
Abstract
Background
Although contraceptive use has increased over 15 years, discontinuation rates remain high. Contraceptive use is becoming more important when addressing unmet need for family planning. Social accountability, defined here as collective processes for holding duty bearers to account for their actions, is a rights-based participatory process that supports service provision and person-centred care, as well as, informed decision-making among community members regarding their health. A study implemented in Ghana and Tanzania was designed to understand and evaluate how social accountability and participatory processes influences quality of care and client satisfaction and whether this results in increased contraceptive uptake and use. We report here on the relationship between social accountability and the use of modern contraceptives, i.e., contraceptive method discontinuation, contraceptive method switching, and contraceptive discontinuation.
Methods
As part of Community and Provider driven Social Accountability Intervention (CaPSAI) Project, a cohort of women aged 15 to 49 years who were new users of contraception and accessing family planning and contraceptives services at the study facilities across both intervention and control groups were followed-up over a 12-month period to measure changes contraceptive use.
Results
In this cohort study over a one-year duration, we did not find a statistically significant difference in Ghana and Tanzania in overall method discontinuation, switching, and contraceptive discontinuation after exposure to a social accountability intervention. In Ghana but not in Tanzania, when stratified by the type of facility (district level vs. health centre), there were significantly less method and contraceptive discontinuation in the district level facility and significantly more method and contraceptive discontinuation in the health centres in the intervention group. In Ghana, the most important reasons reported for stopping a method were fear of side-effects, health concerns and wanting to become pregnant in the control group and fear of side-effects wanting a more effective method and infrequent sex in the intervention group. In Tanzania, the most important reasons reported for stopping a method were fear of side-effects, wanting a more effective method, and method not available in the control group compared to wanting a more effective method, fear of side-effects and health concerns in the intervention group.
Conclusions
We did not demonstrate a statistically significant impact of a six-month CaPSAI intervention on contraceptives use among new users in Tanzania and Ghana. However, since social accountability have important impacts beyond contraceptive use it is important consider results of the intermediate outcomes, cases of change, and process evaluation to fully understand the impact of this intervention.
Trial registration
The CaPSAI Project has been registered at Australian New Zealand Clinical Trials Registry (ACTRN12619000378123, 11/03/2019).
Similar content being viewed by others


Background
In Sub-Saharan Africa, modern contraceptive uptake and use are rising, albeit with considerable geographic variation [1]. The reasons for the rise in modern contraceptive prevalence rates include increased access to and use of long-acting reversible contraceptive options, postpartum contraceptive methods, and community health workers [1]. Using data from Demographic and Health Survey (DHS) reports, the Performance Monitoring and Accountability 2020 project, as well as the United Nations world contraceptive database on contraceptive use, it was reported that although contraceptive use increased over 15 years, discontinuation rates were high [1].
Family planning and importance of method continuation, method switching, and contraception continuation
Contraceptive use is becoming more important when addressing unmet need for family planning [2]. Contraceptive use encompasses method continuation,—discontinuation,—switching, and contraceptive discontinuation. Several factors may influence contraceptive use, such as interpersonal communication and patient-provider communication. The importance of switching to another method has been illustrated by Jain et al. [3]. In a study where they collected data on 36 low and middle-income countries (LMIC) on the use of contraceptives by married women, it was estimated that 38% of unmet need for contraception was due to discontinuation of contraceptive methods among those who desired to avoid pregnancy [4]. This means that contraceptive discontinuation contributes to a huge number of unintended pregnancies. Contraceptive discontinuation accounts for one-third of unintended pregnancies [4]. A way to reduce this unmet need is to reduce contraceptive discontinuation by enabling switching to another effective contraception option.
Contraceptive method discontinuation is not inevitable, based on the reasons given in 45% of the incidents [3]. These include side-effects, wanting a more effective method, lack of access, high costs, inconvenience, infrequent sex/husband away, difficulty getting pregnant/menopausal, marital dissolution/separation [3]. This was confirmed by Ali M et al. [5] in a study on causes and consequences of contraceptive discontinuation using 60 Demographic and Health Surveys. The authors reported that many women who use reversible modern methods do so inconsistently or discontinue use because they are not satisfied with the method, are concerned about the side effects, or have trouble getting supplies [5]. Sully et al. [6] reported dissatisfaction, side-effects, and supply problems as reasons for inconsistent use or discontinuation of the method among women who use reversible modern methods. The duration of method effectiveness also affects continuation as was shown by data for 33 LMICs where 20% of users of short-acting methods who want to avoid pregnancy discontinue use within the first year against 11% of women who used intrauterine device and 8% of women who used contraceptive implants [7].
Strengthening the quality of contraceptive information, education, and counseling services seems implicit, as is providing long-acting contraception to enhance use-effectiveness [1]. High-quality services, including counseling, to women using methods, are as important as adding new users towards meeting unmet need (3). Person-centered care (PCC) is where provider-person (client) relationships, effective communication, and shared-decision making are advocated. High-quality PCC improves both women's experience and may also lead to better outcomes [8]. Some measures of PCC quality appear to impact contraceptive continuation. A systematic review reported mixed findings on relationships between PCC and clinical outcomes, with stronger evidence for positive influences of PCC on satisfaction and self-management, but a lack of understanding of how specific PCC processes relate to patient outcomes [9].
A recent systematic review of interventions focused on PCC for family planning found that most interventions were successful in increasing client knowledge about family planning and overall experience, but results were mixed for family planning uptake and continuation [10]. Furthermore, other studies reported that perceived quality of family planning care is associated with client satisfaction and method and contraceptive continuation [11, 12].
The role of social accountability to change interpersonal care and health behaviours
Social accountability, defined here as "citizen-led collective processes for holding duty bearers, including politicians, government officials, and/or service providers, to account for their actions" [13], is a rights-based participatory process that supports service provision and PCC, as well as, informed decision-making among community members regarding their health. Thus, social accountability processes could potentially ensure that family planning services are responsive to client needs and promote trust between women and girls and the health system [14]. Several studies in reproductive, maternal, newborn, child and adolescent health (RMNCAH) demonstrated positive results, especially in intermediate outcomes such as enhanced infrastructure service delivery, commodities and resources allocation, and service utilization [15,16,17,18]. Several studies have reported positive outcomes of social accountability for contraceptive programs such as improvements in service quality, financial allocation for service provision [16, 19], community awareness and participation [20,21,22,23,24] and increased use of modern methods [23]. Social accountability is therefore well suited to support an enabling environment for family planning programs.
The Community and Provider driven Social Accountability (CaPSAI) Project was designed to understand and evaluate the effects of social accountability and participatory processes in the context of a family planning and contraceptive (FP/C) program. The study design, aims, and theory of change are described in detail a protocol manuscript and the Australian New Zealand clinical trial registry [24, 25]. To summarise, this was a complex-designed study exploring how a social accountability process in the context of FP/C programs/services influences QoC and client satisfaction and whether this results in increased contraceptive uptake and use. The design followed the Medical Research Council (MRC) guidance on measuring complex interventions and was grounded on a theory of change and a co-designed intervention. [24, 26, 27]. It accounts for the multiple components to track the levels and interrelated outcomes and includes a process evaluation component [24].
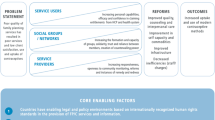
The development of the theory of change (ToC) has been described thoroughly elsewhere [18, 24] (Fig. 1). Briefly, development followed a literature review [28] and findings from a formative phase [17, 24]. Eight core steps were identified as the base of the intervention, which involved community members and health system actors identifying challenges in service provision and care, developing plans of action to improve quality of services, counseling, interpersonal care, staff capacity, and commodity availability [24]. According to ToC, these would lead to positive changes in contraceptive use, such as less contraceptive discontinuation and higher rates of method switching if discontinued.

