
Abstract
Background
Air pollution can cause various respiratory and neurological diseases and continuous exposure can lead to death. Previous studies have reported that particulate matter (PM) exposure increases the risk of depression, suicidal thoughts, and suicidal death; however, the results are inconsistent and limited. This study aimed to examine the relationship between short-term PM exposure and suicide deaths, as well as investigate the short-term effects of PM on suicide death within vulnerable groups based on factors such as sex, age group, suicide-related information (note, method, and cause), psychiatric disorders, and physical diseases.
Methods
Data on a total of 28,670 suicide deaths from 2013 to 2017, provided by the Korea Foundation for Suicide Prevention, were analyzed. The study design employed a time-series analysis with a two-stage approach. In the first step, a generalized additive model combined with a distributed lag nonlinear model was used to estimate the short-term effect of PM exposure on suicide risk specific to each city. In the second step, the estimated results from each city were pooled through a meta-analysis to derive the overall effect. We determined the effects of single lag, cumulative lag, and moving average PM concentrations from days 0–7 before suicide.
Results
We confirmed an association between exposure to PM10 (≤ 10 μm in diameter) and deaths due to suicide. In particular, among individuals with psychiatric disorders and those who employed non-violent suicide methods, increased exposure to PM10 was associated with a higher risk of death by suicide, with percentage changes of 5.92 (95% confidence interval [CI]: 3.95–7.92) and 11.47 (95% CI: 7.95–15.11), respectively. Furthermore, in the group with psychiatric disorders, there was an observed tendency of increasing suicide risk as PM10 levels increased up to 120 µg/m3, whereas in the group with non-violent suicide deaths, there was a pronounced trend of rapid increase in suicide risk with an increase in PM10 up to 100 µg/m3.
Conclusions
These results show an association between short-term exposure to PM and suicide. Our study adds evidence for the benefits of reducing PM in preventing diseases and improving mental health.
Similar content being viewed by others


Background
Suicide is the leading cause of death worldwide, accounting for over 700,000 deaths annually [1]. In particular, Korea’s suicide mortality rate has been declining since 2011 but is still the highest among OECD countries [2]. Suicide being the number one cause of death for people in their 10s, 20s, and 30s in Korea [3] is a significant problem for society. However, risk factors for suicide require further understanding. Studies have identified several factors associated with suicide risk, including individual-level factors (history of depression or other mental disorders, experience of suicide attempts, physical characteristics, and demographic characteristics), psychological factors, biological factors (genetic, epigenetic, and neurobiological), and environmental factors [4,5,6,7,8,9]. These factors combined can have synergistic effects on suicidal behavior [10], and modifiable or potentially treatable risk factors are important considerations in research. Among these risk factors, air pollution, an environmental factor, is an important risk factor related to adverse health effects. Increased concentrations of air pollutants, particularly particulate matter (PM), have consistently been associated with increased respiratory and cardiovascular mortality and morbidity worldwide [11]. Recently, it has been hypothesized that air pollution can also induce self-aggressive behavior by increasing the levels of cytokines and reactive oxygen species [12], and that short- and long-term exposure to air pollution increases the risk of mental health-related diseases [13,14,15]. In addition, with increasing PM exposure, hospitalization and emergency room visits due to mental illness have increased [16, 17]. Furthermore, several studies have reported an association between PM exposure and suicide-related deaths [18,19,20,21], and the varying diameters of PM affect suicide risk differently [19, 20, 22]. The neurotoxic effects of air pollution can be particularly dangerous to vulnerable populations such as people with mental illnesses. In patients with major depressive disorder, a high-risk group for suicide, there was an association between short-term exposure to PM and suicide, and a clear dose-response relationship between short-term exposure to PM and suicide-related death was confirmed [23]. Furthermore, an association has been reported between long-term PM exposure and suicide in patients with physical or mental diseases, and a dose-response relationship has been confirmed [24]. Several studies have identified an association between PM and suicide stratified by sex and age group. Compared to men, the association between PM and suicide was stronger in women [16, 23]. Although no significant association in individuals aged 20–39 years was found, in those aged 40 years or older, the suicide risk tended to increase when both particulate matter ≤ 10 μm in diameter (PM10) and particulate matter ≤ 2.5 μm in diameter (PM2.5) concentrations increased [23]. However, these relationships vary across studies, and the evidence supporting the association between PM and suicide is limited. Considering the analysis in various stratified groups, it is necessary to identify the groups vulnerable to the effects of PM. Our research team conducted a study of the association between PM and suicide deaths in 2010, and we would like to report our latest findings. Therefore, this study aimed to: (1) investigate the relationship between short-term exposure to PM and suicide death and (2) investigate the short-term effects of PM on suicide in vulnerable groups based on factors including sex, age group, suicide note, psychiatric disorder, physical disease, main suicide method, and main suicide cause.
