
Abstract
Background
Attaining acceptable levels of LDL Cholesterol (LDL-C) significantly improves cardiovascular (CV) outcomes in patients with type 2 diabetes mellitus (T2DM). The LDL-C target attainment and the characteristics of patients attaining these targets were investigated in this study. Furthermore, the reasons for not choosing statins and the physicians’ attitudes on the treatment of diabetic dyslipidemia were also examined.
Methods
A nationwide, cross-sectional survey was conducted in tertiary centers for diabetes management. Adult patients with T2DM, who were under follow-up for at least a year in outpatient clinics, were consecutively enrolled for the study. LDL-C goals were defined as below 70 mg/dL for patients with macrovascular complications or diabetic nephropathy, and below 100 mg/dL for other patients. Data about lipid-lowering medications were self-reported.
Results
A total of 4504 patients (female: 58.6%) were enrolled for the study. The mean HbA1c and diabetes duration was 7.73 ± 1.74% and 10.9 ± 7.5 years, respectively. The need for statin treatment was 94.9% (n = 4262); however, only 42.4% (n = 1807) of these patients were under treatment, and only 24.8% (n = 448) of these patients achieved LDL-C targets. The main reason for statin discontinuation was negative media coverage (87.5%), while only a minority of patients (12.5%) mentioned side effects. Physicians initiated lipid-lowering therapy in only 20.3% of patients with high LDL-C levels. It was observed that the female gender was a significant independent predictor of not attaining LDL-C goals (OR: 0.70, 95% CI: 0.59–0.83).
Conclusions
Less than 50 % of patients with T2DM who need statins were under treatment, and only a quarter of them attained their LDL-C targets. There exists a significant gap between the guideline recommendations and the real-world evidence in the treatment of dyslipidemia in T2DM.
Similar content being viewed by others


Introduction
The risk for atherosclerotic cardiovascular diseases (ASCVD) is very high in patients with type 2 diabetes mellitus (T2DM), occurring 10 years earlier than people without diabetes [1, 2]. Although effective glycemic control prevents microvascular complications [3, 4], it is not sufficient to reduce the cardiovascular outcomes [5, 6]. The regulation of other major cardiovascular risk factors is essential for the reduction of the total cardiovascular risk [7, 8]. Dyslipidemia is one of these major risk factors in patients with T2DM [9, 10]. Low-density lipoprotein cholesterol (LDL-C) levels are not significantly elevated. However, these patients have small and dense LDL particles, increased triglyceride, and reduced high-density lipoprotein cholesterol (HDL-C) levels [11, 12]. These alterations in lipid profiles are characteristic of diabetic dyslipidemia, which is highly atherogenic [11, 12]. The treatment of dyslipidemia is effective both in the primary and secondary prevention of cardiovascular morbidity and mortality [8, 13, 14]. However, many patients with T2DM are not receiving lipid-lowering treatment [15,16,17,18,19,20,21,22], and only a minority of those who are treated attain their lipid targets [16,17,18, 20, 21, 23].
The data about the lipid target attainment rates in Turkish patients with T2DM is inconsistent [24,25,26]. Previous studies, which were not representative enough, mentioned LDL-C attainment rates by using higher cut-off levels. Turkish Nationwide SurvEy of Glycemic and Other Metabolic Parameters of Patients with Diabetes Mellitus (TEMD Study), has been recently published, showing that LDL-C levels are < 100 mg/dL in only 37% of the patients with T2DM [25]. The present report, TEMD Dyslipidemia Study, further analyzes the TEMD database by defining two LDL targets for patients with high and very high risk. This study is designed to determine the rate of LDL-C target attainment in patients with T2DM according to the hypothesis of statin utilization, and the target LDL-C attainment rates are very low in Turkish patients with T2DM. Sociodemographic and clinical characteristics of patients who attain LDL-C targets, the reasons for not taking or withdrawing from statins, and physicians’ attitudes on the treatment of diabetic dyslipidemia were also assessed in this study.
Materials and methods
Study design
The TEMD Dyslipidemia Study has been conducted as a nationwide survey, between 01 April and 30 June 2017. The patients were registered from the tertiary centers throughout Turkey, which were allocated according to the 12 nomenclature of territorial units for statistics regions. The study protocol was approved by the Turkish Ministry of Health, Pharmaceuticals and Medical Devices Agency, Central Ethical Committee (14- MAR- 2017/93189304–514.11.01-E.58933), and registered in ClinicalTrials.gov (NCT 03455101). Informed consent forms were signed by the patients before data collection.
Study population
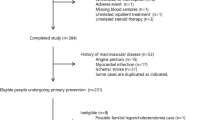
Each study center aimed to consecutively enroll the first 100 patients, who were under follow-up for at least 12 months and meet the inclusion criteria [25]. The present report includes only the data of patients with T2DM (n = 4504). The inclusion and exclusion criteria and the flowchart showing patient enrolment is given in Fig. 1.

Flow diagram of patient enrolment with inclusion and exclusion criteria
Data collection
All participants filled out questionnaires on sociodemographic characteristics, medications, complications, and concomitant diseases. The questionnaires also searched for data on personal diabetes management [diet, exercise, smoking, self-monitoring of blood glucose, and hypoglycemia frequency] and laboratory values. The data on statin usages, such as the history of initiation and discontinuation, the reasons for cessation (side effects, negative effects of the social environment or other), and the percentage of moderate or high potency statins were also evaluated. The introduction of new lipid-lowering medications, as well as changes in their dosing, were also evaluated.
