
Abstract
Objective
To investigate the effect of additional semiautomatic intermittent pneumatic compression device (IPCD) in the prevention of deep vein thrombosis (DVT) of lower extremity in these patients undergoing major orthopedic surgery, when compared with the conventional graduated compression stockings alone.
Methods
The data of 112 patients undergoing major orthopedic surgery were retrospectively analyzed. 51 patients who ever received IPCD and graduated compression stockings during major orthopedic surgery were taken as the experimental group, and 61 patients who only received the conventional graduated compression stockings during surgery were taken as the observation group. The Doppler sonography was utilized to detect the presence of DVT and pulmonary embolism pre- and postoperatively. Besides, the mean and peak velocity of blood flow in femoral vein were recorded before and after surgery. And then, the comparisons between the two groups were made, respectively.
Results
When compared with the conventional graduated compression stockings alone, the intraoperative application of IPCD and stockings contributed the significant reduction of DVT (3.92%, 2/51 versus 9.84%, 6/61, X2 = 5.632, P = 0.034). In terms of the mean and peak velocity of blood flow in femoral vein, the postoperative difference was higher in the observation group than those in the control group (149.56 ± 26.35 versus 130.15 ± 22.56 mm/s, P < 0.05). With respect to perioperative blood loss, the difference between the two groups was statistically significant (800.5 ± 320.7 versus 950.1 ± 305.9 ml, P = 0.031).
Conclusions
Intraoperative application of IPCD could promote blood circulation of lower limbs, and significantly decrease the incidence of potentially fatal DVT in patients undergoing major orthopedic surgery, when compared with the conventional graduated compression stockings.
Similar content being viewed by others

Background
In general, the major orthopedic surgery includes total hip arthroplasty (THA), total knee arthroplasty (TKA), and hip fraction surgery (HFS), which are associated with significant morbidity and mortality, and are especially attributable to the high risk of postoperative venous thromboembolism, on account of excessive production of procoagulants, perioperative immobilization and cement polymerization, etc. [1,2,3,4,5]. During and after major orthopedic surgery, the risk of venous thromboembolism approximates 50–80%, and might persist for up 3 to 6 months after surgery [6]. According to the risk classification of venous thromboembolism in patients undergoing orthopedic surgery, these patients with major orthopaedic surgery are at high risk of deep vein thrombosis (DVT) [7, 8]. And, DVT refers to the abnormal coagulation of blood in the deep veins and obstruction of vein lumen, thereby leading to the blockage of venous return. Additionally, being regarded as a serious and even life-threatening complication, DVT mostly occurs in the lower extremities [9,10,11]. It can not only transform into chronic vascular diseases, affect life quality of patients, but also lead to fateful pulmonary embolism. In addition, on the basis of previous literatures, after the confirmation of venous angiography, the incidences of DVT after THA and TKA without preventive measures was 42% to 57% and 41% to 85%, respectively, and the incidence of DVT after HFS was 45–70% [12,13,14]. Therefore, when compared with other patients, it is more necessary to prevent DVT in patients who ever undergo major orthopedic surgeries [15, 16].
At present, the preventive measures for perioperative DVT in major orthopedic surgery mainly include drug and physical treatment. And, the commonly utilized physical measures are intermittent pneumatic compression device (IPCD), graduated compression stockings (GCS), and plantar vein pumps, etc. These physical treatment can be used alone or combined with drugs. Although the anticoagulant drugs including heparin, coumarins, and fondaparinux, can effectively prevent DVT of lower extremities, it can also increase the bleeding risk. It is not suitable for patients with high bleeding risk. Once the severe bleeding occurs, it is often more intractable than DVT in the lower extremities. In addition, the critically ill patients are generally in critical condition and have relatively high bleeding risk, so they are not suitable for general anticoagulant therapy. The common physical measures include IPCD, gradient elastic stockings, plantar vein pumps, etc. Currently, they can be used alone or as an auxiliary measure for drug prevention, and are an important strategies for DVT prevention [17]. Specifically, IPCD can be considered as one common mechanical precaution for DVT in clinical practice [18, 19]. As far as we are concerned, IPCD is a engineering device that uses external mechanical force to compress the veins of lower extremities and promote blood return, which can effectively prevent the occurrence of DVT [20]. In this research, the authors aimed to investigate the therapeutic effect of intermittent pneumatic compression device in preventing DVT of lower extremity in these patients who ever underwent major orthopedic surgery, and we reported the detailed information as followed.
