
Abstract
Background
High sodium and low potassium intakes are associated with the early development of chronic diseases (e.g., hypertension, obesity). Taking into account the limited data on sodium and potassium intakes by 24-h excretion in urine in pre-adolescents and adolescents, we wished to determine baseline salt intake in Iranian subjects aged 11–18 years.
Methods
This was an observational study involving 374 pre-adolescents and adolescents (154 boys and 220 girls). Sodium and potassium intakes were ascertained by measuring sodium and potassium excretion in urine over 24 h. Creatinine level was used to validate the completeness of the urine collections. The association between sodium and potassium intake and adiposity was determined based on body fat percentage.
Results
The mean 24-h urine sodium concentration was 3130 ± 2200 mg/day, equal to 7.961 ± 5.596 g/day salt intake. Approximately half of the study participants exceeded the upper limit of Na intake. The mean potassium intake was estimated 1480 ± 1050 mg/day. There was a positive association between urinary sodium excretion and adiposity in crude (OR 1.79; 95% CI: 1.08—2.74) and full adjusted model (OR: 3.15; 95% CI: 2.28–4.63). Also, in subsample analysis, there was a positive correlation between urinary sodium and adiposity in both pre-adolescents (OR: 2.71; 95% CI: 2.29—3.93) and adolescents (OR: 3.55; 95% CI: 2.17—4.74). However, no significant association was found between 24-h urinary potassium and adiposity.
Conclusion
Sodium intake, as estimated by 24-h urinary excretion, was higher than recommended and it was positively associated with adiposity. Also, this study reported low compliance of potassium intake recommendations in 11–18 years’ Iranian pre-adolescents and adolescents. Health promotion interventions are needed in order to broaden public awareness of high sodium intake and potassium inadequacy to reduce chronic diseases.
Similar content being viewed by others

Introduction
Excessive sodium (Na) and inadequate potassium (K) intakes are associated with an increased risk of high blood pressure (BP), which is the primary risk factor for cardiovascular diseases (CVDs) [1, 2]. Recent evidence shows that salt plays a key role in regulating BP in children [1, 3]. Subjects with high BP at an early age are more likely to develop hypertension in the future [4]. Also, high Na and low K intakes have detrimental effects on obesity, and both are associated with other chronic diseases and premature death [1, 5]. There is also evidence on Na intake in relation to body weight in children and adolescents independent of energy intake [6]. In addition, it has been found that K intake slows the harmful effects of Na, although this has only been shown in relation to BP [7]. There are few epidemiologic studies indicating a positive correlation between high Na and low K intakes and adiposity measures [8, 9].
Studies on Na and K intakes in young children are relatively few and the global data in this regard are mainly limited to Europe and North America [1]. Likewise, available information about Iranian children's Na and K intake is very limited. One study of Iranian children aged 3–10 years indicated a high intake of Na in this population (2017 mg/day), assessed using a spot urine sample [10].
According to the public health priorities, reducing salt intake is one of the easiest, most efficient, and cost-effective ways to control the burden of health disorders [11]. Therefore, determining Na intake among children using standard measurements is considered an important first step in the implementation of health programs. The use of dietary surveys and databases detailing food composition can over-or underestimate the actual intake [12, 13]. The best method of estimating Na and K intakes is the measurement of its excretion over 24 h, which is considered the gold standard to assess dietary intake [14].
To the best of our knowledge, there is no data on 24-h urinary excretion of Na and K in Iranian pre-adolescents and adolescents. Thus, we aimed to evaluate and provide information about consumption levels of Na and K and their relation to adiposity, measured by 24-h urinary excretion in a sample of Iranian individuals aged 11–18 years old.
Materials and methods
Study design and participants
This cross-sectional study was conducted on healthy individuals aged 11–18 years in Isfahan city, Iran. Using the cluster random sampling method, participants were selected from 13 schools of 4 different districts. Within participating schools, invitations were sent to the parents. All parents/students who agreed to participate in the study signed informed a written consent. Participants with any acute or chronic diseases or on any medication or special diet were excluded from the study.