Anthropometrics and laboratory data
The body mass index (BMI) was calculated by the ratio of weight to the square of height (kg/m2). Arterial blood pressure (BP) was recorded in all centers by the automatic BP monitors Omron M2, HEM-7121-E. The measurements were conducted after 5 min rest, and the average of the three consecutive measurements from the same arm was recorded. Patients were also asked to take blood pressure recordings at home twice a day for a week in the sitting position after 5 min of rest. The recordings were noted on the control visits.
All laboratory measurements were conducted in the hospitals where the interviews were performed. The overnight fasting blood samples were taken from the antecubital veins before 10:00 AM. Blood glucose and lipids were measured enzymatically. More specifically, glucose was measured by the hexokinase method in most hospitals, while the glucose oxidase method was used in several centers. Total Cholesterol was measured by cholesterol oxidase, HDL Cholesterol was measured by cholesterol esterase, and Triglycerides were measured by glycerol oxidase methods. Friedewald’s eq. [LDL-C = total cholesterol – (HDL-C + TG/5)] was used for the calculation of LDL-C levels. The formula was used only when the TG was less than 400 mg/dL [27]. Otherwise, LDL-C measurements were performed by the LDL-C measurement kits where available. Glycohemoglobin (HbA1c) measurement was performed by using one of the following methods: High-performance liquid chromatography, turbidimetric inhibition immunoassay, or enzymatic methods.
Definitions
The definition of dyslipidemia and the treatment targets were taken according to the suggestions of the Clinical Practice Guideline for Diagnosis, Treatment, and Follow-up of Diabetes Mellitus and Its Complications-2017, published by the Society of Endocrinology and Metabolism of Turkey [28], which was prepared according to the ADA-2017 and ESC/EAS-2016 guidelines [29, 30]. Dyslipidemia was defined as TG > 150 mg/dL and/or LDL-C > 100 mg/dL, and/or low HDL-C (men < 40 mg/dL, women < 50 mg/dL), or taking lipid-lowering medications. The target LDL-C level was defined as below 70 mg/dL for very high-risk patients (with macrovascular complications or diabetic nephropathy) and below 100 mg/dL for high-risk patients (without complications). Target TG was defined as < 150 mg/dL, target HDL-C was defined as > 40 mg/dL for men and > 50 mg/dL for women. Patients who attain the target LDL-C levels according to the current guidelines were also analyzed (< 55 mg/dl for very high-risk patients and < 70 mg/dL for high-risk patients) [31]. The following criteria were defined for the patients who need statins: (1) LDL-C levels over 70 mg/dL together with macrovascular complications or diabetic nephropathy; or (2) LDL-C levels over 70 mg/dL in patients over 40 years without any atherosclerotic CVD but with risk factors or markers of target organ damage; or (3) LDL-C levels over 100 mg/dL [29, 30]. A high potency statin was defined as atorvastatin ≥40 mg or rosuvastatin ≥20 mg per day [28,29,30].
Home BP recordings with values ≥135/85 mmHg or being under antihypertensive treatment was defined as Hypertension. If the patients did not have home BP recordings, the mean office BP ≥ 140/90 mmHg in two different visits was defined as hypertension. Having BMI ≥ 30 kg/m2 was defined as Obesity. Treatment targets for glycemia and arterial BP were defined as HbA1c < 7%, home BP < 135/85 mmHg [28, 29]. Performing regular physical activity more than twice per week was regarded as performing regular exercise. Patients having adrenergic symptoms with capillary glucose levels of 70 mg/dL or less were regarded as having hypoglycemia. A high education level was defined as attaining formal education for more than eight years. Macrovascular complications included coronary artery disease, cerebrovascular event, or peripheral artery disease. Additionally, non-palpable extremity pulses, low ankle-brachial index (≤ 0.9), or imaging that revealed established atherosclerotic plaque on coronary or peripheral arteriography, were used to define macrovascular disease. Nephropathy was defined as having albuminuria (≥ 30 mg/g) and/or decreased estimated glomerular filtration rate (eGFR) (< 60 mL/min/1.73 m2). Retinopathy was self-reported. Neuropathy was defined by the symptoms of bilateral symmetric distal neuropathy or other autonomous neuropathies attributed to T2DM.
Statistical analyses
Statistical analyses were performed with SPSS 18.0 (SPSS Inc., Chicago, IL, USA). Data for the categorical variables were expressed as percentages, and continuous variables were expressed as mean ± SD. Continuous variables were compared by using the independent-sample t-test, and the categorical variables were compared by the Chi-square test. The association of LDL-C target attainment with different variables were analyzed by the binominal logistic regression. The inclusion criteria for the model for these variables were the clinical rationale of a potential association with LDL-C target or having a statistical significance (P < 0.05) in univariate analyses. The parameters were gender, age (< 65 years vs. older), BMI (< 29.9 kg/m2 vs. ≥30 kg/m2), HbA1c (< 7% vs. ≥7%), BP (< 135/85 mmHg vs. higher), microvascular and macrovascular complications, regular exercise (<=2/week vs. higher), smoking, statin treatment, and being followed up by a private center vs. government hospital. The significance level of a two-tailed p-value was < 0.05.
