
Abstract
Background
Although potent lipid-lowering therapies are available, patients commonly fall short of recommended low-density lipoprotein cholesterol (LDL-C) levels. The aim of this study was to examine the relationship between familial hypercholesterolemia (FH) and elevated lipoprotein(a) [Lp(a)] and LDL-C goal attainment, as well as the prevalence and severity of coronary artery disease (CAD). Moreover, we characterized patients failing to meet recommended LDL-C goals.
Methods
We performed a cross-sectional analysis in a cohort of patients undergoing cardiac catheterization. Clinical FH was determined by the Dutch Clinical Lipid Network Score, and Lp(a) ≥ 50 mg/dL (≈ 107 nmol/L) was considered elevated.
Results
A total of 838 participants were included. Overall, the prevalence of CAD was 72%, and 62% received lipid-lowering treatment. The prevalence of clinical FH (probable and definite FH) was 4%, and 19% had elevated Lp(a) levels. With 35%, LDL-C goal attainment was generally poor. Among the participants with clinical FH, none reached their LDL-C target. Among patients with elevated Lp(a), LDL-C target achievement was only 28%. The prevalence and severity of CAD were higher in participants with clinical FH (86% prevalence) and elevated Lp(a) (80% prevalence).
Conclusion
Most participants failed to meet their individual LDL-C goals according to the ESC 2016 and 2019 guidelines. In particular, high-risk patients with clinical FH or elevated Lp(a) rarely met their target for LDL-C. The identification of these patients and more intense treatment approaches are crucial for the improvement of CAD primary and secondary prevention.
Similar content being viewed by others
Introduction
The burden of atherosclerotic cardiovascular disease (ASCVD) is still very high, and cardiovascular disease (CVD) is the leading cause of morbidity and mortality globally [1]. In Europe, more than 4 million deaths are due to CVD each year, accounting for approximately 45% of all deaths, according to the latest epidemiological update on CVD [2]. Coronary artery disease (CAD) alone accounts for 20% of all deaths [2].
Elevated low-density lipoprotein cholesterol (LDL-C) and other cholesterol-rich apolipoprotein B (apo B)-containing lipoproteins are key risk factors for ASCVD, and risk reduction is directly and positively correlated with the achieved absolute LDL-C reduction via lipid-lowering therapies [1, 3].
Steadily growing evidence has confirmed that lipoprotein(a) [Lp(a)] is likewise an independent risk factor for ASCVD. Hence, the updated European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) guideline for the management of dyslipidemias has included Lp(a) as a secondary treatment target in patients with otherwise optimally controlled risk factors [3, 4].
Lp(a) is a plasma lipoprotein that structurally resembles LDL-C but differs from LDL-C by containing an additional protein, apolipoprotein a [apo(a)]. Plasma levels of Lp(a) are mainly genetically determined by variations in the APOA gene and are only marginally influenced by diet, physical activity or other lifestyle habits, in contrast to other cholesterol-containing lipoproteins[4, 5]. Certain clinical conditions, such as familial hypercholesterolemia (FH) and chronic kidney disease, are associated with increased Lp(a) levels [6,7,8]. There is robust evidence showing that patients with higher plasma levels of Lp(a) are at greater risk of CAD and stroke [4, 7]. Currently, there are no approved pharmacologic therapies available that specifically target Lp(a) [9, 10].
Similar to elevated Lp(a), FH is independently associated with an increased risk of CVD. FH is caused by a monogenetic mutation and is characterized by defective clearance of LDL-C and premature coronary artery disease (CAD) [6]. FH can be diagnosed either by genetic testing for a causative mutation leading to elevated LDL-C levels or by using clinical criteria [6]. The Dutch Lipid Clinic Network (DLCN) created a scoring system based on clinical criteria assessing the probability of FH, ranging from unlikely, probable, possible to a definite diagnose of FH.
Although CAD mortality has declined and the management of dyslipidemia with lipid-lowering therapies (LLT) has improved over the last decades, mainly due to potent statin therapy [11], the guideline-recommended LDL-C reduction goals are vastly failed by most patients. Lipid goal attainment has been shown to be poor worldwide, including in Germany, ranging between 17 and 62% [12,13,14]. In particular, patients at high and very high cardiovascular risk regularly fail to reach the recommended lipid goals [14]. Unfortunately, those patients failing to meet their recommended goals remain at high risk of cardiovascular morbidity and mortality. Correct CVD risk evaluation is crucial for setting suitable lipid thresholds and preventing CVD and CVD progression. There are various scoring systems (the ESC-SCORE, the pooled cohort equations (PCE), or the PROCAM score, to name just a few) that include major CVD risk factors [3, 15, 16].
There is evidence that patients with genetic dyslipidemias such as FH are at greater risk of CVD and (recurrent) major adverse cardiovascular events (MACEs) than patients without a demonstrable genetic cause of dyslipidemia [18]. Arguably, at least 5% of all premature myocardial infarctions occur in FH individuals [19]. This can plausibly be explained by the long-standing exposure to elevated LDL-C and/or other cholesterol-rich apolipoprotein B (apoB)-containing lipoproteins since early childhood [18].
Reasons for the common failure in lipid goal attainment are not yet well described. A common argument is the lack of medication adherence due to side effects, especially to statins [13, 14, 17]. There is some evidence that high Lp(a) levels and FH impede the achievement of LDL-C goals [20, 21], but since Lp(a) status is often unknown, the association between Lp(a) and LDL-C goal attainment deserves further clarification.