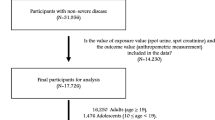
Of 456 participants who received the 24 h urine containers, 50 were not returned. Samples with volumes of less than 500 ml, more than one missed voiding, and/ or 24-h creatinine excretion less than 0.1 mg/ kg body weight were discarded [15]. Also, participants who stated that they had missed any urine collections were excluded from the study.
Also, some discarded urine samples due to volumes of less than 500 ml were excluded (n = 32). Thus, 374 participants had complete and valid urinary samples and questionnaires and were included in the final analysis (response rate 82%). The study protocol was approved by the Research Ethics Committee of Isfahan University of Medical Sciences (IR. mui.rec.1394.3/ 294).
Twenty-four h urine collection
Participants and parents were provided with 24-h urine collection containers, along with verbal and written instructions on how to complete the collection. It was emphasized that no change in dietary intake during the day of collection was allowed. The urine collection was completed over the weekends from Friday to Saturday, during a 24-h period. Each participant was provided with a 2.5-L polypropylene container used for the collection of a 24-h urine sample. All participants were instructed to initiate the collection by emptying their bladder, discarding the first urination after waking on Friday morning, and continuing collection until the morning of the following day. To assist urine collection, an additional 500 ml plastic cup was provided. All participants were asked to keep the container in a cool and dry place and samples were immediately transferred to the laboratory the next day for further analysis in order to prevent microbial degradation. If a person was unable to deliver the urine sample for any reason, the sample was retrieved from their home by a member of the research team.
Measured parameters included 24-h urine volume, Na, K, and creatinine levels. Na and K were estimated by the ion-selective electrode method and urine creatinine was measured using the Jaffe reaction method [16].
Anthropometric assessment
Anthropometric parameters, including weight and height, were measured using the following standard protocols with light clothing and without shoes. Weight, body mass index (BMI), percentage body fat (PBF), and lean body mass (LBM) were all measured using an Omron digital scale (BF511, Kyoto, Japan). Body fat percentage ≥ 25% in boys and 35% in girls was defined as being at risk of adiposity [17].
Assessment of other variables
Additional socio-demographic information, including age, sex, parents’ educational level, household income, and past medical history were obtained from a self-administered questionnaire completed by participants and/or their parents/guardians. Also, children's physical activity was assessed through a self-administrated7-day recall questionnaire (PAQ) with high validity and moderate reliability [18], which was also, fulfilled by participants themselves and/or their parents/guardians. PAQ assesses participants in different physical activities in the school, after school, evenings, and weekends with 9 items, each scored on a 5-point scale. A value from 1 to 5 is obtained for each of the 9 items and used in the physical activity composite score and the mean of these scores becomes the final PAQ activity score. A score of 1 indicates low physical activity, a score of 2–4 indicates moderate physical activity, and a score of 5 indicates high physical activity.
Statistical analysis
Descriptive statistics (mean values and standard deviations for continuous variables or numbers and percentages for categorical variables) were used to describe participants' characteristics. We considered participants aged 11–14 years as pre-adolescents and 15–18 years as adolescents. One-way ANOVA and chi-square tests were used where appropriate. Multiple logistic regression models were used to assess the association between 24-h urinary Na and K excretion with PBF. The unadjusted and adjusted models (age, sex, parental educational level, household income, physical activity) are presented. To assess whether the association between 24-h urinary Na and K excretion with adiposity was independent of energy and sugar-sweetened beverages (SSBs) intake (including carbonated soft drinks, soda, squashes, and industrial fruit drinks), additional models were constructed involving these covariates. In all multiple models, the first tertile of Na and K excretion was considered as the reference. Analyses were completed using SPSS for Windows (version 18, SPSS Inc., Chicago, IL., USA), and a P-value < 0.05 was considered statistically significant.
