
Abstract
Background
The processing of food can cause changes that turn them into risk factors for chronic diseases. A higher degree of food processing is associated with the development of chronic non-communicable diseases (NCDs), including the metabolic syndrome (MetS). The objective of this study was to analyze the relationship between ultra-processed food (UPF) consumption and the prevalence of MetS and its risk factors, focusing on a population group especially subjected to precarious living conditions and food insecurity.
Method
Cross-sectional population-based study with women (19 to 59 years) from Quilombola communities of Alagoas. The socioeconomic, demographic, anthropometric, health status, lifestyle, and food intake (24-h recall) variables were analyzed. The dependent variable was the MetS, defined using the harmonization criteria of the Joint Interim Statement, and its components. The foods consumed were categorized according to the Nova Classification, assuming the highest UPF consumption as risk exposure. The measure of association was the prevalence ratio (PR) and respective 95%CI, calculated by Poisson regression with robust variance. We also analyzed the association with the Nova score of UPF consumption.
Results
We investigated 895 women (38.9 ± 11.0 years), of whom 48.3% had MetS. On average, 15.9% of the total energy intake came from UPF. Lower Nova scores were associated with a lower prevalence of diabetes and low HDL. Higher UPF consumption was associated with a 30% higher prevalence of hypertension (PR = 1.30; 95%CI: 1.06–1.61).
Conclusion
The highest UPF consumption was positively associated with the prevalence of hypertension, while a lower Nova score was a protective factor against diabetes and low HDL. UPF consumption in Quilombola communities is important but lower than that observed in the Brazilian population in general. It is suggested that public health programs be implemented to promote healthy eating while valuing the existing eating habits and traditions among the remaining Brazilian Quilombola people.
Resumo
Introdução
O processamento de alimentos pode causar alterações que os transformam em fatores de risco para doenças crônicas. Um maior grau de processamento de alimentos está associado ao desenvolvimento de doenças crônicas não transmissíveis (DCNT), incluindo a síndrome metabólica (SM). O objetivo deste estudo foi analisar a relação entre o consumo de alimentos ultraprocessados (AUP) e a prevalência de SM e seus fatores de risco, com foco em um grupo populacional especialmente submetido a precárias condições de vida e insegurança alimentar.
Método
Estudo transversal de base populacional com mulheres (19 a 59 anos) de comunidades Quilombolas de Alagoas. Foram analisadas as variáveis socioeconômicas, demográficas, antropométricas, estado de saúde, estilo de vida e ingestão alimentar (recordatório de 24 horas). A variável dependente foi a SM, definida a partir dos critérios de harmonização do Joint Interim Statement, e seus componentes. Os alimentos consumidos foram categorizados de acordo com a Classificação Nova, assumindo como exposição de risco o maior consumo de AUP. A medida de associação foi a razão de prevalência (RP) e respectivo IC 95%, calculado por regressão de Poisson com variância robusta. Também analisou-se a associação com o Escore Nova de consumo de AUP.
Resultados
Foram investigadas 895 mulheres (38,9 ± 11,0 anos), das quais 48,3% tinham SM. Em média, 15,9% da ingestão total de energia provinham de AUP. Escores Nova mais baixos foram associados a uma menor prevalência de diabetes e HDL baixo. O maior consumo de AUP se associou a uma prevalência 30% maior de hipertensão arterial (RP = 1,30; IC95%: 1,06-1,61).
Conclusão
O maior consumo de AUP se associou positivamente à prevalência de hipertensão, enquanto o menor escore Nova foi fator de proteção contra diabetes e baixo HDL. O consumo de AUP nas comunidades Quilombolas é relevante, mas inferior ao observado na população brasileira em geral. Sugere-se a implementação de programas de saúde pública que promovam a alimentação saudável, valorizando os hábitos e tradições alimentares existentes entre os remanescentes Quilombolas brasileiros.
Similar content being viewed by others

Introduction
Unhealthy eating patterns influence the occurrence of several chronic non-communicable diseases (NCDs), including metabolic syndrome (MetS), characterized by the presence of a set of cardiovascular risk factors in the individual [1,2,3]. The prevalence of MetS in adults ranges from 11.0 to 62.5% in different geographic regions of the world [4]. Some studies indicate that the prevalence of MetS is influenced by the ethnic-racial factor, with high prevalences being found in Afro-descendant populations. In Brazil, the prevalence of MetS ranged from 25.8% [5] to 55,4% [6] among African descendants living in Quilombola communities.
The main risk factors for developing MetS are use alcohol abuse, smoking, a sedentary lifestyle, and unhealthy eating habits [7,8,9]. Changes in the eating habits of the population have contributed to the occurrence of MetS due to the increased consumption of foods subjected to a high level of industrial processing [10], with consequent alteration of their natural state, to make them less perishable and improve their organoleptic characteristics, such as color, aroma, and flavor [11, 12].
Studies have shown that a higher degree of food processing is associated with the development of NCDs, constituting a risk factor for hypertension [13], obesity [14, 15], cancer [16], and MetS [17]. This fact is attributed to the high content of sodium, refined carbohydrates, saturated fats, and trans fats often present in these foods. These constituents act synergistically, increasing the risk of several morbid conditions and the etiology of MetS [13, 18, 19].
Currently, there are different classifications regarding the level of food processing. One of them is the so-called Nova classification [20], which has been incorporated into the guidelines in the Food Guide for the Brazilian Population [21]. This classification establishes four categories of foods according to the processing degree: 1) unprocessed and minimally processed foods; 2) processed culinary ingredients; 3) processed foods, and 4) ultra-processed foods (UPF). Among these categories, UPF are defined as a group of foods that include industrial food formulations made mostly or entirely from food-derived or laboratory- synthesized substances [22, 23].
The consumption of UPF is present in the food of individuals from all income levels, jeopardizing potentially the food security situation of different populations [24, 25]. Thus, populations living in a situation of social vulnerability, as in the case of the remaining Quilombola communities, need to have their food consumption better known since an unhealthy dietary pattern puts the health of individuals health at risk [24]. However, there are few studies on the relationship between food consumption of different processing levels and MetS [26], mainly among the Quilombola people.
Research conducted with socially vulnerable populations, characterized by difficulty of access to health services and adequate food, can contribute to the better clinical practice of health professionals and the planning of effective public policies to promote the quality of life of this population contingent.
This research aimed to characterize UPF consumption and identify its association with MetS and its risk factors in women from Quilombola communities in the state of Alagoas, Brazil.
Methods
This study is part of a project entitled "Diagnosis of Health and Food and Nutritional Security of the Families of the Remaining Quilombos Communities in the State of Alagoas", which was approved by the Research Ethics Committee of the Federal University of Alagoas (CAAE 33.527.214.9.0000.5013). All women analyzed agreed to participate in the study and signed the Informed Consent Form.