The aim of this analysis was 1) to examine the current treatment situation of CAD patients with regard to LDL-C reduction in a large German tertiary care facility; 2) to determine the proportion of patients with diagnosed CAD failing to meet guideline recommended LDL-C targets; 3) to assess the association between dyslipidemias of (assumable) predominant genetic etiology (clinical FH and elevated Lp(a)) and LDL-C goal attainment; 4) to assess the predictive diagnostic value of family history regarding lipid disorders and CAD; and 5) to characterize patients with poor LDL-C control in a secondary prevention setting, to inform future studies/interventions aimed at improving lipid-lowering therapy and CAD prevention.
Methods
Study population and design
We performed a cross-sectional analysis of data from the LipidCardio study. The LipidCardio study is a prospective observational study examining patients who underwent elective coronary angiography for diagnostic or therapeutic reasons in the Department of Cardiology at Charité-Universitätsmedizin Berlin from October 2016 to March 2018. Patients who received catheterization for acute coronary syndromes were excluded. Demographic information, medical history, cardiovascular risk factors, extensive family history of first-degree relatives, medication plans before intervention, nonfasting lipid profiles, containing LDL-C (measured directly using an enzymatic colorimetric assay) high-density lipoprotein cholesterol (HDL-C), Lp(a) (using a turbidimetric assay by Roche Diagnostics), apo B, and HbA1c, medical examination results, including measurements of blood pressure (mmHg), pulse wave velocity (m/s), height (cm), weight (kg), and derived body-mass index (BMI, kg/m2), questionnaires on lifestyle habits (sports, smoking, alcohol) and coronary angiography results were collected. The rationale, design and methods of the LipidCardio study have been described in detail by König et al. [22]. Written informed consent was provided by all study participants, and the study was approved by the ethics committee at Charité-Universitätsmedizin Berlin (approval number: EA1/135/16).
In the present analysis, only participants for whom complete data containing family history, lipid profile, including LDL-C and Lp(a), medication, and diagnoses were available (Fig. 1) were included.

Flow chart of sample selection
Statin treatment intensity, projection of statin-naive LDL-C, and LDL-C target achievement
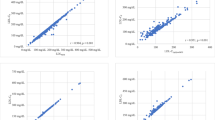
We inferred statin-naive LDL-C levels using published conversion factors (Supplementary table 1) [23,24,25,26,27,28]. Statin therapy was classified into low-intensity, moderate-intensity, and high-intensity groups based on expected LDL-C reductions of 20–32%, 36–50%, and 52–70%, respectively, depending on the statin type and dosage [23]. For 10-year cardiovascular risk estimation, we used the modified PROCAM score [29], and LDL-C target achievement was assessed based on the ESC/EAS guidelines for the management of dyslipidemias both from 2016, which were applicable at the study point, and from 2019 (currently valid). For very high-risk individuals, e.g., participants with CAD, the corresponding LDL-C target level was set at < 70 mg/dL; for high-risk individuals, the LDL-C target level was < 100 mg/dL; and for participants with intermediate or low risk, the LDL-C target level was < 115 mg/dL [30] according to the 2016 recommendations and < 55 mg/dL, < 70 mg/dL, and < 100 mg/dL with the recent recommendations [3].
Definitions of dyslipidemia and CAD
Phenotypical familial hypercholesterolemia (FH) was ascertained according to the DLCN criteria. These were modified as described in the study of Langsted et al. because there was no information available on LDL-C levels in the offspring of participants, nor was there structured information on tendon xanthoma or corneal arcus in our participants and their relatives [31]. The probability of the FH diagnosis was operationalized into unlikely, possible, probable, or definite FH according to the modified DLCN criteria [31]. For the purpose of this analysis, participants with probable or definite FH according to the modified DLCN criteria were grouped together.
If Lp(a) levels were above 50 mg/dL (≈ 107 nmol/L), which equates to the fifth quintile in the examined study population, participants were considered to have “elevated” Lp(a) levels [4, 22].
CAD status was assessed by coronary angiography. Obstructive CAD was defined as a more than 50% obstruction in one of the major coronary arteries (left main coronary artery, left anterior descending artery [LAD], circumflex artery [RCX] and right coronary artery [RCA]). Obstructive CAD was categorized as 1-vessel, 2-vessel, or 3-vessel disease based on the number of coronary arteries with significant stenoses. Obstructions of the left main coronary artery were considered 2-vessel disease (LAD and RCX). Patients with coronary lesions or stenoses with less than 50% lumen obstruction were considered to have nonobstructive CAD, and “no CAD” was defined by normal coronary angiographic results.
Statistical analyses
Participants with either probable or definite phenotypical FH and/or elevated Lp(a) were grouped together in some analyses. Proportions of LDL-C goal attainment were compared across phenotypical FH groups, between participants with and without elevated Lp(a) levels, and participants with and without genetic dyslipoproteinemia (probable and definite FH and/or elevated Lp(a)).
Statistical analyses were performed using the software package IBM SPSS 25.0, and figures were created using MS Excel 2013. Data are given in numbers (percentages), means and standard deviations (SDs), or medians and interquartile ranges (IQRs). We compared LDL-C goal attainment and the prevalence and severity of CAD between groups using the χ2-test for binary categorical variables, Kruskal‒Wallis test for categorical variables and the Jonckheere-Terpstra test for ordinal variables. Continuous variables were compared using t tests or analysis of variance (ANOVA) for more than two groups. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated using multivariable logistic regression. Kendall tau correlation was used to estimate associations between two ordinal variables. The statistical level of significance was set at P value < 0.05.
Results
Sample characteristics
Overall, 1005 participants were enrolled in the LipidCardio study between October 2016 and April 2018. Due to logistical reasons, complete family history, LDL-C, and Lp(a) levels were available from only 838 participants (Fig. 1.).