Results
Table 1 shows the main characteristics of the study participants and information on urinary excretion. Of 374 participants, 58.8% (n = 220) were girls (mean age: 14.4 ± 2.02 years). The mean 24-h urine Na concentration was 3130 ± 2200 mg/ day, equal to 7.961 ± 5.596 g/day salt intake. Approximately half of the study participants exceeded the upper limit of Na intake. The mean K intake was estimated 1480 ± 1050 mg/day, and the excretion of 24-h urine K in girls and boys was 1320 ± 890 and 1700 ± 1200 mg/day. The majority of participants received less than recommended levels.
Odds ratios (ORs) for adiposity across tertiles of Na and K excretion are provided in Table 2 and 3. In the total sample of 11–18-year-olds, those in the highest tertile of Na excretion had higher odds of adiposity based on body fat percentage as compared with those in the lowest category in the crude model (OR: 1.79; 95% CI: 1.08–2.74). The association remained significant after adjusting for potential confounders including age, sex, family income, parents educational level, physical activity, calorie and SSBs intake (OR: 3.15; 95% CI: 2.28- 4.63).
Likewise, in the subgroup analysis on pre-adolescents aged 11–14 years and adolescents aged 15–18 years, both pre-adolescents and adolescents in the highest tertile of Na excretion had higher odds of adiposity compared with those in the lowest category (OR: 2.71; 95% CI: 2.29–3.93) and (OR: 3.55; 95% CI 2.17- 4.74), respectively. Also, after adjusting for confounders, there was a negative but not statistically significant association between urinary potassium excretion and body fat percentage in both pre-adolescents and adolescents.
Discussion
As far as we know, this is the first study in Iran to evaluate Na and K intakes in a sample of pre-adolescents and adolescents aged 11- 18 years using 24-h urine excretion. The results demonstrated poor adherence to Na and K intake recommendations as 46.1% and 80.5% of participants did not meet the recommendations for Na and K intakes, respectively. Also, there was a positive association between Na excretion and adiposity among study participants.
Data related to Na intake in Iran are limited and there is no data based on 24-h urinary samples especially in pre-adolescents and adolescents. A study conducted on Iranian children aged 3- 10 years showed that the mean urinary sodium excretion was 177.17 mmol/day [10]. However, the mentioned study used spot urine samples to estimate the intakes. Similar results were found in other Asian countries using urine samples. In a study of 6–10 years old Lebanese children [19], the estimated mean Na intake was 96.57 ± 61.67 mmol/day. Also, a study in Japan on 3-year-old children found that urinary Na concentration was 140 ± 67 mmol/d [20]. Studies in European adolescents including Italy, Spain, England, and Germany have yielded comparable results [21,22,23,24]. Generally, Na excretion in boys was greater than in girls, which is consistent with our results. This may be due to the higher food consumption levels by boys.
There are also studies evaluating Na intake in children using dietary questionnaires. In Korea, mean Na intake was 4100 mg/d [25] and in Australian 14–16 years old children, mean dietary Na intake was reported to be 2480 mg/d [26]. In the present study, the mean Na intake assessed by a food frequency questionnaire was 269 l mg/d, which is lower than Korean and Australian reports in children.
In this study, the mean K excretion was below WHO recommendations, which is consistent with some other studies reporting low K intake in pre-adolescents and adolescents. Among Dutch children aged 5- 17 years, mean K excretion was 1708.67 mg/d [27] and among Portuguese children, only 6.1% of boys and 7.1% of girls met the recommendations for K intake [28].
