetes and hypertension, and elevated levels of TG, fasting glucose, fasting insulin, and all TyG-related indices. This group also showed lower educational levels, lower PIR, less frequent dental floss usage and a smaller number of permanent teeth.
For a comprehensive understanding of the distributional differences in each parameter, the participants were categorised into quartiles according to TyG-WHtR, TyG-WWI, TyG-WC, and TyG-BMI. Participants in the top quartile for TyG-WHtR, TyG-WWI, and TyG-WC exhibited an increased prevalence in periodontitis in comparison to the bottom quartile, and were more prone to possess lower educational and income levels, less frequent dental floss usage, a smaller number of permanent teeth, higher obesity levels or more recurrent overweight status, more frequent smoking assignments, and a greater prevalence of diabetes and hypertension (Table 2 and Supplementary Tables 1, 2, and 3).
Associations between TyG-related obesity indices and periodontitis
Multivariable logistic regression models were employed to examine the links of TyG-WHtR, TyG-WWI, TyG-WC, and TyG-BMI with periodontitis (Supplementary Table 4). TyG-WHtR [odds ratios (OR) (95% confidence intervals (CI)) = 2.83 (1.58–5.10), P = 0.002], TyG-WWI [OR (95% CI) = 7.50 (3.06–18.34), P < 0.001], and TyG-WC [OR (95% CI) = 2.12 (1.23–3.64), P = 0.011] presented a strong positive correlation with periodontitis in the full adjustment model. Stronger positive correlations were observed in the highest quartile than those in the lowest quartile (Table 3). Specifically, TyG-WWI [OR (95% CI) = 1.72 (1.26–2.33), P = 0.001] and TyG-WC [OR (95% CI) = 1.50 (1.13–1.99), P = 0.009] exhibited a more pronounced positive correlation in model 3, indicating that the higher indices may be associated with an increased risk of periodontitis. Nevertheless, TyG-BMI did not present a discernible trend in association with the periodontitis in the preceding analysis.
Supplementary Table 4 offers further insights by comparing the connections of both TyG-related obesity indices and traditional IR index such as homeostatic model assessment of insulin resistance (HOMA-IR) with periodontitis. The combined indices TyG-WHtR, TyG-WWI, and TyG-WC showed stronger associations with periodontitis, emphasising the potential significance of the complex correlation between IR, obesity, and periodontitis.
Subgroup analyses
The study conducted an in-depth examination of the intricate relationships between the TyG-related obesity indices and periodontitis through subgroup analyses accounting for BMI, gender, age, diabetes, and hypertension (Table 4). Interestingly, a significant correlation between TyG-WHtR, TyG-WWI, or TyG-WC and periodontitis was observed for participants of < 60 years old, with BMI ≥ 25, and without diabetes. However, no significant interactions were observed between the TyG-related obesity indices and periodontitis (P > 0.05 for all interactions).
Dose-response relationships based on restricted cubic spline (RCS)
This study utilized RCS curves to flexibly model the variations in the data and explore the linearity of the correlations between TyG-WHtR, TyG-WWI, TyG-WC, or TyG-BMI and periodontitis. Figure 2 presents positive linear correlations (P-nonlinear > 0.05) between TyG-WHtR, TyG-WWI, and TyG-WC and periodontitis in the three adjustment models.

Restricted cubic spline (RCS) fitting for the associations of TyG-related obesity indices with periodontitis in different models. (A) RCS fitting for TyG-WHtR and periodontitis; (B) RCS fitting for TyG-WWI and periodontitis; (C) RCS fitting for TyG-WC and periodontitis; (D) RCS fitting for TyG-BMI and periodontitis
Discussion
Throughout this national observational study, the correlation between IR, assessed by TyG-related obesity indices, and periodontitis was investigated utilizing the NHANES database for 2009–2014. The predominant discoveries revealed that TyG-WHtR, TyG-WWI, and TyG-WC, but not TyG-BMI, were positively correlated with the occurrence of periodontitis in the full adjustment model. Furthermore, participants in the top quartile had a higher risk of periodontitis relative to those in the bottom quartile, with a risk of 72% associated with TyG-WWI and 50% with TyG-WC. Subgroup analyses showed that strong relationships between TyG-WHtR, TyG-WWI, and TyG-WC and periodontitis were more likely to be observed among participants who were < 60 years of age, had a BMI ≥ 25, and no diabetes. These results indicated that recognizing the potential of TyG combined with obesity indices in epidemiological studies of periodontitis is essential for exploring the relationship between IR and this disease.
