
Abstract
Introduction
Reduction in health inequalities and providing universal access to health care have been identified as two important global milestones by the World Health Organization for countries to achieve by 2030. Therefore, recognizing the magnitude of oral health inequalities in India has become a pressing priority to improve access to dental care within the country. This scoping review was conducted with the aim of reviewing, collating and analysing the current knowledge base on oral health inequalities in India.
Methodology
The scoping review followed Arksey and O’Malley’s approach, and reporting was performed in accordance with the PRISMA-ScR guidelines. A systematic search was conducted on Scopus, PubMed, Web of Science, and EMBASE to identify literature addressing one or more dimensions of oral health inequalities in India, published in English between January 2002 and April 2022. The data were charted, and qualitative analysis was performed to derive themes, highlighting the key concepts emerging from this review.
Results
In accordance with the eligibility criteria, a total of 71 articles retrieved through database search and backward citation search were included in this scoping review. The major themes ranged from individual to diverse sociodemographic factors acting as barriers to and facilitators of access to dental care. Deficiencies in human resources for oral health, along with a wide diversity in dental service provision and dental education were other major themes contributing to inequality. Subsequently, this has resulted in recommendations on restructuring the dental workforce and their development and modifications in oral health care policies and practices. The qualitative synthesis demonstrates the intertwined nature of the multiple factors that influence the goal of achieving an affordable, accessible, extensive and inclusive oral healthcare system in India.
Conclusions
This comprehensive review provides a broad perspective on oral health inequalities in India, providing valuable insights for both researchers and policymakers in this area and guiding their efforts towards achieving universal oral health coverage in the Indian context.
Similar content being viewed by others


Introduction
Universal Health Coverage (UHC) refers to the provision of comprehensive healthcare services to every individual without encountering financial obstacles, regardless of their location or the timing of their needs. These encompass a wide array of health services in an individual’s life span ranging from health promotion and disease prevention to therapeutic care, including rehabilitation and palliative care. Among the 2030 Sustainable Development Goals (SDGs) adopted globally, achieving UHC forms a pivotal component for realizing SDG 3, which aims to ensure good health and well-being for all [1]. While there has been a growing global effort towards achieving UHC, there has been limited advancement in integrating oral health into this framework and moving towards universal oral health coverage (UOHC) [2].
Health inequalities have been recognized as the major barrier in achieving UHC by the World Health Organization [1]. Tsakos et al. referred to the term ‘health inequalities’ as ‘systematic, avoidable, unfair, and unjust differences in health outcomes,’ and throughout this paper, we will be adhering to this definition when discussing oral health inequalities [3]. Globally, inequalities specific to oral health have been established and studied extensively across various domains and contexts, encompassing high, middle and low-income countries [4,5,6]. In the last two decades, literature has emerged that addresses oral health inequalities in India, covering diverse areas including populations experiencing inequalities [7,8,9,10,11,12,13], socioeconomic factors leading to inequality [14,15,16,17], inequalities in the dental workforce [18,19,20] and expert opinions on addressing these gaps [21,22,23,24,25]. The recognition of oral health inequalities, both globally and locally, underscores the importance of comprehending the range of factors that contribute to inequalities in oral health care for effective implementation of targeted interventions.
Therefore, the first step towards attaining universal oral health coverage (UOHC) demands a thorough delineation of the various attributes that contribute to oral health inequalities. While there are existing sources of evidence that summarize various aspects of oral health inequalities worldwide [4,5,6], there is a lack of consolidated evidence specifically addressing this issue in the Indian context. The success of initiatives targeting oral health inequalities, as highlighted in recent literature [3], largely depends on acknowledging the context and ensuring that the proposed interventions align with the needs of stakeholders. This is crucial for effectively addressing the unique challenges associated with oral health inequalities. Although there is literature that addresses certain aspects of oral health inequalities in India, including observational studies on oral health among disadvantaged populations, it is worth noting that a comprehensive and systematically formulated body of literature specifically focused on oral health inequalities in India is currently lacking, to the best of our knowledge. Hence, this scoping review aims to provide decision-makers with comprehensive evidence base on oral health inequalities in India. By precisely documenting the contributing factors responsible for oral health inequalities in India, this review would inform policymakers and dental professionals, enabling them to channelize their efforts and resources effectively to improve access to oral health care services among the masses. Additionally, this scoping review would help to identify research gaps in the literature and delineate necessary modifications for future research in this area.
For achieving the aforementioned goals, the research question for this scoping review was defined as “What is the current evidence base on oral health inequalities in India?“ This research question was designed to fulfil three primary objectives. Firstly, to collate the extent and nature of oral health inequalities in India. Secondly, to identify the sources, types, and quality of evidence in this research area to highlight any research gaps that could guide future recommendations in addressing research related to oral health inequalities in India. Lastly, the review aimed to provide a comprehensive summary of the findings from the available literature, catering specifically to policymakers and dental professionals to facilitate informed decision-making.
Methods
This scoping review was conducted between May 2022 and December 2022 with Arksey and O’Malley’s framework [26] as a guideline and reported in adherence with the PRISMA-ScR checklist which is provided as additional file 1 [27]. As a first step in the framework, we identified the research question with the objective of collecting data on the diverse dimensions of oral health inequalities that exist in India. Therefore, the research question was defined as “What is the current evidence base on oral health inequalities in India?“ The review protocol of the present scoping review was not registered.
Selection criteria
Adhering to the second step of Arksey O’Malley’s framework, relevant studies were identified through a search conducted across four electronic databases (Table 1). Articles addressing one or more aspects of oral health inequalities in India that were published in English between January 2002 and April 2022 were selected. The focus was on the last 20 years, as there was a surge in the establishment of dental colleges in India and the purpose of this review was to examine the trends of oral health inequalities that followed this period of growth of dental colleges across the country. Articles where full-text formats were missing, such as conference proceedings, editorials and letters to editors, were excluded.