CaPSAI Theory of Change [29]
This manuscript reports on the findings of the CaPSAI cohort study, which aimed to measure changes in behaviors around contraceptives.
Methodology
Study design
As part of CaPSAI, a cohort of women aged 15 to 49 years who were new users of contraception and accessing family planning and contraceptives services at the study facilities across both intervention and control groups were followed-up over a 12-month period to measure changes contraceptive use [24]. The outcomes measured include: contraceptive method continuation defined as the proportion of women in the cohort using the same contraceptive method after 12 months; contraceptive switching, the proportion of women initiating a method that change methods within 12 months; and contraceptive discontinuation, the proportion of women initiating contraception who stopped using any method within 12 months.
Study setting
The CaPSAI Project was implemented in Ghana and Tanzania. In Ghana, modern contraceptive prevalence rate (mCPR) among currently married women increased from 18.7% in 2003 to 22.2% in 2014 [30] and 25.0% in 2017 [30]. Further, the contraceptive discontinuation rate was 25% within 12 months of starting its use for any reason [31]. In Tanzania mCPR increased steadily from 23.0% in 2004/2005, 30.8% in 2010 and 34.3% in 2015/2016 [32, 33]. The overall use of modern contraceptives increased by 11.3 percent point. A higher increase in modern contraceptive use was detected between 2004—2010, a 7.8%-point increase compared with a 3.5%-point increase detected between 2010 – 2016 (3130). See trend in use of modern contraceptive methods among currently married women in Ghana and Tanzania (Table 1) In Tanzania, 26% of women using a contraceptive method discontinued the method in less than 12 months [33]. In 6% of episodes, women switched to another method.
In Ghana, the study was conducted in the Central region. Four districts, namely Gomoa East, Agona West, Ekumfi, and Ajumako, were selected for the control group. The intervention group had three districts, which were Abura-Asebu-Kwamankese, Komenda-Edna-Eguafo Abirem, and Mfatsiman. In Tanzania, two districts, Mbeya and Chunya, were selected for the intervention group. Two districts, Iringa Urban and Iringa Rural, were selected to be the control group. In Ghana the health centre/clinic and Community based health planning and services were at the primary level health care and the district hospitals were at the second level of health care. In Tanzania the dispensary and health centre were at the primary level health care and district hospital and regional referral hospitals were at the secondary health care. A summary of the demographic information on the facilities chosen is provided in Table 2.
The implementing partners had not previously implemented their social accountability programmes in the selected districts in the two countries. The selection of districts was also based on similarities in cultural, religious, and socio-economic factors. Following a mapping of facilities in the districts, eight facilities in intervention districts and eight facilities in control districts were selected in each country. Criteria for selecting facilities included type and level, the average number of service users, number of new users, and matching by these criteria between facilities in intervention and control districts.
The intervention
CaPSAI used a co-design process to define the intervention of study [34]. This means that the intervention processes in the two study countries are not identical, but all contain the standard steps identified in the theory of change (Table 3). The standard steps are described in more detail elsewhere [18, 24, 34]. Table 1 summarizes the activities conducted for each of the steps in each country. The implementation of the intervention started end of April or beginning of May 2018 with Step 1. Step 8 was completed in December 2018.
Sample size
The discontinuation rate, a time-to-event outcome with censoring, required the use of sample size estimation methods for survival data. As described in the protocol [24, 25], the sample size estimation was computed using values of hazard ratio (intervention vs. control) of 0.5, 0.6, and 0.7, and given values of the proportion of discontinuing use of modern contraception by the end of the first year, in the control group ranged from 30 to 60%. The estimates were obtained using a Type I error at 5% level, accrual time of 0.01 years, and an exponential loss to follow-up of 20% that enables a two-sided Logrank test to achieve 80% statistical power to detect the difference in discontinuation rates by the end of one year of follow-up. Adjustments for clustering were made on the final sample size since the intervention was not at the individual level. Using an intra-class correlation of 0.05 and an average cluster size of 20 first users of modern contraception resulting in a design effect of 2.0, the final sample size was doubled. The sample was estimated to be 800 women across five to eight study facilities per group. The total sample was 1600 women distributed according to the size of the facilities in the intervention and control groups in each country.
Data collection
Data collection was done in real-time using tablet-based standardized interview questions developed using OpenClinica Participate. During data capture, the electronic data capture system performs edit checks to immediately notify of potential errors and inconsistencies. The local study team kept an updated log of screened and enrolled study participants per the data management standard operating procedure [35].
The two main instruments (intake and follow-up interview) were used to collect data from new users of family planning services at the facilities [36]. A mid-term check-up interview at six months following the intake interview was conducted to minimize loss to follow-up and to confirm if the participants are still using a method and which method it is to estimate continuation [36]. The cohort study instruments were adapted from existing tools. The Demographic Health Survey model questionnaires were used to capture demographic characteristics and contraceptive use [29]. Questions from the MEASURE Evaluation's Quick Investigation of Quality were used to capture outcomes related to client satisfaction [37]. The follow-up questionnaire used by Barden-O'Fallon et al. in a one-year study on contraceptive continuation was adapted [38]. The subject areas covered included an update on socio-demographic characteristics, contraceptive use or pregnancy status or intention, experience with side effects, and reproductive and household decision-making [38]. Exposure to the intervention or knowledge among study participants was also captured.
Participant selection, enrolment, and follow-up
Possible study participants were identified during consultations by health providers who referred them to study staff. Screening was done by the study staff using the eligibility criteria that included age [15,16,17,18,19] and whether they were initiating a modern contraceptive method for the first time, switching from a traditional method, or restarting a method after six months of not using one. Following the consent or assent process, the intake interviews were conducted in person at the facility, or an appointment was set later. For the check-up, study staff contacted study participants who did not come to the facility by telephone to conduct the interview or invite them to come to the facility. For study participants who could not be contacted by phone during the check-up at six months, a letter was delivered inviting them to contact the study team. Appointments are set for the 12-month follow-up during the enrolment. If the study participants missed their appointments, they were contacted by phone to set a new appointment.
The intake interviews were conducted after completion of the main steps of the intervention, namely following the completion of the interface meeting (Step 6), where community members and duty bearers get together to jointly develop action plans based on prioritized issues. In both study settings, data collection for the intake interview started in October 2018 and was completed in December 2018. The follow-up interviews were conducted 12 months later, from October to December 2019. The interim check-up interview was done from May to July 2019.
To minimize loss to follow-up, experienced data collectors were recruited from the study areas who were available for the entire study period. Participants who missed their interview appointments were contacted by phone to remind them of the appointment or a study team member went to their homes if they consented to it. If participants could not be reached by phone, a letter was sent to the participant via a community health nurse, health worker or data collector in accordance with the approved protocol. Additionally, the project supported participants’ travel costs to the facility after each interview.
Statistical methods
The rate of loss to follow-up for the one-year follow-up period was computed [24]. The one-year cumulative method discontinuation and method switching rates were compared between the intervention and control groups. Because of the clustered nature of the outcomes, with the intervention package designed at the cluster level, all time-to-event outcomes, including loss to follow-up, method discontinuation, and method switching, were analyzed with hazard ratios estimated from the shared frailty models. The multivariable frailty model was applied to adjust for potential baseline confounders at the participant and/or facility level. Unadjusted and adjusted hazard rate ratios (HRRs) were reported. Interaction between factors was assessed. Two-sided tests, 5% significance levels, and 95% confidence intervals were used for all relevant parameters. Statistical Analysis System (SAS) Version 9.4 and R Version 3.3.3 software packages were used for the statistical analyses.
Results
Follow-up status
In Ghana, 1,711 women were screened for eligibility (Fig. 2, 1,685 were eligible, 822 in the control and 863 in the intervention group. In the control group, 762 completed the study with 17 lost to follow-up. In the intervention group, 830 completed the study, and seven were lost to follow-up.