Study design and location
This is a population-based cross-sectional study, conducted in Quilombola communities of Alagoas, which, in 2015, comprised 68 communities certified as remaining quilombos, distributed in 34 of the state's 102 municipalities [27]. Alagoas has an estimated population of 3,351,543 inhabitants and has the worst Human Development Index (HDI = 0.683) among the other states of the federation [28]. The per capita monthly income of Quilombola families in Alagoas in 2015 was R$ 77.00, mainly from government contributions (social programs and pensions) and family farming [27, 29].
Population, eligibility criteria, and sample design
The target population for this study was the women from Quilombola communities in Alagoas, aged 19 to 59 years. To obtain the sample size planned for the larger project of which this study is part, 34 of the 68 Quilombola communities in Alagoas state were selected by systematic sampling. The sampling process provided for obtaining a probabilistic sample representative of the families of Quilombola communities in the state [30].
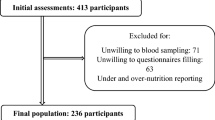
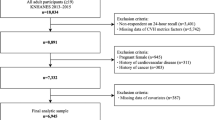
The following eligibility criteria were established for this study: residing in one of the selected quilombola communities and belonging to the target age group. Exclusion criteria were being pregnant or lactating and having consumed alcohol in the last 24 h. Data from women who did not have information to define MetS, as well as those who reported implausible energy intakes (< 400 or > 4800 kcal/day) [31], were excluded from the analysis, given that such values are associated with under- or hyper-reports [32].
With these criteria, a sample of 895 women was obtained. Therefore, the sampling error was calculated a posteriori, considering the following parameters: MetS prevalence of 28.8% [5]; a universe of 6,465 women (estimating the existence of 6,465 Quilombola families in 2015 in Alagoas and assuming that in each household there would be one woman in the target age group); 1.2 for correction of the effect of complex sampling design; and a 95% confidence interval. After the calculations performed in the StatCalc application of the Epi Info 7.2 software (CDC, Atlanta, USA), the sampling error for investigating MetS in this sample was 3.1%.
Data collect
Data collect occurred between April 2017 and January 2018 through interviews conducted during home visits, using structured forms tested in a pilot study. Interviewers were trained to standardize procedures and minimize errors in applying the forms. Demographic, socioeconomic, lifestyle, health, and food consumption variables were collected. All the data were collected at a single opportunity. During the interviews, blood pressure was measured and anthropometric data were collected. The biochemical tests were performed in a predetermined place in each community, to which the women were referred.
The economic class was defined based on the Criterion for Economic Classification Brazil (CCEB), adopted by the Brazilian Association of Research Companies [32], which distinguishes families in classes A, B1, B2, C1, C2, and D + E. This classification is established based on the possession of consumer goods at home, the education of the head of the family, and the infrastructure conditions of the residence. According to a scoring scale, families are classified in descending order, with class D + E being the lowest and class A representing the stratum with the highest economic status [33].
Blood pressure was measured in duplicate with the individual seated after 15 min of rest using Omron® digital devices, model HEM-7200. A third measurement was performed if there was a difference of more than 20 mmHg between the two measurements. A minimum interval of five minutes was established between measurements. For analysis, the most discrepant value was disregarded and the average of the valid values was considered.
The anthropometric variables assessed were body mass index (BMI), neck circumference (NC), waist circumference (WC), and waist-to-height ratio (WHtR). BMI was obtained from weight and height data (kg/m2). The weight was measured using a Seca® model 813 digital scale, with a capacity of up to 200 kg and sensitivity of 100 g, and height was obtained with the use of a Seca® portable stadiometer, model 213, able to measure up to 205 cm. WC and NC were measured with a 150 cm inextensible tape measure and sensitivity to 0.1 cm.
Biochemical tests were performed without prior fasting [34] to define the blood levels of glycated hemoglobin (HbA1C), triglycerides (TG), and high-density lipoprotein cholesterol (HDL). Blood drops obtained by digital puncture with disposable lancets were used. HbA1C was determined using the Alere NycoCard Reader II® (Abbott, USA) device, and HDL and TG were determined using the Alere Cholestech LDX System®.
Variables
The dependents variables were the MetS (defined according to the Joint Interim Statement—JIS harmonization criteria, with adaptation) [35] and its components: (a) Abdominal obesity: WC ≥ 80 cm; (b) Hypertriglyceridemia: TG ≥ 175 mg/dL; (c) Low HDL: HDL < 50 mg/dL; Hypertension: systolic blood pressure ≥ 130 or diastolic blood pressure ≥ 85 mmHg; (e) Diabetes mellitus HbA1C ≥ 6.5 mg/dL, or being under drug treatment for hypertriglyceridemia, hypertension or diabetes. The adaptation consisted of replacing fasting blood glucose, as recommended by the JIS, by using HbA1C as a criterion for the classification of glucose homeostasis, a procedure recommended by the Brazilian Diabetes Society [36]. MetS was defined by the presence of at least three components among those specified in the JIS.
The independent variable was the highest consumption of UPF. We used the 24-h dietary recall (R24h), a method consisting of identifying, through an interview, all the food, and beverages ingested in the previous 24 h. A photographic record album was used to reduce memory bias and to facilitate the quantification of food portions [37]. A single R24h was applied to the study sample.
The quantities of food consumed reported in home measures were converted into grams and milliliters using home measure tables [37,38,39,40]. In the analysis of food nutritional composition, the food composition table of the U.S. Department of Agriculture was used as a base [41]. National reference tables were used for foods belonging to the Brazilian food culture [42,43,44]. According to the Nova classification, consumed foods were divided into four food groups [22]: 1) fresh and minimally processed foods; 2) processed culinary ingredients; 3) processed foods, and 4) UPF. Due to the objective proposed for this study and to have greater clarity in the results, only the ultra-processed group was analyzed as risk exposure, with the lowest consumption used for comparison.
The percentage contribution of the daily energy intake (%/day) of each food group according to the processing degree was obtained by calculating the energy value of each food group by multiplying the value obtained by 100 and dividing the result by the total energy intake of each woman. For the analyses, the percentage of contribution of daily energy intake of the UPF was used (%kcal/day).
In addition, we used the yes-or-no questions about food intake the previous day for 23 UPF subgroups from the Surveillance System of Risk and Protective Factors for Chronic Diseases by Telephone Survey (VIGITEL) questionnaire [45], which makes up the Nova score for UPF intake [46]. Each subgroup of UPF received a score of 0 (did not consume) or 1 (consumed). Since the list of foods in the Nova score is limited, other foods consumed by Quilombola women with characteristics similar to the foods belonging to the protocol originally proposed based on the results of the 2008/2009 Household Budget Survey (POF) were grouped into the subgroups of the list [47].
Covariables
The covariates used to control for possible confounding factors and characterize the sample were:
-
a)
demographic and socioeconomic variables: age (19–29, 30–39, 40–49, and 50–59 years); self-reported skin color (black + brown and different from black + brown); education level in years of study (never studied, 1–4 years, 5–7 years, and ≥ 8 years); marital status (single, married, and widowed/divorced); economic class (A + B + C or D + E); participation in government social programs (yes or no); family income (≤ 1 minimum wage and > 1 minimum wage); employment status (employed or unemployed); food insecurity (yes or no), measured based on the Brazilian Scale of Food Insecurity (EBIA) [48].
