
Abstract
Background
Some observational studies have found a significant association between the use of statin and a reduced risk of dementia. However, the results of these studies are unclear in patients with rheumatoid arthritis (RA). This study is to determine the association between the use of statins and the incidence of dementia according to sex and age-related differences in patients with RA.
Methods
We conducted a nationwide retrospective cohort study using the Taiwan Health Insurance Review and Assessment Service database (2003–2016). The primary outcome assessed was the risk of dementia by estimating hazard ratios (HRs) and 95% confidence intervals (CIs). Multiple Cox regression was used to estimate the adjusted hazard ratio of new-onset dementia. Subgroup analysis was also conducted.
Results
Among the 264,036 eligible patients with RA aged > 40 years, statin users were compared with non-statin users by propensity score matching at a ratio of 1:1 (25,764 in each group). However, no association was found between the use of statins and the risk of new-onset dementia (NOD) in patients with RA (HR: 1.01; 95% CI: 0.97–1.06). The subgroup analysis identified the use of statin as having a protective effect against developing NOD in male and older patients.
Conclusion
No association was observed between the use of a statin and the risk of NOD in patients with RA, including patients of both genders and aged 40–60 years, but these parameters were affected by gender and age. The decreased risk of NOD in patients with RA was greater among older male patients. Use of a statin in older male (> 60 years) patients with RA may be needed in clinical practice to prevent dementia.
Similar content being viewed by others


Background
Rheumatoid arthritis (RA) is a common autoimmune disorder that is characterized by systemic inflammatory polyarthritis. It affects approximately 1% of the global population [1, 2]. Previous studies have suggested an increased risk of cerebrovascular and neurodegenerative diseases among patients with RA [3, 4]. Furthermore, an early inflammation and cardiovascular diseases in patients with RA were associated with an increased risk of dementia [5, 6].
There were more than 50 million people living with dementia in 2016 worldwide, and this number is expected to increase with an increase in life expectancy [7]. It is one of the most common causes of disability among this group [8]. Many studies have demonstrated that RA is associated with an increased risk of cognitive decline and dementia [9,10,11]. Patients with RA and concurrent dementia may put a greater burden on their families and the health care system. Thus, minimizing the impact of incident dementia on patients with RA and their families is a crucial health-related challenge for health care personnel.
It has been suggested that hyperlipidemia is associated with an increased risk of dementia [12]. Statins are effective agents against hyperlipidemia and are widely used in the treatment of cardiovascular diseases [13, 14]. Statin therapy may also reduce the risk of dementia by reducing b-amyloid and serum apolipoprotein levels and exhibiting antithrombotic and anti-inflammatory effects [15]. Some observational studies have found a significant association between the use of statin and a reduced risk of dementia [16, 17]; however, two clinical trials had failed to show its beneficial effects on cognitive function [18, 19]. In fact, these studies presented inconsistent results. Additionally, these previous studies had not focused on patients with RA with respect to sex and age differences, as these patients have a higher risk of dementia. Therefore, the objective of this study is to evaluate the risk of dementia associated with the prescription of statins according to sex and age differences in a nationwide cohort study of patients with RA in Taiwan.
Methods
Study design
This is a retrospective cohort study. We used insurance claims data provided by the Taiwanese Bureau of National Health Insurance (BNHI) from January 2003 to December 2016. The BNHI stores complete follow-up information on major interventions and medications as well as admission, outpatient clinic, and emergency department visit records of the Taiwanese population. Statin users were defined as those patients who received statin prescriptions for more than 6 months during the study period and the respective index date was set as the initial statin use day individually. In contrast, non-stain users were designated as those patients who did not receive a statin prescription throughout the whole study period.
Study population
The study population comprised patients with RA (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code: 714.0) who were admitted to the hospital or outpatients who were newly diagnosed with hyperlipidemia (ICD-9-CM code272.X) and were statin users between 2003 and 2016. At least one of the following enrollment criteria had to be met for inclusion in this study: (1) two or more outpatient visits within a six-month period or (2) all statin prescriptions were continuously administered to the patients for more than 6 months within a 14-year follow-up period. Comorbidities related to dementia were as follows: coronary heart disease (ICD-9-CM code 410–415), hypertension (ICD-9-CM code 401–405), diabetes mellitus (ICD-9-CM code 250), and cerebrovascular attack (ICD-9-CM code 430–438). Patients who fulfilled any of the following criteria were excluded from the study: (1) had a prior history of dementia before January 1, 2003 and (2) patients aged less than 40 years. Given the differences in baseline characteristics and dementia risk between the statin users and non-statin users, we applied age, sex, RA duration, and propensity score matching at a ratio of 1:1 for patients with RA with and without statin use. Finally, the study group comprised 25,764 participants with RA who were statin users, and the control group included 25,764 randomly selected participants with RA who were non-statin users (Fig. 1).