Methods
Data source and study population
The data on suicide deaths in South Korea from January 1, 2013 to December 31, 2017 were obtained from the Korea Foundation for Suicide Prevention. The data were collected by reviewing official police investigation records. The data included personal information about suicide deaths (such as resident registration number, age, and sex), location of discovery, and method and main cause [25].
In this study, complete enumeration data of suicide-related deaths were used. In these data, suicide death was defined as cases falling in the category of intentional self-harm (X60-X84) of the 10th Amendment of the International Classification of Diseases and Related Health Issues (ICD-10). The study population included suicide-related deaths in Seoul, Gyeonggi, and Incheon, metropolitan areas in South Korea. The total number of subjects was 28,670. For the analysis, the index date was defined as the date of suicide death or the date of discovery. If the date of death was earlier than the date of discovery, the index date was defined as the date of death; if the date of death was later than the date of discovery (died after discovery), the index date was defined as the date of discovery. The index place was the place of discovery and was divided into 66 cities and districts. The number of suicide deaths was calculated based on dates and cities/district, and it was used in conjunction with environmental data for analysis. This study was approved by the Institutional Review Board of Yonsei University Wonju College of Medicine, Republic of Korea (CR320301). Data were anonymized using a randomly generated number, and no personally identifiable information of the suicide was included in the study.
Air pollution and meteorological data (environmental data)
The Korea Environment Corporation AirKorea provides hourly average concentration data of air pollution levels for sulfur dioxide (SO2), carbon monoxide (CO), nitrogen dioxide (NO2), ozone (O3), PM10, and PM2.5 collected by 614 measurement stations in 162 cities. We obtained SO2, CO, NO2, O3, and PM10 data for the period 2013–2017 measured at 160 measurement stations in Seoul, Gyeonggi, and Incheon, and PM2.5 data for the period 2015–2017. Air pollution data were provided as 1-h concentrations and converted into 24-h average concentrations for analysis. Meteorological data on temperature, humidity, sunlight, and air pressure at the city level, were obtained from the Korea Meteorological Administration. The data provided were in hourly units, but we converted them to 24-h average concentrations for analysis.
Stratification variables
The stratification variables considered in the study were sex (men/women), age (19–40, 41–64, or > 65 years), suicide notes (presence or absence), psychiatric disorders (with or without), physical disease (with or without), main suicide method (violent or non-violent), and main suicide cause (economic, sociological, or health problem). Physical diseases were determined using statements and medical certificates provided by the bereaved family as documented in the police investigation records and claims data from the National Health Insurance Service. The presence or absence of psychiatric disorders was established by the data investigator. Consequently, if it was not assessed, it was not recorded, resulting in numerous missing values for this variable. The same applies to variables related to physical diseases. Methods of suicide were documented as the main suicide methods. When two or more suicide methods were used, they were recorded in consideration of being registered as the direct cause of death in the investigation record. If there were more than two direct causes of death, they were recorded based on criticality. Violent methods included hanging, jumping from a height, jumping in front of a car or train, cutting and piercing with sharp objects, using firearms or shotguns, and self-immolation. Non-violent methods included ingestion of pesticides, drug overdose, gas poisoning, and suffocation [26]. In addition, the main cause of suicide was recorded as the factor that caused severe pain to the person who committed suicide and had the strongest influence on suicide among the stress factors that lasted until death by reviewing the investigation records. The cause of suicide was classified into occupational problems, economic problems, family problems, interpersonal problems, physical health problems, mental health problems, and other causes. The other causes included academic, political, religious, and unknown problems. For our analysis, we categorized main suicide causes into two groups: socio-economic problems (combining occupational, economic, family, and interpersonal problems) and health problems (combining physical and mental health problems). Finally, as a warning sign, we considered any sign that indicated a suicidal individual’s thoughts or intentions regarding suicide, manifested through linguistic, behavioral, or emotional expressions prior to the suicide. Language signs included directly conveying words suggesting death to the people around the person, primarily family members, or frequently bringing up stories related to suicide. Behavioral signs included a loss of interest in appearance, self-harm behaviors, or cleaning up their surroundings, such as their bank account and home. Emotional signs encompassed changes in emotional states such as guilt, sadness, or emotional distress. While warning signs are closely related to suicide, they were not included as stratification variables and are only presented in Table 1 as baseline characteristics.
Statistical analysis
The association between PM exposure and suicide was investigated using a time-series analysis design. A two-stage analysis was conducted in this study. The first step estimated the city-specific effect using a generalized additive model combined with a distributed lag nonlinear model to estimate the short-term effect of PM exposure on suicide risk. Daily suicide deaths were used as the dependent variable, PM was used as the independent variable, and a quasi-Poisson model was applied to adjust for overdispersion. Daily weather data such as temperature, relative humidity, air pressure, and sunlight, time trends, and holidays were considered as covariates. The time-series analysis model was as follows:
where \(E\left({Y}_{t}\right)\) is the number of suicide deaths on day \(t\), \(\alpha\) is the model intercept, \(\beta\) indicates the log-relative risk of suicide associated with an interquartile range (IQR) increase in the PM level, and \(ns\left( \right)\) represents the natural cubic spline function. To remove the seasonal trend of time-series data, seven degrees of freedom per year were used for time, the smooth function of a natural cubic spline with six degrees of freedom was used for temperature, and the smooth function of a natural cubic spline with three degrees of freedom was used for relative humidity, sunlight, and air pressure. The IQR was calculated as the difference between the third and first quartile each for PM10 and PM2.5 during the study period. In the second stage, a meta-analysis was performed using a fixed and random effects model after confirming heterogeneity to estimate the overall effect using the estimated values from the city-specific model in the first stage.