-
b)
Lifestyle and health-related variables: alcoholism (yes or no); smoking (yes or no); physical activity level (PAL)—active or sedentary—obtained by applying the International Physical Activity Questionnaire (IPAQ), short version [49]; presence of health problems reported as having occurred in the last 15 days (yes or no).
-
c)
Anthropometric variables: Nutritional status was analyzed according to BMI (kg/m2), considering the overweight category: BMI ≥ 25 kg/m2 (yes or no) [50]. In addition, NC ≥ 34 cm (yes or no) [51] and WHtR ≥ 0.53 (yes or no) [52] were also analyzed and were considered predictors of cardiometabolic diseases.
Data analysis
Data, except for food consumption data, were typed in a double independent entry in the Epi info version 3.5.3 software for data comparison and correction of possible typing errors. The food consumption data were entered in the software Dietpro® Clinico, version 6.0. After completing the first typing stage, all data were checked against the electronic spreadsheet obtained with the physical forms, and, when necessary, typing errors were corrected. After this, the consumption data were exported to Microsoft Excel® software.
Descriptive analyses were performed for all variables. Categorical variables were expressed as absolute and relative frequencies, while for continuous or discrete variables, medians, interquartile ranges, means, and standard deviations were used, according to the distribution normality, evaluated by the Kolmogorov–Smirnov test.
The values of the percentage contribution of daily energy intake according to the degree of food processing were classified according to quartiles into four categories. The 1st quartile (Q1) was considered the lowest or no consumption; the 2nd quartile (Q2) was considered moderate consumption; and the quartiles above the median (Q3 and Q4, respectively) were considered higher consumption. The consumption of UPF was evaluated by comparing Q2, Q3, and Q4 with Q1.
The Nova score of each participant's UPF consumption was calculated by adding the score values of each UPF subgroup consumed among the 23 listed, and this score could range from 0 to 23. In the analysis, the scores were categorized as follows: ≤ 1; 2; 3; ≥ 4. Due to the low frequency observed for values equal to or greater than 4, all of these (4 to 23) were grouped into the fourth category. This category indicates a high UPF intake.
The MetS was compared with the different covariates to observe statistical differences between the categories for which Pearson's χ2 test was used. The crude and adjusted prevalence ratios (PR) with respective 95% confidence intervals (95%CI) were established using Poisson regression with robust variance adjustment. The covariates that presented a significance level of up to 20% (p < 0.2) in the crude model were included in the multivariable analysis. Previously, however, to avoid the problem of multicollinearity, the variables (demographics, socioeconomics, lifestyle, health, and anthropometrics) with the highest correlation (r = 0.7) were identified. According to Pearson's correlation matrix, only the anthropometric variables BMI and WHtR (r = 0.73) presented this characteristic. Thus, only BMI (i.e., overweight—yes or no) was kept in the multivariable analysis.
For the multiple model, three blocks were organized: model 1 (adjusted for demographic and socioeconomic features); model 2 (variables from model 1 with a 5% significance level plus information related to lifestyle and health); and model 3 (variables from models 1 and 2 with a p-value < 0.05 plus anthropometric data). In each analysis level, there was, respectively, successive elimination of non-significant variables (backward stepwise). The final adjusted model was composed of all the variables remaining in model 3.
Statistical analysis was performed in Stata/SE version 12.1 software (StataCorp LP. College Station, TX, USA).
Results
A total of 895 women (38.9 ± 11.0 years) were investigated. The majority (56.0%) belonged to the age group of 30 to 49 years, were black (90.8%), married (79.4%), belonged to the economic class D + E (94.4%), and had less than eight years of schooling (71.0%). Overweight was identified in 69.0% of women (Tables 1 and 2).
The prevalence of MetS was 48.3%. As for the components of MetS, 68.2% had abdominal obesity, 45.0% had hypertension, 28.8% had diabetes, 33.1% had hypertriglyceridemia, and 74.9% had low HDL (Supplementary Table 1).
In the crude analysis, the variables associated with a higher prevalence of MetS were older age, married status, low education, participation in government assistance programs, smoking, being overweight, and high WHtR and WC (Tables 1 and 2). The average energy intake was 1,437.2 kcal (± 627.9 kcal), and of this total, the average percentage contribution from the UPF group was 15.9%. The distribution of energy intake by quartiles is shown in Supplemental Table 2, where it is observed that the mean percentage of contribution of the caloric intake from UPA in relation to the total caloric intake was 40.5%.
Supplemental Table 3 shows the consumption frequency for each of the 23 food subgroups of the Nova score. Five food subgroups were most consumed: packaged snacks (or chips) or saltine crackers (26.0%); margarine (20.2%); sweet biscuits with or without filling (16.5%); powdered drink mix (14.5%); and loaves of bread, like of the hot dogs or hamburgers buns or similar (13.6%).
The Nova score distribution ranged from 0 to 9, and scores ≤ 1 (63.6%) and 2 (21.4%) were more frequent. The percentage of women with a score ≥ 4 (high UPF intake) was 6.3% (Table 3).
The associations of UPF consumption, Nova score, MetS, and its components are described in Tables 3, 4, and 5 (for the adjusted analysis, the variables present in each model are shown in Supplementary Tables 4 and 5).
MetS was not associated with any category of the Nova score. However, in the adjusted analysis of the MetS components, it was observed that a lower Nova score (score 3) reduced the prevalence of diabetes by 44% (Table 4): PR = 0.56; 95%CI: 0.31–0.99; p = 0.046. The lower score was also an independent protective factor for low HDL (PR = 0.90; 95%CI: 0.81–0.99; p = 0.046). Hypertension, abdominal obesity, and hypertriglyceridemia were not associated with any level of the Nova score.
No association with MetS was found related to the percentage energy contribution of UPF consumption (Tables 3 and 5). However, it was found for its components that UPF consumption at a moderate level (Q2) increased hypertension prevalence by 30% (PR = 1.30; 95%CI: 1.06–1.61; p = 0.013) compared to the lowest consumption (Q1). The other components were not associated with UPF consumption (Table 5).
Discussion
Compared to the UPF consumption described in studies conducted in populations belonging to more urbanized settings, we can assume that this eating pattern is less established among Quilombola women. According to data from the Vigitel-2020 survey, the consumption frequency of five or more UPF groups (on the day before the interview) for the population aged > 18 years was 18.5% in all 27 Brazilian capitals, and this frequency was 16.1% for women aged > 18 [53], i.e., approximately 2.5 times higher than for the Quilombola women (considering for these the consumption of 4 or more UPF groups).