Ghana enrollment flowchart
In Tanzania, 1,661 women were screened, and 1,624 were eligible (Fig. 3). Of 817 women enrolled in the control group, 742 completed the study, 28 were lost to follow-up, and five were excluded due to a protocol violation (enrolled less than six months of stopping a previous method). In the intervention group, of 807 women enrolled, 770 completed the study, 27 were lost to follow-up, and two were excluded due to protocol violation (one reported initiating a method less than six months of stopping a previous method and another initiated emergency contraception).

Tanzania enrollment flowchart
Demographic characteristics
The demographic characteristics of the study population were comparable among intervention and control groups in both countries, as summarized in Table 2. In Ghana, the majority of women were 21 to 35 years of age, 75.6% and 67.2% in the control and intervention groups, respectively. In Tanzania, the 21 to 35 age group also made up the majority of the study population, 76.5% and 71% in the control and intervention groups, respectively. Majority of participants in both countries were married and not significantly different between the intervention and control groups, 54.3% in the control and 53.3% in the intervention in Ghana, 79.3% in the control and 80.3% in the intervention group in Tanzania. The distribution of the number of living children among women in the control and intervention groups was also similar in both countries.
Method initiated
A quota for the type of method was not imposed during enrolment. In Ghana, the most popular method initiated was the injectable in both control (62.7%) and intervention group (70.9%) followed by implants, by 30.3% and 23.5% of the respondents in the control and intervention groups, respectively. Contraceptive pills were the third most commonly initiated method in both groups (3.3% in the control and 3.5% in the intervention). There were significantly more injectables initiated in the intervention group and more implants in the control group. In Tanzania, the most popular method initiated during the intake interview was the Implant in both control (58.1%) and intervention group (52.2%), followed by injectables used by 28% and 27% of the respondents in the control and intervention groups, respectively. Contraceptive pills were the third most commonly initiated method in both groups (7.1% in the control and 14.9% in the intervention). There were no statistically significant differences between the study and control group in methods initiated.
Several questions to understand informed choice were asked during the intake interview. In Ghana (Table 4), significantly more participants in the intervention group reported that they were told by a health or family planning provider about other methods of family planning that they could use (71.9% vs. 42.9%; (p ˂ 000.1) and significantly more participants in the control group reported that the provider described possible side effects of the specific method they chose (90.3% vs. 84.1%; p = 0.0002). There were no significant differences in the number of women who reported that the healthcare provider gave them a chance to ask questions and that the healthcare provider responded to the questions that they asked in the control and intervention groups.
In Tanzania (Table 5), there were significantly more participants in the control group who reported that: they were told by a health or family planning provider about other methods of family planning that they could use (84.5% vs. 67.1%; p ˂ 000.1), the provider described possible side effects of the specific method they chose (85.6% vs. 73.0%; p ˂ 000.1), the provider informed them what to do if they had any problems for the method they just accepted (93.0% vs. 78.4%; p ˂ 000.1), the healthcare provider gave them a chance to ask questions (76.8% vs. 53.6%; p ˂ 000.1) and the healthcare provider responded to the questions that they asked (97.6% vs. 92.8%;p ˂ 000.1).
Knowledge and exposure to the intervention
Knowledge of and exposure to the intervention remained low in the intervention groups of both Ghana and Tanzania (Table 6 and Table 7). In Ghana, of 118 women who knew of community monitoring and social accountability interventions, 112 had heard of CaPSAI activities, and 56 of 57 who participated in any type of community monitoring and social accountability activities participated in CaPSAI activities. In Tanzania, of 25 who knew about community monitoring and social accountability activities, eleven knew of CaPSAI activities. Only Three women reported participating in CaPSAI activities during the intake interviews in Tanzania.
Use of same facility at intake as compared to follow-up interview
In Ghana, 508 (61.8%) participants in the control and 584 (67.7%) participants in the intervention group attended the same clinic throughout the follow-up period. In Tanzania, 245 (30.2%) participants in the control and 324 (40.2%) participants in the intervention group attended the same clinic throughout the follow-up period.
In Tanzania, 15.01% in the control group and 21.5% in the intervention group were not attending the same facility during the follow-up compared to the intake interview. The main reason for not attending the same facility is that they moved out of area (50.89% in the control vs 50.60% in the intervention). They found the facility difficult to reach (30.36% in the control vs 33.13% in the intervention). Meanwhile, in Ghana, 5.91% and 11.93% were no longer attending the same facility as the intake in the control and intervention groups, respectively. In Ghana, the reasons for changing facilities were moving out of the area (44.44% in the control vs 22.22% in the intervention), not being able to make appointment" (2.22% in the control vs 34.34% in the intervention), and difficulty of reaching the facility (20% control vs 4.04% in the intervention).
Contraceptive method discontinuation
The contraceptive method discontinuation is the proportion of women not using the method that they started after one year of initiation and is expressed in Fig. 4 to Fig. 7 as time-survival estimates of the intervention against the control group.

Ghana: overall contraceptive method discontinuation by 12 months. CaPSAI group: 183 events / 863 at risk and KM survival probability 78.1 (75.8,81.4). Control: 118 events / 822 at risk and KM survival probability 85.1 (82.4,87.4). Frailty model unadjusted HRR CaPSAI vs Control 1.18 (0.59, 2.37), p-value = 0.64
In Ghana, in the intervention group, 183 out of 863 participants discontinued their method and, in the control group, 118 out of 822 participants discontinued their method (Fig. 4). Using the frailty model, there was no significant difference between discontinuation in the intervention and control groups (unadjusted HRR = 1.18; 95%CI 0.59,2.37; p = 0.64). However, there were significant differences when stratified by type of facility. At district level facilities, 15 out of 127 participants in the intervention group and 18 out of 56 in the control group discontinued their method (Unadjusted HRR = 0.29; 95%CI 0.15, 0.57; p-value of 0.0004) (Fig. 5). At the health centre level, 160 of 671 participants in the intervention group and 59 of 603 in the control group discontinued contraceptive method with an unadjusted HRR = 2.42 (95%CI 1.25, 4.69); p-value of 0.0087) indicating higher discontinuation in the intervention group (Fig. 6). These results were did not change after adjusting for important confounders (Table 8), there was a 70% reduction in the rate of contraceptive method discontinuation among users at the district hospital level, among participants who were in the intervention group compared to the control group (adjusted HRR = 0.30; 95% CI 0.06,1.37). However, the reverse was the case, for the users at the health centre, where a higher rate of method contraceptive discontinuation was observed in those in the intervention group, relative to those in the control group, with the rate in the intervention group that was almost twice that of the control. (adjusted HRR = 1.98; (95%CI 1.01,3.91).