The effect of PM exposure on suicide was evaluated as a single lag and a moving average lag effect. The single lag effect confirmed the air pollution exposure effect from the day of suicide to 7 days before the day of suicide, and the moving average effect was estimated as the moving average up to 1, 3, 5, and 7 days prior to the day of suicide. The effect was expressed as the percentage change (95% confidence interval [CI]) in the association between the increased IQR of PM and the risk of suicide.
Additionally, subgroup analysis was conducted for stratification variables using a moving average lag 03 model. The percent change (95% CI) in suicide risk was assessed for each IQR increase in PM. Furthermore, the exposure-response curves were plotted to confirm the association between PM exposure and suicide risk [27]. To compare relative risks between subgroups, we conducted Z-tests. For sensitivity analysis, the concentration of air pollutants other than PM was adjusted, and the association between PM and suicide-related deaths was confirmed through a two-pollution model. In addition, because PM and suicide data exhibit seasonality, a seasonal stratification analysis was conducted. All analyses were reported based on the pooled estimates from a meta-analysis, combining data from 66 cities and districts. A two-sided P-value < 0.05 was considered statistically significant and the analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), R studio, and R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
Table 1 shows the general characteristics of the suicide-related deaths. From 2013 to 2017, the number of suicide-related deaths in Seoul, Gyeonggi, and Incheon was 28,670, with an average age of 52 years; 69% of the suicide victims were male. Violent methods accounted for 77% of the suicide methods, and mental health and economic problems were the most common causes of suicide. Most deaths due to suicide had prior warning signs.
Air pollution and meteorological data
The distributions of the average PM concentrations and meteorological data during the study period are shown in Table 2. The average concentrations were 50.736 µg/m³ for PM10 and 26.011 µg/m³ for PM2.5, with IQRs of 29.12 µg/m³ and 16.68 µg/m³, respectively. The average concentrations of other air pollutants were 0.005 ppm for SO2, 0.552 ppm for CO, 0.024 ppm for O3, and 0.030 ppm for NO2 (Supplementary Table 1, see Additional file 1). The daily average temperature was 12.9 ℃, the relative humidity was 66%, the duration of sunshine was 0.51 h, and the air pressure was 1009.89 hPa. Supplementary Table 2 (see Additional file 1) shows the correlations between air pollution and meteorological data. The relationships differed between substances, but there were significant positive correlations between each air pollutant. The correlation between PM10 and PM2.5 was the highest.
Association between suicide-related death and PM
Table 3 shows the association between PM exposure and suicide among all the subjects. The results confirmed that the suicide risk increased by 2.9% when the IQR of PM10 in lag increased, but there were no significant associations at other single lags. An association was found between increased PM10 and suicide risk in all moving averages. However, there was no statistically significant association between suicide and PM2.5.
Figure 1 shows the association between PM exposure and suicide in stratified subgroups (lag 03). The association between PM10 and suicide was statistically significant in almost all the subgroups. The risk of suicide increased by 6.45% (95% CI: 4.15–8.81) in males and 5.74% (95% CI: 2.17–9.43) in females, as well as by 6.07% (95% CI: 2.71–9.55) in those aged 19–40 years, 7.10% (95% CI: 3.94–10.35) in those aged 41–64 years, and 6.16% (95% CI: 2.72–9.72) in those aged over 65 years. Regarding factors related to suicide, the risk ratio was similar regardless of the presence or absence of a suicide note, and the risk of suicide stratified by the main suicide cause was 6.62% (95% CI: 4.29–9.00) for health problems and 4.92% (95% CI: 2.32–7.58) for socio-economic problems. Although the risk of suicide was higher for the group with health problems than for that with socio-economic problems, this difference was not statistically significant. Depending on the suicide method, the association between PM10 and suicide deaths was stronger for suicides using non-violent methods (4.25%, 95% CI: 2.15–6.40) than for suicides using violent methods (11.47%, 95% CI: 7.95–15.11). Notably, this was the only subgroup analysis with a significant difference (P = 0.001). Additionally, the risk of suicide was similar according to the presence or absence of physical problems. In the absence of psychiatric disorders, the association between PM10 and suicide deaths was not statistically significant, whereas the risk of suicide increased by 5.92% (95% CI: 3.95–7.92) if psychiatric disorders were present. However, the risk was not significantly different between these two groups. In contrast, for PM2.5, the association with suicide risk was not statistically significant. In Fig. 2, the association between PM10 (lag 03) and the risk of suicide in each subgroup is shown as an exposure–response curve. In the group with mental disorders, the risk of suicide tended to increase with an increase in PM10 up to 120 µg/m³, and in the non-violent suicide-related death group, the risk of suicide increased rapidly with an increase in PM10 up to 10 µg/m³.