It should be noted that the Quilombola women analyzed belong to rural communities that, due to cultural issues, often preserve the eating habits acquired from their ancestors who survived on subsistence agriculture and, thus, had a diet consisting basically of natural foods [54]. Today, however, in addition to these foods, the food practices reported revealing the inclusion of processed and ultra-processed foods in their food culture. This may be related to the difficulties faced in developing agricultural practices and the urbanization of cities with the construction of roads that lead more easily to urban areas [55]. In addition, the younger Quilombola generations have lost their relationship with the land and agriculture; therefore, their access to food has been influenced by the globalization process [56].
Regarding the food consumption of populations that have similarities with that of this study (social vulnerability), research comparing food patterns of white and black Americans found a higher frequency of unhealthy eating patterns (consumption of foods such as sausages, fried foods, refined grains, sugar, margarine, sweets, and fats) among blacks [57]. This observation is similar to what occurs in the Brazilian scenario, as shown by data from the National Health Survey, which show that black individuals and those with low socioeconomic status have a worse dietary profile [58]. In Brazil, this situation is a reflection of the precarious living conditions historically imposed on blacks, being a perverse legacy of the slavery process. As in other countries, in Brazil, the black population has a worse socioeconomic condition compared to whites [58].
Given the above, it is worrying how much UPF is available for commercialization in Quilombola communities. Regarding this issue, Serafim et al. [59], in a study carried out in a city in Brazil, found a higher score of availability of UPF in regions with lower income, a higher percentage of non-white people, and a higher number of residents per household. This finding demonstrates that vulnerable populations, such as the Quilombolas, are having their food consumption influenced by the industry and trade of unhealthy food products, especially UPF, which represents a risk to the health of the population due to its relationship with the development of NCDs [60].
The results regarding the Nova score are the first related to the analysis of its association with chronic diseases. A study with this instrument was conducted with the adult population of the 27 Brazilian state capitals using data from the Vigitel-2019 survey. This study showed that being male, younger, and having a lower level of education were factors associated with higher UPF consumption [61].
This study showed that, although no association was found between MetS and UPF consumption, higher consumption of these foods was related to higher hypertension prevalence. A lower Nova score was also a protective factor against diabetes and low HDL.
However, further studies with the female Quilombola population may be necessary since, due to the cultural and socioeconomic characteristics of Quilombola peoples, there was a low frequency of the higher categories of the Nova score, reducing the statistical power to demonstrate the associations investigated (the percentage of women with a score ≥ 5, previously established in the study by Costa et al. [46], was only 1.7%, considering that the score ranges from 0 to 23). It should be noted that in the present study, a score ≥ 4 was considered a high frequency of consumption.
The result that there was no association between the consumption of ultra-processed foods and MetS, unlike that observed in other studies [17, 19, 62], was similar to that found in a study of Lebanese adults, in which no relationship was found between the “ultra-processed food pattern” and MetS [26]. It is worth noting that although UPF consumption was not associated with MetS, it contributes a considerable percentage of women's energy intake, possibly suggesting a trend to transition from a healthy eating pattern to one of relatively high consumption of UPF pattern.
This study showed that even moderate consumption (Q2) of UPF was associated with hypertension. This result corroborates with the findings of a cohort study conducted in Brazil, where individuals with UPF consumption in the upper fifth of daily energy intake had a higher incidence of this pathology (PR = 1.35; 95%CI: 1.10–11.81) [13].
In our study, in the crude analysis up to level 2 of the multiple analysis, high UPF consumption was observed to be a risk factor for abdominal obesity. However, this association lost significance in the final adjusted model (level 3). A similar fact occurred in a study with young Brazilian adults, where UPF intake was found to be a risk factor for abdominal obesity only in the unadjusted analysis (OR = 1.09; 95% CI: 1.01–1.18) [63]. It is worth noting that level 3 was formed by the anthropometric variables, which present a strong positive correlation with the outcomes analyzed. Obviously, the power of these associations weakens the previous levels' relationships, which cannot always be avoided during the adjustment process because of residual effects that may remain.
Even considering the differences between the populations studied and the results achieved, UPF consumption should be cautiously adopted given the high proportion of artificial ingredients in their formulations [21], which are potentially harmful to health, especially when consumed in excess. There is evidence that excessive consumption of these foods is related to an increase in NCDs, such as obesity, cardiovascular, and metabolic diseases [18, 64,65,66].
This relationship is due to the poor nutritional quality of these foods, most of which are characterized by high saturated fat, trans-fatty acids, refined sugars, little or no fiber, vitamins, and minerals [67, 68].
Regarding abdominal obesity, which plays a central role in the triggering of several NCDs, one of the hypotheses supporting its origin related to UPF consumption concerns the high caloric density of these foods that can delay satiety signals and, as a consequence, larger portions are consumed [68, 69].
It is worth mentioning that this study evaluated African-descent women living in Quilombola communities and subjected to great social vulnerability, institutional racism, and food insecurity [30, 70, 71]. Studies on Quilombola communities are still limited, being this the first regarding the consumption of UPF. Because of these characteristics, this population requires priority attention from the government to correct historical distortions and promote health and quality of life. Such aspects justify the importance of studies that can support these actions' planning and implementation.
In this aspect, the importance of food and nutrition education activities stands out. The encouragement and strengthening of healthy eating habits with increased consumption of fresh foods are important practices for preventing MetS and other NCDs [13, 72].
There are few studies that, using the Nova classification, evaluated the relationship between the level of food processing and MetS. Proof of this can be seen in the fact that in a systematic review conducted by Santos et al. [73], only two studies addressing this issue were included. In addition to the studies included in the aforementioned review, later publications by Martinez-Perez et al. [74] and Phillips et al. [75] also investigated the association between UPF and cardiometabolic markers. However, none of them used the Nova score and its association with MetS.
The cross-sectional design is a limitation of this study because of the possible temporality bias. Another limitation concerns the application of a single R24h. Thus, the food consumption data cannot reflect the usual consumption of the women assessed. However, it is noteworthy that several other studies also used a single R24h to assess food intake [26, 52, 76]. In addition, the inclusion of only women in the sample of the present study can be considered another limiting factor. However, it is noteworthy that women influence the composition of family food [77], being considered as the main ones responsible for promoting the food security of their families [78]. The non-inclusion of males in our survey was defined due to two situations: (a) Household surveys are carried out on different days of the week and, almost always, men are not at home, but at their workplaces; (b) In a much higher proportion than other family members, men refuse to participate in the study.
The strengths of the work include the unprecedented nature of the study and the use of a representative sample of a specific population recognized as a priority in the research agenda of the Ministry of Health [79]. It is the first to use the Nova score of UPF consumption in a Quilombola population. Calibrated instruments, anthropometric techniques, and standardized laboratory tests were adopted for the suitable definition of exposure and outcome. Confounding factors were controlled for using hierarchical multiple analysis. We used the Nova classification (in addition to the Nova score of UPF consumption), which is appropriate and recommended worldwide for developing research and policies on food, nutrition, and public health [80,81,82]. With all these characteristics, the study presents internal and external validity, so that the results can be extrapolated to Quilombola populations in other Brazilian states.