A total of 70.4% of participants were men (n = 590), and the mean (± SD) age was 69.4 (± 11.0) years. The majority (98.1%, n = 822) were of European ethnic origin. Overall, 71.5% (n = 599) had angiography-confirmed CAD. A total of 80.9% (n = 678) had a history of hypertension or were taking antihypertensive medication, 27.6% (n = 231) had been diagnosed with type 2 diabetes (T2D), 18.7% (n = 156) were current smokers, 61.6% (n = 516) were on lipid-lowering medication, and 25.9% (n = 216) were obese (BMI ≥ 30 kg/m2). The mean BMI was 27.9 (± 4.9) kg/m2 (Table 1).
Family history of CVD
A total of 30.4% of participants (n = 255) had a positive family history of premature CAD, i.e., a history of myocardial infarction, CAD, or cardiac death in first-degree relatives below the age of 55 years in men and 65 years in women. A total of 6.8% (n = 57) had a positive family history of stroke in first-degree relatives below the age of 55 years in men and 65 years in women. Overall, 34.5% (n = 289) had a positive family history of premature CVD.
Phenotypic familial hypercholesterolemia
According to the modified DLCN criteria, the majority of participants (78.9%, n = 661) were unlikely to have FH, 16.7% (n = 140) were possible cases of FH, 3.1% (n = 26) were probable FH cases, and only 1.3% (n = 11) were definite FH cases. Those with phenotypical FH (probable and definite FH) were on average significantly younger (62.2 vs. 69.8 years, p < 0.001) than participants without FH (unlikely and possible). The distribution of cardiovascular risk factors such as obesity, hypertension, and T2D was comparable between the groups. The proportion of current smokers was higher among participants with FH (45.9% vs. 17.4%, p < 0.001).
Lp(a)
A total of 19.3% of participants (n = 162) had elevated Lp(a) levels (≥ 107 nmol/L). There was no evidence of differences in sex, age, prevalence of hypertension, or current smoking among participants with and without elevated Lp(a) levels. The prevalence of T2D (21.0% vs. 29.1%, p < 0.027) and obesity (18.6% vs. 27.6%, p < 0.019) was significantly lower in patients with elevated Lp(a) than in participants without elevated Lp(a) (Supplementary Table 2a and b).
Overall, 21.5% of participants (n = 180) had either probable or definite phenotypic FH and/or elevated Lp(a) levels, i.e., evidence of a predominant genetic cause of dyslipidemia.
Associations between a positive family history of CAD, Lp(a), FH, LDL-C levels, and CAD status
In participants with a positive family history of premature CAD, the prevalence of CAD was higher than in participants without a family history of CAD (75.7% vs. 67.8%, OR 1.5, CI 1.1 to 2.1, p = 0.024, Fig. 2A), and on average, CAD was significantly more severe with a family history of premature CAD (p for trend = 0.007) (Supplementary Fig. 1A). Remarkably, the mean LDL-C (98.0 mg/dL vs. 100.5 mg/dL), mean recalculated medication-naive LDL-C (143.3 mg/dL vs. 135.7 mg/dL), and median Lp(a) plasma concentrations (20.7 nmol/L vs. 17.9 nmol/L) were similar between patients with and without a positive family history of premature CAD. We did not find evidence of an association between a positive family history of premature CAD and elevated Lp(a) (p = 0.206).

Prevalence of CAD according to. A presence of a positive family history of premature CAD in first degree relatives (men < 55 years, women < 65 years). B phenotypical (unlikely/possible vs. probable/definite) FH. C Lp(a) ≥ 50 mg/dL (107 nmol/L). Percentages of patients with CAD (red) and without CAD (green). *Patients not knowing family history were excluded (n = 77)
The prevalence of CAD increased significantly with increasing FH score (p for trend = 0.005) (Table 1). In participants with phenotypical FH (probable or definite), the prevalence of CAD was significantly higher than in participants without phenotypical FH (87.5% vs. 70.8%, OR 2.6, CI 1.0 – 6.9, p = 0.039; Fig. 2B).
Likewise, CAD prevalence was significantly higher in participants with elevated Lp(a) levels than in participants with normal Lp(a) levels (80.2% vs. 69.4%, OR 1.8, CI 1.2 -2.7, p = 0.006; Fig. 2C). Median Lp(a) levels increased with increasing CAD severity (p for trend = 0.009, Table 2), and participants with elevated Lp(a) levels were more likely to be diagnosed with more severe CAD than participants with normal Lp(a) levels (p for trend = 0.002) (Supplementary Figure 1B).
Lipid profiles and lipid-lowering therapy
Mean levels for total cholesterol (TC), LDL-C, HDL-C, triglycerides (TG), and median levels of Lp(a) are shown in Table 3.
There was evidence of sex differences for TC, LDL-C and HDL-C. Women had higher levels of TC (187.0 mg/dL vs. 161.6 mg/dL), LDL-C (112.4 mg/dL vs. 93.7 mg/dL), and HDL-C (59.1 mg/dL vs. 46.8 mg/dL) than men (p < 0.001). There was no evidence of a sex difference in the distribution of Lp(a) levels.
In the analyzed sample 516 (61.6%) participants received pharmacologic lipid-lowering therapy (LLT). Of these, 508 (98.4%) were treated with statins, 60 participants (11.6%) received ezetimibe, and only one participant used a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor (evolucumab). 465 participants (90.1%) were receiving a lipid-lowering monotherapy with statins, 8 participants (1.6%) were on a lipid-lowering monotherapy with only ezetimibe and 52 participants (10.1%) received a combination therapy of statin plus either ezetimibe or a PCSK9-inhibitor. A total of 322 participants (38.4%) did not receive any LLT. Participants with a preestablished diagnosis of CAD at study enrollment were more likely to be prescribed LLT (OR 8.9, CI 6.4 to 12.3, p < 0.001). However, 15.8% of participants (n = 68) with established CAD prior to study enrollment were not receiving LLT for secondary prevention.