Patients
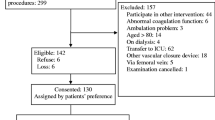
From March 2016 to February 2018, 112 patients who ever underwent major orthopedic surgeries were eligible. The patients who had DVT in lower extremities, life-threatening patients, and patients with APACHE (Acute Physiology and Chronic Health) score ≧ 20 points, the patients suffering from lower extremity lesions could not received IPCD or graduated compression stockings were excluded. Besides, the other exclusion criteria are as follows. (1) age < 18 years; (2) abnormal blood coagulation; (3) combines with heart function ≤ Level 3; (4) chronic renal failure ≥ 3 phase; (5) severe peripheral arterial disease; (6) Acute thrombophlebitis; (7) Neurological diseases of lower limbs; (8) Joint stiffness of lower limbs; (9) Recently received anticoagulant therapy; (10) History of bleeding disorders or malignancy; (11) Allergic to heparin. (12) unavailability of either pre- or postoperative Doppler sonography. On account of lack of pre- or postoperative Doppler sonography, 24 patients were excluded.
After rigorous process of selection, the data of 112 patients undergoing major orthopedic surgery were retrospectively analyzed. 51 patients who ever received IPCD and stockings during major orthopedic surgery were taken as the experimental group, and 61 patients who only received the conventional graduated compression stockings during surgery were taken as the observation group. In the experimental group, there were 29 males and 22 females, the age ranged from 38 to 79 years old, and the average age was 55.6 ± 14.2 years old. 18 cases underwent hip replacement, 12 cases underwent knee replacement, 21 cases underwent fracture surgical treatment. In the control group, there were 36 males and 25 females, the age ranged from 35 to 81 years old, and the average age was 50.6 ± 19.2 years old. 22 cases underwent hip replacement, 15 cases underwent knee replacement, 24 cases underwent fracture surgical treatment. The differences in gender composition, age distribution, and types of diseases between the two groups were not statistically significant (P > 0.05). The baseline characteristics are displayed in Table 1.
Methods
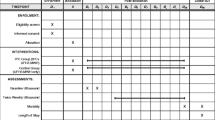
All these selected patients received routinely anticoagulant therapy via intraperitoneal injection (Fraxiparine, 0.4 ml, GlaxoSmithKline) at 12 h before surgery or 10 h after surgery, and then repeated every 24 h until 10 days after surgery. In the experimental group, the patients received IPCD (SCDTM system, Kendal, America) and additional stockings during major orthopedic surgery. And the detailed procedures are described as follows. First of all, the patients were required to wear the graduated compression stockings before operation. Secondly, the patients started to receive IPCD treatment in the non-surgical side once the anesthesia beginned, and then receive bilateral IPCD treatment after operation. On the first postoperative day, continuous use was required for 24 h. Afterwards, the patients could use it several times one day, but should ensure that the total daily use time is 6–8 h. All these patients used IPC until 10 days after surgery, regardless of whether they could be able to get out of bed. By means of a standard air pulse generator, the standard thromboprophylaxis mode was maintained throughout the complete procedure until extubation. And, these were intermittently inflated to a maximum pressure of 45 mm Hg. In particular, the sequential compression which is used once every minute refers to inflate distal chambers fist, then continue to the more proximal chambers in a wavelike.
