
Abstract
Background
In this paper, we demonstrate why and how both temporality and multimodality should be integrated in health related studies that include accessibility perspective, in this case healthy food accessibility. We provide evidence regarding the importance of using multimodal spatio-temporal accessibility measures when conducting research in urban contexts and propose a methodological approach for integrating different travel modes and temporality to spatial accessibility analyses. We use the Helsinki metropolitan area (Finland) as our case study region to demonstrate the effects of temporality and modality on the results.
Methods
Spatial analyses were carried out on 250 m statistical grid squares. We measured travel times between the home location of inhabitants and open grocery stores providing healthy food at 5 p.m., 10 p.m., and 1 a.m. using public transportation and private cars. We applied the so-called door-to-door approach for the travel time measurements to obtain more realistic and comparable results between travel modes. The analyses are based on open access data and publicly available open-source tools, thus similar analyses can be conducted in urban regions worldwide.
Results
Our results show that both time and mode of transport have a prominent impact on the outcome of the analyses; thus, understanding the realities of accessibility in a city may be very different according to the setting of the analysis used. In terms of travel time, there is clear variation in the results at different times of the day. In terms of travel mode, our results show that when analyzed in a comparable manner, public transport can be an even faster mode than a private car to access healthy food, especially in central areas of the city where the service network is dense and public transportation system is effective.
Conclusions
This study demonstrates that time and transport modes are essential components when modeling health-related accessibility in urban environments. Neglecting them from spatial analyses may lead to overly simplified or even erroneous images of the realities of accessibility. Hence, there is a risk that health related planning and decisions based on simplistic accessibility measures might cause unwanted outcomes in terms of inequality among different groups of people.
Similar content being viewed by others
Introduction
Human mobility is an indisputable component to the functioning of our societies [1]. From a social perspective, differentiation in the willingness and ability of individuals to move in physical space can be considered as a factor that contributes to social equality or inequality [2, 3]. Moreover, the interaction of an individual with the surrounding physical environment and social structures shapes not only one’s daily life practices [4], but also one’s health conditions [5–7]. Scholars from the disciplines of geography, urban planning, transportation, epidemiology and health research seek to better understand the linkage between individuals’ health and surrounding environment, such as socio-spatial inequalities in access to healthy food [8–12]. The discourse on access to food is largely about “food deserts”—a spatial concept referring to a geographical area where residents are lacking spatial and socio-economic access to affordable, healthy, and nutritious food [9, 13]. It is commonly considered that without access to healthy food, residents are left with an unhealthy diet leading to increased risk of obesity, diabetes, other chronic illnesses, and generally worsened health [8, 11, 14–20]. However, in analytical studies, the association between access to healthy food or “food deserts” and adverse health outcomes for people remain unclear [21–25]. One reason for the contradictory results may be the differences between conceptual approaches and methodological choices used to calculate accessibility.
Knowledge regarding the ability or need for people to move in order to access services, such as health services or healthy food, is commonly attained through the concept of accessibility [26], which can be defined as the ease of reaching a destination from a specific location using a particular transport mode [27]. Methodologically, in health related research spatial accessibility is measured using different metrics [28], which are predominantly either a naïve count of opportunities within a spatially fixed geographic unit (census tract, buffer zone) or a simple distance measure based on either a rough straight-line distance or road network metrics [11, 13, 19, 29–35]. Such metrics are easy to calculate and fairly robust, however they are static in nature and ignore the dynamics of people’s daily life. Moreover, conceptually speaking, studies neglect two essential domains in current (healthy) food accessibility research: temporality and multimodality. Temporality is a particularly important aspect in a 24/7 society, where people are living with increasingly individual daily rhythms [36]. Considering the mode of transportation, on the other hand, is crucial for considering accessibility across the broad social spectrum of society, including disadvantaged subgroups.
In this research, we aim to contribute to the theoretical and methodological framework of health related accessibility research. We demonstrate the importance of integrating various modes of transportation as well as temporal dynamics in transport and service networks to accessibility analyses. We test and apply this approach to study healthy food accessibility in an urban context. We propose an advanced framework for measuring spatio-temporal food accessibility by transport mode, and present: (1) how spatial access to healthy food is influenced by transport mode in time, and (2) how accessibility patterns vary spatially and temporally in relation to population distribution. The proposed framework provides more realistic analyses of food accessibility, which could help to better understand the association between accessibility and health.
Background
Human mobility and temporality of food accessibility
In line with calls emphasizing temporality and a person-based approach in social sciences [7, 37], there is a trend of incorporating temporal perspectives [38, 39] and a person-based approach [25] in food accessibility research, and measuring access to food beyond residential locations [40]. While spatial accessibility consists of temporal, physical, organizational, and financial components [26], the temporal dimension is essential from three different aspects.
First, arguably the measure closest to an individual’s embodied experience is that of travel time (or travel speed) instead of merely travelled distance, per se, due to the cognition of and/or the valuation of travel time [41]. Two other time-dependent aspects are demand and supply sides of access to and the use of healthy food opportunities by people.