Most participants were prescribed moderate-intensity statin treatment (66.5%, n = 343). A total of 9.5% (n = 49) received low-intensity statin treatment, and 24.0% (n = 124) received high-intensity LLT.
The higher the FH score, i.e., the probability of FH, the higher the LLT intensity was (p for trend < 0.001). No association was observed between elevated Lp(a) and LLT prescription and treatment intensity.
LDL-C goal attainment
Overall, lipid goal achievement was very poor in the analyzed sample. Only 35.4% (n = 297) of the total study population met the recommended LDL-C levels according to the 2016 guidelines [30]. According to the more recent 2019 guidelines, only 17.4% of participants (n = 146) met their respective goals [3].
Considering only participants on previously established lipid-lowering medication, LDL-C goal attainment was 42.2% and 20.5% according to the 2016 and 2019 guidelines, respectively.
Overall, only 32.6% of those with diagnosed CAD (195 of 599 participants) reached their LDL-C targets. If those participants, whose first-time diagnosis of CAD coincided with study inclusion, and in whom LLT had only been established denovo (“new CAD”) were excluded, a slightly higher proportion (38.5%) of participants met their LDL-C goals (166 of 431).
We found evidence that with more intense LLT, more patients accomplished target levels (p for trend 0.016). However, only half of the participants (63 of 124) with high-intensity LLT reached their recommended LDL-C levels.
With increasing FH score, the proportion of participants who reached target levels under LLT decreased (p for trend < 0.001) (Fig. 3A). Remarkably, in those with probable and definite FH (according to the DLCN score), no one met their recommended LDL-C levels.

LDL-C target value attainment under current treatment. (A) probability of phenotypical FH by DLCN criteria (unlikely FH DLCN score < 3, possible FH DLCN score 3–5, probable FN DLCN score 6–8, definite FH DLCN score > 8). (B) Lp(a) ≥ 50 mg/dL (107 nmol/L). (C) prevalence of either probable or definite FH (DLCN criteria) and/or Lp(a) ≥ 50 mg/dL. Percentages of patients reaching (green) or failing (red) their individual LDL-C target based on ESC/EAS guidelines 2016 for risk groups (very high-risk LDL-C < 70 mg/dL, high risk LDL-C < 100 mg/dl, intermediate risk < 115 mg/dL)
Similarly, LDL-C target accomplishment was significantly less likely in participants with elevated Lp(a) levels than in those with nonelevated Lp(a) levels (OR 2.1 CI 1.4- 3.4, 28.4% vs. 45.9%, p < 0.001) (Fig. 3B). When we examined the relationship between Lp(a) plasma concentration quintiles and the proportion of LDL-C target attainment, there was evidence of an inverse linear trend (50% in the 1st quintile, 54.8% in the 2nd quintile, 38.5% in the 3rd quintile, 41.8% in the 4th quintile and 29.5% in the 5th quintile (p for trend < 0.001)). The median distance to LDL-C target levels increased, with higher FH scores of 12.9 mg/dL, 45.8 mg/dL, 86.0 mg/dL and 109.5 mg/dL (participants grouped as unlikely, possible, probable, and definite FH, respectively) (p < 0.001). In an analogous manner, the median distance to the LDL-C target was higher in participants with elevated Lp(a) than in those with nonelevated Lp(a) (32.8 mg/dL vs. 19.3 mg/dL, p < 0.001). Consequently, when participants with either phenotypical FH (probable or definite FH score) or elevated Lp(a) were grouped together, target attainment was significantly less likely (48.6% vs. 23.5%, p < 0.001) compared to participants with neither clinical FH (unlikely or possible) nor elevated Lp(a) levels (Fig. 3C).
Discussion
The present study reveals major treatment gaps in LLT in primary and secondary prevention of CAD. Notably, 16% of participants with previously known CAD were not receiving any LLT. Furthermore, overall LDL-C goal attainment rates were low, a finding that is consistent with other studies [13, 14]. Even among those with high-intensity lipid-lowering (statin) treatment, only half reached the targets set by the 2016 ESC/EAS guidelines for the management of dyslipidemias [32]. Application of the new target goals from the revised 2019 ESC/EAS guidelines resulted in even lower goal achievement rates [14, 33, 34].
While recommendations for LDL-C levels for optimal risk reduction tend to decrease further, current treatments fail to provide sufficient LDL-C lowering. A reason for treatment failure could be noncompliance [13, 14, 17]. Other reasons could be an underestimation of cardiovascular risk by the treating physicians and the reluctance to prescribe high-intensity treatment due to fear of potential side effects [35]. In fact, most participants on LLT received only moderate intensity treatment.