Results
The sociodemographic and clinical characteristics of patients with T2DM (n = 4504, mean age 58.6 ± 10.4 years) are summarized in Table 1. Overall, only 20.5% (n = 922) of the total group attained target LDL-C levels. The target attainment rate was 32.7% (n = 649) for the high-risk patients (LDL goal < 100 mg/dL), and 10.8% (n = 273) for the very high-risk patients (LDL goal < 70 mg/dL). There was a female predominance in patients who did not attain target LDL-C levels (P < 0.001). These patients had higher SBP (P = 0.03), HbA1c (P = 0.015), triglycerides (P < 0.001) and HDL-C levels (P = 0.005), and had spent less time exercising (P < 0.001). The percentage of statin users (P < 0.001) and the ratio of being followed clinically in private medical centers (P = 0.001) were lower in these patients. These patients had higher micro- and macrovascular complications (P < 0.001 for both) and higher obesity rates (P = 0.005). Significantly fewer of these patients attained blood pressure targets (P = 0.02). When patients were assessed to determine if LDL-C targets recommended in current guidelines [31, 32], only 8.4% (n = 152) of patients attained target LDL-C levels.
The percentage of patients who qualified for statin treatment was 94.9% (n = 4262). However, only 44.8% (n = 1807) of these patients received statin treatment. The statin utilization rate was 32.2% (n = 640) for the high risk and 46.3% (n = 1167) for the very-high risk population. Only 24.8% (n = 448) of the patients who were on treatment, achieved the target LDL-C levels (Fig. 2).

Distribution of patients in terms of statin use. T2DM, type 2 diabetes mellitus; LDL, low-density lipoprotein
Only 10% of the patients on statin treatment were taking high potency statins. Most of the patients who were not taking statins had never been advised to do so (71.9%, n = 1869). Others were formerly treated, but treatment was subsequently withdrawn (28.1%, n = 740). Of these patients, 42.6% (n = 315) had their statins discontinued by their physician, while 57.4% (n = 425) chose to discontinue statin therapy of their own accord. Patients who discontinued statins commonly addressed the negative effects of social environment and media coverage (n = 372, 87.5%), while only a minority (n = 53, 12.5%) invoked the side effects of statins as being the cause of discontinuing these medications (Fig. 3). Most of the patients (n = 263, 85.7%) who discontinued statins according to the recommendations of the healthcare providers did not experience significant adverse side effects (Fig. 2). Physicians prescribed new lipid-lowering medications or changed the dosages of ongoing medications in only 20.3% (n = 727) of patients unable to achieve target LDL-C levels.

The reasons of not taking lipid lowering treatment in patients with T2DM
According to the multivariate analyses, the variables independently associated with risk-stratified LDL-C target attainment were the female gender (OR: 0.70, 95% CI: 0.59–0.83), microvascular (OR: 0.27, 95% CI: 0.23–0.32), and macrovascular complications (OR: 0.66, 95% CI: 0.53–0.81), performing exercise (OR: 1.37, 95% CI: 1.13–1.66), and taking statins (OR: 1.86, 95% CI: 1.58–2.19) (Fig. 4).

Multivariate analysis of factors associated with LDL-C goal attainment. BMI, body mass index; HbA1c, glycosylated hemoglobin
Discussion
The results of the TEMD Dyslipidemia study show that almost 80% of patients with T2DM do not attain LDL-C target levels in Turkey. Less than half of patients who need statins are under treatment and only a quarter of them attain LDL-C targets. Most of the patients who are not taking statins report that they were not advised to take statins by their physicians previously. The main reason for statin cessation is not the risk for adverse side effects, but rather the negative thoughts spread socially or by the media. The TEMD Dyslipidemia study also shows that female sex, receiving statin treatment, performing exercise, and having micro and macrovascular complications are independent predictors of LDL-C target attainment. Finally, it appears that Turkish physicians are not eager to prescribe statins to patients with diabetes mellitus.
The CVD risk is significantly increased in patients with T2DM [1, 2]. In order to establish risk reduction, not only glycemia levels, but also other cardiovascular risk factors should be controlled [9]. Dyslipidemia is prevalent in patients with T2DM [10], and attaining target lipid levels significantly reduces the risk of major cardiovascular outcomes in these patients [8, 13, 14]. However, reports from different regions of the world show insufficient LDL-C attainment rates [16, 17, 20, 21, 23]. One of the main reasons for this low level of target attainment may be the different risk states of the patients involved in these reports. It appears that people with diabetes having CVD or chronic kidney disease (CKD), achieve LDL-C targets much better than those without any comorbidities [17, 20, 23]. Among the different risk groups, people with recent acute coronary syndromes have the highest LDL-C goal attainment rates [17, 20]. The differences between the goal attainment rates are also related to the various definitions of LDL-C targets. The highest LDL-C target attainment rates in patients with diabetes are reported in Holland (%56) [16, 33]. However, the LDL-C targets in these reports were taken as ≤100 mg/dL both for the high-risk and very high-risk patients, in accordance with the Dutch lipid guidelines [34]. Finally, the progressive lowering of the LDL-C targets in recent years may be another reason for the discordance between the reports. Previous reports from Turkey mention the LDL-C target attainment rates between 15 to 25% [26, 35,36,37]. However, the target LDL-C was defined as < 100 mg/dl in all of these studies. In the current study, a lower LDL-C target was defined for very high-risk patients. This is probably the reason for relatively low achievement rates of the LDL-C targets (20.5% in total; 32.7% high risk and 10.8% very-high risk groups) in the TEMD Dyslipidemia study. This report is prepared before the publication of the recent dyslipidemia guidelines, which increasingly recommend much lower LDL-C targets in patients with T2DM [31, 38]. When study patients were reanalyzed according to current LDL-C goals, less than 10% of them were found to attain the LDL-C targets (9.6% high risk and 4.7% very-high). Overall, these data point to a significant disparity between the recommendations of the guidelines and real-world evidence in the management of diabetic dyslipidemia.