Information sources and search strategy
A systematic search was performed by one author (PDB) across four electronic databases, i.e., Scopus, PubMed, Web of Science and EMBASE, from May 2022 with the last search conducted in December 2022. The search strategy, including the key terms and Booleans utilized during the initial search across various databases, is provided in Table 1.
Study selection
The initial search results across the four databases were screened for titles by one author (PDB), which yielded 206 articles. Adhering to the selection criteria described above, these articles were subjected to title and abstract screening followed by full-text review by two authors (PDB and RS) independently. Any disagreements were resolved by discussion with the help of a third author (LD). According to the eligibility criteria, a total of 53 articles were selected following full-text review. One author (PDB) conducted a backward citation search on the references of the chosen articles, resulting in the identification of 54 records, which again underwent title and abstract screening followed by full-text review by two authors (PDB and RS) independently.
Charting the data
The data from the selected full-text articles for the current scoping review were independently charted by two authors (PDB and AKS) using a pre-designed format in Microsoft Excel software version 16.54. This format facilitated the collection of information such as author(s), year of publication, study location, type of study/article, study population, aim of the study, methods used, outcome measures, and significant findings. The data extraction tables were later collaboratively reviewed to identify and complete any missing information that was pertinent to the review and combined to give a more comprehensive picture presented by the chosen articles.
Critical appraisal of the selected articles
This scoping review was undertaken primarily to explore and analyse the existing evidence on oral health inequalities in India, including the types of evidence available, and to identify any gaps in the literature. Therefore, a quality appraisal of the selected sources of evidence was undertaken to accurately determine the research gaps within the current body of literature. The Crowe Critical Appraisal Tool (CCAT) facilitates the critical evaluation of papers covering a diverse array of research designs [28]. Hence, for the current scoping review, we opted to use CCAT because there were no limitations on study designs during the article selection process for this review. The quality appraisal of the selected articles was performed by two authors (PDB and GB) independently. The CCAT evaluates each paper across eight aspects: preliminaries, introduction, design, sampling, data collection, ethical issues, results/findings, and discussion. Each category is scored individually on a scale of 0–5, resulting in a maximum potential score of 40. In case of any conflicting ratings, both authors engaged in a collaborative discussion with a third author (LD) to reach a consensus. For ensuring accuracy, a few articles were randomly selected and subjected to quality appraisal by the third author (LD). Based on the appraisal scores, papers receiving a total score of 35 or higher were classified as high quality, those scoring between 25 and 34 were considered medium quality, and papers scoring below 25 were deemed low quality.
Synthesis of results
Following the last step of Arksey O’Malley’s framework, which involves collating, summarizing, and reporting results, each selected article was subjected to qualitative thematic analysis. One author (PDB) extensively reviewed the extracted data from the selected articles, comparing them with the corresponding full-text articles. Through an open coding process, relevant sections of the full-text articles that addressed the research question on oral health inequalities in India were identified and labelled as initial codes, utilizing ATLAS.ti Mac (Version 23.2.0). At this stage, a second author (RS) was invited to independently review the initial codes. Subsequently, both authors (PDB and RS) integrated and refined the initial codes to arrive at the final codes. These final codes underwent further integration, refinement, and categorization to generate sub-themes aligned with the objectives of the study with assistance from the third author (LD). In the subsequent step, the sub-themes were organized to identify and establish main themes based on their core concepts by two authors (PDB and LD). Through comprehensive discussions, the three authors (PDB, RS, and LD) thoroughly examined and assigned labels to the main themes, followed by tabulation of the main themes and sub-themes to enhance clarity and facilitate understanding.
Results
The results are presented as a summary of the sources, types, and quality of evidence followed by the main themes and subthemes regarding inequalities in oral health in India.
Sources, types, and quality of evidence
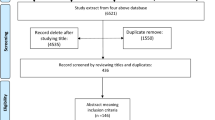
Based on the eligibility criteria, a total of 71 articles retrieved via database search and backward citation search were included in this scoping review. Figure 1 displays the PRISMA flow diagram for this scoping review [29], illustrating the details of the selection process from initial search to final inclusion.

PRISMA flow diagram [29] depicting the process of article selection for the scoping review
Among the sources analysed, a significant portion (55%) were cross-sectional studies. Additional file 2 in the supplementary materials provides a detailed presentation of the features of the evidence sources selected for this scoping review, as well as the data that have been charted from these sources. In Fig. 2, the distribution of the 71 selected papers is illustrated based on the type of study. The majority of the papers were cross-sectional studies (55%), followed by narrative reviews (29.6%). Figure 3 demonstrates that the papers included in this scoping review were predominantly published in the last decade highlighting an increase in research in this area.

Distribution of selected sources of evidence according to type

Distribution of selected sources based on year of publication
The quality appraisal of the selected sources of evidence was performed using CCAT, and detailed scores for each paper are presented in Additional file 3 in the supplementary material. According to the criteria devised by the authors based on the total CCAT scores, the papers were labelled high, medium and low quality for ease of understanding. Among the 71 papers selected for this scoping review, 8 were high-quality papers (11.3%), 42 were medium-quality (59.1%), and 21 were low-quality (29.6%). Most of the cross-sectional studies were evaluated to be of medium quality (84.6%), while few were high quality (12.8%). The majority of the narrative reviews, accounting for 29.6% of the total papers, were deemed to be of low quality (85.7%) due to a lack of methodological clarity. The segregated classification based on quality for the selected papers across various study designs is depicted in Table 2.
Quality assessment was performed using the Crowe Critical Appraisal Tool [28].