Association between the risk of suicide death and PM (lag 03) per IQR increase by stratified subgroup. *Data are presented as percentage changes (%) with 95% confidence intervals. The model included temperature, relative humidity, air pressure, sunlight, calendar time, and holidays as adjustment variables. IQR, interquartile range; PM, particulate matter

Exposure-response curve for the association between risk of suicide death and PM10 (lag 03) by stratified subgroup. *Data are presented as relative risk with 95% confidence intervals. The model included temperature, relative humidity, air pressure, sunlight, calendar time, and holidays as adjustment variables. PM, particulate matter
Sensitivity analysis
After adjusting for air pollutants other than PM, the association between moving average day 3 of PM and suicide-related deaths was confirmed, as shown in Table 4. After adjusting for other air pollutants, we confirmed a statistically significant association between increased PM10 and suicide. After adjusting for CO, which had the highest correlation with PM10, an increase in the IQR of PM10 increased the suicide risk by 9.28% (95% CI: 6.17–12.50). Even after adjusting for SO2, O3, and NO2, the risk of suicide increased by 6.16% (95% CI: 3.60–8.78), 6.58% (95% CI: 4.09–9.14), and 7.32% (95% CI: 4.80–9.91), respectively. In contrast, even after adjusting for other air pollutants, there was no statistically significant association between PM2.5 and suicide risk.
Seasonal stratification analysis results are presented in Supplementary Table 3 (see Additional file 1). In spring, when PM exposure was the highest, the association between increased PM10 and suicide risk was the greatest, but there was no association between increased PM2.5 and suicide risk.
Discussion
This study investigated the association between short-term exposure to PM and suicide-related deaths in 28,670 people who died by suicide in large cities in Korea. The analysis results showed that the risk of suicide-related death increased with short-term exposure to PM10, and this short-term effect of PM10 was consistent and robust even after adjusting for other air pollutants. Subgroup analysis confirmed an association between PM10 exposure and suicide in all groups except subjects without psychiatric disorders. However, no association was found between exposure to PM2.5 and suicide.
Several studies have reported an association between short-term PM exposure and suicide. In a study similar to our study, that examined the association between air pollution and suicide deaths in 10 cities in Northeast Asia, the association between PM10 and suicide death was confirmed, while PM2.5 was not associated with suicide death [20]. Lin et al. reported an association between short-term exposure to PM10 and suicide in a group of suicide victims in Guangzhou, China [21]. In addition, in a previous study conducted by this research team in 2010, it was reported that the risk of suicide increased by 9.0% and 10.1% when the IQR of PM10 and PM2.5 increased, respectively [18]. However, several studies have reported results that contradict our findings [17, 19, 22].
It is well known that exposure to air pollution can activate cytokines that trigger the body’s inflammatory response, thus increasing the systemic inflammatory response and oxidative stress [28, 29]. Experimental studies have shown that long-term exposure to air pollution can lead to neuroinflammation and oxidative stress, leading to brain pathologies that increase the risk of developing depression [30, 31]. In addition, heavy metals, such as lead and mercury, contained in PM can affect the central nervous system and cause depression or suicidal thoughts. Thus, short-term changes in air pollution can cause significant changes in health status based on changes previously induced by long-term exposure to air pollution. Suicide can be influenced by a combination of factors and requires risk management in vulnerable populations.
Subgroup analyses were conducted in stratified groups by sex, age group, suicide notes, psychiatric disorders, physical disease, main suicide method, and main suicide cause and compared the risk of PM and suicide within subgroups. As a result, statistically significant difference was found only in the main suicide method, indicating that individuals who attempt suicide using non-violent methods are more affected by PM10 exposure compared to those who attempt suicide through violent methods. However, no significant differences were observed in other subgroups. In contrast to our findings, Lin et al. reported that PM exposure affects suicide risk only in groups that attempted suicide by violent methods, based on the fact that seasonal changes were significantly correlated with violent suicide-related deaths but not with non-violent suicide-related deaths [21, 32]. However, Sun et al. reported the presence of seasonality among non-violent suicide cases [33]. A psychological autopsy study comparing violent and non-violent suicides among elderly individuals in rural China found that non-violent suicide cases had higher levels of depression compared to violent suicide cases and emphasized that depression and hopelessness were independent risk factors for non-violent suicide [26]. Considering that depression and hopelessness are risk factors for suicidal ideation and death [34], it is possible that non-violent suicide cases may be more vulnerable to environmental factors such as PM.