Statins are the most effective treatment for dyslipidemia, both in primary and secondary CVD prevention, as well as in patients with diabetes [8, 13]. Reports from different regions of the world show varying statin utilization rates, ranging from 20 to 70% [15,16,17,18,19,20,21,22]. One of the main reasons for the variations may be the different risk categories of the patients. Patients without CVD have significantly lower statin utilization rates, while the rates are between 41 and 70% in those with CVD [17, 19, 20, 22, 33]. However, the statin utilization rates of patients with similar cardiovascular risk states are also different in various regions of the world. Recent literature from the Netherlands and UK mention that about 66–70% of patients with diabetes without CVD are receiving statin treatment [16, 19], while the numbers from Germany, USA, China, and Japan are lower, ranging between 22 to 42% [17, 18, 21, 22] . The reason for the disparities of these countries with comparable socioeconomic status is not clear. Finally, increasing awareness about the advantages of statins may improve the statin utilization rates in time. According to reports from the USA, the statin utilization rates in patients with similar risk categories almost doubled in ten years, from 21 to 40% [22, 39]. According to the results of the present study, the 45% statin prescription rate (32.2% for the high risk and 46.3% for the very-high risk groups) in Turkey is similar to the rates reported in studies from countries such as Japan, China, Germany, and the USA [17, 20,21,22]. The results of the current study show that the statin prescription rates are increasing in Turkey. Previous reports mentioned only 20 to 33% of patients with diabetes were receiving statin treatment in Turkey [35, 37]. However, regarding the current recommendations on aggressive lipid therapy, the current rates of statin therapy in patients with diabetes are far from adequate. The current study shows that statins have never been prescribed previously in two-thirds of patients who are not currently being treated with a statin. It should be emphasized that the patients reported upon herein have been followed for at least one year in tertiary diabetes care units. Even in this selected patient population, it appears that physicians largely ignore statins and other lipid-lowering medications.
The TEMD Dyslipidemia study shows that statins were withdrawn in one-third of patients. The most important reason for statin cessation is not the side effects, but rather the negative effects of the media social environment. Negative campaigns on statins in media are effective throughout the world. It has also been shown in other populations that patients are likely to stop taking statins after negative media coverage [40, 41]. Negative campaigns against statins is a prominent issue for statin cessation in Turkey. In a previous survey, high rates of statin cessation was reported in patients with familial hypercholesterolemia due to the negative environmental effects [42]. The TEMD Dyslipidemia Study is the first nationwide study in Turkey, showing the link between negative news stories and the statin cessation rate in patients with T2DM. Negative media coverage appears to be a significant obstacle to the successful management of dyslipidemia, as statin discontinuation is associated with a significant increase in the risk of cardiovascular mortality and morbidity [43]. This problem may also influence doctors’ decisions on statins and their trust in the medical literature as well [44]. Regarding the medical records of the TEMD Study, physicians prescribe or increase the dosages of lipid-lowering drugs only in one-fifth of patients with high LDL-C levels. Unfortunately, the present report does not give us details about the reasons for the physicians’ inertia for the management of dyslipidemia in patients with T2DM. Previous reports point out the desire to avoid potential side effects or the lack of awareness of the guideline recommendations as the reasons for the physicians’ inertia in dyslipidemia treatment [45].
The TEMD Dyslipidemia study allowed us to better define patients who have uncontrolled LDL-C levels. These patients were predominantly women, they did not exercise, and they were likely to have obesity and macro- or microvascular complications. The effect of obesity on the pathogenesis of dyslipidemia is clearly defined [46], and the role of regular physical activity on achieving the LDL-C target is well reported [47]. However, why female sex is disadvantageous for the attainment of LDL-C targets is not clearly known. Reports from different countries also show that men are more likely to have adequate lipid control than women [18, 48, 49]. Possible explanations of the gender disparity may be the lower adherence to medications and lower prescription of statins among women [48,49,50,51]. Also, side effects of statins, especially muscle symptoms, occur more frequently in women, which may increase the statin cessation risk [52]. Women in Turkey often have a home dependent life, perform lesser physical activity than men, and have a higher prevalence of obesity [53]. These are the other possible factors decreasing the LDL-C target achievement rates in women. The TEMD Study also showed that micro- or macrovascular complications are negatively associated with the achievement of LDL-C targets. In the present study, it was found that patients with macro and microvascular complications have higher statin utilization rates than patients without complications (57% vs. 35%, respectively). The reason for the lower rates of achieving LDL-C targets despite the higher utilization of statins in complicated patients is probably to target lower LDL-C levels in these patients [28, 31, 38]. The negative thoughts of patients on statins and the physicians’ inertia might mutually prevent the use of higher dosages of statins in these patients with micro- or macrovascular complications.