Patient flow chart
Main outcome measures
The primary endpoint was the development of dementia, which was defined by the time a code of dementia (ICD-9-CM codes 290) first appeared in the inpatient or outpatient claim records.
Statistical analysis
Initially, the propensity score matching (PSMATCH) was conducted between two groups by using the Statistical Analysis System (SAS) software. The PSMATCH Procedure was used to perform the greedy nearest neighbor matching. First, the logistic regression was performed to estimate the logit probability of exposure to statin for each individual. The details of predictors including RA duration, sex, age, comorbidities, and concurrent medication taken by the patients are listed in Table 1. The algorithm used was the greedy nearest neighbor matching with the caliper of 0.01.
Differences in demographic data and clinical characteristics between statin users and non-statin users were examined using t-test for continuous variables, whereas chi-square tests were used for categorical variables. The dementia-free survival rates in the two groups were calculated using the Kaplan–Meier method and the log-rank test. The Cox proportional hazard regression model was used to compare the developmental risk of dementia (time-to-dementia) between the statin users and non-statin users, while controlling for selected covariates. After the unadjusted model was determined, further adjustments for age, gender, concurrent medication, and comorbidities were included. The hazard ratios (HRs) with 95% confidence intervals (CIs) of incident dementia by the statin users have been reported. P values < 0.05 were considered to be statistically significant for this study. All the statistical calculations were performed using statistical analysis software, version 9.3 (SAS Institute, Inc., Cary, NC, USA).
Results
Baseline information
Between January 2003 and December 2014, we identified 25,764 patients diagnosed with RA, aged > 40 years, and who were statin users. After 1:1 age, sex, the duration of RA, index date, and propensity score matching, 25,764 non-statin users were used for analyzing the relationship between the use of statin and incident dementia. The baseline characteristics of all patients with RA between the statin user group and non-statin user group are presented in Table 1. The absolute standardized differences between the two groups in all the variables were < 0.1 (10%), and the differences between matched pairs were statistically negligible.
The relative risk of incident dementia
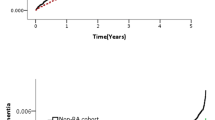
Among the 25,764 eligible patients with RA who were statin users, 1562 (6.1%) statin users and 1549 non-statin users (6.0%) developed dementia between 2003 and 2016. During a mean follow-up of 5.8 (SD, 3.6) years, a total 1549 and 1562 incident dementias/1000 person-years among statin users and nonusers (Table 2). There was no significantly difference of the incidence rate of dementia in the statin user group as compared to the non-statin user group (HR: 1.01; 95% CI: 0.97–1.06) (Table 2). The result of the Kaplan–Meier survival analysis also indicated that the risk of developing NODs showed no significantly difference between statin users and non-statin users (p = 0.6577) (Fig. 2).

Kaplan–Meier analysis of incidence probability of dementia in patients with rheumatoid arthritis, log rank p = 0.6577. Median of follow up time: Non-statin = 61 months, Statin user = 62
The relative risk of incident dementia in subgroup analysis
After adjusting sex, age, comorbidities, and concurrent medication, the age subgroup analysis showed a decreasing risk of incident dementia in statin users as compared to non-statin users (adjusted HR: 0.93; 95% CI: 0.86–1.00, p = 0.046) in patients with RA aged > 60 years (Table 3). Similarly, male statin users revealed a significantly lower development risk of dementia (adjusted HR: 0.88; 95%CI: 0.81–0.95, p = 0.0015) than female patients with RA aged > 60 years. However, the comparison of the duration of RA > 3 or 1–3 years with the duration of RA < 1 year showed no significant association with the developmental risk of dementia in both patients aged > 60 years (adjusted HR: 0.95 and 0.93; 95% CI: 0.86–1.04 and 0.85–1.02) and patients aged 40–60 years (adjusted HR: 1.18 and 1.35; 95% CI: 0.80–1.74 and 0.97–1.88) (Table 3).