PM10 and suicide-related deaths were not associated in individuals without psychiatric disorders, but our data confirmed an increased risk of suicide in individuals with psychiatric disorders when the IQR of PM10 was increased. Patients who visited the hospital for depression may have had preexisting depressive symptoms, and short-term changes in air pollution may trigger severe depressive symptoms in patients with prior moderate disease manifestation. As PM is expected to affect suicide-related deaths more sensitively in patients with mental illnesses, it is necessary to recommend the prevention of PM exposure in such patients.
Similar to our study, Kim et al. [20] reported no clear pattern in effect modification by sex and age. However, some studies [18, 19] have shown that PM has a stronger impact on suicide in men, while other studies [23, 35] have reported a more significant effect on women. For men, PM exposure may increase due to increased outdoor activities, and for women, PM exposure may be related to the inflammatory effects of estrogen and the immunosuppressive effect of androgens [23]. The effects of PM exposure according to age groups were reported diversely, and the range of age groups was extensive [18, 21, 23, 36,37,38]. In the study by Casas et al. [39], which tested for effect modification, the effect of PM10 on suicide was only confirmed in extreme age groups - children (5–14 years) and the elderly (over 85 years), showing significant p for interaction. However, in our study, a subgroup analysis for patients under 18 years was not conducted due to a small number of cases, so the results for extreme age could not be confirmed. Lin et al. [21] have suggested that younger people are more likely to work outdoors, increasing their exposure to air pollution. Since our study focused on the metropolitan area, there might have been less variation in occupational differences between age groups compared to other regions, which could have resulted in no differences in the PM effect across age groups.
Furthermore, we have not found suicide causes, physical disease, and suicide note as effect modifiers. Individuals with socio-economic problems may have an increased risk of suicide due to the stress and psychological pressure resulting from these issues and may not have received appropriate treatment for mental health problems or depression due to economic problems. People with physical problems may experience inherent stress and depression, and those already suffering from health problems could be more vulnerable to environmental factors. In addition, previous studies [18, 23] have reported a PM effect on suicide among subjects with physical diseases, with most of these studies assessing the impact based on the type of illness (e.g., cardiovascular disease, cancer, depression, etc.). However, we analyzed using only the presence or absence of physical illnesses, which might explain why the differences were not as clear. Considering factors such as the type of illness, its severity, and management status would be necessary to establish a clear relationship. There are very few studies that have examined the impact of PM exposure by the presence or absence of a suicide note. In studies comparing people who wrote suicide notes to those who didn’t, it was reported that those who left notes often had issues like intimate partner problems, as well as financial difficulties or illnesses [40]. It is speculated that the relatively minor impact of PM exposure may not have been pronounced due to the complex interplay of various factors that can already influence the risk of suicide.
The strength of this study is that it included subgroups based on various suicide-related factors. The results of the subgroup analysis can provide insights into vulnerable populations and have implications for research and public health management. As the data used in this study were collected based on official police investigation records of suicide victims, it was possible to investigate data closely related to suicide. In addition, we were able to study the relationship between PM exposure and suicide-related death using information on the cause of the suicide and through interviews with bereaved families and in-depth analysis of the progression of suicidal behavior. These research findings can serve as a basis for identifying vulnerable populations and developing suicide prevention strategies within various subgroups by examining the relationship between PM and suicide. Furthermore, we analyzed the concentration of PM based on the smallest unit area centered on metropolitan areas. According to data from the Korea Psychological Autopsy Center, there is a large difference in the number of suicide-related deaths and the average suicide rate by city, county, and district in Korea [25]. In addition, even if the physical distance is small, the PM concentration varies greatly from region to region owing to differences in geographic characteristics. Air pollution monitoring stations are limited, and their analyses may not be sufficient for analyzing the long-term effects of PM, especially due to changes in administrative districts and monitoring stations in the past. Therefore, we conducted a study based on metropolitan areas where PM was consistently measured and used PM exposure information by region divided into fine units. In particular, we attempted to quantify PM exposure by considering each individual’s actual residence and suicide attempt area. Finally, a time-series analysis design was used in this study. We expected that a time-series analysis design, rather than a case-crossover analysis design, would provide more reliable outcomes because the residuals have less autocorrelation [41, 42].
Our study had several limitations. First, suicide cases may have been underestimated because only those who died after a suicide attempt were included, and not those who did not die. Second, in Korea, PM2.5 data have been recorded since 2015; therefore, only data from a total of 3 years could be used, which may not include enough cases. Third, the number of deaths by suicide was low compared with other disease studies. This may be the reason for the lack of a significant association in the sub-analysis. In previous studies investigating the relationship between PM and mental health outcomes, researchers have included data spanning more than 5 years for mental health-related outcomes, aiming to overcome these limitations [17, 19, 35, 43]. The limited number of cases may result in a lower level of confidence in the research findings. However, the low incidence of suicide deaths is an unavoidable restriction of our study. Fourth, a subgroup analysis of patients younger than 18 years of age was not performed because of the small number of cases. As the brain and respiratory system are still developing in children and teenagers, they are considered more vulnerable to air pollution, and future studies should focus on individuals in this age group [16]. Fifth, various variables considered in this study have a relatively high proportion of missing data. Particularly, data on physical and mental diseases are missing in 28.2% and 42.6% of cases, respectively. Despite the potential for decreased reliability, the presence of physical illnesses and psychiatric disorders is crucial for assessing suicide risk. Therefore, these factors could not be excluded from the analysis, as they play a vital role in understanding the risk. However, for a generalization of our results, further extensive research with a larger dataset is required. Finally, only the presence or absence of mental diseases was considered, although the aggravation of mental diseases is known to increase the risk of suicide, and there are many stages of mental diseases. To evaluate the increased vulnerability due to PM exposure, it will be necessary to specifically evaluate the impact on mental health, as well as physical diseases.