There are various tools to assess the risk of ASCVD in clinical practice, such as "PROCAM”, the “SCORE” by the ESC/EAS, and pooled cohort equations, to name just a few [3, 16, 29]. Most focus on TC and LDL-C as treatment targets. Other ASCVD biomarkers, such as Lp(a), non-HDL-C, and apo B, are considered secondary treatment targets in patients with otherwise optimally controlled risk factors but have not yet been established in risk estimation [3, 36]. There is growing evidence that non-HDL-C and apo B are especially better markers for risk estimation of CVD, as both are less prone to biased measurement than LDL-C [37,38,39]. To date, the determination of apo B and non-HDL-C as treatment targets in clinical trials is not common, and more investigation on this topic is needed. In our study sample, the use of combination therapy with statins and either ezetimibe or PCSK9 inhibitors was very scarce, which certainly contributed to the overall low LDL-C goal attainment, as statin monotherapy is known to be insufficient for LDL-C management in high- and very-high-risk patients, which was the case in our study cohort [34]. Since recruitment took place from 2016 to 2018, when PCSK9 inhibitors had been on the market for only 2 years, just one participant in our sample received a PCSK9 inhibitor. However, even today, the prescription of PCSK9 inhibitors is very limited, presumably due to high costs [17, 34]. Indeed, more widespread use of combination therapies, including the common use of PCSK9 inhibitors in (very) high-risk patients, could contribute to higher goal attainment rates [35]. It has been shown that adding a PCSK9 inhibitor to statin-based LLT can increase LDL-C goal achievement rates significantly, up to 68% [17, 35].
Secondary to the LDL-C-lowering effect, PCSK9 inhibitors, in contrast to statins, have been shown to reduce Lp(a) levels as well [10, 26], which also contributes to cardiovascular risk reduction. Unfortunately, this effect is mainly observed in patients with low Lp(a) levels, leaving patients with high CVD risk due to Lp(a) elevation unaffected [33].
Other Lp(a)-lowering therapies, such as an antisense oligonucleotide targeting apolipoprotein a (APO(a)-LRx), will be available soon. [20]. Furthermore, more innovative pharmacotherapeutic approaches are in progress [40]. Thus, the therapeutic armamentarium will be growing.
As another aim of the study, we examined the importance of probable or definite genetic causes of dyslipidemia, namely, phenotypical FH and elevated Lp(a), for achieving LDL-C targets. Both those with high Lp(a) and probable or definite FH were less likely to meet recommended lipid targets despite the use of intense lipid-lowering therapeutics by the majority. This finding is in line with studies, which have shown shortcomings in the effective treatment of FH patients [17, 35]. Insufficient LDL-C control in FH patients despite intense statin treatment might be explained by higher pretreatment LDL-C levels, which cannot be lowered to a sufficient level by statins alone [17]. As another explanation, mutations in the LDL-C receptor, which are responsible for the clinical FH phenotype, might also mitigate the effects of statins [41].
Regarding the poor LDL-C control in participants with elevated Lp(a), there are indications that when measuring the LDL-C concentration, the cholesterol contained in Lp(a) is also measured; thus, this part is quasi “statin-resistant”, i.e., it cannot be modified via statin therapy [31, 42]. To clarify this question, in-depth further studies need to be conducted.
It should be noted that in the clinical routine, LDL-C is often calculated based on TC, HDL-C, and TG, instead of being measured directly. Depending on the equation used, LDL-C determination is susceptible to bias, especially when TG levels are high [36]. For instance, when calculated by the Friedewald formula, LDL-C is underestimated if TG levels are high, which may result in undertreatment. Other equations, e.g., by Martin et al. or Sampson, have been shown to give more accurate estimates, as do direct measurements [43, 44].
We not only observed poor LDL-C management but also higher CAD prevalence and severity in participants both with phenotypical FH and elevated Lp(a). Arguably, life-long exposure to higher LDL-C levels in FH patients, mutation status and elevated Lp(a) levels, in addition to other established risk factors for ASCVD, are responsible for increased CAD incidence, prevalence, and progression in these patients [4, 18]. There is evidence that those with phenotypical FH or elevated Lp(a) are at particularly high risk of CAD and CAD progression [9]. The importance of early detection and decisive prevention cannot be overstated. Hence, guidelines suggest measuring Lp(a) levels at least once in life for risk stratification [3, 45].
The prevalence of phenotypical FH according to the DLCN criteria was higher in our sample than the assumed prevalence in the general population [6]. This may be explained by the selection of our sample. As patients with clinical FH are at greater risk of CAD, it seems reasonable that in a cohort of patients admitted for catheterization due to (suspected) CAD FH prevalence would be higher than in the general population. However, the distribution of Lp(a) and the proportion of elevated Lp(a) were in accordance with the reported distribution and proportion, respectively, in the total population [4].
The Frederickson dyslipidemia classification has long been the standard. However, novel approaches in the phenotypical classification of dyslipidemias are needed. Contemporary advances suggest a simplified classification based on the lipid perturbance found in routine lipid profiles and the inclusion of Lp(a) and apo B [46]. A recent study by Sampson et al. developed a new phenotypical classification system based on non-HDL-C and TG levels following the classical Fredrickson-like phenotypes. Depending on the classification, guidance for physicians on adequate treatment was derived [47]. However, this categorization also lacks the inclusion of Lp(a).
Another aim of this study was to assess the importance of a positive family history of premature CAD. Our findings confirm that the prevalence of CAD and, in particular, cases of more severe CAD were increased in patients with a positive family history of premature CAD. At the same time, patients with and without a positive family history had similar LDL-C levels and inferred treatment-naive LDL-C levels. In this regard, a previous study by Bachmann et al. showed that men with a family history of premature CAD had a 50% increased relative risk for CAD development than participants without a family history of CAD [48]. These findings underline the importance of obtaining a family history of premature CVD, as it may inform and guide the diagnostic procedure. In addition, taking a family history of premature CAD together with LDL-C measurement remains a simple way to identify patients with probable genetically caused dyslipidemias [49].
While there has been evidence for an association between Lp(a) levels and a family history of premature CVD from several studies in children and adolescents [50,51,52], we did not find a significant association between elevated Lp(a) and a positive family history of premature CVD in our sample and other studies in adults [53]. Reasons for this discrepancy remain unclear.