Previous studies have indicated that IR-associated metabolic syndrome is not only critical in the development and progression of diabetes but also increases the risk of developing periodontitis [22, 23]. The HOMA-IR, which is based on fasting glucose and insulin levels, is a classical IR index [24]. However, given the cost of insulin detection and the limitations of HOMA-IR in populations receiving insulin therapy, a more representative, efficient, and convenient index is still required. The TyG index has emerged as a comprehensive alternative in the estimation of IR due to its simplicity of calculation, sensitivity, and specificity [25]. Prior researches have shown that it provides comparable or better performance than HOMA-IR in evaluating IR [26,27,28]. Importantly, individuals with an increased level of IR usually present with obesity, making it a noteworthy driver of periodontitis occurrence [29]. The validity of the traditional anthropometric parameters, including WHtR, WC, and BMI, as well as the latest proposed WWI in predicting obesity has been confirmed [13]. Recently, the applicability of the TyG-related obesity indices has been widely investigated in chronic conditions such as cardiovascular disease [30, 31]. A national cohort study reported that integrating obesity metrics with TyG could better predictive metabolic syndrome risk than using these indices alone [32]. Furthermore, in the general population, TyG-WHtR, TyG-WC, and TyG-BMI were usually more robust in predicting IR compared to TyG alone [33]. Thus, combining obesity indices with TyG may more accurately reflect the correlation between IR and periodontitis.
Several studies have been conducted to support our discovery. According to Lee et al. [34], a significant association between the TyG index and periodontitis among Korean adults. Benguigui et al. [35] displayed a positive relationship between HOMA-IR and periodontitis, which was compatible with our findings. In addition, analysis of a cross-sectional study including 13,684 Koreans revealed a statistically significant elevation in the risk of periodontitis among those in the highest quartile for TyG-WHtR, TyG-WC, and TyG-BMI compared with those in the lowest quartile [36]. Notably, there was no correlation between TyG-BMI and periodontitis in the full adjustment model in this study, the reason is likely to be that the accuracy of using BMI to reflect obesity varies by disease and region [37, 38]. Hence, the superiority of TyG-related obesity metrics over single metrics remains controversial, and additional research is necessary to elucidate the different features of the parameters.
Although the precise pathophysiological relevance of the correlations between TyG-related obesity indices and periodontitis remains unclear, several factors may account for this relationship. The crosstalk between IR and oxidative stress as well as inflammation alters the host immune response. Mass inflammatory cytokine and mediator production causes abnormal insulin receptor signalling that ultimately impairs downstream metabolism [8]. Notably, these inflammatory mechanisms are closely correlated with periodontal bacterial lipopolysaccharide production in oral flora dysbiosis [39]. A recent investigation by Zeze et al. [40] showed that IR decreased the expression of vascular cell adhesion molecules, which exacerbated the inflammatory response in periodontal tissues by interfering insulin-mediated Forkhead Box O1 activity. Additionally, elevated levels of oxidative stress directly contribute to periodontal tissue destruction by inducing lipid metabolism abnormalities and others, protein structural alterations, and cell membrane disruption [41]. Furthermore, chronic inflammation induced by obesity not only affects insulin sensitivity but also promotes oral immune microenvironment disorders, ultimately exacerbating the severity of periodontitis [23, 42]. As a measure of obesity, BMI is commonly taken to describe overall obesity, while WC and WHtR are recognized as metrics of central obesity. Simultaneously, WWI is a new anthropometric parameter designed to represent central obesity regardless of body weight [43]. The location of fat distribution is known to has stronger implications for obesity-related risk than the amount of fat. For example, abdominal obesity is more closely associated with IR and metabolic dysfunction than peripheral obesity because it affects insulin metabolism by altering the release of fatty acids [44].