From the demand side, time to access and buy healthy food depends on the persons’ complex spatial activity-travel behavior that varies on an hourly, daily, and weekly basis [41], and is influenced by seasonality [42, 43]. In our contemporary 24/7 society, activity-travel behavior of people is becoming more flexible and fragmented in space and time [44], particularly due to the flexibility in working schedules and night-shift working [45]. Thus, food purchasing is occurring throughout the day and includes a need for night shopping [46]. Neglecting the latter in calculating access to healthy food may lead to biased input regarding accessibility measures for health studies.
From the supply side, temporal variations in healthy food accessibility depends on both the structure of the facilities providing food as well as transport system. Opening hours of facilities providing food determine access to food as beyond opening hours the desired services are still inaccessible, regardless of spatial location [47, 48]. Access to food also changes on a monthly basis (seasonal markets) and across years as the network of facilities providing food changes [32, 49–51]. In the case of transport systems, access to food stores by public transport depends on time schedules, frequencies and transfer times of public transport and considering time-of-day, weekday and seasonality [52]. Even though users of private cars are less limited to move in space, at certain times of the day travelling by car is still more time-consuming due to traffic congestion [53–55] and difficulties in finding a parking place [56].
Therefore, disregarding an individual’s spatio-temporal travel behavior, the temporality of both transport systems and grocery services and interconnection between these components in accessibility modeling would result in significant overestimation of an individual’s actual access to food stores and underestimation of socio-spatial inequalities. Given the latter, this questions the conventional spatial definition of the “food desert” in health studies, which was well formulated by Widener and Shannon ([38], p. 3)—“[the question is] not just where we might find food deserts, but when”.
Realistic multimodal accessibility modeling
Another aspect to consider in line with the developments in Geographic Information Systems (GIS) [57] is the advancement in modeling the accessibility by private car and the incorporation of public transport. More realistic accessibility by private car is produced by implementing the stages of a journey and additional components of travel, such as traffic congestions, intersection delays, searching for free parking places, and mandatory walking from/to one’s car [53, 54, 56, 58]. Transport modes other than private car are often ignored and only recently are being incorporated, although with oversimplified assumptions.
In particular, when it comes to public transport with predefined routes and schedules, rather coarse and naïve (constant) assumptions are applied regarding travel distances of routes, travel speeds and transfer waiting times [59–61]. Fortunately, open data such as General Transit Feed Specification (GTFS) and crowdsourcing initiatives such as Open Street Map (OSM) enable advanced public transport and multimodal accessibility modeling. This provides more realistic comparisons of food accessibility between different transport modes, especially in densely populated urban areas with well-established public transport systems [55, 62–64].
In food accessibility research, studies by Farber et al. [47] and Widener et al. [25] are some of the first attempts to implement more advanced public transport modeling for access to food stores. However, many of the comparisons of modal accessibility disparities to date are based on rather oversimplified measures from the shortest travel distances based on road networks [65] to the optimistic “free float” travel times derived from speed limits of road segments [14]. These approaches question the realism and feasibility of such multimodal comparisons in practice. To the authors’ knowledge, this study is the first attempt to implement sophisticated modal accessibility disparity comparisons in health-related research.
We propose that the inclusion of transport modes and an adequate and realistic transport mode comparison are essential to examine food accessibility, given that: (1) from a public health perspective, the use of non-private car usage is related to more active physical activity that is associated with better health outcomes of people [66], whereas (2) from a social justice perspective, certain social groups (youth, elderly, disabled, marginalized or environmentally aware) may not (wish to) have access to a private car and therefore rely on other modes to reach services such as grocery stores [52, 61].
Methods
Study design
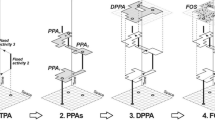
We explore multimodal, spatio-temporal food accessibility by measuring the travel times by private car and public transportation (PT) between the inhabitants and their closest open grocery store that offers healthy food at different times of the day. We use a widely applicable and sophisticated approach to analyze accessibility, which is presented in Fig. 1.

Study design using a nationally/internationally applicable framework to analyze multimodal spatio-temporal accessibility using open data and tools
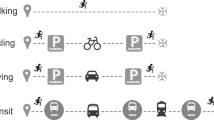
We use three different scenarios to demonstrate how changing service and transport networks in time affect access to healthy food. We chose the times for different scenarios (5 p.m., 10 p.m. and 1 a.m.) based on the general rhythm of the grocery store service network: (1) at 5 p.m. all the stores are open (baseline for the analysis), (2) at 10 p.m. only stores less than 400 m2 in size and (3) at 1 a.m. only small 24/7 grocery stores are allowed to stay open, according to legislation. The evolving 24/7 urban societies worldwide increase the demand for grocery shopping beyond non-standard working hours (e.g., at night) for different reasons [46, 67]. Night-time grocery shopping is predominantly due to the limited time availability of people working in shifts or having a variable work schedule. Finland is among the countries having the highest share of night workers (7.5 % in 2014) in Europe [67, 68]. This indicates a potential demand for grocery services around the clock, although there are only few grocery stores in the Helsinki region that are open at night (Fig. 2).