It is worth pointing out that the results presented are relevant for a greater understanding of the Quilombola population's eating habits and their relationship to health, despite being carried out only with women, and may represent the practices of other residents, since women, who are mainly responsible for managing the food in the home, play a key role in shaping the family's eating habits.
Conclusion
The highest UPF consumption was positively associated with the prevalence of hypertension, while a lower Nova score was a protective factor against diabetes and low HDL.
UPF consumption in quilombola communities is important but still lower than that observed in the Brazilian population in general.
It is suggested that public health programs be implemented to promote healthy eating while valuing the existing eating habits and traditions among the remaining Brazilian Quilombola people.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- 95% CI:
-
95% Confidence intervals
- BMI:
-
Body Mass Index
- CECB:
-
Criterion for Economic Classification Brazil
- EBIA:
-
Brazilian Scale of Food Insecurity
- HbA1C:
-
Glycated hemoglobin
- HDI:
-
Human Development Index
- HDL:
-
High-density lipoprotein cholesterol
- IPAQ:
-
International Physical Activity Questionnaire
- JIS:
-
Joint Interim Statement
- MetS:
-
Metabolic syndrome
- NC:
-
Neck circumference
- NCDs:
-
Chronic non-communicable diseases
- OR:
-
Odds ratio
- PAL:
-
Physical activity level
- POF:
-
Household Budget Survey
- PR:
-
Prevalence ratio
- Q1:
-
1st quarter
- Q2:
-
2nd quarter
- Q3:
-
3rd quarter
- Q4:
-
4th quarter
- R24h:
-
24-hour dietary recall
- TG:
-
Triglycerides
- UPF:
-
Ultra-processed food
- VIGITEL:
-
Surveillance system of risk and protective factors for chronic diseases by telephone survey
- WC:
-
Waist circumference
- WHtR:
-
Waist-to-height ratio
References
Desroches SD, Lamarche BL. The evolving definitions and increasing prevalence of the metabolic syndrome. Appl Physiol Nutr Metab. 2007;32:23–32. Available from: https://doi.org/10.1139/h06-095.
Dragsbæk K, Neergaard JS, Laursen JM, Hansen HB, Christiansen C, Beck-Nielsen H, et al. Metabolic syndrome and subsequent risk of type 2 diabetes and cardiovascular disease in elderly women. Med. 2016;95:e4806. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5023917/. Cited 22 July 2021.
Harrison S, Couture P, Lamarche B. Diet Quality, Saturated Fat and Metabolic Syndrome. Nutrients. 2020;12:3232. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7690379/. Cited 14 Mar 2021.
Ranasinghe P, Mathangasinghe Y, Jayawardena R, Hills AP, Misra A. Prevalence and trends of metabolic syndrome among adults in the asia-pacific region: a systematic review. BMC Public Health. 2017;17:101. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5251315/. Cited 22 July 2021.
Mussi RF de F, Petróski EL. Metabolic syndrome and associated factors in quilombolas (inhabitants of black communities) from Bahia, Brazil. Cien Saude Colet. Abrasco - Associação Brasileira de Saúde Coletiva; 2019;24:2481–90. Available from: http://www.scielo.br/j/csc/a/sBzZtKwxNCyXjYvw9Cxpwnb/?lang=pt. Cited 14 Aug 2021.
Aragão JA, Bós ÂJG, Souza GC. Síndrome metabólica em adultos e idosos de comunidades quilombolas do centro-sul do Piauí, Brasil. Estud Interdiscip sobre o Envelhec. 2014;19. Available from: https://seer.ufrgs.br/RevEnvelhecer/article/view/41851. Cited 23 May 2021.
World Health Organization. Noncommunicable diseases country profiles 2018. World Health Organization; 2018.
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–60. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)61766-8/abstract. Cited 14 Mar 2021.
World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020. 2013. Available from: https://www.who.int/nmh/publications/ncd-action-plan/en/. cited 14 Mar 2021.
Popkin BM. The nutrition transition and its health implications in lower-income countries. Public Health Nutr. 1998;1:5–21.
Laudan R. A Plea for Culinary Modernism: Why We Should Love New, Fast, Processed Food. Gastronomica. 2001;1:36–44. Available from: https://online.ucpress.edu/gastronomica/article/1/1/36/93394/A-Plea-for-Culinary-Modernism-Why-We-Should-Love. Cited 14 Mar 2021.
Dwyer JT, Fulgoni VL, Clemens RA, Schmidt DB, Freedman MR. Is “Processed” a Four-Letter Word? The Role of Processed Foods in Achieving Dietary Guidelines and Nutrient Recommendations. Adv Nutr. 2012;3:536–48. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3649724/. Cited 14 Mar 2021.
Rezende-Alves K, Hermsdorff HHM, Miranda AE da S, Lopes ACS, Bressan J, Pimenta AM. Food processing and risk of hypertension: Cohort of Universities of Minas Gerais, Brazil (CUME Project). Public Health Nutr. 2021;24:4071–9
Canella DS, Levy RB, Martins APB, Claro RM, Moubarac J-C, Baraldi LG, et al. Ultra-processed food products and obesity in Brazilian households (2008–2009). PLoS ONE. 2014;9: e92752.
Mendonça RD, Lopes ACS, Pimenta AM, Gea A, Martinez-Gonzalez MA, Bes-Rastrollo M. Ultra-Processed Food Consumption and the Incidence of Hypertension in a Mediterranean Cohort: The Seguimiento Universidad de Navarra Project. Am J Hypertens. 2017;30:358–66. Available from: https://doi.org/10.1093/ajh/hpw137. Cited 15 Feb 2021.
Fiolet T, Srour B, Sellem L, Kesse-Guyot E, Allès B, Méjean C, et al. Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ. 2018;360: k322.
Tavares LF, Fonseca SC, Garcia Rosa ML, Yokoo EM. Relationship between ultra-processed foods and metabolic syndrome in adolescents from a Brazilian Family Doctor Program. Public Health Nutr. 2012;15:82–7.
Martínez Steele E, Juul F, Neri D, Rauber F, Monteiro CA. Dietary share of ultra-processed foods and metabolic syndrome in the US adult population. Prev Med. 2019;125:40–8.
Louzada MLC, Martins APB, Canella DS, Baraldi LG, Levy RB, Claro RM, et al. Impacto de alimentos ultraprocessados sobre o teor de micronutrientes da dieta no Brasil. Rev Saude Publica. 2015;49. Available from: http://www.scielo.br/scielo.php?script=sci_abstract&pid=S0034-89102015000100238&lng=en&nrm=iso&tlng=pt. Cited 15 Feb 2021.
Monteiro CA, Levy RB, Claro RM, Castro IRR, Cannon G. A new classification of foods based on the extent and purpose of their processing. Cad Saúde Pública. 2010;26:2039–49. Available from: http://www.scielo.br/j/csp/a/fQWy8tBbJkMFhGq6gPzsGkb/?lang=en. Cited 5 Aug 2021.
Brasil, Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. Guia alimentar para a população brasileira. Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica, editors. Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica; 2014.