Study strength and limitations
The enrollment of large numbers of patients and multicenter design are the notable strengths of the TEMD Dyslipidemia study. However, there are several limitations. First, the cross-sectional design of the study may preclude causal relationships between predictive factors and the achievement of LDL-C targets. Moreover, as all the enrolled patients were followed-up in tertiary endocrine or diabetes units, they were more likely to have multiple comorbidities and complications. The data about the lack of or withdrawal of lipid-lowering medications and presence of retinopathy were obtained by the interviews with patients, which may not be reliable. Also, the adherence of patients to lipid-lowering drugs was not evaluated. Finally, the physicians’ attitudes on lipid-lowering medications are not investigated in detail.
Conclusion
In conclusion, the TEMD Dyslipidemia study points out a significant gap between the recommendations of the guidelines and the real-world experience in Turkey. Only one in every five patients with diabetes achieves risk-stratified LDL-C targets even in the tertiary care centers for diabetes management. The negative media coverage appears to be the most common cause of statin withdrawal, and the physicians’ inertia to prescribe lipid-lowering drugs is prominent. Overall, these data point out that urgent measures should be taken to improve diabetes care in Turkey. In order to establish a nationwide policy change; it is extremely important to lead physicians by emphasizing the importance of lipid-lowering therapy on the cardiovascular outcomes of patients with diabetes. Also, public opinion should be affected by constantly educating patients about the evidence-based data and positive effects of statins in the lay media. Finally, further prospective studies should be implemented to observe the effects of these policy changes on patient outcomes.
Availability of data and materials
Data are available from the authors on request.
Abbreviations
- ASCVD:
-
Atherosclerotic cardiovascular diseases
- BP:
-
Blood pressure
- BMI:
-
Body mass index
- CKD:
-
Chronic kidney disease
- CVD:
-
Cardiovascular disease
- eGFR:
-
Estimated glomerular filtration rate
- HbA1c:
-
Glycohemoglobin
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- TEMD Study:
-
Turkish Nationwide SurvEy of Glycemic and Other Metabolic Parameters of Patients with Diabetes Mellitus
- T2DM:
-
Type 2 diabetes mellitus.
References
Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, et al. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation. 1999;100:1134–46.
Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1·9 million people. Lancet Diabetes Endocrinol. 2015;3:105–13.
Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837–53. https://pubmed.ncbi.nlm.nih.gov/9742976/.
Control TD, Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86.
ADVANCE Collaborative Group, Patel A, MacMahon S, Chalmers J, Neal B, Billot L, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560–72.
ACCORD Study Group, Cushman WC, Evans GW, Byington RP, Goff DC, Grimm RH, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362:1575–85.
Gæde P, Oellgaard J, Carstensen B, Rossing P, Lund-Andersen H, Parving H-H, et al. Years of life gained by multifactorial intervention in patients with type 2 diabetes mellitus and microalbuminuria: 21 years follow-up on the Steno-2 randomised trial. Diabetologia. 2016;59:2298–307.
Collins R, Armitage J, Parish S, Sleight P, Peto R, Group HPSC. MRC/BHF heart protection study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet. 2003;361:2005–16.
Rawshani A, Rawshani A, Franzén S, Sattar N, Eliasson B, Svensson A-M, et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2018;379:633–44.
Turner RC, Millns H, Neil HA, Stratton IM, Manley SE, Matthews DR, et al. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom prospective diabetes study (UKPDS: 23). BMJ. 1998;316:823–8.
Vergès B. Pathophysiology of diabetic dyslipidaemia: where are we? Diabetologia. 2015;58:886–99.
Soran H, Schofield JD, Adam S, Durrington PN. Diabetic dyslipidaemia. Curr Opin Lipidol. 2016;27:313–22.
Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HAW, Livingstone SJ, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the collaborative atorvastatin diabetes study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364:685–96.
Goldberg RB, Mellies MJ, Sacks FM, Moyé LA, Howard BV, Howard WJ, et al. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the cholesterol and recurrent events (CARE) trial. The Care Investigators. Circulation. 1998;98:2513–9.
Pauff BR, Jiroutek MR, Holland MA, Sutton BS. Statin prescribing patterns: an analysis of data from patients with diabetes in the National Hospital Ambulatory Medical Care Survey Outpatient Department and National Ambulatory Medical Care Survey Databases, 2005-2010. Clin Ther. 2015;37:1329–39.
Kuiper JG, Sanchez RJ, Houben E, Heintjes EM, Penning-van Beest FJA, Khan I, et al. Use of Lipid-modifying Therapy and LDL-C Goal Attainment in a High-Cardiovascular-Risk Population in the Netherlands. Clin Ther. 2017;39:819–27 e1.
März W, Dippel F-W, Theobald K, Gorcyca K, Iorga ŞR, Ansell D. Utilization of lipid-modifying therapy and low-density lipoprotein cholesterol goal attainment in patients at high and very-high cardiovascular risk: real-world evidence from Germany. Atherosclerosis. 2018;268:99–107.
Zhang X, Ji L, Ran X, Su B, Ji Q, Hu D. Gender disparities in lipid goal attainment among type 2 diabetes outpatients with coronary heart disease: results from the CCMR-3B study. Sci Rep. 2017;7:12648–7.