The Doppler sonography (Sonoline Antares, Siemens Sector Healthcare) was utilized to detect the presence of DVT and pulmonary embolism pre- and postoperatively, and this performance was carried out by the same examiner who has the professional certification and was blinded to the group status of all patients. Besides, the mean and peak velocity of blood flow in femoral vein, and blood flow volume were recorded before the surgery and on the 2th, 5th and 7th day after surgery. And then, the comparisons between the two groups were made, respectively. In addition, the intraoperative blood loss and postoperative wound drainage were recorded, and the bleeding signs were observed within 4 weeks after the operation, such as fetal hemorrhage, hemoptysis, hematuria, cerebral hemorrhage, etc. (Figs. 1, 2).

Comparison of primary diseases between graduated compression stockings alone and IPCD in addition

Comparison of anesthesia method and prosthesis fixation between graduated compression stockings alone and IPCD in addition
Statistical analysis
Statistical Package for the Social Sciences (SPSS) version 6.0 was used for the analyses. To analyze the differences between the specialties, we used cross tabs with Chi square test and correlation was calculated with the Spearman’s rho. The alpha level was set at 0.05.
Results
Comparison of DVT incidence between graduated compression stockings alone and IPCD in addition
In the control group, 6 of 61 patients (9.84%) developed DVT by the postoperative Doppler sonography. On the contrary, only 2 of 51 patients (3.92%) in the experimental group developed DVT. The difference in DVT incidence between both groups as determined by Fisher’s test was statistically significant (X2 = 5.632, P = 0.034). When compared with the conventional graduated compression stockings alone, the intraoperative application of IPCD and stockings contributed the significant reduction of DVT (3.92%, 2/51 versus 9.84%, 6/61, X2 = 5.632, P = 0.034), as shown in Fig. 3.

Comparison of DVT incidence between graduated compression stockings alone and IPCD in addition
Comparison of hemodynamic parameters between graduated compression stockings alone and IPCD in addition
In terms of the mean and peak velocity of blood flow in femoral vein, the postoperative difference was higher in the observation group than those in the control group (P < 0.05). As shown in Table 2 and Fig. 4, the perioperative blood flow of femoral vein in graduated compression stockings alone was 130.15 ± 22.56 mm/s, and the perioperative blood flow of femoral vein in graduated compression stockings plus IPCD group was 149.56 ± 26.35 mm/s. Prior to treatment, the difference between the two groups was not statistically significant (114.23 ± 23.69 versus 118.12 ± 22.11 mm/s, P > 0.05).

Comparison of blood flow in femoral vein between graduated compression stockings alone and IPCD in addition
Comparison of perioperative blood loss and bleeding signs between graduated compression stockings alone and IPCD in addition
With respect to perioperative blood loss, as shown in Table 3 and Fig. 5, the perioperative blood loss in graduated compression stockings alone was 950.1 ± 305.9 ml, and the perioperative blood loss in graduated compression stockings plus IPCD group was 800.5 ± 320.7 ml. After statistical analysis, the difference between the two groups was statistically significant (P = 0.031). Besides, concerning the bleeding signs, only one patient in the control group suffered from postoperative upper gastrointestinal hemorrhage.

Comparison of perioperative blood loss and bleeding signs between graduated compression stockings alone and IPCD in addition
Discussion
In general, the slow blood flow, injured venous wall and blood hypercoagulability have been recognized as the three major factors leading to venous thromboembolism [21,22,23]. In clinical practice, these patients underwent major orthopedic surgery are routinely confined to bed rest for a long time, the blood flow becomes slow, and venous thromboembolisms are easy to form [24]. Generally speaking, the major orthopedic surgery can result in the high risk for venous thromboembolism, which can potentially lead to various chronic complications. Therefore, the DVT prophylaxis has been the conventional care for patients who ever undergo major orthopedic surgery in clinical practice [25, 26]. At present, a variety of treatment to prevent DVT are necessary and available in clinical practice, and the two primary approaches are pharmacological strategy and mechanical devices, such as antiplatelet, anticoagulant, IPCD, graduated compression stockings, and plantar vein pumps, etc. [27, 28]. Although the pharmacological strategy play an significant role in the prevention of DVT, it also has important potential risk of bleeding, prosthetic joint infections, and reoperation [28, 29]. According to previous publications, these increased risks after major orthopedic surgery has been widely documented in general population. And, all these above complications might cause increased hospital length of stay and costs, higher morbidities and death, and permanent removal of the prosthetic joint [30, 31]. Hence, the mechanical devices are thought to be inferior to pharmacological agents to prevent DVT [32].