a Population density in HMA, b spatial distribution of grocery stores at different times of the day, c location of the study area in southern Finland
We explore the differences of the scenarios by showing their change in time geographically and in terms of modal differences, and in relation to accessible population by using cumulative accessibility curves and bar plots showing the variation between different municipalities in the Helsinki metropolitan area. In this study, we demonstrate the temporal and modal effects using a register-based night-time population; however, the underlying population could be chosen based on different socio-economic characteristics, for instance, which is often the case in health related research.
Study area
We use Helsinki metropolitan area (HMA) in Finland as our case study area to demonstrate the effect of temporality and multimodality to health related accessibility analyses. HMA is the capital region of Finland consisting of four municipalities: Helsinki, Espoo, Vantaa, and Kauniainen (Fig. 2). The tiny municipality of Kauniainen is an enclave of Espoo; therefore, we include Kauniainen hereafter as part of Espoo. HMA is the biggest urban region with around one million inhabitants.
HMA is a good example of a region where more sustainable and healthier options for transport (i.e., public transport and cycling) are promoted in government policies and city planning strategies, but where the service centralization and urban sprawl [68] in the last decades have increased the travel need and distances between customers and services, which in turn tends to promote car usage [69–71]. In terms of services, HMA has gone through a structural change where the number of grocery stores has dramatically declined [72] while the average size of the stores has increased [73], mostly concentrating on hypermarkets (>2500 m2 in size, selling groceries and general merchandise).
Data sources
The grocery store dataFootnote 1 includes addresses and opening hours of grocery stores that were collected from the websites of store chains or single stores (openly available). We only take into account grocery stores that offer healthy food, thus the product selection must include fruits, vegetables and dairy products (e.g., in supermarkets and hypermarkets, small convenience stores and natural food stores). Ethnic stores, gas stations and kiosks were excluded from the analysis, since their selection of products is typically rather limited. In all, the analysis included 396 stores (see Fig. 2), which were all treated equally (i.e., given equal weight) in the analysis (c.f. Yeager and Gatrell [29]). Other important data sources are listed in Table 1 and described as part of the computational tools.
Multimodal travel time calculations
We apply 250 m × 250 m statistical grid cells as the most precise spatial units corresponding to the official spatial database of Statistics Finland (i.e., the spatial division of residential population). We calculated the fastest routes from the centroids of all statistical grid cells to the nearest grocery store. Grocery shopping, of course, is influenced by many factors (e.g., accessibility, the selection of products, price level, customer loyalty) [74, 75]; however, to highlight the temporal variability in accessibility we measure travel time only to the (timewise) nearest store without using a gravity-based spatial access model (e.g., Huff’s [76]), which is often used for predicting customer behavior in a more detailed way [77]. Only the open stores at each particular time were included in the calculations.
We applied two freely available open-source tools for spatio-temporal multimodal routing in the Helsinki region to model travel times by private car and public transport. The tools for both travel modes are based on an advanced temporally sensitive door-to-door approach where every stage of a journey between origin and destination is taken into account. This enables the calculation of more realistic and comparable travel times from the origin location to the destination at different times of the day.
In terms of private car use, our accessibility model calculates travel times by taking into account: speed limits and distances of each road segment, cross-road penalties by road class, an average time spent for walking from home to a parking place, an average time spent for searching a vacant parking space at the destination, and an average time spent for walking from a parking place to the destination. For PT, travel times are calculated based on up-to-date PT routes and schedules and also consider walking segments during the trip and transfer times between PT vehicles. Applied models are explained in more detail in Salonen and Toivonen [64] and their technical implementations and source codes are openly available in Github.Footnote 2
We used the MetropAccess-DigiroadFootnote 3 (runs on Windows/Linux with ArcGISFootnote 4 software) for car travel time/distance calculations that takes into account traffic conditions at different times of the day (rush hour vs daytime). The tool transforms the national road and street database DigiroadFootnote 5 into a network dataset and adds empirically defined intersection delay values to different types of crossings [64, 78]. The tool calculates travel times between given origins and destinations by first defining the “free-flow” drive-through time for each road segment, based on the speed limit information and the length of the respective road segment, then adding an intersection movement delay value specific to the respective road class at certain time, and finally adding an estimate of parking-related time. The intersection movement delay values are derived from floating car measurements where real travel times during different times of the day along different types of roads in HMA are measured with a GPS, similar to Ziliaskopoulos and Mahmassani [53], Vetter and Geisberger [58] and Yiannakoulias et al. [54]. The rush hour intersection delay values were used in the calculation at 5 p.m. and normal daytime values (indicating approximate travel times at noon) at 10 p.m. and 1 a.m.