Furthermore, this study for the first time shows a positive correlation between PBF and 24 h urinary Na excretion in Iranian pre-adolescents and adolescents, which is consistent with previous studies suggesting a higher likelihood of obesity in children with high Na intake [6, 29]. Among Australian children aged 4–12 years, with an additional 17 mmol/d of Na, the risk of being overweight/obese or abdominally obese increased by 23% and 15%, respectively[30]. They revealed that the potential adipogenic effect of Na is associated with the total body weight and is not specific to central fat distribution. Similar to our study, in a longitudinal study conducted on German children and adolescents aged 3–18 years, a positive association was found between Na intake and BMI z score [31]. It shows that the effects of Na on weight are not affected by puberty and hormones, suggesting that Na can cause obesity in all ages and both genders [31].
Studies on the association between K intake and risk of obesity have led to different results. While Murakami et al. [32] in their study on Japanese young women showed a reciprocal relationship between 24 h urine K and abdominal obesity, studies performed by Shin et al. [33] and Lee et al. [34] showed that receiving K had no effect on obesity. Also, the results of a pooled analysis and systematic review done by Cai X et al. [35] showed that high K intake could not reduce the risk of obesity, while serum K was associated with obesity. In the present study, K showed only an inverse association with adiposity after adjusting the effect of 24 h urine Na, indicating that high K, along with a reduction in dietary Na intake, can reduce the risk of obesity. Most studies in this field have been conducted over the past five years, indicating that K effect on obesity is a new topic, and more robust studies with better design are warranted [34].
Several mechanisms may explain the association of Na and K intakes with obesity risk. First, diets high in Na and low in K are often high in energy and therefore may promote weight gain [26]. Besides, through the effects on thirst, a salty diet may cause a greater consumption of SSBs, which are associated with weight gain [26, 30, 36]. However, after adjusting for intake of energy and SSBs, we found that the association between Na intake and adiposity remained significant, suggesting that other mechanisms may be involved [30, 37]. Experimental studies suggest that higher Na intake is associated with increased lipogenic activity and the formation of adipocyte tissue [38]. Moreover, the uptake of glucose and its conversion to lipids within adipocytes increased in mice as their Na intake increased [38, 39]. The mechanism of dietary K intake in relation to obesity risk is less well- understood. It has been suggested that obesity is associated with K channel function [40, 41]. K can influence carbohydrate accumulation and glucose homeostasis [42, 43] and can lay an important role in insulin secretion and carbohydrate metabolism [43, 44]. Also, the protective effect of K against obesity could be due to the high intake of fruits and vegetables, as the main sources of K in diet [45]. In summary, more studies are needed to elucidate the exact mechanism of action of dietary K in obesity control.
One of the strengths of the present study was the use of 24-h urinary samples, the most valid and objective indicator to measure total Na and K intakes. However, we only had one 24-h urine excretion per participant, which can cause over/under-estimation of Na and K intake and may be considered a limitation. In addition, although Omron digital scale is a portable measuring tool that enables investigators to assess body composition in a larger population, as we can see in previous studies [46,47,48], the validity of the device has not been confirmed, thus, the result should be interpreted with caution.
Conclusion
In conclusion, we found that Na intake among Iranian children and adolescents is high and K intake is lower than recommended levels, with a positive association between Na intake and adiposity. The results provide better insight into the possible relationship between these nutrients and adiposity, emphasizing the necessity of more investigations in this area, which can be resulted in providing a ground for new nutrition policies- such as promoting health interventions and broadening public awareness- to prevent obesity in the future.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due to institution’s policy but will be available through contacts with the corresponding author on reasonable requests.
Abbreviations
- CVD:
-
Cardiovascular disease;
- PAQ:
-
Physical Activity Questionnaire;
- BMI:
-
Body mass index;
- PBF:
-
Percentage body fat;
- LBM:
-
Lean body mass;
- FFQ:
-
Food Frequency Questionnaire;
- SSBs:
-
Sugar-sweetened beverages;
- ANOVA:
-
One-way Analysis of Variance
References
Aburto NJ, Ziolkovska A, Hooper L, Elliott P, Cappuccio FP, Meerpohl JJ. Effect of lower sodium intake on health: systematic review and meta-analyses. BMJ. 2013;346: f1326.