Monteiro CA, Cannon G, Levy RB, Moubarac J-C, Jaime P, Martins AP, et al. NOVA. The star shines bright Food classification. Public health. World Nutr. 2016. p. 28–40.
Menegassi B, Almeida JB, Olimpio MYM, Brunharo MSM, Langa FR. A nova classificação de alimentos: teoria, prática e dificuldades. Cien Saude Colet. ABRASCO - Associação Brasileira de Saúde Coletiva; 2018;23:4165–76. Available from: http://www.scielo.br/j/csc/a/8HKxqkyGm7YBRdDKxVWcCLj/?lang=pt. Cited 16 Jun 2022.
Barbosa LD, Sousa LKM, Schott E, Rezende FAC, Ribeiro AQ, Priore SE, et al. Household availability of food based on the new classification of food and nutritional (in)security. Cien Saude Colet. ABRASCO - Associação Brasileira de Saúde Coletiva; 2020;25:2701–9. Available from: http://www.scielo.br/j/csc/a/9WkzGxy36TjHW6MDG9D9g9D/?lang=pt. Cited 26 Aug 2021.
Martins APB, Levy RB, Claro RM, Moubarac JC, Monteiro CA. Increased contribution of ultra-processed food products in the Brazilian diet (1987–2009). Rev Saude Publica. Faculdade de Saúde Pública da Universidade de São Paulo; 2013;47:656–65. Available from: http://www.scielo.br/j/rsp/a/VxDyNppnrq8vv6jQtZfSsRP/?lang=en. Cited 26 Aug 2021.
Nasreddine L, Tamim H, Itani L, Nasrallah MP, Isma’eel H, Nakhoul NF, et al. A minimally processed dietary pattern is associated with lower odds of metabolic syndrome among Lebanese adults. Public Health Nutr. 2018;21:160–71. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5729841/. Cited 15 Feb 2021.
Alagoas. Estudo Sobre as Comunidades Quilombolas de Alagoas. SEPLAG, editor. Maceió: Secretaria de Estado do Planejamento, Gestão e Patrimônio/SEPLAG; 2015.
Instituto de Pesquisa Econômica Aplicada, Programa das Nações Unidas para o Desenvolvimento, Fundação João Pinheiro. Radar IDHM : evolução do IDHM e de seus índices componentes no período de 2012 a 2017. FJP, IPEA, PNUD, editors. Brasília: IPEA: PNUD: FJP; 2019.
Instituto Brasileiro de Geografia e Estatística. Alagoas/Cidades e Estados. 2021. Available from: https://www.ibge.gov.br/cidades-e-estados/al.html. Cited 1 Jun 2021.
Ferreira HS, Soares ML, Krakauer NY, Santos EA, Krakauer JC, Uchôa TC, et al. What is the best anthropometric predictor for identifying higher risk for cardiovascular diseases in afro-descendant Brazilian women? A cross-sectional population-based study. Am J Hum Biol. John Wiley & Sons, Ltd; 2021;e23652. Available from: https://doi.org/10.1002/ajhb.23652. Cited 26 Aug 2021.
Mattei J, McClain AC, Falcón LM, Noel SE, Tucker KL. Dietary acculturation among puerto rican adults varies by acculturation construct and dietary measure. J Nutr. 2018;148:1804–13.
Castro MA, Baltar VT, Marchioni DM, Fisberg RM. Examining associations between dietary patterns and metabolic CVD risk factors: a novel use of structural equation modelling. Br J Nutr. 2016;115:1586–97. Available from: https://www.cambridge.org/core/product/identifier/S0007114516000556/type/journal_article.
Associação Brasileira de Empresas de Pesquisa - ABEP. Classificação Econômica Brasil: Associação Brasileira de Empresas de Pesquisa. 2016. Available from: https://www.abep.org/criterio-brasil. Cited 22 July 2021.
Faludi AA, Izar MCO, Saraiva JFK, Chacra APM, Bianco HT, Afiune A, et al. Atualização da Diretriz Brasileira de Dislipidemias e Prevenção da Aterosclerose – 2017. Arq Bras Cardiol. 2017;109:1–76.
Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Circulation. Circulation; 2009;120:1640–5. Available from: https://doi.org/10.1161/CIRCULATIONAHA.109.192644. Cited 26 Aug 2021.
Sociedade Brasileira Brasileira de Diabetes. Diretrizes da Sociedade Brasileira de Diabetes 2019–2020. Editora Clannad; 2019.
Monteiro JP, Pfrimer K, Tremeschin MH, Molina MC, Chiarello P, Vannucchi H. Consumo Alimentar: Visualizando Porções. 1a ed. Editora Guanabara Koogan; 2007.
Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares 2008–2009 - Tabela de Medidas Referidas para os Alimentos Consumidos no Brasil. 2011.
Magalhães SG, Rodrigues EL. Fichas de Preparações e Análise do Valor Nutricional. 1st ed. Rubio; 2015.
Pinheiro ABV, Lacerda EM, Benzecry EH, Gomes MCS. Tabela para avaliação de consumo alimentar em medidas caseiras. 5a edição. Editora Atheneu; 2008.
US Department of Agriculture. Agricultural Research Service. utrient Data Laboratory. USDA National Nutrient Database for Standard Reference, Release 28. US Department of Agriculture- Agricultural Research Service; 2016.
Philippi ST. Tabela de composição de alimentos: suporte para decisão nutricional. 6a edição. Editora Manole; 2017.
Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares 2008–2009: Tabelas de Composição Nutricional dos Alimentos Consumidos no Brasil. 2011.
Tabela Brasileira de Composição de Alimentos - TACO. NEPA – UNICAMP; 2011.
Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis. Vigitel Brasil 2018: população negra: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas para a popula. Brasiília: Ministério da Saúde; 2019. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2018_populacao_negra.pdf. Cited 31 Oct 2021.
Costa CDS, Faria FR, Gabe KT, Sattamini IF, Khandpur N, Leite FHM, et al. Nova score for the consumption of ultra-processed foods: description and performance evaluation in Brazil. Rev Saude Publica Univ Saopaulo. 2021;55:1–9.
Instituto Brasileiro de Geografia e Estatística. Pesquisa de orçamentos familiares 2008–2009 : análise do consumo alimentar pessoal no Brasil. Rio de Janeiro, RJ: Instituto Brasileiro de Geografia e Estatística - IBGE; 2011.
Segall-Corrêa AM, Marin-León L, Melgar-Quiñonez H, Pérez-Escamilla R. Refinement of the Brazilian Household Food Insecurity Measurement Scale: Recommendation for a 14-item {EBIA}. Rev Nutr. 2014;27:241–51. Available from: http://www.scielo.br/j/rn/a/X9vkr9sc7WX8tH8dcWP8XPN/?lang=en. Cited 22 July 2021.