Discussion
This study showed no association between the use of statin and the risk of NOD in patients with RA, but these parameters were influenced by gender and age differences. The decreased risk of dementia in patients with RA was greater in male and older (age > 60 years) patients. This study also demonstrated that RA duration showed no association of dementia incidence between patients who were using statins and patients who were not using statins.
The mechanism underlying the association between statin use and a decreased dementia risk in older male patients with RA may be complex [10, 20]. Several studies showed that systemic inflammation was involved in the pathogenesis of RA and dementia [3, 20, 21]. Additionally, these studies had suggested that an increased systemic inflammation is associated with an increased risk of dementia. Statin treatment is associated with a reduction in serum cytokine levels and C-reactive protein levels that might lower the risk of dementia in patients with RA. Another data show that serum cholesterol levels are linked with the deposition of β-amyloid and pathology of dementia [22, 23]. Statins may reduce the production of b-amyloid by the inhibition of cholesterol biosynthesis to decrease the production of amyloids and it could affect the onset and progression of dementia. However, the decreased risk of dementia in patients with RA was observed only in male patients in this study. Previous observational studies have also found results similar to our study [24, 25]. Zissimopoulos et al. evaluated 399,979 patients and the use of statin was associated with a reduced risk of Alzheimer’s disease in white women and men, Hispanic women and men, and black women. Their study showed that only statin use was not associated with a reduced risk of Alzheimer’s disease among black patients [24]. Finally, they concluded that factors such as race and sex showed an association between the use of statins and the incidence of dementia. Furthermore, it is explained that the clinical response to statins to reduce cholesterol and lipoproteins is variable and related to genetic heterogeneity [26].
Risk factors for dementia include old age and vascular atherosclerosis [27]. Old age causes vascular atherosclerosis, atrophy of the cerebral cortex, and hippocampus, which is associated with memory and spatial impairment. In our study, patients aged > 60 years exhibited a significant protective effect against NODs, whereas patients aged < 60 years did not show any significant association with a risk of developing NODs. This result demonstrates that age difference plays a major role in lowering the risk of NOD by statins among patients with RA. Further comprehensive basic and clinical research is warranted to elucidate the mechanisms underlying this association.
In addition to age, there was a gender-related difference of incident dementia in patients with RA between the statin and non-statin users in our study. Similarly, previous studies have demonstrated gender-related differences in statin treatment across a variety of study populations [24, 28, 29]. These gender-related differences in statin use can be attributed to the following reasons: females were less likely to report having been offered statin therapy, more likely to decline statin therapy when offered, and more likely to discontinue statin therapy after starting [30, 31].
Strengths and limitations
The strengths of our study are its population-based nature and a large sample size. This study was tested using propensity score matching to control for potential confounders, which established the feasibility of this hypothesis feasible. This study is the first one to provide a comprehensive evaluation on the association between the use of statin and dementia in patients with RA. Moreover, it also found a statistically significant decrease in the risk of NOD among older male patients who are statin users, along with an overall 14% decreased risk as compared to non-statin users. Nonetheless, there were some limitations in this study. Thus, the results should be interpreted with caution. First, our study lacks laboratory data such as blood cholesterol levels, low-density lipoprotein cholesterol levels, renal function, and liver function. Although we used the propensity score matching method to balance a wide range of dementia risk factors between statin users and non-statin users, we cannot exclude the effects of unmeasured confounders. Therefore, there were still other unmeasured confounding factors that may have biased our results. Second, we ascertained that the exposure to statin in the cohort is real and supported by the claims data, which include medication prescription. However, treatment adherence was not available from these secondary data. The protective effect of statins in the development of dementia in patients with RA may be underestimated. Third, we did not document the specific statin types used by the patients as they differ in their pharmacological properties; therefore, we could not evaluate the correlations between the specific statin types used and incident dementia in patients with RA. Finally, this study was based on the Taiwan NHI program and claims data sets, which may be of limited applicability to other countries; therefore, it is unclear that how those findings can be generalized to patient in different areas of the world.
Conclusion
There is no association between the use of statin and the risk of NOD in patients with RA; however, these parameters are influenced by gender and age. The decreased risk of NOD in patients with RA was greater among male and older patients. We suggested that statin should be used routinely in older male (> 60 years) patients with RA for the prevention of dementia in clinical practice.
Availability of data and materials
The data set analyzed in this study can be reasonably obtained from the corresponding author.