Ghana: contraceptive method discontinuation by 12 months—District level. CaPSAI group: 15 events / 127 at risk and KM survival probability 88.1 (81.1,92.7). Control: 18 events / 56 at risk and KM survival probability 64.7 (49.9,76.2). Frailty model unadjusted HRR CaPSAI vs Control 0.29 (0.14, 0.57), p-value = 0.0004

Ghana: contraceptive method discontinuation by 12 months: Health centre. CaPSAI group: 160 events / 671 at risk and KM survival probability 75.3 (71.8,78.5). Control: 59 events / 603 at risk and KM survival probability 89.9 (87.2,92.1). Frailty model unadjusted HRR CaPSAI vs Control 2.39 (1.25, 6.88), p-value = 0.0087
In Tanzania, 184 out of 812 participants discontinued their method in the intervention group,and in the control group, 218 out of 805 discontinued their method. Using the unadjusted Frailty model, there was no significant difference contraceptive method discontinuation in the intervention relative to the control group, (unadjusted HRR 1.34 95% CI 0.85, 2.12; p = 0.21) (Fig. 7). The results did not change after multivariable adjustment, in the frailty model with no significant difference in method discontinuation rate in the intervention compared to the control group (adjusted HRR 1.35 95% CI 0.85, 2.12; p = 0.21) (Table 9).

Tanzania: contraceptive method discontinuation by 12 months. CaPSAI group: 184 events / 812 at risk and KM survival probability 71.8 (68.5,74.8). Control: 218 events / 805 at risk and KM survival probability 75.8 (72.6,78.7). Frailty model unadjusted HRR CaPSAI vs Control 1.34 (0.85, 2.12), p-value = 0.21
Method switching
Contraceptive method switching is the proportion of women changing their method within one year of initiation expressed in Fig. 8 and Fig. 9 as time-survival estimates of the intervention against the control group.

Ghana: contraceptive method switching by 12 months. CaPSAI group: 63 events / 863 at risk and KM survival probability 91.8 (89.6,93.6). Control: 29 events / 822 at risk and KM survival probability 95.9 (94.1,97.2). Frailty model unadjusted HRR CaPSAI vs Control 1.59 (0.80, 3.14), p-value = 0.18

Tanzania: contraceptive method switch by 12 months. CaPSAI group: 80 events / 812 at risk and KM survival probability 83.2 (80.2,85.7). Control: 122 events / 805 at risk and KM survival probability 88.7 (86.1,90.8). Frailty model unadjusted HRR CaPSAI vs Control 1.66 (0.93, 2.96), p-value = 0.085
In Ghana, in the intervention group, 63 out of 863 participants and 29 out of 822 in the control group switched (Fig. 8). Before adjustment of confounders, the frailty model estimated a 59% increased rate in switching between methods in the intervention group relative to the control group, which was, however, not significant (Unadjusted HRR = 1.59; 95%CI 0.80, 3.14; p = 0.18). After multivariate adjustment, the multivariable frailty model showed that the adjusted HRR = 1.55 (95% CI: 0.79, 3.06; p = 0.20) (Table 10).
In Tanzania, in the intervention group, 80 out of 812 participants switched, and in the control group, 122 out of 805 participants switched. Using the univariate frailty model, there was 66% increased switching rate in the intervention group relative to the control, which was however non-significant at 5% level (HRR = 1.66; 95% CI: 0.79, 3.06; p = 0.20 p = 0.085) (Fig. 9). After adjusting for important confounders in a multivariable frailty model the adjusted HRR = 1.71 (95%CI: 0.96, 3.04; p = 0.07) in favor of increased rate in the control group (Table 11).
Contraceptive discontinuation
Contraceptive discontinuation was measured as the proportion of women in the cohort discontinuing contraceptives in the first year of use and expressed in Fig. 10 to Fig. 13 as a time-survival estimate of the intervention against the control group.

Ghana: contraceptive discontinuation by 12 months. CaPSAI group: 142 events / 863 at risk and KM survival probability 83.4 (80.7,85.8). Control: 111 events / 822 at risk and KM survival probability 85.9 (83.3,88.1). Frailty model unadjusted HRR CaPSAI vs Control 0.95 (0.43, 2.12), p-value = 0.91
In Ghana, in the intervention group, 143 out of 863 participants discontinued contraception and, in the control group, 11 out of 822 participants discontinued their method. Using the Frailty model, there was no significant difference between discontinuation in the intervention and control groups (unadjusted HRR = 0.95; 95%CI: 0.43, 2.12; p = 0.91) (Fig. 10). However, there were significant differences in contraceptive discontinuation when stratified by type of facility. At the district level, 7 out of 127 participants in the intervention group discontinued their contraception, and 18 out of 56 participants in the control group. At this level, there was a 87% reduction in contraceptive discontinuation in the intervention relative to the control group (unadjusted HRR = 0.13; 95%CI 0.06, 0.32; p-value = 0.0004) (Fig. 11). At the health centre level, 130 out of 571 participants in the intervention group discontinued their method, and 55 out of 603 participants in the control group, with the intervention group having twice the rate than that of the control, in discontinuing the contraception method (unadjusted HRR = 2.08; 95%CI:0.92, 4.65; p-value = 0.0078) (Fig. 12).

Ghana: contraceptive discontinuation by 12 months – District Hospital. CaPSAI group: 7 events / 127 at risk and KM survival probability 94.5 (88.8,97.3). Control: 18 events / 56 at risk and KM survival probability 64.7 (49.9,76.2). Frailty model unadjusted HRR CaPSAI vs Control 0.13 (0.06, 0.32), p-value = 0.0004

Ghana: contraceptive discontinuation by 12 months – Health Centre. CaPSAI group: 130 events / 671 at risk and KM survival probability 79.6 (76.2,82.6). Control: 55 events / 603 at risk and KM survival probability 90.6 (87.9,92.7). Frailty model unadjusted HRR CaPSAI vs Control 2.07 (0.92, 4.65), p-value = 0.078
Following adjusting for important confounders (Table 12), there was an 86% reduction in the rate of contraceptive discontinuation among users at the district hospital level, in participants who were in the intervention group relative to the users in the control group (adjusted HRR = 0.14; 95% CI 0.02,0.95). However, the opposite was the case, for the users at the health centre, there was a reported close to the three-quarter increase in the contraceptive discontinuation rate in the intervention relative to the control group, which however did not reach the margin of statistical significance at 5% level (adjusted HRR = 1.72; (95%CI 0.76,3.88).
In Tanzania, 145 out of 812 participants discontinued their method in the intervention group, and in the control group, 150 out of 805 participants discontinued their method. Using the Frailty model, there was no significant difference between discontinuation in the intervention and control groups (unadjusted HRR = 1.13; 95% CI: 0.66, 1.91; p = 0.66) (Fig. 13). After adjusting for important confounders in a multivariable frailty model, the adjusted HRR = 1.04 (95%CI: 0.64, 1.70) was not statistically significant difference between the two groups (Table 13).

