
Abstract
Background
Ghana adopted the 2012 World Health Organization (WHO) policy on intermittent preventive treatment of malaria in pregnancy (IPTp) and implemented it in 2014 in all regions of Ghana. Despite the implementation of this policy, there has been an unacceptably low percentage of eligible women receiving the optimal dose of IPTp in Ghana which leaves millions of pregnant women unprotected from malaria. The study, therefore, assessed the predictors of three or more doses (optimal dose) of sulfadoxine-pyrimethamine (SP) in Northern Ghana.
Methods
A cross-sectional study was conducted among 1188 women in four selected health facilities in Northern Ghana from September 2016 to August 2017. Information on socio-demographic and obstetric characteristics reported SP use, and maternal and neonatal outcomes were collected which was double-checked from the maternal health book as well as the antenatal care register. Pearson chi-Square and ordered logistic regression were used to determine the predictors of reported optimal SP use.
Results
Out of the 1146 women, 42.4% received 3 or more doses of IPTp-SP as recommended by the national malaria control strategy. SP uptake was significantly associated with antenatal care (ANC) attendance (aOR 0.49, 95% CI 0.36–0.66, P < 0.001), primary education (aOR 0.70, 95% CI 0.52–0.95, P = 0.022), four or more antenatal care visits (aOR 1.65, 95% CI 1.11–2.45, P = 0.014), ANC care visit in second trimester (aOR 0.63, 95% CI 0.49–0.80, P < 0.001) and third trimester (aOR 0.38, 95% CI 0.19–0.75, P = 0.006) and malaria infection during late gestation (aOR 0.56, 95% CI 0.43–0.73, p < 0.001).
Conclusion
The percentage of pregnant women who received three or more doses is below the target of the National Malaria Control Programme (NMCP). The push factors for the optimal use of SP are higher educational attainment, four or more ANC visits, and early initiation of ANC. The study also confirmed earlier findings that IPTp-SP uptake of three or more doses prevents malaria in pregnancy and improves birth weight. The uptake of IPTp-SP among expectant women will be informed and increased by encouraging formal general education beyond the primary level and encouraging early initiation of ANC visits.
Similar content being viewed by others


Background
Pregnant women and their unborn babies are exposed to several harmful diseases including malaria which remains a global public health problem [1]. The most affected groups are pregnant women and children under 5 years of age. Most maternal deaths and miscarriages have been caused by malaria infection [2, 3].
It is estimated that about 125 million pregnancies in malaria-endemic areas of the world suffer yearly from malaria-related infant mortalities in the region of 75,000 and 200,000 [4]. In sub-Saharan Africa, the main infecting parasite is Plasmodium falciparum, which is responsible for 99% of all malaria in pregnancy (MiP) cases [5]. In areas where parasite transmission is stable, over 20 million pregnancies are at risk annually [6,7,8]. These mortalities are due to limitations in the effective detection and management of malaria cases in pregnant women and the further risk of anaemia in the mothers. Nationally, pregnant women who reported to out-patient departments (OPD) with malaria in 2014 were 224,542 (representing 2.7%, that is the proportion attributable to malaria). Out of this number, 6.7% were admitted because of MiP. The case fatality rate was 1.0%. At the regional level, the Northern Region recorded the highest number of deaths due to malaria [9]. Analyzed data in the country revealed that Ghana has the highest (48%) prevalence of MiP in the sub-region both in the wet (59%) and in the dry seasons (41%) [10].
One of the interventions for controlling the negative effect of malaria in pregnancy is the use of SP. Until 2012, IPTp-SP consisted of administering at least two doses of SP to pregnant women (at least once a month) spaced in time by at least a month. The WHO Evidence Review Group recommends the use of SP under Directly Observed Therapy (DOT) starting from the second trimester or after quickening and at subsequent visits separated by a month interval until delivery in October 2012 [11]. Through the National Malaria Control Programme (NMCP), Ghana adopted the implementation of the use of IPTp-SP in 2014 as part of the antenatal care package [12]. The increased dosing with three or more doses of SP was advocated to ensure maximum protection against malaria in pregnancy [13] and greater therapeutic results [14]. For instance, meta-analysis and mathematical models showed that taking at least three SP doses provided additional protection against malaria and was associated with low birth weight and stillbirth [13]. According to the Ghana Demographic Health Survey, there was an improvement in the coverage of two or more doses of IPTp-SP, ranging from 44% in 2008 to 68% in the two years preceding the 2014 survey. Further, the percentage of pregnant women who received 3 or more doses was 39% [15].
According to a 2014 survey conducted by the Ghana NMCP, SP coverage for IPT1, IPT2, and IPT3 was 54.1%, 38.7%, and 24.6%, respectively [16]. Moreover, women who received one or more doses of IPTp-SP increased from 58% in 2008 to 91% in 2019, while those who received two or more doses increased from 46 to 80%. During the same period, the percentage of women receiving three or more IPTp-SP doses increased from 28 to 61% [17]. Comparing the coverage of IPT over the past years, the 2019 Ghana Malaria Indicator Survey (GMIS) saw an improvement in the reported use of SP in Ghana. However, GMISs reported use of there or more doses of SP (61.0%) is less than the NMCP target of 85% set in 2011 [16]. This study is rationalized by the need to find out the predictors of the uptake of three or more doses of the SP to inform health policy planning, intervention, and implementation. The outcome of this research will contribute to the achievement of the Sustainable Development Goal (SDG) 3 and Target 3.3 [18].