Graudal NA, Hubeck-Graudal T, Jurgens G: Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride. The Cochrane database of systematic reviews 2011(11):Cd004022.
He FJ, MacGregor GA. Importance of salt in determining blood pressure in children: meta-analysis of controlled trials. Hypertension. 2006;48(5):861–9.
He FJ, Marrero NM, Macgregor GA. Salt and blood pressure in children and adolescents. J Hum Hypertens. 2008;22(1):4–11.
D’Elia L, Barba G, Cappuccio FP, Strazzullo P. Potassium intake, stroke, and cardiovascular disease a meta-analysis of prospective studies. J Am Coll Cardiol. 2011;57(10):1210–9.
Yoon YS, Oh SW. Sodium density and obesity; the Korea National Health and Nutrition Examination Survey 2007–2010. Eur J Clin Nutr. 2013;67(2):141–6.
Rodrigues SL, Baldo MP, Machado RC, Forechi L. Molina MdCB, Mill JG: High potassium intake blunts the effect of elevated sodium intake on blood pressure levels. J Am Soc Hypertens. 2014;8(4):232–8.
Ge Z, Zhang J, Chen X, Yan L, Guo X, Lu Z, Xu A, Ma J. Are 24 h urinary sodium excretion and sodium: potassium independently associated with obesity in Chinese adults? Public Health Nutr. 2016;19(06):1074–80.
Jain N, Minhajuddin AT, Neeland IJ, Elsayed EF, Vega GL, Hedayati SS. Association of urinary sodium-to-potassium ratio with obesity in a multiethnic cohort. Am J Clin Nutr. 2014;99(5):992–8.
Kelishadi R, Gheisari A, Zare N, Farajian S, Shariatinejad K. Salt intake and the association with blood pressure in young Iranian children: first report from the middle East and north Africa. Int J Prev Med. 2013;4(4):475–83.
He FJ, MacGregor GA. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J Hum Hypertens. 2009;23(6):363–84.
Kristbjornsdottir OK, Halldorsson TI, Thorsdottir I, Gunnarsdottir I. Association between 24-hour urine sodium and potassium excretion and diet quality in six-year-old children: a cross sectional study. Nutr J. 2012;11:94.
Ortega RM, López-Sobaler AM, Ballesteros JM, Pérez-Farinós N, Rodríguez-Rodríguez E, Aparicio A, Perea JM, Andrés P. Estimation of salt intake by 24 h urinary sodium excretion in a representative sample of Spanish adults. Br J Nutr. 2011;105(5):787–94.
Aparicio A, Rodríguez-Rodríguez E, Cuadrado-Soto E, Navia B, López-Sobaler A, Ortega R. Estimation of salt intake assessed by urinary excretion of sodium over 24 h in Spanish subjects aged 7–11 years. Eur J Nutr. 2017;56(1):171–8.
Remer T, Neubert A, Maser-Gluth C. Anthropometry-based reference values for 24-h urinary creatinine excretion during growth and their use in endocrine and nutritional research. Am J Clin Nutr. 2002;75(3):561–9.
Hedayati SS, Minhajuddin AT, Ijaz A, Moe OW, Elsayed EF, Reilly RF, Huang C-L. Association of urinary sodium/potassium ratio with blood pressure: sex and racial differences. Clin J Am Soc Nephrol. 2012;7(2):315–22.
Lee S-K, Kim MK. Relationship of sodium intake with obesity among Korean children and adolescents: Korea National Health and Nutrition Examination Survey. Br J Nutr. 2016;115(05):834–41.
Richardson D, Cavill N, Ells L, Roberts K: Measuring diet and physical activity in weight management interventions: a briefing paper. National Obesity Observatory 2011.
El Mallah C, Merhi K, Ghattas H, Shatila D, Francis S, Hlais S, Toufeili I, Obeid O: Elevated urinary Na/K ratio among Lebanese elementary school children is attributable to low K intake. European journal of nutrition 2016.