Abbreviations
- CI:
-
Confidence interval
- HR:
-
Hazard ratio
- ICD-9 CM:
-
International Classification of Diseases, Ninth Revision Clinical Modification
- NOD:
-
New-onset dementia
- RA:
-
Rheumatoid arthritis
References
Einarsson JT, Willim M, Ernestam S, Saxne T, Geborek P, Kapetanovic MC. Prevalence of sustained remission in rheumatoid arthritis: impact of criteria sets and disease duration, a Nationwide study in Sweden. Rheumatology. 2019;58(2):227–36. https://doi.org/10.1093/rheumatology/key054.
van der Woude D, van der Helm-van Mil AHM. Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2018;32(2):174–87. https://doi.org/10.1016/j.berh.2018.10.005.
Min C, Bang WJ, Kim M, Oh DJ, Choi HG. Rheumatoid arthritis and neurodegenerative dementia: a nested case-control study and a follow-up study using a national sample cohort. Clin Rheumatol. 2020;39(1):159–66. https://doi.org/10.1007/s10067-019-04769-x.
Liou TH, Huang SW, Lin JW, Chang YS, Wu CW, Lin HW. Risk of stroke in patients with rheumatism: a nationwide longitudinal population-based study. Sci Rep. 2014;4:5110.
Halacoglu J, Shea LA. Cardiovascular risk assessment and therapeutic implications in rheumatoid arthritis. J Cardiovasc Transl Res. 2020;13(5):878–90. https://doi.org/10.1007/s12265-020-09964-9.
England BR, Thiele GM, Anderson DR, Mikuls TR. Increased cardiovascular risk in rheumatoid arthritis: mechanisms and implications. BMJ. 2018;361:k1036.
Goerdten J, Čukić I, Danso SO, Carrière I, Muniz-Terrera G. Statistical methods for dementia risk prediction and recommendations for future work: a systematic review. Alzheimers Dement (NY). 2019;5(1):563–9. https://doi.org/10.1016/j.trci.2019.08.001.
GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–602.
Chou MH, Wang JY, Lin CL, Chung WS. DMARD use is associated with a higher risk of dementia in patients with rheumatoid arthritis: a propensity score-matched case-control study. Toxicol Appl Pharmacol. 2017;1:217–22.
Sangha PS, Thakur M, Akhtar Z, Ramani S, Gyamfi RS. The link between rheumatoid arthritis and dementia: A review. Cureus. 2020;12(4):e7855. https://doi.org/10.7759/cureus.7855.
Cosan F, Arda S, Demirci NO. The association of Parkinson disease with rheumatoid arthritis. Ann Rheum Dis. 2019;78(Suppl 2):1613.
Fan YC, Chou CC, You SL, Sun CA, Chen CJ, Bai CH. Impact of worsened metabolic syndrome on the risk of dementia: a nationwide cohort study. J Am Heart Assoc. 2017;6(9):e004749.
Cesena FHY, Valente VA, Santos RD, Bittencourt MS. Cardiovascular risk and statin eligibility in primary prevention: a comparison between the Brazilian and the AHA/ACC guidelines. Arq Bras Cardiol. 2020;115(3):440–9. https://doi.org/10.36660/abc.20190519.
Last AR, Ference JD, Menzel ER. Hyperlipidemia: drugs for cardiovascular risk reduction in adults. Am Fam Physician. 2017;95(2):78–87.
Tramacere I, Boncoraglio GB, Banzi R, Del Giovane C, Kwag KH, Squizzato A, et al. Comparison of statins for secondary prevention in patients with ischemic stroke or transient ischemic attack: a systematic review and network meta-analysis. BMC Med. 2019;17(1):67. https://doi.org/10.1186/s12916-019-1298-5.
Barthold D, Joyce G, Diaz Brinton R, Wharton W, Kehoe PG, Zissimopoulos J. Association of combination statin and antihypertensive therapy with reduced Alzheimer's disease and related dementia risk. PLoS One. 2020;15(3):e0229541. https://doi.org/10.1371/journal.pone.0229541.
Chang CF, Liou YS, Lin TK, Ma S, Hu YR, Chen HY, et al. High exposure to statins decrease the risk of new-onset dementia: a nationwide population-based longitudinal cohort study. Medicine. 2019 Aug;98(34):e16931. https://doi.org/10.1097/MD.0000000000016931.
Shepherd J, Blauw GJ, Murphy MB, Bollen EL, Buckley BM, Cobbe SM, et al. Pravastatin in elderly individuals at risk of vascular disease (PROS-PER): a randomised controlled trial. Lancet. 2002;360(9346):1623–30. https://doi.org/10.1016/S0140-6736(02)11600-X.