It is difficult to define the characteristics of a suicidal person because suicide can be induced by a combination of various factors. Although there are known important risk factors, the complexity increases when combined with various individual characteristics; furthermore, various types of suicide exist, making it difficult to isolate the contribution of PM exposure. Performing stratification analysis in environmental epidemiology allows us to analyze these complex factors separately.
In conclusion, we investigated the effects of PM exposure on suicide-related deaths using stratified analysis. Previous studies have demonstrated that air pollution can increase the risk of mental disorders. Our research findings also show an association between PM10 and suicide, and we have confirmed that this impact varies across subgroups. It suggests that PM needs to be carefully managed in vulnerable groups, and as most suicide victims show warning signs before death, sufficient management is considered essential for high-risk groups. Despite several limitations, we elucidated the association between PM and suicide deaths in various subgroups. We hope that our findings can serve as compelling evidence for disease prevention and improvements in mental well-being through the reduction of air pollution.
Data Availability
The data are not publicly available but will be provided upon request with the permission of the Korea Foundation for Suicide Prevention.
Abbreviations
- SO2 :
-
Sulfur dioxide
- CO:
-
Carbon monoxide
- O3 :
-
Ozone
- NO2 :
-
Nitrogen dioxide
- PM:
-
Particulate matter
- PM10 :
-
Particulate matter ≤ 10 μm in diameter
- PM2.5, :
-
Particulate matter ≤ 2.5 μm in diameter
- IQR:
-
Interquartile range
- CI:
-
Confidence interval
References
WHO. : Suicide worldwide in 2019: Global Health Estimates https://apps.who.int/iris/bitstream/handle/10665/341728/9789240026643-eng.pdf (2021). Accessed 9 Dec 2022.
OECD. : Health Status: Causes of mortality (Intentional self-harm) https://stats.oecd.org (2022). Accessed 9 Dec 2022.
Statistics Korea: Causes of Death Statistics in 2021 https://kostat.go.kr/boardDownload.es?bid=11773&list_no=421206&seq=1. (2022). Accessed 9 Dec 2022.
Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to family history of completed Suicide and psychiatric disorders: a nested case-control study based on longitudinal registers. Lancet. 2002;360(9340):1126–30. https://doi.org/10.1016/s0140-6736(02)11197-4.
Cornelius SL, Berry T, Goodrich AJ, Shiner B, Riblet NB. The effect of meteorological, pollution, and geographic exposures on death by Suicide: a scoping review. Int J Environ Res Public Health. 2021;18(15):7809.
Fazel S, Runeson B, Suicide. N Engl J Med. 2020;382(3):266–74. https://doi.org/10.1056/NEJMra1902944.
Hawton K, van Heeringen K, Suicide. Lancet. 2009;373(9672):1372–81. https://doi.org/10.1016/S0140-6736(09)60372-X.
Turecki G, Brent DA, Gunnell D, O’Connor RC, Oquendo MA, Pirkis J, et al. Suicide and Suicide risk. Nat Rev Dis Primers. 2019;5(1):74. https://doi.org/10.1038/s41572-019-0121-0.
van Heeringen K, Mann JJ. The neurobiology of Suicide. Lancet Psychiatry. 2014;1(1):63–72. https://doi.org/10.1016/s2215-0366(14)70220-2.
Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Suicide and suicidal behavior. Epidemiol Rev. 2008;30(1):133–54. https://doi.org/10.1093/epirev/mxn002.
Brunekreef B, Holgate ST. Air pollution and health. Lancet. 2002;360(9341):1233–42. https://doi.org/10.1016/s0140-6736(02)11274-8.
Jayaraj RL, Rodriguez EA, Wang Y, Block ML. Outdoor ambient air pollution and neurodegenerative Diseases: the neuroinflammation hypothesis. Curr Environ Health Rep. 2017;4(2):166–79. https://doi.org/10.1007/s40572-017-0142-3.
Andersen ZJ, Zhang J, Jørgensen JT, Samoli E, Liu S, Chen J, et al. Long-term exposure to air pollution and mortality from Dementia, psychiatric disorders, and Suicide in a large pooled European cohort: ELAPSE study. Environ Int. 2022;170:107581. https://doi.org/10.1016/j.envint.2022.107581.