We used MetropAccess-ReititinFootnote 6 [79] (runs on Windows/Linux, requires Node.jsFootnote 7 package) to calculate public transportation travel times and distances between given origin and destination points by public transport based on the advanced door-to-door approach [64]. A modified version of Dijkstra’s algorithm [79, 80] is used to optimize routes between the given origins and destinations. OpenStreetMapFootnote 8 (OSM) is used for calculating the walking parts of the routes, whereas several routing parameters, such as walking speed, departure/arrival date and time, transport mode, and maximum walking distance can be adjusted flexibly. Calculations were based on schedules of a normal weekday (May 5, 2014), walking speed was set to 70 m/min (4.2 km/h), and arrival times were set as 5 p.m., 10 p.m., and 1 a.m. The calculations are based on openly available PT route and schedule dataFootnote 9 from the Helsinki Region Transport. As a result, the tool creates a text file where each row presents one origin–destination pair and the calculated route between the respective points, with extensive attribute information (e.g., route travel time, route distance and the travel modes used, access/egress times, etc.).
For short travel distances, walking is often the fastest travel mode and in such case the tool uses only walking for calculating the travel time as it is the most optimal transport mode for reaching the destination. Thus PT in our approach represents either public transport (including walking stages) or just walking.
Results
Access to healthy food is affected by temporality
Our results show that both the transport mode and the time of the day have a prominent impact on accessibility of grocery stores providing healthy food. Figure 3 shows the temporal variation in terms of how fast the population can reach the closest grocery store in our case study region. Depending on the time of the analysis the results are notably different. For instance, if looking at the proportion of population that reaches the closest grocery store within 15 min, the results by PT vary from 90 % (5 p.m.), 70 % (10 p.m.) to only 15 % (1 a.m.). Travel times by private car are significantly lower, thus almost 100 % of the citizens would reach the closest grocery store in 15 min at 5 p.m. and 10 p.m., but only 55 % during the night-time (1 a.m.). Overall, there is significant variation in the results that is caused by temporal changes in the transport system and in the service network.

Temporal variation in accessibility to closest grocery stores reached by HMA citizens with different modes of transportation. 100 % ≈ 1,000,000 inhabitants
Mode of transport affects the spatio-temporal access to healthy food
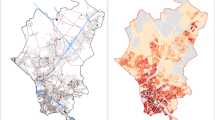
Maps in Fig. 4 extend the previous findings and show the modal differences in accessibility to grocery stores in spatial terms. Results show that there are distinct differences between travel modes in addition to temporal variation. In terms of travel time, PT is actually the fastest travel mode, especially in central Helsinki where PT is always faster (orange areas) or equally fast (white areas) compared to private cars. This might be a slightly surprising finding, although a rational one, as walking and PT are often faster in downtown areas where there is a lot of traffic and it is difficult to find a parking place for a car. In general, even though there are differences between travel modes in terms of travel time, they remain less than 10 min in all areas where there is population (c.f. Fig. 2) at 5 p.m. and 10 p.m. This indicates that PT and private car are equally lucrative options for accessing healthy food in the HMA in terms of travel time, which is a positive result from the perspective of social justice. In outer areas of the HMA private car is still the most viable travel mode in terms of travel time; however, such areas are typically sparsely populated.

Spatio-temporal accessibility comparisons showing the competitiveness of a transport mode (PT or private car) when travelling from home to the closest grocery store offering healthy food. Values represent the difference in travel times between PT and private car (PTt − Cart)
In health research the spatio-temporal accessibility patterns shown previously are not necessarily the most interesting results, per se. However, when adding underlying population information to the analyses, it is possible to obtain highly relevant and important information supporting health related decision making. Comparing the share of population by transport mode competitiveness zones (Fig. 5) in different municipalities of the HMA at different times of the day shows that there are significant changes in the results, both in temporal and modal terms. Looking at the general situation in the whole HMA, the results show that PT is highly competitive against car use at 5 p.m. when all the food stores are open. At 5 p.m. every third inhabitant lives in areas where PT is faster than a car, and over 60 % of the population lives in areas where PT is a faster or equally fast option compared with using a car. At 10 p.m., when some 60 % of the studied food stores are closed, PT still remains a lucrative travel mode for shopping for more than 40 % of the people. However, at night-time (1 a.m.) the feasibility of PT decreases dramatically and using a car is faster, except in the neighborhoods around the 24 h grocery stores. Hence, car is the faster transport option for 91 % of the people at this given time.

Population distribution by transport mode competitiveness zones (see Fig. 4 for the zones on a map), municipality and time of the day
In addition, there are clear differences in competitiveness of PT against car usage between different municipalities of the HMA. In Helsinki, PT is clearly the most viable travel mode for reaching the closest grocery store at 5 p.m.: more than 40 % of the population can access the closest store with PT faster than by car, and nearly 80 % of the population faster or equally fast as by car. In contrast, the situation in Vantaa and Espoo is fairly different as the competitiveness of PT is clearly lower: approximately 20 % of the population can reach the closest store faster by PT in Vantaa and Espoo, and less than half of the population faster or equally fast as by driving with car. Thus, the results support our current understanding that Helsinki is the most PT oriented city in the HMA, whereas Espoo and Vantaa are more car oriented cities.