In healthy populations, the venous pressure in the lower extremities is increasing from top to bottom. On the basis of this principle, the graduated compression stocking is one kind of elastic stocking that promotes venous return of the lower extremities. The basic mechanisms of DVT prevention by graduated compression stocking are as follows. Firstly, it can provide continuous pressure protection. The persistent and moderate venous wall pressure can offset the increased venous pressure caused by various causes [33]. The overly dilated veins of lower extremities are reduced, and the vein stasis can be improved, in order to accelerate the blood flow of lower extremities, prevent the aggregation of clotting factors and adhesion to the vascular intima, and promote the return of venous blood. Secondly, it can also provide the instant supercharging. Through the gradient pressure from bottom to top, the contraction of lower extremity muscle can produce an immediate and antidromic pressure wave which acts on the deep veins [5]. And this pressure can instantaneously increase the blood flow velocity. Such repeated contraction of muscles can continue to produce the antidromic compression force, which promotes venous return, maintains pulsation and circulation, and thereby effectively prevent DVT. Nevertheless, the following patients should not use elastic socks. (1) Suspect or confirm peripheral vascular disease; (2) Peripheral nerve or other sensory impairments; (3) Skin diseases, such as dermatitis, gangrene; (4) Allergy to elastic stockings; (5) Severe leg edema or pulmonary edema caused by heart failure, congestive heart failure; (6) Lower limb deformity. In addition, with respect to the pressure selection, the domestic and international guidelines are consistent with each other. The domestic guidelines for perioperative thromboprophylaxis in general surgery recommend that the ankle pressure should be maintained at 18–23 (1 mmHg = 0.133 kPa). And, the recommendation of international guideline is that the optimal pressures from ankle to middle thigh are 18, 14, 10, and 8 mmHg, respectively. The patients should constantly focus on whether the elastic stockings are worn correctly, because the actual pressure value is closely related to the correct wearing. In further, according to the guideline of health promotion in UK national institute, the patients should start to use elastic stockings until they have complete activity ability [5, 17, 33]. On the other hand, IPCD is a engineering device that can provide progressive pressure on the ankle, calf, and thigh. It also promotes venous blood flow of lower extremities and prevents DVT in this locations. The basic mechanisms of DVT prevention by IPCD are as follows. Firstly, it can accelerate the venous blood flow of lower extremities and promote the emptying of blood stasis. IPCD periodically pressurizes and decompresses the lower limbs, and thereby generates pulsatile blood flow which easily enters into the deep venous system of distal limb [34]. Hence, it can help to promote blood circulation in the lower extremities, to prevent coagulation factor aggregation and adhesion to the vascular intima, and thereby to prevent DVT. Secondly, it can increase the activity of fibrinolytic system. Not only for healthy population, but also for patients suffering from venous thrombosis, IPCD can help to stimulates endogenous fibrinolytic activity [35]. The use taboos of IPCD and graduated compression stockings are similar, and the patients suffering from deep venous thrombosis, thrombophlebitis, or pulmonary embolism should not received IPCD treatment [36]. This device can pressurize in a short time to accelerate venous blood flow of lower limbs, and the different pressure parameters can be adjusted. Usually, the pressures at ankle, calf and thigh are 45, 35 and 30 mmHg, respectively. Concerning the usage time, the guideline of British national health promotion institute recommends that the patients should start to use IPCD from hospital admission, until they have complete activity ability [37]. And the American Association of Chest Physicians recommends that the daily usage time should be more than 18 h. Although the physical prevention of deep venous thrombosis is the preferred method for patients with low, medium, and high risk of bleeding, it is still confronted with dire challenges, especially the patient compliance. And the measures which might improve compliance should be recommended, for instance, increase the equipment number, carry out professional training, increase the visit number by nurses, change health education methods and timing, improve or innovate device designs, strengthen nurses’ awareness of deep vein thrombosis prevention, etc. [18, 38].