Morinaga Y, Tsuchihashi T, Ohta Y, Matsumura K. Salt intake in 3-year-old Japanese children. Hypertension research : official journal of the Japanese Society of Hypertension. 2011;34(7):836–9.
Campanozzi A, Avallone S, Barbato A, Iacone R, Russo O, De Filippo G, D’Angelo G, Pensabene L, Malamisura B, Cecere G, et al. High sodium and low potassium intake among Italian children: relationship with age, body mass and blood pressure. PLoS ONE. 2015;10(4): e0121183.
Maldonado-Martin A, Garcia-Matarin L, Gil-Extremera B, Avivar-Oyonarte C, Garcia-Granados ME, Gil-Garcia F, Latorre-Hernandez J, Miro-Gutierrez J, Soria-Bonilla A, Vergara-Martin J, et al. Blood pressure and urinary excretion of electrolytes in Spanish schoolchildren. J Hum Hypertens. 2002;16(7):473–8.
Marrero NM, He FJ, Whincup P, Macgregor GA. Salt intake of children and adolescents in South London: consumption levels and dietary sources. Hypertension. 2014;63(5):1026–32.
Shi L, Krupp D, Remer T. Salt, fruit and vegetable consumption and blood pressure development: a longitudinal investigation in healthy children. Br J Nutr. 2014;111(4):662–71.
Lee HS, Duffey KJ, Popkin BM. Sodium and potassium intake patterns and trends in South Korea. J Hum Hypertens. 2013;27(5):298–303.
Grimes CA, Riddell LJ, Campbell KJ, Nowson CA. Dietary salt intake, sugar-sweetened beverage consumption, and obesity risk. Pediatrics. 2013;131(1):14–21.
Geleijnse JM, Grobbee DE, Hofman A. Sodium and potassium intake and blood pressure change in childhood. BMJ (Clinical research ed). 1990;300(6729):899–902.
Oliveira AC, Padrao P, Moreira A, Pinto M, Neto M, Santos T, Madureira J, Fernandes Ede O, Graca P, Breda J, et al. Potassium urinary excretion and dietary intake: a cross-sectional analysis in 8–10 year-old children. BMC Pediatr. 2015;15:60.
Zhu H, Pollock NK, Kotak I, Gutin B, Wang X, Bhagatwala J, Parikh S, Harshfield GA, Dong Y. Dietary sodium, adiposity, and inflammation in healthy adolescents. Pediatrics. 2014;133(3):e635-642.
Grimes CA, Riddell LJ, Campbell KJ, He FJ, Nowson CA. 24-h urinary sodium excretion is associated with obesity in a cross-sectional sample of Australian schoolchildren. Br J Nutr. 2016;115(6):1071–9.
Libuda L, Kersting M, Alexy U. Consumption of dietary salt measured by urinary sodium excretion and its association with body weight status in healthy children and adolescents. Public Health Nutr. 2012;15(3):433–41.
Murakami K, Livingstone MBE, Sasaki S, Uenishi K. Ability of self-reported estimates of dietary sodium, potassium and protein to detect an association with general and abdominal obesity: comparison with the estimates derived from 24 h urinary excretion. Br J Nutr. 2015;113(8):1308–18.
Shin D, Joh H-K, Kim KH, Park SM. Benefits of potassium intake on metabolic syndrome: The fourth Korean National Health and Nutrition Examination Survey (KNHANES IV). Atherosclerosis. 2013;230(1):80–5.
Lee H, Lee J. Hwang S-s, Kim S, Chin HJ, Han JS, Heo NJ: Potassium intake and the prevalence of metabolic syndrome: the Korean National Health and Nutrition Examination Survey 2008–2010. PLoS ONE. 2013;8(1):e55106.
Cai X, Li X, Fan W, Yu W, Wang S, Li Z, Scott EM, Li X. Potassium and obesity/metabolic syndrome: a systematic review and meta-analysis of the epidemiological evidence. Nutrients. 2016;8(4):183.