Steen DL, Khan I, Ansell D, Sanchez RJ, Ray KK. Retrospective examination of lipid-lowering treatment patterns in a real-world high-risk cohort in the UK in 2014: comparison with the National Institute for health and care excellence (NICE) 2014 lipid modification guidelines. BMJ Open. 2017;7:e013255.
Wang X, He Y, Wang T, Li C, Ma Z, Zhang H, et al. Lipid-lowering therapy and low-density lipoprotein cholesterol (LDL-C) goal achievement in high-cardiovascular-risk patients in Fuzhou. China J Cardiovasc Pharmacol Ther. 2020;46:1074248419899298.
Teramoto T, Uno K, Miyoshi I, Khan I, Gorcyca K, Sanchez RJ, et al. Low-density lipoprotein cholesterol levels and lipid-modifying therapy prescription patterns in the real world: an analysis of more than 33,000 high cardiovascular risk patients in Japan. Atherosclerosis. 2016;251:248–54.
Steen DL, Khan I, Becker L, Foody JM, Gorcyca K, Sanchez RJ, et al. Patterns and predictors of lipid-lowering therapy in patients with atherosclerotic cardiovascular disease and/or diabetes mellitus in 2014: insights from a large US managed-care population. Clin Cardiol. 2017;40:155–62.
Gitt AK, Lautsch D, Ferrieres J, Kastelein J, Drexel H, Horack M, et al. Low-density lipoprotein cholesterol in a global cohort of 57,885 statin-treated patients. Atherosclerosis. 2016;255:200–9.
Satman I, Imamoglu S, Yilmaz C, ADMIRE Study Group. A patient-based study on the adherence of physicians to guidelines for the management of type 2 diabetes in Turkey. Diabetes Res Clin Pract. 2012;98:75–82.
Sonmez A, Haymana C, Bayram F, Salman S, Dizdar OS, Gurkan E, et al. Turkish nationwide survEy of glycemic and other metabolic parameters of patients with diabetes mellitus (TEMD study). Diabetes Res Clin Pract. 2018;146:138–47.
İlkova H, Damcı T, Karşıdağ K, Çömlekçi A, Ayvaz G. The international diabetes management practices study (IDMPS) - Turkey’s 5th wave results. Turk J Endocrinol Metab. 2016;20:88–96.
Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502.
SEMT Diabetes Mellitus Study Group. Clinical Practice Guideline for Diagnosis, Treatment, and Follow-up of Diabetes Mellitus and Its Complications-2017. 9th Edition, 2017. ISBN: 978-605-4011-26-1.
American Diabetes Association. 2. Classification and Diagnosis of Diabetes. Diabetes Care. 2017;40:S11–24. https://pubmed.ncbi.nlm.nih.gov/27979889/.
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS guidelines for the Management of Dyslipidaemias. Eur Heart J. 2016;37:2999–3058.
Mach F, Baigent C, Catapano AL, Casula M, Badimon L, Chapman MJ, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2019;41:111–88.
SEMT Diabetes Mellitus Study Group. Clinical Practice Guideline for Diagnosis, Treatment, and Follow-up of Diabetes Mellitus and Its Complications-2020. 14th Edition, 2020. ISBN: 978-605-4011-40-7.
Heintjes E, Kuiper J, Lucius B, Penning-van Beest F, Kutikova L, Liem A, et al. Characterization and cholesterol management in patients with cardiovascular events and/or type 2 diabetes in the Netherlands. Curr Med Res Opin. 2017;33:91–100.
Wiersma T, Smulders YM, Stehouwer CD, Konings KT, Lanphen J. Samenvatting van de multidisciplinaire richtlijn 'Cardiovasculair risicomanagement' (herziening 2011) [summary of the multidisciplinary guideline on cardiovascular risk management (revision 2011)]. Ned Tijdschr Geneeskd. 2012;156(36):A5104.
Oguz A, Benroubi M, Brismar K, Melo P, Morar C, Cleall SP, et al. Clinical outcomes after 24 months of insulin therapy in patients with type 2 diabetes in five countries: results from the TREAT study. Curr Med Res Opin. 2013;29:911–20.
Kahya Eren N, Harman E, Dolek D, Emren S, Tütüncüoğlu AP, Nazli C, et al. The gap between the current dyslipidemia guidelines and the physicians' treatment targets in patients with type 2 diabetes in Turkey. Minerva Cardioangiol. 2014;62:287–95.
Damci T, Kultursay H, Oguz A, Pehlivanoglu S, Tokgozoglu L, Vascular risk study group. Sub-optimal drug treatment of diabetes and cardiovascular risk in diabetic patients in Turkey. A countrywide survey. Diabetes Metab. 2004;30:327–33.
Jellinger PS, Handelsman Y, Rosenblit PD, Bloomgarden ZT, Fonseca VA, Garber AJ, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease - Executive Summary. Endocr Pract. 2017;23(4):479–97.
Segars LW, Lea AR. Assessing prescriptions for statins in ambulatory diabetic patients in the United States: a national, cross-sectional study. Clin Ther. 2008;30:2159–66.
Matthews A, Herrett E, Gasparrini A, Van Staa T, Goldacre B, Smeeth L, et al. Impact of statin related media coverage on use of statins: interrupted time series analysis with UK primary care data. BMJ. 2016;353:i3283.