Study strengths and limitations
A major strength of the study is the well characterized study population, including angiographic evidence of the presence of CAD, comprehensive lipid profiles and extensive family history assessment. A limitation is the lack of genetically verified FH diagnosis and the small proportion of phenotypical FH participants in the study sample. Another limitation is the absence of baseline LDL-C levels before the initiation of lipid-lowering treatment, so that treatment-naive had to be calculated instead, using published conversion factors. Furthermore, we had to use the PROCAM score for CVD risk estimation, as TC was not available in all cases. However, most of our cohort was already at very high risk given their CAD diagnosis, which made the risk calculation secondary in many cases. Last, there was no information about medication adherence or the duration of lipid-lowering treatment up to the time of the study.
Conclusion
In conclusion, our results reflect the current unsatisfactory treatment situation in the management of dyslipidemias for (secondary) prevention of ASCVD, pointing out the discrepancy between clinical recommendations and reality. Goal attainment was even worse when there was evidence of a definite or probable genetic cause of dyslipidemia, i.e., phenotypical FH and elevated Lp(a). The identification of these high-risk patients from the heterogeneous group of CAD patients is crucial to provide suitable prevention strategies and appropriate therapy. For that, more innovative treatment approaches need to be established.
Availability of data and materials
The datasets used and/or analyzed during the current study are available upon reasonable request (contact: ilja.demuth@charite.de).
Abbreviations
- Apo(a):
-
Apolipoprotein A
- ApoB:
-
Apolipoprotein B
- ASCVD:
-
Atherosclerotic cardiovascular disease
- CAD:
-
Coronary artery disease
- CVD:
-
Cardiovascular disease
- DLCN:
-
Dutch Lipid Clinic Network
- EAS:
-
European Artherosclerosis Society
- ESC:
-
European Society of Cardiology
- FH:
-
Familial hypercholesterolemia
- HDL-C:
-
High-density lipoprotein cholesterol
- LAD:
-
Left anterior descending artery
- LDL-C:
-
Low-density lipoprotein cholesterol
- Lp(a):
-
Lipoprotein(a)
- LLT:
-
Lipid-lowering therapies
- MACE:
-
Major adverse cardiovascular events
- PCSK9:
-
Proprotein convertase subtilisin/kexin type 9
- RCA:
-
Right coronary artery
- RCX:
-
Circumflex artery
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- T2D:
-
Type 2 diabetes
References
Ference BA, Ginsberg HN, Graham I, Ray KK, Packard CJ, Bruckert E, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease 1 Evidence from genetic, epidemiologic, and clinical studies A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459–72.
Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. 2016;37(42):3232–45.
Authors TF, M, Guidelines ESCCfP, Societies ESCNC. ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis. 2019;2019(290):140–205.
Nordestgaard BG, Chapman MJ, Ray K, Boren J, Andreotti F, Watts GF, et al. Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J. 2010;31(23):2844–53.
Schmidt K, Noureen A, Kronenberg F, Utermann G. Structure, function, and genetics of lipoprotein (a). J Lipid Res. 2016;57(8):1339–59.
Nordestgaard BG, Chapman MJ, Humphries SE, Ginsberg HN, Masana L, Descamps OS, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013;34(45):3478–90.
Gencer B, Kronenberg F, Stroes ES, Mach F. Lipoprotein(a): the revenant. Eur Heart J. 2017;38(20):1553–60.
Hopewell JC, Haynes R, Baigent C. The role of lipoprotein (a) in chronic kidney disease. J Lipid Res. 2018;59(4):577–85.
Willeit P, Ridker PM, Nestel PJ, Simes J, Tonkin AM, Pedersen TR, et al. Baseline and on-statin treatment lipoprotein(a) levels for prediction of cardiovascular events: individual patient-data meta-analysis of statin outcome trials. Lancet. 2018;392(10155):1311–20.
Ruscica M, Greco MF, Ferri N, Corsini A. Lipoprotein(a) and PCSK9 inhibition: clinical evidence. Eur Heart J Suppl. 2020;22(Suppl L):L53–6.
Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N Engl J Med. 2007;356(23):2388–98.
Wong ND, Chuang J, Wong K, Pham A, Neff D, Marrett E. Residual dyslipidemia among United States adults treated with lipid modifying therapy (data from National Health and Nutrition Examination Survey 2009–2010). Am J Cardiol. 2013;112(3):373–9.
Jones PH, Nair R, Thakker KM. Prevalence of dyslipidemia and lipid goal attainment in statin-treated subjects from 3 data sources: a retrospective analysis. J Am Heart Assoc. 2012;1(6): e001800.
Gitt AK, Lautsch D, Ferrieres J, Kastelein J, Drexel H, Horack M, et al. Low-density lipoprotein cholesterol in a global cohort of 57,885 statin-treated patients. Atherosclerosis. 2016;255:200–9.
Cooney MT, Dudina A, D’Agostino R, Graham IM. Cardiovascular risk-estimation systems in primary prevention: do they differ? Do they make a difference? Can we see the future? Circulation. 2010;122(3):300–10.
Goff DC Jr, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB Sr, Gibbons R, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63((25 Pt B)):2935–59.
Bogsrud MP, Graesdal A, Johansen D, Langslet G, Hovland A, Arnesen KE, et al. LDL-cholesterol goal achievement, cardiovascular disease, and attributed risk of Lp(a) in a large cohort of predominantly genetically verified familial hypercholesterolemia. J Clin Lipidol. 2019;13(2):279–86.