Yoo E-H, Roberts JE, Eum Y, Li X, Chu L, Wang P, et al. Short-term exposure to air pollution and mental disorders: a case-crossover study in New York City. Environ Research: Health. 2023;1(1):015001. https://doi.org/10.1088/2752-5309/ac6439.
Kim SY, Bang M, Wee JH, Min C, Yoo DM, Han SM, et al. Short- and long-term exposure to air pollution and lack of sunlight are associated with an increased risk of depression: a nested case-control study using meteorological data and national sample cohort data. Sci Total Environ. 2021;757:143960. https://doi.org/10.1016/j.scitotenv.2020.143960.
Gu X, Guo T, Si Y, Wang J, Zhang W, Deng F, et al. Association between ambient air pollution and daily hospital admissions for depression in 75 Chinese cities. Am J Psychiatry. 2020;177(8):735–43. https://doi.org/10.1176/appi.ajp.2020.19070748.
Liu JJ, Wang F, Liu H, Wei YB, Li H, Yue J, et al. Ambient fine particulate matter is associated with increased emergency ambulance dispatches for psychiatric emergencies. Environ Res. 2019;177:108611. https://doi.org/10.1016/j.envres.2019.108611.
Kim C, Jung SH, Kang DR, Kim HC, Moon KT, Hur NW, et al. Ambient particulate matter as a risk factor for Suicide. Am J Psychiatry. 2010;167(9):1100–7. https://doi.org/10.1176/appi.ajp.2010.09050706.
Bakian AV, Huber RS, Coon H, Gray D, Wilson P, McMahon WM, et al. Acute air pollution exposure and risk of Suicide completion. Am J Epidemiol. 2015;181(5):295–303. https://doi.org/10.1093/aje/kwu341.
Kim Y, Ng CFS, Chung Y, Kim H, Honda Y, Guo YL, et al. Air pollution and Suicide in 10 cities in Northeast Asia: a time-stratified case-crossover analysis. Environ Health Perspect. 2018;126(3):037002. https://doi.org/10.1289/ehp2223.
Lin G-Z, Li L, Song Y-F, Zhou Y-X, Shen S-Q, Ou C-Q. The impact of ambient air pollution on Suicide mortality: a case-crossover study in Guangzhou, China. Environ Health. 2016;15(1):90. https://doi.org/10.1186/s12940-016-0177-1.
Astudillo-García CI, Rodríguez-Villamizar LA, Cortez-Lugo M, Cruz-De la Cruz JC, Fernández-Niño JA. Air pollution and Suicide in Mexico City: a time series analysis, 2000–2016. Int J Environ Res Public Health. 2019;16(16):2971. https://doi.org/10.3390/ijerph16162971.
Hwang IY, Choi D, Kim JA, Choi S, Chang J, Goo AJ, et al. Association of short-term particulate matter exposure with Suicide death among major depressive disorder patients: a time-stratified case-crossover analysis. Sci Rep. 2022;12(1):8471. https://doi.org/10.1038/s41598-022-12421-z.
Min JY, Kim HJ, Min KB. Long-term exposure to air pollution and the risk of Suicide death: a population-based cohort study. Sci Total Environ. 2018;628–629:573–9. https://doi.org/10.1016/j.scitotenv.2018.02.011.
Na EJ, Choi J, Kim D, Kwon H, Lee Y, Lee G, et al. Design and methods of the Korean national investigations of 70,000 Suicide victims through police records (the KNIGHTS Study). Psychiatry Investig. 2019;16(10):777–88. https://doi.org/10.30773/pi.2019.07.14.
Zhu RT, Ma ZY, Jia CX, Zhou L. Completed Suicide with violent and non-violent methods by the elderly in rural China: a psychological autopsy study. Front Psychiatry. 2021;12:624398. https://doi.org/10.3389/fpsyt.2021.624398.
Gasparrini A, Armstrong B. Reducing and meta-analysing estimates from distributed lag non-linear models. BMC Med Res Methodol. 2013;13(1):1. https://doi.org/10.1186/1471-2288-13-1.
Bai N, Khazaei M, van Eeden SF, Laher I. The pharmacology of particulate matter air pollution-induced cardiovascular dysfunction. Pharmacol Ther. 2007;113(1):16–29. https://doi.org/10.1016/j.pharmthera.2006.06.005.
Riedl M, Diaz-Sanchez D. Biology of diesel exhaust effects on respiratory function. J Allergy Clin Immunol. 2005;115(2):221–8. https://doi.org/10.1016/j.jaci.2004.11.047. quiz 9.
Fonken LK, Xu X, Weil ZM, Chen G, Sun Q, Rajagopalan S, et al. Air pollution impairs cognition, provokes depressive-like behaviors and alters hippocampal cytokine expression and morphology. Mol Psychiatry. 2011;16(10):987–95. https://doi.org/10.1038/mp.2011.76.
Davis DA, Bortolato M, Godar SC, Sander TK, Iwata N, Pakbin P, et al. Prenatal exposure to urban air nanoparticles in mice causes altered neuronal differentiation and depression-like responses. PLoS ONE. 2013;8(5):e64128. https://doi.org/10.1371/journal.pone.0064128.