In this research, concerning the comparison of DVT incidence between two groups, when compared with the conventional graduated compression stockings alone, the intraoperative application of IPCD and stockings contributed the significant reduction of DVT (3.92%, 2/51 versus 9.84%, 6/61, X2 = 5.632, P = 0.034). In terms of the mean and peak velocity of blood flow in femoral vein, the postoperative difference was higher in the observation group than those in the control group (P < 0.05). With respect to perioperative blood loss, the perioperative blood loss in graduated compression stockings alone was 950.1 ± 305.9 ml, and the perioperative blood loss in graduated compression stockings plus IPCD group was 800.5 ± 320.7 ml. After statistical analysis, the difference between the two groups was statistically significant (P = 0.031). Of course, several limitations should be acknowledged in this study, Firstly, the number of patients included in the study was relatively small and the pathological types were relatively simplex. Secondly, the optimal treatment time and period were not evaluated. Therefore, further multi-center studies with large samples are needed urgently.
Conclusions
In summary, the intraoperative application of IPCD could promote blood circulation of lower limbs, and significantly decrease the incidence of potentially fatal DVT in patients undergoing major orthopedic surgery, when compared with the conventional graduated compression stockings alone.
References
Balk EM, Ellis AG, Di M, Adam GP, Trikalinos TA, Venous thromboembolism prophylaxis in major orthopedic surgery: systematic review update 2017, Rockville, MD.
Sobieraj DM, Coleman CI, Tongbram V, Chen W, Colby J, Lee S, Kluger J, Makanji S, Ashaye A, White CM. Comparative effectiveness of combined pharmacologic and mechanical thromboprophylaxis versus either method alone in major orthopedic surgery: a systematic review and meta-analysis. Pharmacotherapy. 2013;33:275–83.
Caldeira D, Rodrigues FB, Pinto FJ, Ferreira JJ, Costa J. Thromboprophylaxis with apixaban in patients undergoing major orthopedic surgery: meta-analysis and trial-sequential analysis. Clin Med Insights Blood Disord. 2017. https://doi.org/10.1177/1179545X17704660.
Wang L, Zhang C, Mu S, Yeh CH, Chen L, Zhang Z, Wang X. Safety of catheter-directed thrombolysis for the treatment of acute lower extremity deep vein thrombosis: a systematic review and meta-analysis. Medicine (Baltimore). 2017;96:e7922.
Munoz-Figueroa GP, Ojo O. Venous thromboembolism: use of graduated compression stockings. Br J Nurs. 2015;24(680):682–5.
Farfan M, Bautista M, Bonilla G, Rojas J, Llinas A, Navas J. Worldwide adherence to ACCP guidelines for thromboprophylaxis after major orthopedic surgery: a systematic review of the literature and meta-analysis. Thromb Res. 2016;141:163–70.
Stubbs MJ, Mouyis M, Thomas M. Deep vein thrombosis. BMJ. 2018;360:k351.
Grigorian A, Nahmias JT. Deep Venous Thrombosis (DVT), Upper Extremity, in StatPearls. Treasure Island FL: StatPearls Publishing LLC; 2018.
Hardman RL. Management of chronic deep vein thrombosis in women. Semin Intervent Radiol. 2018;35:3–8.