Matsudo S, Araújo T, Matsudo V, Andrade D, Andrade E, Oliveira LC, et al. Questionário Internacional de Atividade Física (IPAQ): estudo de validade e reprodutibilidade no Brasil. Rev Bras Atividade Física Saúde. 2001;6:5–18. Available from: https://rbafs.org.br/RBAFS/article/view/931. Cited 6 Aug 2021.
World Health Organization. Physical status : the use of and interpretation of anthropometry , report of a WHO expert committee. World Health Organization; 1995.
Busnello FM, Bodanese LC, Pellanda LC, Santos ZE de A. Nutritional intervention and the impact on adherence to treatment in patients with metabolic syndrome. Arq Bras Cardiol. 2011;97:217–24. Available from: http://www.scielo.br/j/abc/a/jwTMPJRpqpzdwWnWHGSFHkf/?lang=pt. Cited 22 July 2021.
Pitanga FJG, Lessa I. Razão cintura-estatura como discriminador do risco coronariano de adultos. Rev Assoc Med Bras. 2006;52:157–61. Available from: http://www.scielo.br/j/ramb/a/G98ddhYv6xnk9WWzcTYMxDs/?lang=pt. Cited 22 July 2021.
Brasil. Vigitel Brasil 2020 : vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico : estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados. Ministério da Saúde, editor. Brasiília: Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças Não Transmissíveis.; 2021. Available from: www.saude.gov.br/svs.
Furtado MB, Pedroza RLS, Alves CB. Cultura, identidade e subjetividade quilombola: uma leitura a partir da psicologia cultural. Psicol Soc. Associação Brasileira de Psicologia Social; 2014;26:106–15. Available from: http://www.scielo.br/j/psoc/a/7m7spDq5Xm6vNYFqmh89X7g/?lang=pt. Cited 30 Oct 2021.
Cordeiro MM, Monego ET, Martins KA. Overweight in Goiás’quilombola students and food insecurity in their families. Rev Nutr. Pontifícia Universidade Católica de Campinas; 2014;27:405–12. Available from: http://www.scielo.br/j/rn/a/XCxnMQmVCb77QyvQzxNyFPk/abstract/?lang=pt. Cited 30 Oct 2021.
Gubert MB, Segall-Corrêa AM, Spaniol AM, Pedroso J, Coelho SEAC, Pérez-Escamilla R. Household food insecurity in black-slaves descendant communities in Brazil: has the legacy of slavery truly ended? Public Health Nutr. 2017;20:1513–22. Available from: https://www.cambridge.org/core/journals/public-health-nutrition/article/household-food-insecurity-in-blackslaves-descendant-communities-in-brazil-has-the-legacy-of-slavery-truly-ended/486C22F7D836B6ECBCB16BC3AD61F98D. Cited 20 May 2021.
Judd SE, Gutiérrez OM, Newby P, Howard G, Howard VJ, Locher JL, et al. Dietary patterns are associated with incident stroke and contribute to excess risk of stroke in Black Americans. Stroke. NIH Public Access; 2013;44:3305. Available from: https://doi.org/10.1161/STROKEAHA.113.002636. Cited 6 Nov 2021.
Medina L de PB, Barros MB de A, Sousa NF da S, Bastos TF, Lima MG, Szwarcwald CL. Desigualdades sociais no perfil de consumo de alimentos da população brasileira: Pesquisa Nacional de Saúde, 2013. Rev bras epidemiol. Medina, Lhais de Paula Barbosa; Universidade Estadual de Campinas. Faculdade de Ciências Médicas. Departamento de Saúde Coletiva. Campinas. BR; 2019;22:E190011.SUPL.2-E190011.SUPL.2. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&.
Serafim P, Borges CA, Cabral-Miranda W, Jaime PC. Ultra-Processed Food Availability and Sociodemographic Associated Factors in a Brazilian Municipality. Front Nutr. 2022;9. Available from: https://www.frontiersin.org/articles/10.3389/fnut.2022.858089/full.
Organização Pan-Americana da Saúde. Marco de Referência sobre a Dimensão Comercial dos Determinantes Sociais da Saúde na Agenda de Enfrentamento das Doenças Crônicas Não Transmissíveis. Brasília, D.F; 2020. Available from: https://iris.paho.org/handle/10665.2/52975.
Costa CD, Sattamini IF, Steele EM, Louzada ML, Claro RM, Monteiro CA. Consumption of ultra-processed foods and its association with sociodemographic factors in the adult population of the 27 Brazilian state capitals (2019). Rev Saude Publica. Faculdade de Saúde Pública da Universidade de São Paulo; 2021;55:1–9. Available from: http://www.scielo.br/j/rsp/a/Vxw8tqZHMbWHDGm6Qb5KDWn/abstract/?lang=pt. Cited 15 Dec 2021.
Lavigne-Robichaud M, Moubarac J-C, Lantagne-Lopez S, Johnson-Down L, Batal M, Laouan Sidi EA, et al. Diet quality indices in relation to metabolic syndrome in an Indigenous Cree (Eeyouch) population in northern Québec. Canada Public Heal Nutr. 2018;21:172–80.
Santana GJ, Silva NJ, Costa JO, Vásquez CMP, Vila-Nova TMS, Vieira DAS, et al. Contribution of minimally processed and ultra-processed foods to the cardiometabolic risk of Brazilian young adults: a cross-sectional study. Nutr Hosp. Sociedad Española de Nutrición Parenteral y Enteral (SENPE); 2021;38:328–36. Available from: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0212-16112021000200328&lng=es&nrm=iso&tlng=en. Cited 16 Dec 2021.
Silva DCG da, Ferreira FG, Pereira DLM, Magalhães ELG de, Longo GZ, Silva DCG da, et al. Degree of food processing and its relationship with overweight and body adiposity in Brazilian adults. Rev Nutr. 2021;34. Available from: http://www.scielo.br/scielo.php?script=sci_abstract&pid=S1415-52732021000100304&lng=en&nrm=iso&tlng=en. Cited 16 Feb 2021.
Moreira PVL, Hyseni L, Moubarac J-C, Martins APB, Baraldi LG, Capewell S, et al. Effects of reducing processed culinary ingredients and ultra-processed foods in the Brazilian diet: a cardiovascular modelling study. Public Health Nutr. 2018;21:181–8. Available from: https://www-cambridge.ez9.periodicos.capes.gov.br/core/journals/public-health-nutrition/article/effects-of-reducing-processed-culinary-ingredients-and-ultraprocessed-foods-in-the-brazilian-diet-a-cardiovascular-modelling-study/1E73F7D594B55B8915481B5F0CB8. Cited 15 Feb 2021.
Sung H, Park JM, Oh SU, Ha K, Joung H. Consumption of Ultra-Processed Foods Increases the Likelihood of Having Obesity in Korean Women. Nutrients. 2021;13:698. Available from: https://www.mdpi.com/2072-6643/13/2/698. Cited 22 July 2021.
Organização Pan-Americana da Saúde. Alimentos e bebidas ultraprocessados na América Latina: Tendências, impacto sobre a obesidade, implicações políticas. Brasília, D.F: OPAS- Organização Pan-Americana da Saúde; 2018.