Main themes and subthemes concerning oral health inequalities in India: Breaking down the complexities, policy implications and solutions
Each of the main themes is reported with its key findings as listed in Table 3, along with the reference papers. The main themes and sub-themes were organized in a hierarchical manner, starting with individual factors, followed by socio-demographic characteristics and factors influencing access to dental care. This is followed by operational factors influencing oral health care, beginning with the current deficiencies in dental services, dental workforce development and policies, followed by the proposed solutions for each of these areas.
Individual factors were associated with how the knowledge, behaviours, beliefs, and perceptions of the studied populations influence their utilization of accessible dental care services. For instance, fear at different levels, such as fear of dental treatment, discrimination, or concerns about being financially taken advantage of by dental professionals, influenced individuals and deterred them from seeking necessary dental treatment.
Socio-demographic factors, such as age, gender, geographical location, and socioeconomic factors, encompass a range of elements that contribute to the decision-making process of individuals when accessing dental care services. Both individual and socio-demographic factors can directly or indirectly give shape to the emerging barriers and facilitators in accessing oral health care services, which further include factors like affordability, cost of care and other factors such as transportation.
Deficiencies in human resources in oral healthcare emerged as an important theme centred on organizational aspects. For example, when examining factors relating to human resources for oral health, the thematic analysis revealed shortcomings in dental education, inadequacies in dental workforce planning and the limited utilization of dental auxiliaries. Interestingly, several solutions were also suggested in the selected papers, forming another main theme of restructuring of the dental workforce and their development strategies.
Furthermore, at the organizational level, the next main theme was the shortcomings in the provision of dental services, with primary emphasis on identifying deficiencies in current policies and recognizing constraints within public health systems. In conjunction with this, a diverse range of strategies were proposed to enhance oral healthcare services and policies in India. These measures constituted the last main theme of modifications in oral health policies and practices, which included promoting oral health, implementing policy reforms, improving public health systems, and upgrading infrastructure. In the next section, these above results are discussed in the context of current literature, along with their relevance to oral health care in India, followed by seven key recommendations.
Discussion
The purpose of this scoping review was to conduct a comprehensive examination of oral health inequalities in the Indian context. The goal was to establish a solid groundwork for guiding policy makers and dental professionals in addressing these issues and unearthing the research gaps in this area by examining the currently available evidence.
Summary and interpretation of the results
A total of 71 papers were considered for the synthesis of evidence in this scoping review. Most of the papers included in this scoping review were published within the last decade, highlighting the significance and urgency of addressing oral health inequalities in India. The main themes were organized in a structured manner, progressing from individual factors to intermediate sociodemographic factors and their influence on access to care. Following that the themes encompassed structural and organizational factors, such as dental workforce, their education and public and oral health policies that contribute to oral health inequalities. This approach aligns with recent literature, and therefore provides insights into the theoretical frameworks and research pathways that should be considered when conducting research on oral health inequalities [3]. While the main themes follow this arrangement, it is important to note that the core concepts emerging from different themes are intricately linked and exert influence on each another. Therefore, in the subsequent five sub-sections, the key principles derived from the themes at various levels within this hierarchical order will be explored together, interweaving with one another to provide a deeper understanding, rather than examining them individually.
Oral health inequalities in India: upstream and downstream
In the realm of oral healthcare policy, there is a growing recognition to transition from traditional behavioural downstream approaches towards more comprehensive upstream approaches to counter oral health inequalities [8, 31, 32]. The upstream approaches will ensure a more sustainable improvement in oral health promotion since these focus on creating a social environment that is conducive to good oral health for the entire population through fiscal measures, legislation, and local and national policy initiatives [33]. This complements efforts to combat the lack of awareness of the importance of oral health, a significant individual factor identified in this review, which influences how people perceive oral health and ultimately their utilization of oral healthcare services. While upstream strategies are crucial, it’s essential to acknowledge the continued importance of downstream approaches in the Indian context. Individual factors like fear, cultural beliefs, and patient perceptions significantly impact oral health and service utilization. Therefore, in alignment with the recommendations presented by Watt [33] and supported by evidence from various sources in this scoping review [8, 34], adopting complementary strategies that encompass both downstream and upstream approaches in oral healthcare within the Indian context could be a promising path towards achieving oral health equality.
Oral health inequalities in India: harnessing new and leveraging existing systems
Estimates indicate that the treatment of oral diseases is the fourth most expensive in developed nations and can surpass the entire healthcare budget assigned in several countries [35]. This partly explains the insufficient funding dedicated to oral healthcare in India, as emphasized by the findings of this review [2, 21, 36,37,38, 85], thereby highlighting the need to prioritize oral disease prevention over treatment. The review reveals a contrasting situation in the Indian oral public health sector, where there is a lack of emphasis on organized primary oral health programs, with greater attention given to tertiary treatments in government healthcare packages [2, 21, 39].
Consolidating the diverse range of recommendations analysed in this review, it is recommended that instead of generating additional resources for oral health, a more effective approach would be to optimize the utility of the available limited public health resources available. This can be achieved by prioritizing primary prevention and health promotion, utilizing the existing healthcare systems in India. In light of this, the common risk factor approach, which integrates general and oral health, is crucial [12, 15, 20, 22, 37, 38, 40, 41]. Notably, it has been observed that 47.4% of the urban population seeks oral and maxillofacial care at Primary Health Centers (PHCs) maintained by the state government, where non-dental primary care providers, such as medical officers at PHCs, serve as the initial point of contact [42]. Consequently, it becomes crucial to equip all medical professionals and healthcare workers with essential oral healthcare knowledge as well as integrate oral health and medical services at various levels ranging from providing referrals and utilizing technology for virtual integration to sharing locations and funds and ultimately achieving complete integration [22, 36, 42,43,44].