Schaffer AL, Buckley NA, Dobbins TA, Banks E, Pearson S-A. The crux of the matter: did the ABC's catalyst program change statin use in Australia? Med J Aust. 2015;202:591–5.
Haymana C, Berlik H, Güneş Y, Tunçez OE, Aytekin C, Tapıkara Z, et al. Identifying undiagnosed or undertreated patients with familial hypercholesterolemia from the laboratory records of a tertiary medical center. Turk Kardiyol Dern Ars. 2017;45:731–8.
Nielsen SF, Nordestgaard BG. Negative statin-related news stories decrease statin persistence and increase myocardial infarction and cardiovascular mortality: a nationwide prospective cohort study. Eur Heart J. 2016;37:908–16.
Nordestgaard BG. Why do the media report negative news about statins? Eur Heart J. 2018;39:337–8.
Laufs U, Karmann B, Pittrow D. Atorvastatin treatment and LDL cholesterol target attainment in patients at very high cardiovascular risk. Clin Res Cardiol. 2016;105:783–90.
Klop B, Elte J, Elte JWF, Cabezas M, Cabezas MC. Dyslipidemia in obesity: mechanisms and potential targets. Nutrients. 2013;5:1218–40.
Kraus WE, Houmard JA, Duscha BD, Knetzger KJ, Wharton MB, McCartney JS, et al. Effects of the amount and intensity of exercise on plasma lipoproteins. N Engl J Med. 2002;347:1483–92.
De Smedt D, De Bacquer D, De Sutter J, Dallongeville J, Gevaert S, De Backer G, et al. The gender gap in risk factor control: effects of age and education on the control of cardiovascular risk factors in male and female coronary patients. The EUROASPIRE IV study by the European Society of Cardiology. Int J Cardiol. 2016;209:284–90.
Ansell BJ, Fonarow GC, Maki KC, Dicklin MR, Bell M, Davidson MH, et al. Reduced treatment success in lipid management among women with coronary heart disease or risk equivalents: results of a national survey. Am Heart J. 2006;152:976–81.
Lewey J, Shrank WH, Bowry ADK, Kilabuk E, Brennan TA, Choudhry NK. Gender and racial disparities in adherence to statin therapy: a meta-analysis. Am Heart J. 2013;165:665–78 678.e1.
Ballo P, Balzi D, Barchielli A, Turco L, Franconi F, Zuppiroli A. Gender differences in statin prescription rates, adequacy of dosing, and association of statin therapy with outcome after heart failure hospitalization: a retrospective analysis in a community setting. Eur J Clin Pharmacol. 2016;72:311–9.
Karalis DG, Wild RA, Maki KC, Gaskins R, Jacobson TA, Sponseller CA, et al. Gender differences in side effects and attitudes regarding statin use in the understanding statin use in America and gaps in patient education (USAGE) study. J Clin Lipidol. 2016;10:833–41.
Satman I, Omer B, Tutuncu Y, Kalaca S, Gedik S, Dinccag N, et al. Twelve-year trends in the prevalence and risk factors of diabetes and prediabetes in Turkish adults. Eur J Epidemiol. 2013;28:169–80.
Acknowledgments
The physicians and nurses in every TEMD study center who took role in recruitment of patients are acknowledged as the collaborators of TEMD Dyslipidemia Study (see supplementary data). The authors also appreciatively acknowledge the critical reviews and contributions of Professor Meral Kayikcioglu and Professor Ilker Tasci during the preparation of the manuscript.
Consortium members and affiliations
TEMD Study Group:
Sibel Guldiken 19, Semra Ayturk 19, Murat Yilmaz 20, Mehmet Asik 21, Nevin Dinccag 18, Ramazan Cakmak 18, Fulya Turker 18, Cemile Idiz 18, Hulya Hacisahinogullari 18, Elif Bagdemir 18, Busra Yildiz 18, Ozlem Haliloglu 16, Seda Sancak 22, Levent Ozsari 23, Eylem Cagiltay 23, Oguzhan Deyneli 24, Eren Imre 24, Sait Gonen 25, S Nur Boysan 19, Yuksel Altuntas 26, Feyza Yener Ozturk 26, Meral Mert 27, Hamide Piskinpasa 27, Hasan Aydin 28, Sazi Imamoglu 29, Ozen Oz Gul 25, Sinem Kucuksarac Kiyici 30, Berrin Cetinarslan 31, Alev Selek 31, Teoman Dogru 32, Ali Kirik 32, Belgin Efe 14, Ahmet Kaya 33, Ilker Cordan 33, Suleyman Baldane 34, Cem Onur Kirac 34, Zehra Capa 3, Mustafa Cesur 35, Ilhan Yetkin 36, Demet Corapcioglu 37, Sule Canlar 37, Okan Bulent Yildiz 38, Suleyman Nahit Sendur 38, Bekir Cakir 9, Ahmet Corakci 39, Mustafa Kutlu 40, Neslihan Bascil Tutuncu 41, Yusuf Bozkus 41, Erman Cakal 42, Berrin Demirbas 43, Sibel Ertek 44, Mustafa Altay 45, Murat Dagdeviren 45, Amir Hossein Abedi 1, Sevki Cetinkalp 46, Hatice Ozisik 46, Guzide Gonca Oruk 47, Serkan Yener 48, Basak Ozgen Saydam 48, Engin Guney 49, Mustafa Unubol 49, Guzin Fidan Yaylali 50, Senay Topsakal 50, Zeliha Hekimsoy 51, Gulhan Akbaba 52, Ibrahim Aslan 53, Sefika Dalkiran 13, Esen Akbay 54, Kamile Gul 55, Muge Ozsan Yilmaz 6, Emre Bozkirli 56, Seher Cetinkaya Altuntas 12, Aysegul Atmaca 57, Elif Tutku Durmuş 57, Turkan Mete 58, Faruk Kutluturk 59, Ferit Kerim Kucukler 60, Oguz Dikbas 61, Safak Akin 62, Irfan Nuhoglu 63, Halil Onder Ersoz 63, Taner Bayraktaroglu 64, Pınar Sisman 65, Ibrahim Sahin 66, Sedat Cetin 66, Ilyas Capoglu 67, Emin Murat Akbas 67, Rıfkı Ucler 68, Mehmet Ali Eren 4, Alpaslan Kemal Tuzcu 69, Zafer Pekkolay 69, Mesut Ozkaya 70, Mustafa Araz 71.