He FJ, Marrero NM, MacGregor GA. Salt Intake Is Related to Soft Drink Consumption in Children and Adolescents A Link to Obesity? Hypertension. 2008;51(3):629–34.
He FJ, Marrero NM, MacGregor GA. Salt intake is related to soft drink consumption in children and adolescents: a link to obesity? Hypertension. 2008;51(3):629–34.
Fonseca-Alaniz MH, Brito LC, Borges-Silva CN, Takada J, Andreotti S, Lima FB. High dietary sodium intake increases white adipose tissue mass and plasma leptin in rats. Obesity. 2007;15(9):2200–8.
Fonseca-Alaniz MH, Takada J, Andreotti S, Campos TB, Campaña AB, Borges-Silva CN, Lima FB. High sodium intake enhances insulin-stimulated glucose uptake in rat epididymal adipose tissue. Obesity. 2008;16(6):1186–92.
Climent B, Simonsen U, Rivera L. Effects of obesity on vascular potassium channels. Curr Vasc Pharmacol. 2014;12(3):438–52.
Crunkhorn S. Metabolic disease: Potassium channel blocker prevents obesity. Nat Rev Drug Discovery. 2013;12(8):577–577.
Mariosa LSS, Ribeiro-Filho FF, Batista MC, Hirota AH, Borges RL, Ribeiro AB, Zanella MT. Abdominal obesity is associated with potassium depletion and changes in glucose homeostasis during diuretic therapy. The Journal of Clinical Hypertension. 2008;10(6):443–9.
Yang Y, Jiang H, Wang M, Korpelainen H, Li C. Male poplars have a stronger ability to balance growth and carbohydrate accumulation than do females in response to a short-term potassium deficiency. Physiol Plant. 2015;155(4):400–13.
Ashcroft FM. ATP-sensitive potassium channelopathies: focus on insulin secretion. J Clin Investig. 2005;115(8):2047–58.
Murakami K, Sasaki S, Uenishi K. for Nutrition JDSS, Group B: The degree of misreporting of the energy-adjusted intake of protein, potassium, and sodium does not differ among under-, acceptable, and over-reporters of energy intake. Nutr Res. 2012;32(10):741–50.
Rezazadegan M, Soheilipour M, Tarrahi MJ, Amani R: Correlation Between Zinc Nutritional Status with Serum Zonulin and Gastrointestinal Symptoms in Diarrhea-Predominant Irritable Bowel Syndrome: A Case–Control Study. Digestive diseases and sciences 2022:1–7.
Vatandoost A, Azadbakht L, Morvaridi M, Kabir A, Farsani GM: Association between dietary inflammatory index and risk of cardiovascular diseases among firefighters. International Journal of Preventive Medicine 2020, 11.
Atule M, Larbie C, Afriyie C. Dietary Pattern and Prevalence of Metabolic Syndrome in Hypertensive Outpatients and Associated Effect on Target Organ Damage. J Clin Nutr Diet. 2019;5(1):4.
Acknowledgements
The authors thank all the study participants and staff for their valuable contributions.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
S.G-H. and N.R. make substantial contributions to conception, design, acquisition of data, analysis and interpretation of data, and drafting of this study. S.G-H. and S-M. S. participate in drafting the article or revising it. M.P. gives final approval of the version to be submitted and any revised version. N.M. is the guarantor of this work. All authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Ethical approval and consent to participate
The study protocol was approved by Research Council and the Ethics Committee of Isfahan University of Medical Sciences (IR. mui.rec.1394.3/ 294).
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Golpour-Hamedani, S., Rafie, N., Pourmasoumi, M. et al. Sodium and potassium intakes and adiposity among Iranian pre-adolescents and adolescents: a cross-sectional study. Nutr J 21, 23 (2022). https://doi.org/10.1186/s12937-022-00776-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-022-00776-y