Available resources could be channelized by utilizing the services of Accredited Social Health Activists (ASHAs) and Anganwadi workers for oral health promotion, particularly in rural areas [45]. Furthermore, a significant number of papers emphasized the need for partnerships encompassing public‒private collaborations, collaborations across various health professions in both public and private sectors, partnerships between the government, private sector, and civil society, and community and public partnerships [21, 25, 31, 32, 34, 37, 41, 42, 44, 46,47,48]. More specifically, allocating funding for community preventive oral health programs conducted by dental colleges in India, implementing community-based oral health programs specifically targeting government-run schools in rural areas and forming partnerships with charitable organizations that are well received by the community, are a few examples in this realm.
An imperative element of optimizing existing resources involves embracing successful healthcare models tailored to oral health promotion within the Indian context. For example, the “Fit for School” program employed for school children in the Philippines, where handwashing, periodic deworming was included with toothbrushing with fluoridated toothpaste [49]. This initiative employs a directed population approach and has the potential to be replicated in India, with a particular emphasis on children in rural areas, providing a sustainable and cost-efficient method to promote both oral and general health on a large scale. Furthermore, established frameworks of successful public health campaigns, such as the “Pulse Polio” and the “Mid-Day Meals Scheme,“ can be utilized to enhance oral health initiatives for children [32].
Adoption of novel approaches is equally important to enhance the existing system, like the implementation of updated oral health care policies with necessary modifications [18, 19, 30, 31, 38,39,40, 43, 50], having adequate representation of dentists in decision-making bodies [18, 23, 51], allocation of sufficient resources to establish dedicated dental units within Primary Health Centres, employing cost-effective measures such as utilization of dental auxiliaries in primary healthcare and embracing newer technological advancements, such as teledentistry for remote dental consultations and leveraging technology for oral health promotion [44, 50, 52].
Oral health inequalities in India: demand vs. supply
Access to oral health care is primarily influenced by demand and supply dynamics [21]. The supply side of this equation, as revealed by this scoping review revealed significant inadequacies in the development of human resources for oral health in India, particularly an uneven distribution of dental colleges across rural and urban areas, as well as among different states [18, 21, 23, 24, 31, 39, 53, 54]. This disparity is further magnified with shortage of dental professionals working in rural areas and limited opportunities in the public health sector, resulting in an imbalance in the allocation of dentists, between the private and public sectors as well as between urban and rural regions [18,19,20,21, 23, 24, 37,38,39, 41, 43, 44, 46, 53, 55]. It has been found that public dental facilities, like Primary and Community Health Centres, face shortages of dental professionals, including dentists and dental auxiliaries, and the available dentists are underutilized due to a lack of necessary equipment and materials [2, 21, 23, 37, 42, 46, 52, 56, 57].
In alignment with the World Health Organization’s vision document “Global strategy on human resources for health: Workforce 2030” [58], ensuring universal access to oral healthcare in India requires strategic planning to balance the distribution of dental colleges and optimize the utilization of existing dental graduates to reshape the dentist-to-population ratio in underserved areas. Promoting rural dental practices, encouraging dentists to work in the public sector and primary care, and increasing the use of skill-mix are essential to ensure better dental workforce planning. This would also contribute to tackling the issue of Indian dental graduates leaving the country due to factors such as shortcomings in the oral healthcare system, a scarcity of public sector job opportunities, and career stagnation [87]. Better utilization of dental auxiliaries within the Primary Health centres could be more cost-effective and support dentists with high workload [57]. Global trends suggest that dental auxiliaries have the potential to play a crucial role in oral disease prevention, health promotion, raising awareness, and improving access to oral care services. Skill mix models are utilized across the globe, where the services of dental therapists, dental hygienists and dental nurses are employed to enhance access to oral health care [59, 60, 88,89,90].
Directing attention to the demand side of this dynamic, individual factors such as patient perception, perceived needs, and cultural beliefs play a vital role in determining the utilization of dental services [21]. Therefore, consideration should be given to enriching the population’s oral health literacy and modifying health behaviours to enhance the utilization of available dental services.
Oral health inequalities in India: accessibility and affordability
Accessibility and affordability significantly affect healthcare utilization [42]. Based on the results of this scoping review, access to oral healthcare is influenced by socio-demographic factors like education, income, social support, and area of residence, particularly in rural areas, urban slums and resettlement colonies [13,14,15,16, 19, 22, 30, 31, 55, 61,62,63,64,65,66,67,68]. Recommendations to improve access to dental care include a primary healthcare approach and community-centered dental education, which involve measures like increasing the number of public health dentists, implementing mandatory rotations in mobile dental vans, satellite clinics, and rural areas, as well as establishing partnerships between dental colleges and Primary Health Centers (PHCs) and districts.
Affordability emerged as a crucial factor in this scoping review. Some of the barriers to accessing dental care included financial constraints, such as the inability to afford the cost of care, high expenses in the private sector, the absence of dental insurance plans in India as well as transportation difficulties and the associated costs of travelling. This can be better understood through a statement made by Budetti et al., where they described people who could not afford health care as “people who cannot afford to get sick” [21].Therefore, policy and infrastructure reforms involving measures such as providing dental insurance, subsidizing dental care and products, promoting local production of dental materials to reduce costs, and lowering taxes on dental health products such as toothpaste emerged as important avenues to enhance the affordability of dental healthcare among the masses.
Oral health inequities in India: extensive and inclusive
An extensive understanding of the socio-demographic factors brings us closer to grasping the contextual landscape from which we must operate when addressing inequalities in oral health care in India. Therefore, the implementation of organized data recording systems to maintain electronic dental health records in the Indian context becomes significant [36, 38, 52] to better understand the dental needs of various stakeholders belonging to different communities and populations. Inequalities can be based on gender, age, area of residence, social position, and particularly among marginalized populations, including socially isolated individuals such as tribal people [12], immigrants [69], as well as the disadvantaged high-needs group, which comprises individuals with special care requirements [10, 45, 70], health conditions such as HIV leading to discrimination [7, 8], visually impaired individuals [71], orphans [9], and patients with substance abuse issues [72].