Tanzania: contraceptive discontinuation by 12 months. CaPSAI group: 145 events / 812 at risk and KM survival probability 80.2 (77.2,82.9). Control: 150 events / 805 at risk and KM survival probability 80.6 (77.6,83.3). Frailty model unadjusted HRR CaPSAI vs Control 1.13 (0.66, 1.91), p-value = 0.66
Reasons for discontinuation in methods at follow up interview
In Ghana, the most important reasons reported for stopping a method were fear of side-effects (34.1%), health concerns (13.6%) and wanting to become pregnant (13.6%) in the control group and fear of side-effects (25.8%), wanting a more effective method (17.7%) and infrequent sex (16.7%) in the intervention group (Table 14). In Tanzania, the most important reasons reported for stopping a method were fear of side-effects (24.6%), wanting a more effective method (18%), and method not available (18%) in the control group compared to wanting a more effective method (27.6%), fear of side-effects (17.2%) and health concerns (17.7%) in the intervention group (Table 14).
Satisfaction
In both countries, questions eliciting satisfaction with the provider care and facility care yielded a very high positive response with the intake. They could not be analysed to see differences over time (Table 15 and Table 16). A high percentage (close to 100%) of women said that they would return to the same provider during the intake interview in both control and intervention groups. The same was found when women were asked if they would refer a friend or a relative to the facility or provider.
Discussion
The study's overall aim is to demonstrate how a social accountability process in family planning and contraceptive -programs and -services influence Quality of Care and client satisfaction and whether this leads to increased contraceptive uptake and use. We report here on the relationship between social accountability and the use of modern contraceptives, i.e., contraceptive method discontinuation, contraceptive method switching, and contraceptive discontinuation. To our knowledge, this is the first study reporting on contraceptive use after a social accountability intervention. In this cohort study over a one-year duration, we did not find a statistically significant difference in Ghana and Tanzania in overall method discontinuation, switching, and contraceptive discontinuation after exposure to a social accountability intervention.
Differences in Ghana when stratified according to the level of facility and the health system structure
However, in Ghana but not in Tanzania, when stratified by the type of facility (district level vs. health centre), there were significantly less method and contraceptive discontinuation in the district level facility and significantly more method and contraceptive discontinuation in the health centres in the intervention group. These findings validate our ToC and previous study findings that social accountability is context-driven process, and understanding the different factors, including the health care system structure, is key to evaluating their effect. Health systems are made up of complex networks of interconnected actors that influence service delivery at varying degrees [28]. Policy decisions and institutional organizations and procedures may affect how interventions change contraceptive use. Meanwhile, the interface between infrastructure, clients, and providers determines the quality of services. Several health system characteristics have been identified as enabling social accountability. Decentralization of governance and service delivery structures are essential as it puts priority setting closer to the community [28]. When the decentralization processes are not fully realized, local government systems, cannot meaningfully engage with clients and community members. They may not have the capacity or the resources to respond to the demands resulting from the social accountability process [39, 40].
In the case of Ghana, significant differences in the unexpected direction" were demonstrated when stratified by facility type. This may be explained through the health system perspective, where less discontinuation is expected at the health centre level as communities are assumed to have closer interaction with the health centre providers, both in terms of services but also through family planning and reproductive health activities and mechanisms. Meanwhile, it is also expected that district hospitals will have a higher cadre of health personnel who can offer more elaborate FP methods such as IUD compared to lower cadre of health personnel who staff health centres and CHPS compounds at a lower level. We found less discontinuation in district hospitals which are likely to offer a variety of methods and higher cadre of personnel [41,42,43].
The state may also not be the only provider of contraceptive services. In many settings, commercial service providers and non-profit organizations also provide family planning [44]. These non-state actors may also influence family planning decision-making and use. For CaPSAI, context mapping in-depth interviews were conducted at the district level in both countries to capture these family planning services done by non-state actors but will be reported elsewhere.
Method choice and continuation
These interventions are context-specific, as shown by the methods of choice at the initiation of enrollment [45, 46]. In this study, in Ghana, women overwhelmingly chose injectables followed by implants, and in Tanzania, it was implants followed by injectables. These are in line with existing method prevalence data in both countries [33]. Continuation rates are different between the two methods, with implants having a higher continuation rate [47]. Despite the differences in method mix, overall method discontinuation was not affected in both countries suggesting no differential impact of SA intervention by method used.
There is no clear reason why this was the case. Possible explanations could be explored, include that the intervention was not long enough sustained and the intermediate effects, such as behavioural changes, including myths and structural changes have not taken hold or that there was not enough time before the intervention was evaluated to observe these changes. Another explanation may be that the pathway of the Theory of Change did not lead to the expected changes. Lastly commodity availability may have influenced the results. The drivers are being explored further in the process evaluation which will be published separately [25].
Informed choice: differences in the two groups
On provider behavior to enable women to make an informed choice the study found variability by behavior and country. In Ghana, after the intervention, the provider was more likely to give information on method options but gave better counseling on side effects in the control group. There were no significant differences on whether health providers gave women an opportunity to ask questions and respond to questions.
In Tanzania, the findings from the informed choice questions were significantly better in the control group except for one question (Table 5). These findings could be due to an impact of the SA intervention on provider behavior or women being more demanding or less satisfied with the status quo [48]. There can also be differences because of contextual factors such as outreach and training provided by NGOs to facility staff. This will be further analysed through the context mapping and intermediate outcomes and will be reported elsewhere.
Satisfaction of family planning care and services
In both countries and in both groups, there were overall high rates of "very satisfied" and "satisfied" responses before and after the intervention. This high level of satisfaction may have limited the interventions’ impact on contraceptive use by improving satisfaction. The assumption in the ToC that there was low satisfaction whose improvement would be a pathway through which contraceptive use is affected did not hold in these particular contexts.
Importance of intermediate outcomes and process evaluation