19Trakya University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
20Corlu REYAP Private Hospital, Department of Endocrinology and Metabolism, Turkey.
21Canakkale 18 March University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
22University of Health Sciences, School of Medicine, Fatih Sultan Mehmet Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
23University of Health Sciences, School of Medicine, Sultanabdulhamit Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
24Marmara University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
25Istanbul Science University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
26University of Health Sciences, School of Medicine, Sisli Hamidiye Etfal Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
27University of Health Sciences, School of Medicine, İstanbul Bakırkoy Dr. Sadi Konuk Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
28Yeditepe University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
29Private Office.
30University of Health Sciences, School of Medicine, Bursa Sevket Yılmaz Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
31Kocaeli University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
32Balikesir University, School of Medicine, Department of Internal Medicine, Turkey.
33Necmettin Erbakan University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
34Selcuk University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
35Private Guven Hospital, Department of Endocrinology and Metabolism, Turkey.
36Gazi University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
37Ankara University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
38Hacettepe University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
39Ufuk University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
40Private Bayındır Hospital, Department of Endocrinology and Metabolism, Turkey.
41Baskent University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
42University of Health Sciences, School of Medicine, Diskapi Yildirim Beyazit Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
43TOBB University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
44Private Memorial Hospital, Department of Endocrinology and Metabolism, Turkey.
45University of Health Sciences, School of Medicine, Kecioren Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
46Ege University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
47University of Health Sciences, School of Medicine, Izmir Ataturk Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
48Dokuz Eylul University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
49Adnan Menderes University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
50Pamukkale University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
51Celal Bayar University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
52Mugla University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
53University of Health Sciences, School of Medicine, Antalya Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
54Mersin University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
55Kahramanmaras Sutcu Imam University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
56Baskent University, Adana Training Hospital, Department of Endocrinology and Metabolism, Turkey.
5719 Mayıs University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
58University of Health Sciences, School of Medicine, Samsun Training and Research Hospital, Department of Endocrinology and Metabolism, Turkey.
59Gaziosmanpasa University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
60Hitit University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
61Giresun University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
62Recep Tayyip Erdogan University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
63Karadeniz Technical University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
64Bulent Ecevit University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
65Kars Harakani State Hospital, Department of Endocrinology and Metabolism, Turkey.
66Inonu University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
67Erzincan University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
68Yuzuncu Yil University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
69Dicle University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
70University of Health Sciences, School of Medicine, Gaziantep Ersin Arslan Research and Training Hospital, Turkey.
71Gaziantep University, School of Medicine, Department of Endocrinology and Metabolism, Turkey.
Funding
The TEMD study has been funded by the Society of Endocrinology and Metabolism of Turkey (Grant no. 04/10/2016–01). Automated BP monitors were provided by Sanovel A/S. The funding agencies had no role in the design and conduct of the study; the collection, management, analysis and interpretation of the data; or the preparation, review or approval of the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
A.S. was the principal investigator of the study and responsible for study design and manuscript preparation. A.S. and F.B. wrote the manuscript in collaboration and share the first authorship. F.B., I.S., and T.S. took part in the study design, assignment of the health centers. C.H., and I.D. took part in data revisions and manuscript preparation. O.S.D., E.G., A.K.C., K.A., D.Ö., S.S., T.T., M.K.B., N.K., C.E. and V.Y. participated in the data revisions and final controls. I.S. was the senior advisor. She participated in the design of the study and made critical revisions on the final draft. C.B. was responsible for the design and statistical analyses. A.S., T.S., F.B., and I.S. are the guarantors of this work to the name of the Society of Endocrinology and Metabolism of Turkey (TEMD). They were responsible for the integrity of the data and they had fool accesses to the dataset. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study has been approved by The Central Ethical Committee (Turkish Ministry of Health, Pharmaceuticals and Medical Devices Agency, 14- MAR- 2017/93189304–514.11.01-E.58933).
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest within the context of this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bayram, F., Sonmez, A., Haymana, C. et al. Utilization of statins and LDL-cholesterol target attainment in Turkish patients with type 2 diabetes - a nationwide cross-sectional study (TEMD dyslipidemia study). Lipids Health Dis 19, 237 (2020). https://doi.org/10.1186/s12944-020-01408-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-020-01408-2