Discussion
In this paper we have demonstrated why and how both temporality and multimodality should be integrated to health related studies that include an accessibility perspective. Today, the majority of accessibility related studies in health research apply only static and very simplistic accessibility measures and analyze only a single transport mode. Hence, these studies neglect the multifaceted spatialities of people that daily social life presuppose in our mobile 24/7 societies [36].
The proposed advanced accessibility approach utilizes door-to-door modeling with temporally sensitive accessibility measures. Such an approach was previously difficult to implement in practice due to the lack of reliable data. The recent open data development and novel data sources, such as those listed in Fig. 1 have made it possible to carry out more realistic and up-to-date analyses. Our proposed approach is generic and widely applicable given that it is built on openly available input data sources that are available for hundreds of regions worldwide. For example, we could have used up-to-date spatio-temporal information on public transportation in GTFSFootnote 10 format, which would allow us to make comparative studies, for instance between different European cities in a similar manner to that demonstrated here by comparing the results between municipalities of the HMA. Furthermore, similar to the applied tools in this study [64], other openly available GIS-based accessibility tools, such as Open Trip PlannerFootnote 11 and Google Maps Directions APIFootnote 12 are freely available for everyone and these can be used to analyze spatio-temporal accessibility patterns by various travel modes.
Our results show that both time and mode of transport clearly affect the outcomes of the analyses and depending on the time and mode of transportation, the understanding of accessibility realities of a city may be very different. In terms of time, the variation in accessibility patterns is evident especially considering PT, but also with private cars, particularly after more significant changes in the service network. In the case of comparing transport modes, our results show that car is not always the fastest travel mode for accessing services: PT can be as fast as, or even faster than private car especially if the PT system is efficient and the service network (e.g., healthy food stores) is fairly dense. These components, in turn, are largely affected by the time of day due to varying opening hours, changing traffic conditions and PT schedules. In our study area, the differences between travel modes were actually fairly modest due to the efficient and comprehensive PT network. However, if similar comparisons were to be made in a region with a less efficient PT network, the modal inequality among residents (or subgroups) could be much higher and accessibility realities might even be contradictory [81]. In this study the analyses were based on static (night time) population distribution; however, novel data sources such as mobile phone data [42] or social media data [82] could be used to evaluate the whereabouts of the population at different times of the day. Incorporating spatio-temporal information about population distribution would further enhance our approach because all analysis components (transport network, service network, and underlying population) would be dynamic.
Why are aforementioned findings significant in terms of health research? In health geography studying how specific groups of people (such as elderly, young people, obese, low-income etc.) can access services such as healthcare or food stores providing healthy food is an increasingly relevant topic. Our results also contribute to the food desert discussion by clearly indicating that time is an essential determinant in access to healthy food (and other health related services), especially for those who work during a non-standard working hours [67]. Night-shift working increases the risk of unhealthier lifestyles, which may be due to poorer access to health promoting services [83, 84]. Moreover, our results show clearly how access to services also depends on transport mode. For example the current spatial concept of “food desert”, referring to a geographical area where disadvantaged (e.g., low-income) residents are lacking spatial access to affordable and healthy food, should be revised to include not only the time dimension [38] but also different modes of transport in order to obtain more realistic outcomes. For example, while low-income population tend to use PT as their main transport mode for daily mobility, it is relevant to measure potential food deserts based on accessibility by PT and not only by private car. Overall, when planning health related systems or implementing policy interventions for tackling health inequalities, realistic information about multidimensional accessibility is needed to ensure equitable services for people with different socio-economic and demographic backgrounds.
Conclusions
To conclude, we have demonstrated that the realities of accessibility may be very different at different times of the day and from the perspective of a person who uses a car compared to a person who does not; facts that are often neglected in accessibility related health research. Therefore, we propose that more realistic, temporally sensitive, multimodal approaches for accessibility measurements should be adopted in accessibility research [7, 37, 48], health research [12, 57], and in relation to access to healthy food [38, 39, 47].
Notes
References
Urry J. Mobilities. 1st ed. London: Wiley; 2007.
Kaufmann V, Bergman MM, Joye D. Motility: mobility as capital. Int J Urban Reg Res. 2004;28:745–56.
Järv O, Muurisepp K, Ahas R, Derudder B, Witlox F. Ethnic differences in activity spaces as a characteristic of segregation: a study based on mobile phone usage in Tallinn, Estonia. Urban Stud. 2015;52:2680–98.
Hägerstrand T. What about people in regional science? Pap Reg Sci Assoc. 1970;24:6–21.
Gee GC, Payne-Sturges DC. Environmental health disparities: a framework integrating psychosocial and environmental concepts. Environ Health Perspect. 2004;112:1645–53.
Pearce JR, Richardson EA, Mitchell RJ, Shortt NK. Environmental justice and health: the implications of the socio-spatial distribution of multiple environmental deprivation for health inequalities in the United Kingdom. Trans Inst Br Geogr. 2010;35:522–39.