The reasons why women discontinued remained the same in intervention and control, suggesting a limited impact of the intervention on them. In Ghana, the main reasons for discontinuation in the control group and intervention group were fear of method side-effects. In the intervention group, other main reasons were wanting a more effective method and infrequent sex. In Tanzania, the most important reasons reported for stopping a method were fear of side-effects in the control group and wanting a more effective method followed by fear of side-effects in the intervention group. This is in keeping with other studies showing that side effects are major reasons for the discontinuation of methods [49]. This is also reflected in the wider literature on family planning and contraceptive discontinuation [49, 50]. In a review, reasons for discontinuing included the reduced need for family planning, which may include changes in fertility status and fertility intentions, infrequent sex [7, 50]. Among discontinuers who still need, reasons for stopping their contraception include becoming pregnant despite being on a method, health concerns, those who switch to a more effective method, lack of access to their method, and husband or partner opposition [50]. In Ghana, a national-level survey revealed that the top three reasons why women discontinue use of contraceptives were wanting to become pregnant (27%), side effects/health concerns (21%), and becoming pregnant while using (20%) [31]. In Tanzania, the most common reason for discontinuing a method in less than 12 months is the desire to become pregnant (38%), followed by method-related side effects or health concerns (26%) [33]. Other common reasons are infrequent sex, inconvenient to use, health concerns, desire to become pregnant, difficulty in getting pregnant, menopause, marital dissolution, and method failure were frequently reported by other studies [51, 52].
To understand the link between social accountability and contraceptive use as reported in this paper, there is need to: evaluate how women make decisions, their self-efficacy, knowledge, attitude and practices, their interaction with service providers, the accessibility and availability of methods, norms, and gender dynamics in specific settings, and how these are affected by social accountability processes. CaPSAI captured the impact of social accountability on some of these issues and these findings will be reported elsewhere.Footnote 1 Specifically, a cross-sectional survey with validated psychometric scales explored the links between social accountability interventions and service users perceptions of empowerment, efficacy, and engagement with the health care providers [25]. Within and across the two countries, the results were mixed whereby two domains registered positive changes, while five domains registered negative changes over time and four reversed directions during the study period. Moreover, a process evaluation that included case studies of change aimed to capture the changes related to the intervention and collected data to determine what factors were present and key for a change to take hold1 [24].
Limitations
We selected facilities/districts that were comparable for basic characteristics (level and number of users), but there may be differences between the groups that we did not account for. There are clear differences between the countries, but the basic demographics are similar between the groups within a country. In general, there were similar demographic characteristics between the control and the intervention groups in both countries. However, further analysis of the contextual factors, i.e. ongoing facility-led outreach and NGO activities, are needed to examine the comparability of the groups and will be reported elsewhere1.
Even though the follow up rate is very impressive for a study conducted in these countries, there is also a major difference in follow-up rates in the same facilities between the countries. It is more important to note that many women, especially in Tanzania, did not use the same facility where they were recruited during the intake interview. Although the women responded that they were not anticipating to move outside the intervention area/district during the period of study during the screening, this was the leading reason for attending a different facility at follow up.
Knowledge and exposure to the intervention were low in the intervention groups of both Ghana and Tanzania at the intake as well as the follow-up interview. According to the ToC, this should not have affected the study as the intervention had its effect at the facility level resulting in changes that would enhance the use of contraceptive methods. There is also a risk of under-estimation bias if, despite intervention coverage in the intervention facility/catchment area, some women choose to go to one facility over another facility in the same catchment area.
Processes that require changes in behavior, including social accountability interventions, take time to be effective and behaviour change maintenance depends on motives, self-regulation, resources (psychological and physical), habits, environmental and social influences [53, 54]. Both these timing of the measurement and maintenance of the behavioural change may have played a role in the outcomes measured here.
Qualitative data at the community level to understand social and gender dynamics in the context of social accountability was not purposefully collected due to budgetary constraints for a more intensive process evaluation. Firstly, the CaPSAI study process evaluation focused on collecting data at the district level in both intervention and control groups to understand family planning initiatives and other community participation programs as part of the context mapping1. Secondly, non-participant observation of key intervention activities and in-depth interviews were conducted in four of the eight interventions sites in each country with intervention participants to trace the implementation and gain a fuller description of the social accountability process and how the outcomes were produced1. Finally, case studies were conducted to retrospectively explore reported changes resulting from the intervention1.
Conclusion
We did not demonstrate a statistically significant impact of a six-month CaPSAI intervention on contraceptives use among new users in Tanzania and Ghana. However, since social accountability have important impacts beyond contraceptive use it is important consider results of the intermediate outcomes, cases of change, and process evaluation to fully understand the impact of this intervention. Studies to understand potential links between SA and service utilization should include counterfactual analysis and be supported by structured process evaluation.
Social accountability is complex and may result in complex actions which may not be straightforward to explain. A social accountability intervention could lead to women who have been exposed to a social accountability-related activity resulting in more demanding or less satisfied with the status quo. Social accountability may not consistently decrease discontinuation and its impact are complicated by other health system and contextual factors, including the responsiveness of the health care system such as the level of service, including setting.
Availability of data and materials
The de-identified dataset used and/or analysed during the current study can be requested from the Primary Sponsor or Principal Investigators, and data will be shared contingent on approval by the internal review and approval by local internal ethics review board.
Notes
All published manuscripts related to the Community and Provider driven Social Accountability Intervention (CaPSAI) Project are and will be uploaded on the Australian New Zealand Clinical Trials Registry (ACTRN12619000378123).
References
Tsui AO, Brown W, Li Q. Contraceptive practice in Sub-Saharan Africa. Popul Dev Rev. 2017;43(Suppl Suppl 1):166–91. https://doi.org/10.1111/padr.12051.
Sarnak DO, Wood SN, Zimmerman LA, Karp C, Makumbi F, Kibira SP, Moreau C. The role of partner influence in contraceptive adoption, discontinuation, and switching in a nationally representative cohort of Ugandan women. PLoS ONE. 2021;16(1): e0238662.
Jain AK, Obare F, RamaRao S, Askew I. Reducing unmet need by supporting women with met need. International perspectives on sexual and reproductive health. 2013 Sep 1:133–41.Accessed 12 July 2021. http://www.jstor.org/stable/23596124.