Lin HC, Chen CS, Xirasagar S, Lee HC. Seasonality and climatic associations with violent and nonviolent Suicide: a population-based study. Neuropsychobiology. 2008;57(1–2):32–7. https://doi.org/10.1159/000129664.
Sun J, Guo X, Ma J, Zhang J, Jia C, Xu A. Seasonality of Suicide in Shandong China, 1991–2009: associations with gender, age, area and methods of Suicide. J Affect Disord. 2011;135(1):258–66. https://doi.org/10.1016/j.jad.2011.08.008.
Ribeiro JD, Huang X, Fox KR, Franklin JC. Depression and hopelessness as risk factors for Suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psychiatry. 2018;212(5):279–86. https://doi.org/10.1192/bjp.2018.27.
Villeneuve PJ, Huynh D, Lavigne É, Colman I, Anisman H, Peters C, et al. Daily changes in ambient air pollution concentrations and temperature and Suicide mortality in Canada: findings from a national time-stratified case-crossover study. Environ Res. 2023;223:115477. https://doi.org/10.1016/j.envres.2023.115477.
Ng CFS, Stickley A, Konishi S, Watanabe C. Ambient air pollution and Suicide in Tokyo, 2001–2011. J Affect Disord. 2016;201:194–202. https://doi.org/10.1016/j.jad.2016.05.006.
Lee H, Myung W, Kim SE, Kim DK, Kim H. Ambient air pollution and completed Suicide in 26 South Korean cities: effect modification by demographic and socioeconomic factors. Sci Total Environ. 2018;639:944–51. https://doi.org/10.1016/j.scitotenv.2018.05.210.
Braithwaite I, Zhang S, Kirkbride JB, Osborn DPJ, Hayes JF. Air Pollution (Particulate Matter) exposure and associations with Depression, anxiety, bipolar, psychosis and Suicide risk: a systematic review and Meta-analysis. Environ Health Perspect. 2019;127(12):126002. https://doi.org/10.1289/ehp4595.
Casas L, Cox B, Bauwelinck M, Nemery B, Deboosere P, Nawrot TS. Does air pollution trigger Suicide? A case-crossover analysis of Suicide deaths over the life span. Eur J Epidemiol. 2017;32(11):973–81. https://doi.org/10.1007/s10654-017-0273-8.
Lang A, Brieger P, Menzel S, Hamann J. Differences between Suicide note leavers and other suicides: a German psychological autopsy study. J Psychiatr Res. 2021;137:173–7. https://doi.org/10.1016/j.jpsychires.2021.02.049.
Guo Y, Barnett AG, Zhang Y, Tong S, Yu W, Pan X. The short-term effect of air pollution on cardiovascular mortality in Tianjin, China: comparison of time series and case–crossover analyses. Sci Total Environ. 2010;409(2):300–6. https://doi.org/10.1016/j.scitotenv.2010.10.013.
Ren M, Li N, Wang Z, Liu Y, Chen X, Chu Y, et al. The short-term effects of air pollutants on Respiratory Disease mortality in Wuhan, China: comparison of time-series and case-crossover analyses. Sci Rep. 2017;7:40482. https://doi.org/10.1038/srep40482.
Nguyen A-M, Malig BJ, Basu R. The association between ozone and fine particles and mental health-related emergency department visits in California, 2005–2013. PLoS ONE. 2021;16(4):e0249675. https://doi.org/10.1371/journal.pone.0249675.
Acknowledgements
This study used the part of complete survey statistics data provided by the Korea Foundation for Suicide Prevention (2-PSYAUTO-2004-012). Also, this study was supported by the Korea Disease Control and Prevention Agency (2020ER670700).
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
TH Go designed the study, performed statistical analyses, and drafted the manuscript. MH Kim interpreted the results and drafted the manuscript. YY Choi conducted the literature review and contributed to the paper preparation. JH Han conducted the literature review and curated the database. CS Kim designed the study. DR Kang drafted and revised the manuscript. All authors contributed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Yonsei University Wonju College of Medicine, Republic of Korea (CR320301).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
12940_2023_1042_MOESM1_ESM.docx
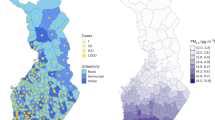
Additional file 1: Fig. 1. PM10, PM2.5 concentrations and Trend in Suicide Death in South Korea from 2013 to 2017. Table (1) Distributions of SO2, CO, O3, and NO2 concentrations in three Korean cities from 2013 to 2017. Table (2) Spearman’s coefficient of meteorological factors and air pollutants. Table (3) Association between the risk of suicide death and PM (lag 03) per interquartile range (IQR) increase by season.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Go, TH., Kim, MH., Choi, YY. et al. The short-term effect of ambient particulate matter on suicide death. Environ Health 23, 3 (2024). https://doi.org/10.1186/s12940-023-01042-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-023-01042-2