Khera AV, Won HH, Peloso GM, Lawson KS, Bartz TM, Deng X, et al. Diagnostic Yield and Clinical Utility of Sequencing Familial Hypercholesterolemia Genes in Patients With Severe Hypercholesterolemia. J Am Coll Cardiol. 2016;67(22):2578–89.
Cui Y, Li S, Zhang F, Song J, Lee C, Wu M, et al. Prevalence of familial hypercholesterolemia in patients with premature myocardial infarction. Clin Cardiol. 2019;42(3):385–90.
Tsimikas S, Karwatowska-Prokopczuk E, Gouni-Berthold I, Tardif JC, Baum SJ, Steinhagen-Thiessen E, et al. Lipoprotein(a) Reduction in Persons with Cardiovascular Disease. N Engl J Med. 2020;382(3):244–55.
Deshmukh HA, Colhoun HM, Johnson T, McKeigue PM, Betteridge DJ, Durrington PN, et al. Genome-wide association study of genetic determinants of LDL-c response to atorvastatin therapy: importance of Lp(a). J Lipid Res. 2012;53(5):1000–11.
Konig M, Joshi S, Leistner DM, Landmesser U, Sinning D, Steinhagen-Thiessen E, et al. Cohort profile: role of lipoproteins in cardiovascular disease-the LipidCardio study. BMJ Open. 2019;9(9):e030097.
Foody JM, Toth PP, Tomassini JE, Sajjan S, Ramey DR, Neff D, et al. Changes in LDL-C levels and goal attainment associated with addition of ezetimibe to simvastatin, atorvastatin, or rosuvastatin compared with titrating statin monotherapy. Vasc Health Risk Manag. 2013;9:719–27.
Melani L, Mills R, Hassman D, Lipetz R, Lipka L, LeBeaut A, et al. Efficacy and safety of ezetimibe coadministered with pravastatin in patients with primary hypercholesterolemia: a prospective, randomized, double-blind trial. Eur Heart J. 2003;24(8):717–28.
Stein EA, Ballantyne CM, Windler E, Sirnes PA, Sussekov A, Yigit Z, et al. Efficacy and tolerability of fluvastatin XL 80 mg alone, ezetimibe alone, and the combination of fluvastatin XL 80 mg with ezetimibe in patients with a history of muscle-related side effects with other statins. Am J Cardiol. 2008;101(4):490–6.
Schmidt AF, Pearce LS, Wilkins JT, Overington JP, Hingorani AD, Casas JP. PCSK9 monoclonal antibodies for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2017;4:CD011748.
Walma EP, Visseren FL, Jukema JW, Kastelein JJ, Hoes AW, Stalenhoef AF. The practice guideline “Diagnosis and treatment of familial hypercholesterolaemia” of the Dutch Health Care Insurance Board. Ned Tijdschr Geneeskd. 2006;150(1):18–23.
Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. BMJ. 2003;326(7404):1423.
Assmann G, Schulte H, Cullen P, Seedorf U. Assessing risk of myocardial infarction and stroke: new data from the Prospective Cardiovascular Munster (PROCAM) study. Eur J Clin Invest. 2007;37(12):925–32.
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Rev Esp Cardiol (Engl Ed). 2017;70(2):115.
Langsted A, Kamstrup PR, Benn M, Tybjaerg-Hansen A, Nordestgaard BG. High lipoprotein(a) as a possible cause of clinical familial hypercholesterolaemia: a prospective cohort study. Lancet Diabetes Endocrinol. 2016;4(7):577–87.
Fox KM, Tai MH, Kostev K, Hatz M, Qian Y, Laufs U. Treatment patterns and low-density lipoprotein cholesterol (LDL-C) goal attainment among patients receiving high- or moderate-intensity statins. Clin Res Cardiol. 2018;107(5):380–8.
Mahase E. Half of patients prescribed statins fail to hit target reduction in LDL cholesterol. BMJ. 2019;365:l1838.
Ray KK, Molemans B, Schoonen WM, Giovas P, Bray S, Kiru G, et al. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: the DA VINCI study. Eur J Prev Cardiol. 2021;28(11):1279–89.
Schmidt N, Dressel A, Grammer TB, Gouni-Berthold I, Julius U, Kassner U, et al. Lipid-modifying therapy and low-density lipoprotein cholesterol goal attainment in patients with familial hypercholesterolemia in Germany: The CaReHigh Registry. Atherosclerosis. 2018;277:314–22.
Carr SS, Hooper AJ, Sullivan DR, Burnett JR. Non-HDL-cholesterol and apolipoprotein B compared with LDL-cholesterol in atherosclerotic cardiovascular disease risk assessment. Pathology. 2019;51(2):148–54.
Sniderman A, Langlois M, Cobbaert C. Update on apolipoprotein B. Curr Opin Lipidol. 2021;32(4):226–30.
Sniderman AD, Robinson JG. ApoB in clinical care: Pro and Con. Atherosclerosis. 2019;282:169–75.
Marston NA, Giugliano RP, Melloni GEM, Park JG, Morrill V, Blazing MA, et al. Association of Apolipoprotein B-Containing Lipoproteins and Risk of Myocardial Infarction in Individuals With and Without Atherosclerosis: Distinguishing Between Particle Concentration, Type, and Content. JAMA Cardiol. 2022;7(3):250–6.
Nurmohamed NS, Navar AM, Kastelein JJP. New and Emerging Therapies for Reduction of LDL-Cholesterol and Apolipoprotein B: JACC Focus Seminar 1/4. J Am Coll Cardiol. 2021;77(12):1564–75.