Jain AK, Winfrey W. Contribution of contraceptive discontinuation in 36 developing countries. Stud Fam Plann. 2017;48:269–78 (pmid:28398595).
Ali M, Cleland J and Shah I, Causes and Consequences of Contraceptive Discontinuation: Evidence from 60 Demographic and Health Surveys, Geneva: WHO, 2012. https://apps.who.int/iris/bitstream/handle/10665/75429/?sequence=1
Sully E, Biddlecom A, Darroch JE, Riley T, Ashford LS, Lince-Deroche N, Firestein L, Murro R. Adding it up: investing in sexual and reproductive health 2019. Guttmacher Institute. https://www.guttmacher.org/report/adding-it-up-investing-in-sexual-reproductive-health-2019
Family Planning 2020 (FP2020), FP2020: Women at the Center 2018–2019, 2019, http://progress.familyplanning2020.org/.
Rubashkin N, Warnock R, Diamond-Smith N. A systematic review of person-centered care interventions to improve quality of facility-based delivery. Reprod Health. 2018;15(1):169. https://doi.org/10.1186/s12978-018-0588-2.PMID:30305129;PMCID:PMC6180507.
Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70:351–79.
Diamond-Smith N, Warnock R, Sudhinaraset M. Interventions to improve the person-centered quality of family planning services: a narrative review. Reprod Health. 2018;15(1):144. https://doi.org/10.1186/s12978-018-0592-6.
Dehlendorf C, Henderson JT, Vittinghoff E, et al. Association of the quality of interpersonal care during family planning counseling with contraceptive use. Am J Obstet Gynecol. 2016;215(1):78.e1-78.e9. https://doi.org/10.1016/j.ajog.2016.01.173.
Liu J, Shen J, Diamond-Smith N. Predictors of DMPA-SC continuation among urban Nigerian women: the influence of counseling quality and side effects. Contraception. 2018. https://doi.org/10.1016/j.contraception.2018.04.015.
Joshi A. Legal empowerment and social accountability: complementary strategies toward rights-based development in health?. World Development. 2017 Nov 1;99:160–72. https://doi.org/10.1016/j.worlddev.2017.07.008160. Accessed 13 July 2021.
High Impact Practices in Family Planning (HIP). Social accountability to improve family planning information and services. Washington, DC: HIP Partnership; April 2022. Available from: http://www.fphighimpactpractices.org/briefs/social-accountability/. Accessed 21 February 2023
Squires F, Martin Hilber A, Cordero JP, Boydell V, Portela A, Lewis Sabin M, Steyn P. Social accountability for reproductive, maternal, newborn, child and adolescent health: a review of reviews. PLoS ONE. 2020;15(10): e0238776.
Boydell V, Neema S, Wright K, Hardee K. Closing the gap between people and programs: lessons from implementation of social accountability for family planning and reproductive health in Uganda. Afr J Reprod Health. 2018;22(1):73–84.
Steyn PS, Cordero JP, Gichangi P, et al. Participatory approaches involving community and healthcare providers in family planning/contraceptive information and service provision: a scoping review. Reprod Health. 2016;13(1):88. https://doi.org/10.1186/s12978-016-0198-9.
Steyn PS, Cordero JP, Nai D, Shamba D, Fuseini K, Mrema S, Habib N, Nguyen MH, Kiarie J. Impact of community and provider-driven social accountability interventions on contraceptive uptake in Ghana and Tanzania. Int J Equity Health. 2022;21(1):142.
Boydell V, Nulu N, Hardee K, Gay J. Implementing social accountability for contraceptive services: lessons from Uganda. BMC Womens Health. 2020;20(1):1-2.
Hamal M, de Cock BT, De Brouwere V, Bardají A, Dieleman M. How does social accountability contribute to better maternal health outcomes? A qualitative study on perceived changes with government and civil society actors in Gujarat India. BMC Health Serv Res. 2018;18(1):1–5.
Otchere S, Jacob V, Toppo AA, Massey A, Samson S. Social accountability and education revives health sub-centers in India and increases access to family planning services. Christian J Glob Health. 2017;4(2):10–8.
Panthi GP. Social accountability for adolescent sexual and reproductive health. Himalayan J Sociol Anthropol. 2016;7:13–39.
Gullo S, Galavotti C, Altman L. A review of CARE’s Community Score Card experience and evidence. Health Policy Plan. 2016;31(10):1467–78. https://doi.org/10.1093/heapol/czw064.
Steyn PS, Boydell V, Cordero JP, McMullen H, Habib N, Nguyen TM, Nai D, Shamba D, Kiarie J, Project C. Rationale and design of a complex intervention measuring the impact and processes of social accountability applied to contraceptive programming: CaPSAI Project. [version 2; peer review: 2 approved]. Gates Open Res. 2020;4:26.
Steyn, P.S., Boydell, V., Cordero, J.P., Habib, H.M., Nai, N., Shamba, D., Kiarie, J.: Community and provider driven social accountability intervention (CaPSAI) project: study protocol. 2020. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=376797&isReview=true. (2020) Accessed on 13 July 2021
Moore G, Audrey S, Barker M, et al. Process evaluation of complex interventions: a summary of Medical Research Council guidance. In: Richards D, Hallberg IR, editors. Complex interventions in health: an overview of research methods Abingdon. New York: Routledge; 2015.
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. Bmj. 2008;337:a1655.
Boydell V, Keesbury J. Social accountability: What are the lessons for improving family planning and reproductive health programs? Working Paper. Washington, DC: Population Council, Evidence Project; 2014.
Demographic and Health Surveys Program: DHS Model Questionnaires: General Information, current use of family planning, continuation, informed decision making. 2019. https://dhsprogram.com/methodology/Survey-Types/DHS-Questionnaires.cfm#CP_JUMP_16179. Last accessed 30 June 2021
Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF. Ghana Maternal Health Survey. Accra. Ghana: GSS, GHS, and ICF; 2017. p. 2018.
Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF International. Ghana Demographic and Health Survey 2014. Maryland, USA: GSS, GHS, and ICF International; 2015.
Yussuf MH, Elewonibi BR, Rwabilimbo MM, Mboya IB, Mahande MJ. Trends and predictors of changes in modern contraceptive use among women aged 15–49 years in Tanzania from 2004–2016: evidence from Tanzania demographic and health surveys. PLoS ONE. 2020;15(6): e0234980.
Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), and ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015–16. Dar es Salaam, Tanzania, and Rockville, Maryland, USA: MoHCDGEC, MoH, NBS, OCGS, and ICF; 2016.
McMullen H, Boydell V, Cordero JP, Steyn PS, Kiarie J, Kinemo P, Monyo A, Addah MA, Ahuno JT, Gyamfi OB. Accounting for complexity–Intervention design in the context of studying social accountability for reproductive health. Gates Open Res. 2021;5(107):107.
CaPSAI Project Team. CaPSAI Project - Standard Operating Procedures. figshare. Online resource. 2021. https://doi.org/10.6084/m9.figshare.14363336.
Steyn PS, Boydell V, Cordero J, McMullen H, Habib N, Shamba D, et al. CaPSAI Project - Extended Data (Study Instruments). figshare. Online resource. 2020. https://doi.org/10.6084/m9.figshare.11743206.v1.
MEASURE Evaluation. Quick Investigation of Quality (QIQ): A User's Guide for Monitoring Quality of Care in Family Planning. (2nd ed.). Chapel Hill: MEASURE Evaluation, University of North Carolina; 2016.
Barden-O'Fallon J, Speizer I, Cáceres Zelaya S, et al.: Contraceptive Discontinuation: A One-Year Follow-Up Study of Female Reversible Method Users in Urban Honduras – Final Report. MEASURE Evaluation. 2008.
Butler N, Johnson G, Chiweza A, Aung KM, Quinley J, Rogers K, Bedford J. A strategic approach to social accountability: Bwalo forums within the reproductive maternal and child health accountability ecosystem in Malawi. BMC Health Serv Res. 2020;20(1):1–6.
Van Belle S, Boydell V, George AS, Brinkerhof DW, Khosla R. Broadening understanding of accountability ecosystems in sexual and reproductive health and rights: a systematic review. PLoS ONE. 2018;13(5): e0196788.
Agongo EEA, Issah K, Williams JE, Ayaba F, Kunfah B, and Ofosu KW. Improving Family Planning Service Delivery in Ghana. Working paper. 2018. MEASURE Evaluation. document (measureevaluation.org).
Kweku M, Amu H, Adjuik M, Aku FY, Manu E, Tarkang EE, Komesuor J, Asalu GA, Amuna NN, Boateng LA, Alornyo JS. Community utilisation and satisfaction with the community-based health planning and services initiative in Ghana: a comparative study in two system learning districts of the CHPS+ project. BMC Health Serv Res. 2020;20(1):1–4. https://doi.org/10.1186/s12913-020-05678-5.