Perchoux C, Chaix B, Cummins S, Kestens Y. Conceptualization and measurement of environmental exposure in epidemiology: accounting for activity space related to daily mobility. Health Place. 2013;21:86–93.
Cummins S, Macintyre S. “Food deserts”—evidence and assumption in health policy making. BMJ. 2002;325:436–8.
Wrigley N. “Food Deserts” in British Cities: policy context and research priorities. Urban Stud. 2002;39:2029–40.
Paez A, Mercado RG, Farber S, Morency C, Roorda M. Accessibility to health care facilities in Montreal Island: an application of relative accessibility indicators from the perspective of senior and non-senior residents. Int J Health Geogr. 2010;9:52.
Michimi A, Wimberly MC. Associations of supermarket accessibility with obesity and fruit and vegetable consumption in the conterminous United States. Int J Health Geogr. 2010;9:49.
Neutens T. Accessibility, equity and health care: review and research directions for transport geographers. J Transp Geogr. 2015;43:14–27.
Apparicio P, Cloutier M-S, Shearmur R. The case of Montréal’s missing food deserts: evaluation of accessibility to food supermarkets. Int J Health Geogr. 2007;6:4.
Burns CM, Inglis AD. Measuring food access in Melbourne: access to healthy and fast foods by car, bus and foot in an urban municipality in Melbourne. Health Place. 2007;13:877–85.
Moore LV, Diez Roux AV, Evenson KR, McGinn AP, Brines SJ. Availability of recreational resources in minority and low socioeconomic status areas. Am J Prev Med. 2008;34:16–22.
Pearce J, Hiscock R, Blakely T, Witten K. The contextual effects of neighbourhood access to supermarkets and convenience stores on individual fruit and vegetable consumption. J Epidemiol Community Health. 2008;62:198–201.
Hubley TA. Assessing the proximity of healthy food options and food deserts in a rural area in Maine. Appl Geogr. 2011;31:1224–31.
Breyer B, Voss-Andreae A. Food mirages: geographic and economic barriers to healthful food access in Portland, Oregon. Health Place. 2013;24:131–9.
Walker RE, Keane CR, Burke JG. Disparities and access to healthy food in the United States: a review of food deserts literature. Health Place. 2010;16:876–84.
Lind PL, Jensen PV, Glümer C, Toft U. The association between accessibility of local convenience stores and unhealthy diet. Eur J Public Health. 2016:1–6. doi:10.1093/eurpub/ckv242
Boone-Heinonen J, Gordon-Larsen P, Kiefe CI, Shikany JM, Lewis CE, Popkin BM. Fast food restaurants and food stores: longitudinal associations with diet in young to middle-aged adults: the CARDIA study. Arch Intern Med. 2011;171:1162–70.
An R, Sturm R. School and residential neighborhood food environment and diet among California youth. Am J Prev Med. 2012;42:129–35.
Lee H. The role of local food availability in explaining obesity risk among young school-aged children. Soc Sci Med. 2012;74:1193–203.
Holsten JE. Obesity and the community food environment: a systematic review. Public Health Nutr. 2009;12:397–405.
Widener MJ, Farber S, Neutens T, Horner M. Spatiotemporal accessibility to supermarkets using public transit: an interaction potential approach in Cincinnati, Ohio. J Transp Geogr. 2015;42:72–83.
Cass N, Shove E, Urry J. Social exclusion, mobility and access. Sociol Rev. 2005;53:539–55.
Dalvi MQ, Martin KM. The measurement of accessibility: some preliminary results. Transportation. 1976;5:17–42.
Burgoine T, Alvanides S, Lake AA. Creating “obesogenic realities”; do our methodological choices make a difference when measuring the food environment? Int J Health Geogr. 2013;12:33.
Yeager CD, Gatrell JD. Rural food accessibility: an analysis of travel impedance and the risk of potential grocery closures. Appl Geogr. 2014;53:1–10.
Larsen K, Gilliland J. Mapping the evolution of “food deserts” in a Canadian city: supermarket accessibility in London, Ontario, 1961–2005. Int J Health Geogr. 2008;7:16.
McEntee J, Agyeman J. Towards the development of a GIS method for identifying rural food deserts: geographic access in Vermont, USA. Appl Geogr. 2010;30:165–76.
Luan H, Law J, Quick M. Identifying food deserts and swamps based on relative healthy food access: a spatio-temporal Bayesian approach. Int J Health Geogr. 2015;14:37.
Djurhuus S, Hansen HS, Aadahl M, Glümer C. Individual public transportation accessibility is positively associated with self-reported active commuting. Front Public Heal. 2014;2:240.
Ferguson WJ, Kemp K, Kost G. Using a geographic information system to enhance patient access to point-of-care diagnostics in a limited-resource setting. Int J Health Geogr. 2016;15:10.