Sandoval-Insausti H, Jiménez-Onsurbe M, Donat-Vargas C, Rey-García J, Banegas JR, Rodríguez-Artalejo F, et al. Ultra-Processed Food Consumption Is Associated with Abdominal Obesity: A Prospective Cohort Study in Older Adults. Nutrients. Multidisciplinary Digital Publishing Institute (MDPI); 2020;12:1–11. Available from: https://doi.org/10.3390/nu12082368. Cited 16 Dec 2021.
Monteiro CA, Cannon G, Moubarac JC, Levy RB, Louzada MLC, Jaime PC. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. Public Health Nutr; 2018;21:5–17. Available from: https://pubmed.ncbi.nlm.nih.gov/28322183/. Cited 16 Dec 2021.
Ferreira HS, Silva WO, Santos EA, Bezerra MKA, Silva BCV, Horta BL. Body composition and hypertension: a comparative study involving women from maroon communities and from the general population of Alagoas State, Brazil. Rev Nutr. Pontifícia Universidade Católica de Campinas; 2013;26:539–49. Available from: http://www.scielo.br/j/rn/a/Y4vYPSyQXt88vD4bSZM78qc/?lang=en. Cited 10 Jan 2022.
Silva EKP, Medeiros DS, Martins PC, Almeida Sousa L, Lima GP, Rêgo MAS, et al. Insegurança alimentar em comunidades rurais no Nordeste brasileiro: faz diferença ser quilombola? Cad Saude Publica [Internet]. Escola Nacional de Saúde Pública Sergio Arouca, Fundação Oswaldo Cruz; 2017;33. Available from: http://www.scielo.br/j/csp/a/XmQMNwcCT8jPq5gp36Jv7pF/?lang=pt. Cited 10 Jan 2022.
Melo ISV, Costa CA, Santos JV, Santos AF, Florêncio TM, Bueno NB. Consumption of minimally processed food is inversely associated with excess weight in adolescents living in an underdeveloped city. PLoS One. 2017;12:e0188401. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5708826/. Cited 22 July 2021.
Santos FS, Dias MS, Mintem GC, Oliveira IO, Gigante DP, Santos FS, et al. Food processing and cardiometabolic risk factors: a systematic review. Rev Saude Publica. 2020;54. Available from: http://www.scielo.br/scielo.php?script=sci_abstract&pid=S0034-89102020000100507&lng=en&nrm=iso&tlng=pt. Cited 16 Feb 2021.
Martinez-Perez C, San-Cristobal R, Guallar-Castillon P, Martínez-González MÁ, Salas-Salvadó J, Corella D, et al. Use of Different Food Classification Systems to Assess the Association between Ultra-Processed Food Consumption and Cardiometabolic Health in an Elderly Population with Metabolic Syndrome (PREDIMED-Plus Cohort). Nutrients. 2021;13. Available from: https://www.mdpi.com/2072-6643/13/7/2471.
Phillips NE, Mareschal J, Schwab N, Manoogian ENC, Borloz S, Ostinelli G, et al. The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults. Nutrients. 2021;13.
Evans EW, Lipton RB, Peterlin BL, Raynor HA, Thomas JG, O’Leary KC, et al. Dietary Intake Patterns and Diet Quality in a Nationally Representative Sample of Women With and Without Severe Headache or Migraine. Headache. 2015;55:550–61. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4443434/. Cited 4 Mar 2021.
Pereira RA, Andrade RG, Sichieri R. Mudanças no consumo alimentar de mulheres do Município do Rio de Janeiro, Brasil, 1995–2005. Cad Saude Publica. 2009;25:2419–32. Available from:http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2009001100012&lng=pt&tlng=pt.
Lima AC, Lima RSV, Silva JMA. Gênero feminino, contexto histórico e segurança alimentar. Demetra Aliment Nutr Saúde. 2016;11:789–802. Available from: http://www.e-publicacoes.uerj.br/index.php/demetra/article/view/22511.
Brasil. Ministério da Saúde. Agenda de Prioridades de Pesquisa do Ministério da Saúde - APPMS. Brasília: Ministério da Saúde, Secretaria de Ciência, Tecnologia e Insumos Estratégicos, Departamento de Ciência e Tecnologia; 2018. p. 26. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/agenda_prioridades_pesquisa_ms.pdf.
Food and Agriculture Organization of the United Nations- FAO. Guidelines on the Collection of Information on Food Processing through Food Consumption Surveys. FAO; 2015. Available from: http://www.fao.org/documents/card/en/c/a7e19774-1170-4891-b4ae-b7477514ab4e/. Cited 31 July 2021.
PAHO - Pan American Health Organization. Ultra-processed food and drink products in Latin America: Trends, impact on obesity, policy implications. PAHO; 2015.
Rauber F, Steele EM, Louzada MLC, Millett C, Monteiro CA, Levy RB. Ultra-processed food consumption and indicators of obesity in the United Kingdom population (2008–2016). PloS One. 2020;15:e0232676. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0232676. Cited 31 July 2021.
Funding
This study was funded by the Brazilian National Council of Technological and Scientific Development—CNPq (Grant No. 466718/2014–4) and the Foundation for Research Support of the State of Alagoas—Fapeal (Grant No. 60030.000849/2016). The views expressed in the present article are those of the authors and not necessarily those of any funding agencies. The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conceptualisation and the design of the project. LBB managed the dataset, analysed the data, and was a major contributor in writing the manuscript with critical revisions and guidance from HSF, who was also responsible for obtaining financial support. NBRV, EAS, TRS, TAS. and HSF contributed to the analysis and interpretation of data and drafting of the article. All authors reviewed and approved the final version of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is part of a project entitled "Diagnosis of Health and Food and Nutritional Security of the Families of the Remaining Quilombo Communities in the State of Alagoas", which was approved by the Research Ethics Committee of the Federal University of Alagoas (CAAE 33527214.9.0000.5013). All women analyzed agreed to participate in the study and signed the Informed Consent Form.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Distribution of the metabolic syndrome according to the categories of its components in quilombola women from Alagoas, Brazil, 2018. Supplementary Table 2. Mean total energy intake and absolute and relative contribution of this intake that was derived from ultra-processed foods. Supplementary Table 3. Percent distribution of the consumption, on the day before the interview, of food groups included in the Nova score of consumption of ultra-processed foods by Quilombola women in Alagoas, Brazil, 2018. Supplementary Tables 4. Description of the covariates (confounding factors) controlled in the adjusted analysis of table 4, according to the outcome evaluated. Supplementary Tables 5. Description of the covariates (confounding factors) controlled in the adjusted analysis of Table 5, according to the outcome evaluated.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Barbosa, L.B., Vasconcelos, N.B.R., dos Santos, E.A. et al. Ultra-processed food consumption and metabolic syndrome: a cross-sectional study in Quilombola communities of Alagoas, Brazil. Int J Equity Health 22, 14 (2023). https://doi.org/10.1186/s12939-022-01816-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12939-022-01816-z