Oral health care services can be made more inclusive by tailoring educational programs to meet the needs of various stakeholders, including diverse ethnic groups and underprivileged populations [12, 30, 44, 65, 69], as well as implementing school-based oral health programs [55, 67, 73], initiatives in old-age homes, institutionalized settings as well as implementing community outreach programs for individuals affected by HIV [8]. These proposals align with the directed downstream population approach, which targets specific populations within specific geographic areas [32]. Moreover, these proposals encompassed replicating existing dental outreach models to reach inaccessible populations and utilizing mobile dental units to provide educational initiatives in underserved areas [12, 32, 44].
Enhancing the dental curriculum with a focus on behavioural sciences, ethics, and social responsibility is vital for preparing future dental professionals to serve underprivileged and disadvantaged groups effectively [11, 12, 23, 38, 48, 55, 70, 74]. These measures aim to build empathy among trainees and promote inclusiveness in oral healthcare, ultimately creating an extensive and inclusive oral healthcare delivery system.
Implications of the review
Overall, the findings of this scoping review indicate that we have a substantial, albeit fragmented, understanding of the extent and magnitude of oral health inequalities in India. It seems crucial to move beyond mere documentation and translate this knowledge into practical applications in the field of oral healthcare in India. Policy interventions need to be built upon solid foundations that intricately weave together various factors in the hierarchical framework while recognizing the interdependency among these factors to achieve significant advancements and promote equality in oral healthcare.
Seven key recommendations are proposed as a result of this comprehensive scoping review. First, implement measures that promote the integration of general and oral health across various domains. Second, educate all medical and healthcare workers with essential oral health care knowledge, while also increasing awareness among the population about the significance of oral health and its connection to general well-being. One potential avenue is to propose that health profession councils introduce ongoing professional development courses specifically focused on oral health. Third, fostering collaborations between private and public entities, across diverse health disciplines, communities, and organizations, to enhance access to oral care. Fourth, a crucial practical recommendation is to establish dedicated dental units within Primary Health Centres, equipped with the necessary dental materials, instruments, and workforce to ensure effective operation. The fifth recommendation is to make oral disease prevention cost effective through the utilization of dental auxiliaries within primary healthcare frameworks. The sixth recommendation calls for a shift in dental education toward a more community-oriented approach to sensitize the upcoming dental graduates towards the needs of the community. Lastly, to remain attuned to the prevailing realities of the population, the seventh recommendation suggests implementing organized data recording systems for maintaining electronic dental health records to closely monitor the oral healthcare needs of the population.
Strengths and limitations
This scoping review has provided an in-depth analysis of the literature on oral health inequalities in India through qualitative synthesis of data, which is unique. One of the limitations is that the sources of evidence were confined to four electronic databases, however they were sufficient to identify the existing evidence base. Additionally, some articles that received low-quality scores during critical appraisal were included in the analysis. This decision was made to ensure the inclusion of all relevant literature, aiming to offer a more comprehensive overview of oral health inequalities in India. Although the research designs of the papers included were varied, utilising a structured framework enabled identification of the complex interlinkages and influences they exerted on the oral health system in India.
Future research directions
A need for more higher-quality observational studies and a shift from narrative to more systematic and meta-analytical reviews was identified as essential in establishing robust evidence concerning oral health inequalities in India. Additionally, it is also important to highlight that only one mixed-methods study was found [11], which thoroughly explored the issue of oral health inequality using qualitative methods. Future research in this area, particularly when studying disadvantaged populations, should also prioritize the inclusion of stakeholders’ perspectives and individual’s lived experiences as a central component [3]. This can be achieved by employing qualitative research methods in future investigations to gain a deeper understanding of the underlying causes of oral health inequalities.
Conclusion
This comprehensive review provides a broad perspective on oral health inequalities in India, providing valuable insights for both researchers and policymakers in this area and guiding their efforts towards achieving universal oral health coverage in the Indian context. The spectrum of factors contributing to these inequalities encompass individual and sociodemographic aspects, access considerations, human resources for oral health, various dimensions of dental services, and policy considerations. The qualitative synthesis unveiled the complexity and the intricate interplay among these elements to progress towards universal oral health coverage. The review has identified a lack of awareness among the population and health care providers regarding the importance of oral healthcare and its connection to overall health. Furthermore, it has highlighted limited public funding, necessitating a redirection of resources towards primary prevention strategies rather than solely focusing on treatment of disease. It is imperative to enhance the integration of oral and general healthcare through partnerships involving public, private, and educational institutions. Additionally, there is a pressing need to create and support a well-trained dental workforce, which should include skilled dental auxiliaries. The review culminates in seven recommendations that underscore the effectiveness of employing complementary approaches in oral health, restructuring the dental workforce, and integrating new strategies while optimizing existing systems. These measures aim to address the need for an affordable, accessible, extensive, and inclusive oral healthcare system in India. Furthermore, the review emphasized the necessity for higher-quality experimental research that incorporates qualitative research methods. Overall, this scoping review provides a panoramic view of oral health inequalities in India, to inform policymakers and ensure oral healthcare for all.
Data Availability
The data that supports the findings of this study is available within the manuscript and no additional source of data is required.
References
World Health Organization. WHO. 2023 [cited 2023 Aug 8]. Universal Health Coverage (UHC). Available from: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc).
Purohit BM, Kharbanda OP, Priya H. Universal oral health coverage – perspectives from a developing country. Int J Health Plann Manage. 2022;37(2):610–8.
Tsakos G, Watt RG, Guarnizo-Herreño CC. Reflections on oral health inequalities: theories, pathways and next steps for research priorities. Community Dent Oral Epidemiol. 2023;51(1):17–27.
Bastani P, Mohammadpour M, Mehraliain G, Delavari S, Edirippulige S. What makes inequality in the area of dental and oral health in developing countries? A scoping review. Cost Eff Resour Alloc. 2021;19(1):1–12.