Study strengths and limitations
There are several advantages to this study. Notably, it provided valuable evidence highlighting the positive relationships between TyG-related obesity indices and periodontitis. As the data originated from the NHANES database, the dataset was characterised by a substantial sample size and national representativeness. Furthermore, these analyses accounted for confounding variables associated with periodontitis, thus reinforcing the reliability of findings. However, certain limitations warrant consideration. First, the observational study design limited the ability to explore the causative correlations between TyG-related obesity indices and periodontitis. Second, despite efforts to adjust for various confounding factors, fully eliminating the potential impact of other confounding variables remains to be a challenge. Finally, this research focused on the US population, which may restrict the broader applicability of the findings to the global population. Future studies should consider larger and more diverse cohorts to determine the most effective TyG-related obesity indices for predicting periodontitis and to establish universally applicable threshold values.
Conclusions
The study observed a strong association between TyG-WHtR, TyG-WWI, or TyG-WC and periodontitis in the American population. This underscores the potential of TyG-related obesity indices for identifying periodontitis risk, and emphasises the importance of fat distribution and insulin resistance in the pathogenesis of periodontitis. This study offers valuable perspectives for risk stratification, early intervention strategies, and cost-effective screening methods in high-risk populations.
Data availability
The NHANES data that support the findings of this study are openly available at https://www.cdc.gov/nchs/nhanes/index.htm.
Abbreviations
- NHANES:
-
National Health and Nutrition Examination Survey
- TyG:
-
Triglyceride glucose
- WHtR:
-
Waist-to-height ratio
- WWI:
-
Weight-adjusted-waist index
- BMI:
-
Body mass index
- WC:
-
Waist circumference
- RCS:
-
Restricted cubic spline
- IR:
-
Insulin resistance
- TG:
-
Triglyceride
- PIR:
-
Income-to-poverty ratio
References
Eke PI, Thornton-Evans GO, Wei L, Borgnakke WS, Dye BA, Genco RJ. Periodontitis in US adults: National Health and Nutrition Examination Survey 2009–2014. J Am Dent Assoc. 2018;149:576–e5886.
Hasan A, Palmer RM. A clinical guide to periodontology: Pathology of periodontal disease. Br Dent J. 2014;216:457–61.
Takedachi M, Shimabukuro Y, Sawada K, Koshimizu M, Shinada K, Asai H, et al. Evaluation of periodontitis-related tooth loss according to the new 2018 classification of periodontitis. Sci Rep. 2022;12:11893.
Reynolds I, Duane B. Periodontal disease has an impact on patients’ quality of life. Evid Based Dent. 2018;19:14–5.
Pirih FQ, Monajemzadeh S, Singh N, Sinacola RS, Shin JM, Chen T et al. Association between metabolic syndrome and periodontitis: The role of lipids, inflammatory cytokines, altered host response, and the microbiome. Periodontol. 2000. 2021;87:50–75.
D’Aiuto F, Gkranias N, Bhowruth D, Khan T, Orlandi M, Suvan J, et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: a 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. 2018;6:954–65.
Molina A, Huck O, Herrera D, Montero E. The association between respiratory diseases and periodontitis: a systematic review and meta-analysis. J Clin Periodontol. 2023;50:842–87.
Thouvenot K, Turpin T, Taïlé J, Clément K, Meilhac O, Gonthier M-P. Links between Insulin Resistance and Periodontal Bacteria: insights on molecular players and therapeutic potential of polyphenols. Biomolecules. 2022;12:378.
Lee J, Kim B, Kim W, Ahn C, Choi HY, Kim JG, et al. Lipid indices as simple and clinically useful surrogate markers for insulin resistance in the U.S. population. Sci Rep. 2021;11:2366.
Son D-H, Lee HS, Lee Y-J, Lee J-H, Han J-H. Comparison of triglyceride-glucose index and HOMA-IR for predicting prevalence and incidence of metabolic syndrome. Nutr Metab Cardiovasc Dis. 2022;32:596–604.