Kweku M, Amu H, Awolu A, Adjuik M, Ayanore MA, Manu E, Tarkang EE, Komesuor J, Asalu GA, Aku FY, Kugbey N. Community-based health planning and services plus programme in Ghana: a qualitative study with stakeholders in two systems learning districts on improving the implementation of primary health care. PLoS ONE. 2020;15(1): e0226808.
Freedman LP, Schaaf M. Act global, but think local: accountability at the frontlines. Reprod Health Matters. 2013;21(42):103–12.
Jacobstein R. Liftoff: the blossoming of contraceptive implant use in Africa. Global Health: Sci Pract. 2018;6(1):17–39.
United Nations, Department of Economic and Social Affairs, Population Division (2019). Contraceptive Use by Method 2019: Data Booklet (ST/ESA/SER.A/435).
Peipert JF, Zhao Q, Allsworth JE, Petrosky E, Madden T, Eisenberg D, Secura G. Continuation and satisfaction of reversible contraception. Obstet Gynecol. 2011;117(5):1105.
Gullo S, Kuhlmann AS, Galavotti C, Msiska T, Marti CN, Hastings P. Creating spaces for dialogue: a cluster-randomized evaluation of CARE’s Community Score Card on health governance outcomes. BMC Health Serv Res. 2018;18(1):1–2.
Nega G, Abera M, Tadele A. Discontinuation rate and associated factors among contraceptive implant users in Kersa district, southwestern Ethiopia. Arch Public Health. 2021;79(1):1–9.
Bradley SE, Schwandt H, Khan S. Levels, trends, and reasons for contraceptive discontinuation. DHS analytical studies. 2009;20:27–9.
Safari W, Urassa M, Mtenga B, Changalucha J, Beard J, Church K, Zaba B, Todd J. Contraceptive use and discontinuation among women in rural North-West Tanzania. Contracept Reprod Med. 2019;4(1):1.
Sato R, Elewonibi B, Msuya S, Manongi R, Canning D, Shah I. Why do women discontinue contraception and what are the post-discontinuation outcomes? Evidence from the Arusha Region, Tanzania. Sexual Reprod Health Matters. 2020;28(1):1723321.
Kwasnicka D, Dombrowski SU, White M, Sniehotta F. Theoretical explanations for maintenance of behaviour change: a systematic review of behaviour theories. Health Psychol Rev. 2016;10(3):277–96. https://doi.org/10.1080/17437199.2016.1151372.
Moore MJ. The transtheoretical model of the stages of change and the phases of transformative learning: comparing two theories of transformational change. J Transform Educ. 2005;3(4):394–415. https://doi.org/10.1177/1541344605279386.
Acknowledgements
The authors would like to acknowledge the following in Tanzania: Regional Medical Officers of participating regions, District health authorities in participating districts for their support throughout the study period. The authors thank all study participants in all study districts, the whole team of research assistants and all the people involved in the study. Authors would also like to acknowledge the support of the Chief Executive Director of IHI Dr. Honorati Masanja, the CaPSAI data manager in Tanzania-Mr. Selemani Mmbaga and the IHI administrative team (Ms. Catherine Ringo, Ms. Adeline Herman, Ms. Doreen Philemon, and Ms. Pamela Sao).
In Ghana, the authors would like to acknowledge the Ministry of Health, Ghana Health Service as well as regional and district health authorities of Central region. The authors thank all the study participants in all study districts, the whole team of research assistants and all the people involved in the study. Authors would also like to acknowledge the support of colleagues from Population Council Ghana and New York (Augustine Ankomah, Michelle Hindin, Henry Tagoe, Rachel Narki Anum, Kojo Mensah Sedzro, Martin Agbodzi, Seth Boateng and Emmanuel Amevor).
The authors would also like to acknowledge CaPSAI Project implementation team, specifically: Victoria Boydell (independent); Mary Awelana Addah and Osei-Bonsu Gyamfi (Ghana Integrity Initiative); Alice Monyo, Happy Myovela and Joshua Nkila (Sikika). Implementation support was provided by Heather McMullen (Queen Mary University) and Vernon Mochache (independent).
Additional analytical input was provided by Soe Soe Thwin (WHO) and data management support was provided by Antonio-Lucio Fersurella (WHO). Additional conceptual input on the CaPSAI protocol was provided by Ian Askew (WHO) and Karen Hardee (Evidence Project). The CaPSAI Project team would also like to acknowledge the support of Roseline Doe and Edwin Swai from the WHO country offices in Ghana and Tanzania, respectively.
Funding
This work was supported by the Bill and Melinda Gates Foundation [OPP1084560] and United States Agency for International Development (USAID) to the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training Human Reproduction, which is the main instrument and leading research agency within the United Nations system concerned with sexual and reproductive health and rights.
Author information
Authors and Affiliations
Contributions
PSS, JPC and JK contributed to the conception of the study. PSS, JPC, NH, MHN and JK contributed in the design of the protocol. DN, DS, KF, SM, MHN were responsible for data acquisition. MHN created the software used in the work. All authors contributed in the analysis and interpretation of data. Drafting was done by PSS and JPC and all authors substantially contributed in the review, revision and finalisation of the manuscript. All authors approved the submitted version.
Authors’ information
The authors alone are responsible for the views expressed in this article, and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
Corresponding author
Ethics declarations
Ethics approvals and consent to participate
The master and country protocols (Project ID A65896) were approved by technical and ethics review committees at the World Health Organization (WHO). The country protocols were reviewed and approved at country level. The Population Council Institutional Review Board (exemption approval—# EX201714) and Ghana Health Service Ethics Review Committee (GHS-ERC:009/08/2017) approved the Ghana country protocol. In Tanzania, the protocol was approved by Ifakara Health Institute Institutional Review Board (IHI/IRB/No:18–2018 and IHI/IRB/AMM/No:03–2019) and the National Institute of Medical Research (NIMR) review board (NIMR/HQ/R.8a/Vol.IX/2668), and the NIMR/Mbeya Medical Research and Ethics Review Committee (GB.152/377/01/214a). The study was conducted in accordance with the Declaration of Helsinki.
All study participants underwent informed consent procedures. For adolescents, the consenting/assenting and interviewing were done using a two-step process. The researcher explained the study and informed the adolescents meeting the inclusion criteria that their parent or guardian would need to be informed about the study and give their consent unless they are emancipated adolescents. When the adolescents agreed to participate and they were accompanied by their parents or guardian, consent was obtained from the parents/guardian, followed by assent from the adolescent. If they were not accompanied by a parent or guardian, they were invited to return for another appointment to go through the consent/assent process before the interview.
Consent for publication
Not Applicable.
Competing interests
The authors did not declare any competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under the terms of the Creative Commons Attribution 3.0 IGO License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the World Health Organization, provide a link to the Creative Commons licence and indicate if changes were made..The use of the World Health Organization’s name, and the use of the World Health Organization’s logo, shall be subject to a separate written licence agreement between the World Health Organization and the user and is not authorized as part of this CC-IGO licence. Note that the link provided below includes additional terms and conditions of the licence. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/3.0/igo/.
About this article

Cite this article
Steyn, P.S., Cordero, J.P., Nai, D. et al. The impact of community and provider-driven social accountability interventions on contraceptive use: findings from a cohort study of new users in Ghana and Tanzania. Int J Equity Health 22, 167 (2023). https://doi.org/10.1186/s12939-023-01928-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12939-023-01928-0