Ghanbarzadegan A, Balasubramanian M, Luzzi L, Brennan D, Bastani P. Inequality in dental services: a scoping review on the role of access toward achieving universal health coverage in oral health. BMC Oral Health. 2021;21(1):1–1.
Como DH, Stein Duker LI, Polido JC, Cermak SA. The persistence of oral health disparities for African American children: a scoping review. Int J Environ Res Public Health. 2019;16(5):710.
Samuel SR, Muragaboopathy V, Patil S. Transgender HIV status, self-perceived dental care barriers, and residents’ stigma, willingness to treat them in a community dental outreach program: cross-sectional study. Spec Care Dentist. 2018;38:307–12.
Koyio L, Ranganathan K, Kattappagari KK, Williams DM, Robinson PG. Oral health needs assessment world-wide in relation to HIV. Themes: oral health needs and inequalities, oral health promotion, co-ordinating research and enhancing dissemination in relation to HIV- a workshop report. Oral Dis. 2016;22:199–205.
Kumar S, Goyal A, Tadakamadla J, Tibdewal H, Duraiswamy P, Kulkarni S. Oral health related quality of life among children with parents and those with no parents. Community Dent Health. 2011;28(3):227–31.
Rajput S, Kumar A, Puranik MP, Sowmya KR. Oral health inequalities between differently abled and healthy school children in Bengaluru—A cross-sectional study. Spec Care Dentist. 2020;40(1):55–61.
Suresh LR, Rai K, Hegde AM, D’souza CV. Barriers to utilisation of dental services among children with disabilities in a coordinated healthcare programme in Mangalore in India: a mixed methods study. Disabil CBR Incl Dev. 2020;31(4):66–89.
Anil M, Chandrashekar J, Vinita S, Arun K, Joe J, Raj RS, et al. Reaching the Unreached-A retrospection of the Nine Yearlong Oral Rehabilitative Program in the tribal hamlets of Kerala. Indian J Public Health Res Dev. 2019;10(6):81–4.
Shah N. Gender issues and oral health in elderly indians. Int Dent J. 2003;53(5):475–84.
Mathur MR, Tsakos G, Parmar P, Millett CJ, Watt RG. Socioeconomic inequalities and determinants of oral hygiene status among urban Indian adolescents. Community Dent Oral Epidemiol. 2016;44(3):248–54.
Megalamanegowdru J, Vijayanath V. Socioeconomic status and oral health inequity in Karnataka. Indian J Public Health Res Dev. 2013;4(3):121–4.
Mathur MR, Tsakos G, Millett C, Arora M, Watt R. Socioeconomic inequalities in dental caries and their determinants in adolescents in New Delhi, India. BMJ Open. 2014;4:e006391.
Chandra Shekar BR, Reddy CVK. Oral health status in relation to socioeconomic factors among the municipal employees of Mysore city. Indian J Dent Res. 2011;22(3):410–8.
Halappa M, Naveen BH, Kumar S, Sreenivasa H. SWOT analysis of dental health workforce in India: a dental alarm. J Clin Diagn Res. 2014;8(11):ZE03–5.
Singh A, Purohit BM. Addressing oral health disparities, inequity in access and workforce issues in a developing country. Int Dent J. 2013;63(5):225–9.
Mathur M, Singh A, Watt R. Addressing inequalities in oral health in India: need for skill mix in the dental workforce. J Family Med Prim Care. 2015;4(2):200–2.
Janakiram C, Rudrappa RB, Taha F, Ramanarayanan V, Akalgud HG, Kadanakuppe S. Equity in Oral Healthcare in India A Review on Health System Analysis. Econ Polit Wkly. 2017;LII(9):82–9.
Puzhankara L, Janakiram C. Medical-dental integration-achieving equity in periodontal and general healthcare in the Indian scenario. J Int Soc Prev Community Den. 2021;11(4):359–66.
Tandon S. Challenges to the oral health workforce in India. J Dent Educ. 2004;68(7 Supplement):28–33.
Nanda Kishor K. Public health implications of oral health-inequity in India. J Adv Dent Res. 2010;I(I):1–10.
Kakde S, Bedi R, Verma M. Oral health inequalities: a call for action to improve oral health in India. Int Dent J. 2013;63(6):324–8.
Arksey, Hilary. O’Malley Lisa. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Tricco AC, Lillie E, Zarin W, O’Brien K, Colquhoun H, Kastner M, et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med Res Methodol. 2016;16:1–10.
Crowe M, Sheppard L, Campbell A. Reliability analysis for a proposed critical appraisal tool demonstrated value for diverse research designs. J Clin Epidemiol. 2012;65(4):375–83.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Kailembo A, Preet R, Stewart Williams J. Socioeconomic inequality in self-reported unmet need for oral health services in adults aged 50 years and over in China, Ghana, and India. Int J Equity Health. 2018;17(1):1–14.
Mehta Vi V, Rajesh G, Rao A, Shenoy R, Pai M. Social determinants of health and oral health: an Indian perspective. Indian J Occup Environ Med. 2015;19(2):71–5.
Jawdekar AM. A proposed model for infant and child oral health promotion in India. Int J Dent. 2013;2013:1–6.
Watt RG. From victim blaming to upstream action: tackling the social determinants of oral health inequalities. Community Dent Oral Epidemiol. 2007;35(1):1–11.
Satyarup D, Kumar M, Dalai RP, Rathor KR. Basic Package for oral care: a means to Tackle Community Dental needs. Indian J Forensic Med Toxicol. 2020;14(4):8365–71.
Janakiram C, Dye BA. A public health approach for prevention of periodontal Disease. Periodontol 2000. 2020;84(1):202–14.
Siddharthan S, Naing NN, Wan-Arfah N, Assiry AA, Adil AH. Oral Health Care Services in India. Int J Pharm Res. 2021;13(01):3786–90.