Heath KE, Gudnason V, Humphries SE, Seed M. The type of mutation in the low density lipoprotein receptor gene influences the cholesterol-lowering response of the HMG-CoA reductase inhibitor simvastatin in patients with heterozygous familial hypercholesterolaemia. Atherosclerosis. 1999;143(1):41–54.
Tsimikas S. A Test in Context: Lipoprotein(a): Diagnosis, Prognosis, Controversies, and Emerging Therapies. J Am Coll Cardiol. 2017;69(6):692–711.
Erturk Zararsiz G, Bolat S, Cephe A, Kochan N, Yerlitas SI, Dogan HO, et al. Validation of Friedewald, Martin-Hopkins and Sampson low-density lipoprotein cholesterol equations. PLoS ONE. 2022;17(5):e0263860.
Vargas-Vazquez A, Bello-Chavolla OY, Antonio-Villa NE, Mehta R, Cruz-Bautista I, Aguilar-Salinas CA. Comparative assessment of LDL-C and VLDL-C estimation in familial combined hyperlipidemia using Sampson’s, Martin’s and Friedewald’s equations. Lipids Health Dis. 2021;20(1):46.
Ellis KL, Perez de Isla L, Alonso R, Fuentes F, Watts GF, Mata P. Value of Measuring Lipoprotein(a) During Cascade Testing for Familial Hypercholesterolemia. J Am Coll Cardiol. 2019;73(9):1029–39.
Berberich AJ, Hegele RA. A Modern Approach to Dyslipidemia. Endocr Rev. 2022;43(4):611–53.
Sampson M, Ballout RA, Soffer D, Wolska A, Wilson S, Meeusen J, et al. A new phenotypic classification system for dyslipidemias based on the standard lipid panel. Lipids Health Dis. 2021;20(1):170.
Bachmann JM, Willis BL, Ayers CR, Khera A, Berry JD. Association between family history and coronary heart disease death across long-term follow-up in men: the Cooper Center Longitudinal Study. Circulation. 2012;125(25):3092–8.
Grenkowitz T, Kassner U, Wuhle-Demuth M, Salewsky B, Rosada A, Zemojtel T, et al. Clinical characterization and mutation spectrum of German patients with familial hypercholesterolemia. Atherosclerosis. 2016;253:88–93.
Glowinska B, Urban M, Koput A. Cardiovascular risk factors in children with obesity, hypertension and diabetes: lipoprotein(a) levels and body mass index correlate with family history of cardiovascular disease. Eur J Pediatr. 2002;161(10):511–8.
Pac-Kozuchowska E, Krawiec P, Grywalska E. Selected risk factors for atherosclerosis in children and their parents with positive family history of premature cardiovascular diseases: a prospective study. BMC Pediatr. 2018;18(1):123.
Qayum O, Alshami N, Ibezim CF, Reid KJ, Noel-MacDonnell JR, Raghuveer G. Lipoprotein (a): Examination of Cardiovascular Risk in a Pediatric Referral Population. Pediatr Cardiol. 2018;39(8):1540–6.
Jubran A, Zetser A, Zafrir B. Lipoprotein(a) screening in young and middle-aged patients presenting with acute coronary syndrome. Cardiol J. 2019;26(5):511–8.
Acknowledgements
We would like to thank Sanofi-Aventis Deutschland GmbH for financial support and I.E.M GmbH, Germany for support of the pulse wave analysis. We kindly acknowledge the excellent cooperation with the Central Biomaterial Bank, the joint core facility of the Charité-Universitätsmedizin Berlin and the Berlin Institute for Health. We thank our student research assistants Fabiola Lugano, Marc Martinovic, Sabrina Bäther, Samita Joshi, Radostina Misirkova, and Ilona Enarovic for their excellent assistance during study implementation. Furthermore, we appreciate the great support by the whole team of the interventional cardiology unit. We acknowledge support from the German Research Foundation (DFG).
Funding
Open Access funding enabled and organized by Projekt DEAL. The LipidCardio Study was partially funded by Sanofi-Aventis Deutschland GmbH. This funder did not play a role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript and only provided financial support.
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: AS, ID, MK and ES-T. Recruitment of participants: AS, ID, UL, AH, MK. Providing routine clinical data: UL and AH. Collected study-specific data: MK and AS. Analyzed the data: MK and AS. Wrote the manuscript: MK, ES-T and AS. All authors revised and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was provided by all study participants, and the study was approved by the ethics committee at Charité-Universitätsmedizin Berlin (approval number: EA1/135/16).
Consent for publication
Not applicable.
Competing interests
No competing interests declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Figure 1.
severity of CAD for (A) patients with a positive family history of premature CAD in first degree relatives (men <55years, women < 65 years) *. (B) Lp(a) ≥ 50mg/dL (107nmol/L). Percentages of patients with no CAD, non-obstructive CAD, 1-vessel, 2-vessel, and 3-vessel CAD. *Participants not knowing family history were excluded (n=77).
Additional file 2: Supplementary Table 1.
Calculated LDL cholesterol reduction by LLT.
Additional file 3: Supplementary Table 2a.
Baseline characteristics of the sample, according to Lp(a) below and above upper quintile (50mg/dL ≈ 107 nmol/L). Supplementary Table 2b. Lipid profile of the sample, according to Lp(a)below and above upper quintile (50mg/dL ≈ 107 nmol/L).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schwarz, A., Demuth, I., Landmesser, U. et al. Low-density lipoprotein cholesterol goal attainment in patients with clinical evidence of familial hypercholesterolemia and elevated Lp(a). Lipids Health Dis 21, 114 (2022). https://doi.org/10.1186/s12944-022-01708-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-022-01708-9