Stone J, Hangge P, Albadawi H, Wallace A, Shamoun F, Knuttien MG, Naidu S, Oklu R. Deep vein thrombosis: pathogenesis, diagnosis, and medical management. Cardiovasc Diagn Ther. 2017;7:S276–84.
Jacobs B, Henke PK. Evidence-based therapies for pharmacologic prevention and treatment of acute deep vein thrombosis and pulmonary embolism. Surg Clin North Am. 2018;98:239–53.
Jiang Z, Ma J, Wang Q, Wu F, Ping J, Ming L. Circulating microRNA expression and their target genes in deep vein thrombosis: a systematic review and bioinformatics analysis. Medicine (Baltimore). 2017;96:e9330.
Khan MT, Ikram A, Saeed O, Afridi T, Sila CA, Smith MS, Irshad K, Shuaib A. Deep vein thrombosis in acute stroke—a systemic review of the literature. Cureus. 2017;9:e1982.
Marietta M, Romagnoli E, Cosmi B, Coluccio V, Luppi M. Is there a role for intervention radiology for the treatment of lower limb deep vein thrombosis in the era of direct oral anticoagulants? A comprehensive review. Eur J Intern Med. 2018;52:13–21.
Mustafa J, Asher I, Sthoeger Z. Upper extremity deep vein thrombosis: symptoms, diagnosis, and treatment. Isr Med Assoc J. 2018;20:53–7.
Shi Y, Shi W, Chen L, Gu J. A systematic review of ultrasound-accelerated catheter-directed thrombolysis in the treatment of deep vein thrombosis. J Thromb Thrombolysis. 2018;45:440–51.
Wade R, Paton F, Woolacott N. Systematic review of patient preference and adherence to the correct use of graduated compression stockings to prevent deep vein thrombosis in surgical patients. J Adv Nurs. 2017;73:336–48.
Dunn N, Ramos R. Preventing venous thromboembolism: the role of nursing with intermittent pneumatic compression. Am J Crit Care. 2017;26:164–7.
Tran K, Argaez C. Intermittent pneumatic compression devices for the management of lymphedema: a review of clinical effectiveness and guidelines. Ottawa ON: Canadian Agency for Drugs and Technologies in Health; 2017.
Pavon JM, Williams JW Jr, Adam SS, Razouki ZA, McDuffie JR, Lachiewicz PF, Kosinski AS, Beadles CA, Ortel TL, Nagi A. Effectiveness of intermittent pneumatic compression devices for venous thromboembolism prophylaxis in high-risk surgical and medical patients. J Arthroplasty. 2015;31(2):524–32.
Huang F, Zhao Q, Guo C, Ma G, Wang Q, Yin Y, Wu Y. Use of aprotinin to reduce blood loss and transfusion in major orthopedic surgery: a meta-analysis. Transfus Apher Sci. 2014;51:152–61.
Rostagno C. New oral anticoagulants in prophylaxis of venous thromboembolic disease in major orthopedic surgery. Cardiovasc Hematol Disord: Drug Targets. 2016;15:204–9.
Rostagno C. Prophylaxis of venous thromboembolism in major orthopedic surgery: a practical approach. Cardiovasc Hematol Agents Med Chem. 2013;11:230–42.
Rachidi S, Aldin ES, Greenberg C, Sachs B, Streiff M, Zeidan AM. The use of novel oral anticoagulants for thromboprophylaxis after elective major orthopedic surgery. Expert Rev Hematol. 2013;6:677–95.
Mitchell MD, Betesh JS, Ahn J, Hume EL, Mehta S, Umscheid CA. Transfusion thresholds for major orthopedic surgery: a systematic review and meta-analysis. J Arthroplasty. 2017;32:3815–21.
Maniscalco P, Caforio M, Imberti D, Porcellini G, Benedetti R. Apixaban versus enoxaparin in elective major orthopedic surgery: a clinical review. Clin Appl Thromb Hemost. 2015;21:115–9.