Janakiram C, Sanjeevan V, Rajeev BR, Joseph J, Stauf N, Benzian H. Political priority of oral health in India: analysis of the reasons for neglect. J Public Health Dent. 2018;78(2):144–53.
Singh A, Purohit BM. Addressing geriatric oral health concerns through national oral health policy in India. Int J Health Policy Manag. 2015;4(1):39–42.
Vundavalli S. Dental manpower planning in India: current scenario and future projections for the year 2020. Int Dent J. 2014;64(2):62–7.
Gupta S, Ranjan V, Rai S, Mathur H, Solanki J, Koppula SK. Oral health services utilization among the rural population of western Rajasthan, India. J Indian Acad Oral Med Radiol. 2014;26(4):410–3.
Chandu V, Pachava S, Vadapalli V, Sanikommu S. Is the intention being realized in Execution: Evaluation of Oral Health Promotion Program at a south Indian University. J Orofac Sci. 2018;10(2):121–6.
Iyer K, Krishnamurthy A, Pathak M, Krishnan L, Kshetrimayum N, Moothedath M. Oral health taking a back seat at primary health centers of Bangalore urban district, India – A situation analysis. J Family Med Prim Care. 2019;8(1):251–5.
Kothia NR, Bommireddy VS, Devaki T, Vinnakota NR, Ravoori S, Sanikommu S, et al. Assessment of the status of national oral health policy in India. Int J Health Policy Manag. 2015;4(9):575–81.
Khemka S, Baliga S, Thosar N. Approaches to improve access to dental care services. Int Dent Med J Adv Res. 2015;1:1–4.
Subramaniam N, Muthukrishnan A. Barriers to oral health care in patients with special needs-a cross-sectional study. Res J Pharm Technol. 2021;14(4):2167–71.
Sehgal P, Lal S. Enhancing Public Private Partnership in oral Health Care. J Indian Association Public Health Dentistry. 2011;2011(18, Suppl. II):923–4.
Chavan S, Kemparaj U, Rajdha A, Baghele ON. Public-private partnership to enhance oral health in India. J Interdisciplinary Dentistry. 2012;2(2):135–7.
Gambhir R, Gupta T. Need for oral health policy in India. Ann Med Health Sci Res. 2016;6(1):50–5.
Monse B, Benzian H, Naliponguit E, Belizario V, Schratz A, Van Palenstein Helderman W. The fit for School health outcome study - A longitudinal survey to assess health impacts of an integrated school health programme in the Philippines. BMC Public Health. 2013;13(1).
Saha S, Jagannatha GV, Singh S, Singh E. Affordable quality oral health care. Indian J Public Health Res Dev. 2014;5(3):189–94.
Chandu VC, Pachava S, Vishwanath V. Strategies for improving accessibility to Oral Health Care Services in Rural India: an insight. Int J Oral Health Med Res. 2017;4(2):44–6.
Menon S. Provisioning of dental health in public hospitals: a case study of District Jalandhar, Punjab. Indian J Dent Res. 2016;27(6):592–6.
Yadav P, Kaur B, Srivastava R. Oral health disparities: review. IOSR J Dent Med Sci. 2014;13(9):69–72.
Sandhu K, Kruger E, Tennant M. Dental schools in the Republic of India: a geographic and population analysis of their distribution. Int J Oral Health Sci. 2014;4(1):13–7.
Gambhir RS, Brar P, Singh G, Sofat A, Kakar H. Utilization of dental care: an Indian outlook. J Nat Sci Biol Med. 2013;4(2):292–7.
Tandon S, Tandon S, Acharya S, Kaur H. Utilization of Mobile Dental Health Care Services to answer the oral health needs of Rural Population related papers. J Oral Health Community Dentistry. 2012;6(2):56–63.
Verma H, Aggarwal AK, Rattan V, Mohanty U. Access to public dental care facilities in Chandigarh. Indian J Dent Res. 2012;23(1):121.
World Health Organization. Global strategy on human resources for health: workforce 2030. 2016.
Nash DA, Friedman JW, Mathu-Muju KR, Robinson PG, Satur J, Moffat S, et al. A review of the global literature on dental therapists. Community Dent Oral Epidemiol. 2014;42(1):1–10.
Freeman R, Lush C, MacGillveray S, Themessl-Huber M, Richards D. Dental therapists/hygienists working in remote-rural primary care: a structured review of effectiveness, efficiency, sustainability, acceptability and affordability. Int Dent J. 2013;63(2):103–12.
Gupta E, Robinson PG, Marya CM, Baker SR. Oral health inequalities: relationships between environmental and individual factors. J Dent Res. 2015;94(10):1362–8.
Paul B, Basu M, Dutta S, Chattopadhyay S, Sinha D, Misra R. Awareness and practices of oral hygiene and its relation to sociodemographic factors among patients attending the general outpatient department in a tertiary care hospital of Kolkata, India. J Family Med Prim Care. 2014;3(2):107–11.
Kadanakuppe S, Bhat PK. Oral health status and treatment needs of Iruligas at Ramanagara District, Karnataka, India. West Indian Med J. 2013;62(1):73–80.
Krishnan L, Balasubramanium A, Iyer K, Kumar PDM. Factors affecting the Unmet Dental needs and Dental Service Utilisation among Urban Slum dwellers of Chennai City, India. Indian J Public Health Res Dev. 2019;10(11):1451–6.
Oberoi SS, Sharma G, Oberoi A. A cross-sectional survey to assess the effect of socioeconomic status on the oral hygiene habits. J Indian Soc Periodonto. 2016;20(5):531–42.
Chaturvedi R, Aggarwal V, Goyal C, Jain A. Impact of accessibility to Dental schools on oral Health Status of North Indian Children Population. Indian J Public Health Res Dev. 2013;5(2):206–10.