Moosaie F, Fatemi Abhari SM, Deravi N, Karimi Behnagh A, Esteghamati S, Dehghani Firouzabadi F, et al. Waist-To-Height ratio is a more Accurate Tool for Predicting Hypertension Than Waist-To-Hip circumference and BMI in patients with type 2 diabetes: a prospective study. Front Public Health. 2021;9:726288.
Katzmarzyk PT, Hu G, Cefalu WT, Mire E, Bouchard C. The importance of waist circumference and BMI for mortality risk in diabetic adults. Diabetes Care. 2013;36:3128–30.
Park Y, Kim NH, Kwon TY, Kim SG. A novel adiposity index as an integrated predictor of cardiometabolic disease morbidity and mortality. Sci Rep. 2018;8:16753.
Raimi TH, Dele-Ojo BF, Dada SA, Fadare JO, Ajayi DD, Ajayi EA, et al. Triglyceride-glucose index and related parameters predicted metabolic syndrome in nigerians. Metab Syndr Relat Disord. 2021;19:76–82.
Li X, Sun M, Yang Y, Yao N, Yan S, Wang L, et al. Predictive effect of triglyceride glucose-related parameters, obesity indices, and lipid ratios for diabetes in a Chinese Population: a prospective cohort study. Front Endocrinol (Lausanne). 2022;13:862919.
Yan S, Wang D, Jia Y. Comparison of insulin resistance-associated parameters in US adults: a cross-sectional study. Horm (Athens). 2023;22:331–41.
Ghimire S, Baral BK, Feng D, Sy FS, Rodriguez R. Is selenium intake associated with the presence of depressive symptoms among US adults? Findings from National Health and Nutrition Examination Survey (NHANES) 2011–2014. Nutrition. 2019;62:169–76.
Dang K, Wang X, Hu J, Zhang Y, Cheng L, Qi X, et al. The association between triglyceride-glucose index and its combination with obesity indicators and cardiovascular disease: NHANES 2003–2018. Cardiovasc Diabetol. 2024;23:8.
Eke PI, Page RC, Wei L, Thornton-Evans G, Genco RJ. Update of the case definitions for population-based surveillance of periodontitis. J Periodontol. 2012;83:1449–54.
Hou K, Song W, He J, Ma Z. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and prevalence of periodontitis among US adults: a cross-sectional NHANES study. Sci Rep. 2024;14:5558.
Hussein M, Farag YMK, Sonis S. Differential associations of rheumatoid arthritis and periodontitis or tooth loss: a cross-sectional study. J Clin Periodontol. 2023;50:307–15.
Shinjo T, Nishimura F. The bidirectional association between diabetes and periodontitis, from basic to clinical. Jpn Dent Sci Rev. 2024;60:15–21.
Jepsen S, Suvan J, Deschner J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontol 2000. 2020;83:125–53.
Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Diabetes Care. 2004;27:1487–95.
Tahapary DL, Pratisthita LB, Fitri NA, Marcella C, Wafa S, Kurniawan F, et al. Challenges in the diagnosis of insulin resistance: focusing on the role of HOMA-IR and Tryglyceride/glucose index. Diabetes Metab Syndr. 2022;16:102581.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6:299–304.
Guerrero-Romero F, Villalobos-Molina R, Jiménez-Flores JR, Simental-Mendia LE, Méndez-Cruz R, Murguía-Romero M, et al. Fasting triglycerides and glucose index as a diagnostic test for insulin resistance in young adults. Arch Med Res. 2016;47:382–7.
Wang S, Shi J, Peng Y, Fang Q, Mu Q, Gu W, et al. Stronger association of triglyceride glucose index than the HOMA-IR with arterial stiffness in patients with type 2 diabetes: a real-world single-centre study. Cardiovasc Diabetol. 2021;20:82.
Suren Garg S, Kushwaha K, Dubey R, Gupta J. Association between obesity, inflammation and insulin resistance: insights into signaling pathways and therapeutic interventions. Diabetes Res Clin Pract. 2023;200:110691.
Huang D, Ma R, Zhong X, Jiang Y, Lu J, Li Y, et al. Positive association between different triglyceride glucose index-related indicators and psoriasis: evidence from NHANES. Front Immunol. 2023;14:1325557.