Heart Protection Study Collaborative Group. MRC/BHF heart protection study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360(9326):7–22.
Mason A, Holmes C, Edwards CJ. Inflammation and dementia: using rheumatoid arthritis as a model to develop treatments? Autoimmun Rev. 2018;17(9):919–25. https://doi.org/10.1016/j.autrev.2018.04.001.
Huang LC, Chang YH, Yang YH. Can disease-modifying anti-rheumatic drugs reduce the risk of developing dementia in patients with rheumatoid arthritis? Neurotherapeutics. 2019;16(3):703–9. https://doi.org/10.1007/s13311-019-00715-6.
Refolo LM, Pappolla MA, LaFrancois J, Malester B, Schmidt SD, Thomas-Bryant T, et al. A cholesterol-lowering drug reduces β-amyloid pathology in a transgenic mouse model of Alzheimer’s disease. Neurobiol Dis. 2001;8(5):890–9. https://doi.org/10.1006/nbdi.2001.0422.
Simons M, Keller P, Dichgans J, Schulz JB. Cholesterol and Alzheimer’s disease: is there a link? Neurology. 2001;57(6):1089–93. https://doi.org/10.1212/WNL.57.6.1089.
Zissimopoulos JM, Barthold D, Brinton RD, Joyce G. Sex and race differences in the association between statin use and the incidence of Alzheimer disease. JAMA Neurol. 2017;74(2):225–32. https://doi.org/10.1001/jamaneurol.2016.3783.
Wichmann MA, Cruickshanks KJ, Carlsson CM, Chappell R, Fischer ME, Klein BE, et al. Long-term systemic inflammation and cognitive impairment in a population-based cohort. J Am Geriatr Soc. 2014;62(9):1683–91. https://doi.org/10.1111/jgs.12994.
Mangravite LM, Thorn CF, Krauss RM. Clinical implications of pharmacogenomics of statin treatment. Pharm J. 2006;6(6):360–74. https://doi.org/10.1038/sj.tpj.6500384.
Uchoa MF, Moser VA, Pike CJ. Interactions between inflammation, sex steroids, and Alzheimer’s disease risk factors. Front Neuroendocrinol. 2016;43:60–82. https://doi.org/10.1016/j.yfrne.2016.09.001.
Hendrie HC, Hake A, Lane K, et al. Statin use, incident dementia and Alzheimer disease in elderly African Americans. Ethn Dis. 2015;25(3):345–54. https://doi.org/10.18865/ed.25.3.345.
Lin F-C, Chuang Y-S, Hsieh H-M, Lee TC, Chiu KF, Liu CK, et al. Early statin use and the progression of Alzheimer disease: a total population-based case-control study. Medicine (Baltimore). 2015;94(47):e2143. https://doi.org/10.1097/MD.0000000000002143.
Santalucia P, Franchi C, Djade CD, Tettamanti M, Pasina L, Corrao S, et al. Gender difference in drug use in hospitalized elderly patients. Eur J Intern Med. 2015;26(7):483–90. https://doi.org/10.1016/j.ejim.2015.07.006.
An T, Hao J, Sun S, Li R, Yang M, Cheng G, et al. Efficacy of statins for osteoporosis: a systematic review and meta-analysis. Osteoporos Int. 2017;28(1):47–57. https://doi.org/10.1007/s00198-016-3844-8.
Funding
This study was supported in parts by grants (TYAFGH-D-109041) from the Taoyuan Armed Forces General Hospital.
Author information
Authors and Affiliations
Contributions
TKL and LFP contributed to the data analyse and drafting of the manuscript. JYH collected and collated the data. GPJcontributed to the ideas and critical revisions of the manuscript and approved the final version of the manuscript to submit. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Chung Shan Medical University Hospital (CS2–19048). Written consent was not obtained from the study participants as only de-identified data were obtained from the Longitudinal Health Insurance Database, and a waiver of patient consent was provided by the Ethics Committee for this study.
Consent for publication
Not applicable.
Competing interests
The authors have declared no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lin, TK., Huang, JY., Pan, LF. et al. Gender- and age-related differences of statin use on incident dementia in patients with rheumatoid arthritis: a Nationwide population-based cohort study. Lipids Health Dis 20, 37 (2021). https://doi.org/10.1186/s12944-021-01465-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-021-01465-1