Gupta D, Momin RK, Mathur A, Srinivas KT, Jain A, Dommaraju N, et al. Dental caries and their treatment needs in 3–5 year old preschool children in a rural district of India. N Am J Med Sci. 2015;7(4):143–50.
Kumar A, Virdi M, Veeresha K, Bansal V, Kumar CA. Oral health status & treatment needs of rural population of Ambala, Haryana, India. Internet J Epidemiol. 2009;8(2):1–7.
Radha G, Pushpanjali K, Aruna CN. Acculturation and oral health status among Tibetan immigrants residing in Bangalore city, India. J Clin Exp Dent. 2011;3(4):274–9.
Adyanthaya A, Sreelakshmi N, Ismail S, Raheema M. Barriers to dental care for children with special needs: general dentists’ perception in Kerala, India. J Indian Soc Pedod Prev Dent. 2017;35(3):216–22.
Jawahar A, Maragathavalli G. Assessment of oral health and treatment needs in Population with Visual Impairment. J Indian Acad Oral Med Radiol. 2022;34(1):60.
Madhan B, Gayathri H, Garhnayak L, Naik ES. Dental Students’ regard for patients from often-stigmatized populations: findings from an Indian Dental School. J Dent Educ. 2012;76(2):210–7.
Chauhan Z, Vyas N, Acharya S, Joshi NK, Maheshwari S. Development of a health risk communication tool to address oral health issues of schoolchildren of Balotra block, Rajasthan. World J Dentistry. 2017;8(6):461–6.
Kumar V, Atre S, Jain R, Bhanushali N, Singh S, Chaudhari S. Include-integrate-involve: deciphering oral healthcare providers’ professional demeanor towards sexual and gender minority cohorts in a metropolitan city of western India. J Oral Biol Craniofac Res. 2021;11(2):149–57.
Bommireddy VS, Koka KM, Pachava S, Sanikommu S, Ravoori S, Chandu VC. Dental service utilization: patterns and barriers among rural elderly in Guntur District, Andhra Pradesh. J Clin Diagn Res. 2016;10(3):ZC43–7.
Jain VK, Sequeira P, Jain J, Chancy U, Maliyil M, Bhagwandas S. Barriers in Utilization of Oral Health Care Services among Patients Attending Primary and Community Health Centres in Virajpet, South Karnataka. Natl J Med Dent Res. 2013;1(3):39–47.
Kadaluru U, Kempraj V, Muddaiah P. Utilization of oral health care services among adults attending community outreach programs. Indian J Dent Res. 2012;23(6):841.
Bhatt S, Rajesh GR, Rao A, Shenoy R, Pai MBH, Nayak V. Factors influencing oral health and utilization of oral health care in an Indian fishing community, Mangaluru city, India. World J Dentistry. 2017;8(4):321–6.
Nagaraj A, Ganta S, Yousuf A, Pareek S. Enculturation, myths and misconceptions regarding oral health care practices among rural female folk of Rajasthan. Stud Ethno-Medicine. 2014;8(2):157–64.
Garcha V, Shetiya SH, Kakodkar P. Barriers to oral health care amongst different social classes in India. Community Dent Health. 2010;27(3):158–62.
Subramaniam P, Surendran R. Oral health related quality of life and its association with dental caries of preschool children in urban and rural areas of India. J Clin Pediatr Dent. 2020;44(3):154–60.
Singh A, Sequiera P, Acharya S, Bhat M. Oral Health Status of two 12-year-old socially disadvantaged groups in South India: a comparative study. Oral Health Prev Dent. 2011;9(1).
Shwetha KM, Ranganath K, Pushpanjali K. Attitude of accredited social health activists towards creating awareness on Oral cancer in rural community of Chikkaballapur district, Karnataka. Indian J Community Med. 2019;44(5):46–9.
Manpreet K, Ajmal MB, Raheel SA, Saleem MC, Mubeen K, Gaballah K, et al. Oral health status among transgender young adults: a cross-sectional study. BMC Oral Health. 2021;21(1):575.
Bhandari B, Newton JT, Bernabé E. Income inequality and use of dental services in 66 countries. J Dent Res. 2015;94(8):1048–54.
Mahal AS, Naseem MNAMS. Implications of the growth of Dental Education in India. J Dent Educ. 2006;70(8):884–91.
Davda LS, Radford DR, Scambler S, Gallagher JE. Accreditation and professional integration experiences of internationally qualified dentists working in the United Kingdom. Hum Resour Health. 2022;20(1):1–2.
Davda L. (2020). Oral health care professionals: a call to centre stage. Dent Health. http://www.bsdht.org.uk/publications/dental-health.
Quach DD, Davda JS, Radford LR, Louca D. Are dental schools doing enough to prepare dental hygiene & therapy students for direct access? Bdj Team. 2020;7(10):36–7.
Balasubramanian M, Hasan A, Ganbavale S, Alolayah A, Gallagher J. Planning the future oral health workforce: a rapid review of supply, demand and need models, data sources and skill mix considerations. Int J Environ Res Public Health. 2021;18(6):2891.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
RS and LSD conceptualized the scoping review. PDB, RS, and AKS contributed in data curation. PDB, LSD and GB performed quality appraisal of articles. RS and KM supervised the scoping review at various stages. PDB, RS, LSD and AR contributed to visualization of the scoping review. PDB drafted the original manuscript with inputs from RS, LSD, KM and GB and while PDB, RS, LSD, KM, AR, MP, PJ and ABR provided substantial contributions to final reviewing and editing of the manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dasson Bajaj, P., Shenoy, R., Davda, L.S. et al. A scoping review exploring oral health inequalities in India: a call for action to reform policy, practice and research. Int J Equity Health 22, 242 (2023). https://doi.org/10.1186/s12939-023-02056-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12939-023-02056-5