Fantoni C, Dentali F, Ageno W. Chronobiologic aspects of venous thromboembolism. Heart Fail Clin. 2017;13:691–6.
Kraaijpoel N, van Es N, Porreca E, Buller HR, Di Nisio M. The diagnostic management of upper extremity deep vein thrombosis: a review of the literature. Thromb Res. 2017;156:54–9.
Bartlett M, Mauck KF, Bierle DM, Saadiq RA, Daniels PR. Updates in venous thromboembolism management: evidence published in 2016. Hosp Pract. 1995;2017(45):65–9.
Cho HJ, Dunn AS. The value of using ultrasound to rule out deep vein thrombosis in cases of cellulitis. J Hosp Med. 2017;12:259–61.
Dunham CM, Huang GS. Lethal trauma pulmonary embolism is a black swan event in patients at risk for deep vein thrombosis: an evidence-based review. Am Surg. 2017;83:403–13.
Ganau M, Prisco L, Cebula H, Todeschi J, Abid H, Ligarotti G, Pop R, Proust F, Chibbaro S. Risk of Deep vein thrombosis in neurosurgery: state of the art on prophylaxis protocols and best clinical practices. J Clin Neurosci. 2017;45:60–6.
Clarke MJ, Broderick C, Hopewell S, Juszczak E, Eisinga A. Compression stockings for preventing deep vein thrombosis in airline passengers. Cochrane Database Syst Rev 2016;9:CD004002.
Pavon JM, Adam SS, Razouki ZA, McDuffie JR, Lachiewicz PF, Kosinski AS, Beadles CA, Ortel TL, Nagi A, Williams JW Jr. Effectiveness of intermittent pneumatic compression devices for venous thromboembolism prophylaxis in high-risk surgical patients: a systematic review. J Arthroplasty. 2016;31:524–32.
O’Connell S, Bashar K, Broderick BJ, Sheehan J, Quondamatteo F, Walsh SR. G OL, Quinlan LR. The use of intermittent pneumatic compression in orthopedic and neurosurgical postoperative patients: a systematic review and meta-analysis. Ann Surg. 2016;263:888–9.
Lauvrak V, Hafstad E, Fure B. Intermittent pneumatic compression to prevent venous thromboembolism in hospitalized patients: systematic scoping review, Oslo, Norway: 2016 by The Norwegian Institute of Public Health (NIPH).
Feng JP, Xiong YT, Fan ZQ, Yan LJ, Wang JY, Gu ZJ. Efficacy of intermittent pneumatic compression for venous thromboembolism prophylaxis in patients undergoing gynecologic surgery: a systematic review and meta-analysis. Oncotarget. 2017;8:20371–9.
Elbuluk AM, Kim KY, Chen KK, Anoushiravani AA, Schwarzkopf R, Iorio R. respiratory synchronized versus intermittent pneumatic compression in prevention of venous thromboembolism after total joint arthroplasty: a systematic review and meta-analysis. Orthop Clin North Am. 2018;49:123–33.
Declarations
Authors’ contributions
All authors checked and confirmed this manuscript. Literature review: DW; Research performance: DW, FB, QL, YT; Modification: JL; Checked the validity of data: DW, FB, QL, YT, JL. All authors read and approved the final manuscript.
Competing interests
On behalf of our team, we declare that there is no competing interests in this research.
Availability of data and materials
On behalf of our team, we declare that all the data and material in this research is available.
Consent for publication
We are all consent for publication if accepted.
Ethics approval and consent to participate
Before carrying out this research, we obtained the informed consents of each patient. And this research protocol was approved by institutional review board in our hospital.
Funding
This study was funded by the National Science Foundation of Liaoning Province (No. 201602835).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wang, D., Bao, F., Li, Q. et al. Semiautomatic intermittent pneumatic compression device applied to deep vein thrombosis in major orthopedic surgery. BioMed Eng OnLine 17, 78 (2018). https://doi.org/10.1186/s12938-018-0513-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12938-018-0513-5