Koike S, Matsumoto M, Ide H, Kashima S, Atarashi H, Yasunaga H. The effect of concentrating obstetrics services in fewer hospitals on patient access: a simulation. Int J Health Geogr. 2016;15:4.
Delafontaine M, Neutens T, Schwanen T, Van De Weghe N. The impact of opening hours on the equity of individual space-time accessibility. Comput Environ Urban Syst. 2011;35:276–88.
Kwan M-P. Beyond space (As We Knew It): toward temporally integrated geographies of segregation, health, and accessibility. Ann Assoc Am Geogr. 2013;103:1078–86.
Widener MJ, Shannon J. When are food deserts? Integrating time into research on food accessibility. Health Place. 2014;30:1–3.
Widener MJ, Farber S, Neutens T, Horner MW. Using urban commuting data to calculate a spatiotemporal accessibility measure for food environment studies. Health Place. 2013;21:1–9.
Horner MW, Wood BS. Capturing individuals’ food environments using flexible space-time accessibility measures. Appl Geogr. 2014;51:99–107.
Schönfelder S, Axhausen K. Urban rhythms and travel behaviour. Urban rhythms and travel behaviour. Surrey: Ashgate Publishing Ltd.; 2010.
Järv O, Ahas R, Witlox F. Understanding monthly variability in human activity spaces: a twelve-month study using mobile phone call detail records. Transp Res Part C. 2014;38:122–35.
Tenkanen H, Salonen M, Lattu M, Toivonen T. Seasonal fluctuation of riverine navigation and accessibility in Western Amazonia: an analysis combining a cost-efficient GPS-based observation system and interviews. Appl Geogr. 2015;63:273–82.
Hubers C, Schwanen T, Dijst M. ICT and temporal fragmentation of activities: an analytical framework and initial empiricial findings. Tijdschr voor Econ en Soc Geogr. 2008;99:528–46.
Glorieux I, Mestdag I, Minnen J. The coming of the 24-hour economy? Changing work schedules in Belgium between 1966 and 1999. Time Soc. 2008;17:63–83.
Geiger S. Exploring night-time grocery shopping behaviour. J Retail Consum Serv. 2007;14:24–34.
Farber S, Morang MZ, Widener MJ. Temporal variability in transit-based accessibility to supermarkets. Appl Geogr. 2014;53:149–59.
Neutens T, Delafontaine M, Schwanen T, Van de Weghe N. The relationship between opening hours and accessibility of public service delivery. J Transp Geogr. 2012;25:128–40.
Vignali C, Gomez E, Vignali M, Vranesevic T. The influence of consumer behaviour within the Spanish food retail industry. Br Food J. 2001;103:460–78.
Haraldsson M, Svensson T. Economic evaluation of grocery store nets in cities—a model approach. Linköping: Swedish National Road & Transport Research Institute (VTI); 2007.
Haraldsson M, Svensson T. Car accessibility in inner cities and residential areas-discrete choice analysis of stated preference data. Trafikdage på Aalborg Universitet 2001; 2001.
Martin D, Jordan H, Roderick P. Taking the bus: incorporating public transport timetable data into health care accessibility modelling. Environ Plan A. 2008;40:2510–25.
Ziliaskopoulos AK, Mahmassani HS. A note on least time path computation considering delays and prohibitions for intersection movements. Transp Res Part B Methodol. 1996;30:359–67.
Yiannakoulias N, Bland W, Svenson LW. Estimating the effect of turn penalties and traffic congestion on measuring spatial accessibility to primary health care. Appl Geogr. 2013;39:172–82.
Dewulf B, Neutens T, Vanlommel M, Logghe S, De Maeyer P, Witlox F, De Weerdt Y, Van de Weghe N. Examining commuting patterns using Floating Car Data and circular statistics: exploring the use of new methods and visualizations to study travel times. J Transp Geogr. 2015;48:41–51.
Shoup DC. Cruising for parking. Transp Policy. 2006;13:479–86.
Shaw NT. Geographical information systems and health: current state and future directions. Healthc Inform Res. 2012;18:88–96.
Vetter C, Geisberger R. Experimental algorithms. In: Pardalos PM, Rebennack S, editors. Experimental Algorithms. Lecture Notes in Computer Science, vol. 6630. Berlin: Springer; 2011. p. 100–11.
Kawabata M, Shen Q. Commuting Inequality between cars and public transit: the case of the San Francisco Bay Area, 1990–2000. Urban Stud. 2007;44:1759–80.
Peipins LA, Graham S, Young R, Lewis B, Foster S, Flanagan B, Dent A. Time and distance barriers to mammography facilities in the Atlanta metropolitan area. J Community Health. 2011;36:675–83.
Mavoa S, Witten K, McCreanor T, O’Sullivan D. GIS based destination accessibility via public transit and walking in Auckland, New Zealand. J Transp Geogr. 2012;20:15–22.
Lei TL, Church RL. Mapping transit-based access: integrating GIS, routes and schedules. Int J Geogr Inf Sci. 2010;24:283–304.