Tan L, Liu Y, Liu J, Zhang G, Liu Z, Shi R. Association between insulin resistance and uncontrolled hypertension and arterial stiffness among US adults: a population-based study. Cardiovasc Diabetol. 2023;22:311.
Gui J, Li Y, Liu H, Guo L, Li J, Lei Y, et al. Obesity- and lipid-related indices as a predictor of obesity metabolic syndrome in a national cohort study. Front Public Health. 2023;11:1073824.
Lim J, Kim J, Koo SH, Kwon GC. Comparison of triglyceride glucose index, and related parameters to predict insulin resistance in Korean adults: an analysis of the 2007–2010 Korean National Health and Nutrition Examination Survey. PLoS ONE. 2019;14:e0212963.
Lee Y-C, Lee J-W, Kwon Y-J. Comparison of the triglyceride glucose (TyG) index, triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) ratio, and metabolic score for insulin resistance (METS-IR) associated with periodontitis in Korean adults. Ther Adv Chronic Dis. 2022;13:20406223221122671.
Benguigui C, Bongard V, Ruidavets J-B, Chamontin B, Sixou M, Ferrières J, et al. Metabolic syndrome, insulin resistance, and periodontitis: a cross-sectional study in a middle-aged French population. J Clin Periodontol. 2010;37:601–8.
Lee H-J, Lee J-W, Kim S, Kwon Y-J. Comparison of the triglyceride glucose index and modified triglyceride glucose indices in assessing periodontitis in Korean adults. J Periodontal Res. 2023;58:503–10.
Elagizi A, Kachur S, Lavie CJ, Carbone S, Pandey A, Ortega FB, et al. An overview and update on obesity and the obesity Paradox in Cardiovascular diseases. Prog Cardiovasc Dis. 2018;61:142–50.
Kleine C-E, Moradi H, Streja E, Kalantar-Zadeh K. Racial and ethnic disparities in the obesity Paradox. Am J Kidney Dis. 2018;72:S26–32.
Le Sage F, Meilhac O, Gonthier M-P. Porphyromonas gingivalis lipopolysaccharide induces pro-inflammatory adipokine secretion and oxidative stress by regulating toll-like receptor-mediated signaling pathways and redox enzymes in adipocytes. Mol Cell Endocrinol. 2017;446:102–10.
Zeze T, Shinjo T, Sato K, Nishimura Y, Imagawa M, Chen S, et al. Endothelial insulin resistance exacerbates experimental Periodontitis. J Dent Res. 2023;102:1152–61.
Buranasin P, Kominato H, Mizutani K, Mikami R, Saito N, Takeda K, et al. Influence of reactive oxygen species on Wound Healing and tissue regeneration in Periodontal and Peri-implant tissues in Diabetic patients. Antioxid (Basel). 2023;12:1787.
Byun J-S, Lee HY, Tian J, Moon JS, Choi J, Lee S-H, et al. Effect of salivary exosomal mir-25-3p on Periodontitis with insulin resistance. Front Immunol. 2021;12:775046.
Hu Q, Han K, Shen J, Sun W, Gao L, Gao Y. Association of weight-adjusted-waist index with non-alcoholic fatty liver disease and liver fibrosis: a cross-sectional study based on NHANES. Eur J Med Res. 2023;28:263.
Björntorp P. Metabolic implications of body fat distribution. Diabetes Care. 1991;14:1132–43.
Acknowledgements
We would like to thank the initiators and participants of the NHANES database.
Funding
This work was supported by the Anhui Province Academic and Technical Leader Reserve Candidate Research Funding (No. 2021H253).
Author information
Authors and Affiliations
Contributions
LY and RX designed the study. LY performed the research procedures, including data collection, data analysis, and data interpretation. LY and SF were involved in the preparation of figures, drafting and revising the manuscript. RX and RZ provided academic guidance. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The NHANES protocol was approved by the NCHS Ethics Review Board, and informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, L., Fang, S., Zhang, R. et al. Associations between different triglyceride glucose index-related obesity indices and periodontitis: results from NHANES 2009–2014. Lipids Health Dis 23, 213 (2024). https://doi.org/10.1186/s12944-024-02192-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02192-z