Benenson I, Martens K, Rofé Y, Kwartler A. Public transport versus private car GIS-based estimation of accessibility applied to the Tel Aviv metropolitan area. Ann Reg Sci. 2011;47:499–515.
Salonen M, Toivonen T. Modelling travel time in urban networks: comparable measures for private car and public transport. J Transp Geogr. 2013;31:143–53.
Fuller D, Cummins S, Matthews SA. Does transportation mode modify associations between distance to food store, fruit and vegetable consumption, and BMI in low-income neighborhoods? Am J Clin Nutr. 2013;97:167–72.
Djurhuus S, Hansen HS, Aadahl M, Glümer C. The association between access to public transportation and self-reported active commuting. Int J Environ Res Public Health. 2014;11:12632–51.
Richbell S, Kite V. Night shoppers in the “open 24 hours” supermarket: a profile. Int J Retail Distrib Manag. 2007;35:54–68.
European Environment Agency. Urban sprawl in Europe—the ignored challenge. Copenhagen: European Environment Agency; 2006.
Næss P. Residential location affects travel behavior—but how and why? The case of Copenhagen metropolitan area. Prog Plann. 2005;63:167–257.
Buys L, Miller E. Conceptualising convenience: transportation practices and perceptions of inner-urban high density residents in Brisbane, Australia. Transp Policy. 2011;18:289–97.
Salonen M, Broberg A, Kyttä M, Toivonen T. Do suburban residents prefer the fastest or low-carbon travel modes? Combining public participation GIS and multimodal travel time analysis for daily mobility research. Appl Geogr. 2014;53:438–48.
Päivittäistavarakauppa ry. Päivittäistavarakauppa 2013. 2013.
Koistinen K, Vesala T. Päivittäistavarakaupan rakennemuutos Suomen keskeisillä kaupunkiseuduilla 1995–2003. 2006.
LeDoux TF, Vojnovic I. Going outside the neighborhood: the shopping patterns and adaptations of disadvantaged consumers living in the lower eastside neighborhoods of Detroit, Michigan. Health Place. 2013;19:1–14.
Zenk SN, Schulz AJ, Matthews SA, Odoms-Young A, Wilbur J, Wegrzyn L, Gibbs K, Braunschweig C, Stokes C. Activity space environment and dietary and physical activity behaviors: a pilot study. Health Place. 2011;17:1150–61.
Huff DL. A probabilistic analysis of shopping center trade areas. Land Econ. 1963;39:81.
Luo J. Integrating the Huff model and floating catchment area methods to analyze spatial access to healthcare services. Trans GIS. 2014;18:436–48.
Toivonen T, Salonen M, Tenkanen H, Saarsalmi P, Jaakkola T, Järvi J. Joukkoliikenteellä, autolla ja kävellen: avoin saavutettavuusaineisto pääkaupunkiseudulla. Terra (Hels). 2014;126:127–36.
Järvi J, Salonen M, Saarsalmi P, Tenkanen H, Toivonen T. Reititin: an open source tool for analysing accessibility by public transport in Greater Helsinki. In: 3rd open source geospatial research & education symposium OGRS 2014; 2014.
Dijkstra EW. A note on two problems in connexion with graphs. Numer Math. 1959;1:269–71.
Laatikainen T, Tenkanen H, Kyttä M, Toivonen T. Comparing conventional and PPGIS approaches in measuring equality of access to urban aquatic environments. Landsc Urban Plan. 2015;144:22–33.
Di Minin E, Tenkanen H, Toivonen T. Prospects and challenges for social media data in conservation science. Front Environ Sci. 2015;3.
Reeves SL, Newling-Ward E, Gissane C. The effect of shift-work on food intake and eating habits. Nutr Food Sci. 2004;34:216–21.
Zhao I, Turner C. The impact of shift work on people’s daily health habits and adverse health outcomes. Aust J Adv Nurs. 2008;25:8–22.
Authors’ contributions
PS, MS, HT and TT developed the original research idea. HT and PS collected, processed and analyzed the data, and prepared the figures and tables. HT, OJ and PS wrote the manuscript, with contributions from other authors. TT conceived and led the study. All authors read and approved the final manuscript.
Acknowledgements
We thank the Helsinki Metropolitan Region Urban Research Program for supporting the research work. H.T. thanks the DENVI doctoral program at University of Helsinki for support. We wish to thank also our (former) team members Jaani Lahtinen, Sakari Jäppinen, Timo Jaakkola and Juha Järvi for their contributions for our methodological development.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The tools and datasets supporting the conclusions of this article are available from the website of Accessibility Research Group, University of Helsinki, www.helsinki.fi/science/accessibility.
Funding
The work was funded by Helsinki Metropolitan Region Urban Research Program. The work of H.T. was funded by DENVI doctoral program at University of Helsinki.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Tenkanen, H., Saarsalmi, P., Järv, O. et al. Health research needs more comprehensive accessibility measures: integrating time and transport modes from open data. Int J Health Geogr 15, 23 (2016). https://doi.org/10.1186/s12942-016-0052-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12942-016-0052-x