Methods
Study design and setting
This research determined the predictors of optimal use of SP using a quantitative facility-based cross-sectional survey conducted in four selected health facilities within the Tamale metropolis catchment area in Ghana’s Northern Region. Teaching, Regional, and District health facilities within the Tamale Metropolis. Tamale Metropolis was chosen because it serves a diverse ethnic and socioeconomic population, and the Teaching Hospital also serves as a referral centre for the region. In Ghana, health care is organized at three levels: national, regional, and district [19]. The study drew on areas from Ghana's three levels of health care.
Study population, sampling and sample size
The study population included post-delivery women who had delivered in any of the four health facilities in the Tamale metropolis. Women who attended ANC during pregnancy and had term delivery in any of the 4 selected health facilities were included in the study. Mothers who miscarried and had a preterm delivery, HIV positive and G6PD defects were excluded from the study. IPTp-SP is contraindicated in pregnant women in the first trimester of gestation [20].
The sample size was calculated based on the target population of pregnant women who attended ANC in 2015 (64,908) for the selected health facilities in the Tamale Metropolis. Using an estimated proportion of 85%, that is, the national target for IPTp coverage among pregnant women for 2011 in Ghana [21] at 95% confidence level and a precision of 3%, assuming a design effect of 2, the sample size obtained was calculated as 1080. The precision of 3% was assumed to help increase the sample size and decrease any uncertainty about the data.
A non-response rate of 10% was adjusted. The required sample size estimated was 1188. Probability Proportional to size (PPS) was used and the sample size for each health facility was 298, 352 and 538 for Teaching, Regional, and District health facilities, respectively. The sample size was 1188; however, 1146 respondents were used in the analysis because 46 of the pregnant women delivered before 36 weeks of pregnancy which made it impossible to assess the recommended number of doses expected.
Study variables
The dependent variable was the receipt of three or more doses of IPTp 3, and the independent variables were socio-demographic factors, obstetric information, and maternal and neonatal outcomes. Table 1 shows independent variables and their definitions.
Data collection tool and method
The study questionnaire was designed to collect the following variables: socio-demographic and reproductive information, IPTp-SP uptake history, haemoglobin level, malaria in pregnancy, and birth outcomes. The study data were taken from three main sources: the maternal health record book, the birth register and through participant interviews. Data extracted from the maternal health record book were cross-checked with the register at the labour ward in accordance with the study protocol and the participants were subsequently interviewed directly to corroborate the validity of all obtained information.
During the interviews, the questionnaires were administered by the principal investigator and the study research assistants (who could also speak the local dialect) to the pregnant women. The respondents who could not understand and communicate in English language were interviewed by a research assistant in Dagbani, Hausa or Akan. The responses were then transcribed back to English and documented on the questionnaires. Data collection from the post-delivery women lasted for a maximum of about 10 min per woman. Data collection spanned a period of 12 months, from September 2016 to August 2017 to help account for seasonality in malaria.
Quality control
Several precautionary measures were undertaken to enhance the quality of the study data. The study questionnaires were designed by using portions of UNICEF documents and extracts of published studies, so they reflected universal standards. A pilot study was done to ensure that the best methods were used to collect, process and examine study data and outcomes to avoid exaggerations.
Again, three dummy sessions were held for study data collectors to rehearse methods and communication strategies designed to extract the relevant information from interviewees. Data were edited daily on the field for necessary corrections by the principal investigator to minimize errors in the database. Two different data entry clerks were trained to enter the same data into the database to minimize errors and enhance data quality.
There were four scheduled data cleanings to ensure that all relevant information had been captured. Two different statisticians were made to analyze the study data to enhance the quality of the analysis. All collected study documents and data had restricted access, with access allowed for limited persons when necessary.
Data analysis
All data entries and management were conducted using the Statistical Package for the Social Sciences software (SPSS) version 20.0 for Windows (SPSS Inc., Chicago) and transported to STATA 12.1 for the analysis (Stata Corporation, College Station, TX, USA). SP intake was grouped as no IPTp-SP, less than three (< 3) IPTp-SP doses and greater than or equal to three (≥ 3) IPTp-SP doses.
For the ordered logistic regression of predictors of optimal SP uptake, SP doses received were categorised into optimal (≥ 3) and suboptimal (< 3) based on WHO recommendations [22]. Pearson Chi-square test, and univariate and multivariate logistic regression analyses were performed. At the end of the bivariate analysis, variables for the multivariate analysis were selected into the model based on the p-value of 0.5 and the clinical significance of some risk factors [23, 24], results of past studies [25, 26] and interests in all the selected general characteristics irrespective of their statistical significance. P < 0.05 was considered statistically significant. The odd ratio (OR) was used to estimate the association between the dependent variable and the independent variables.
Ethical consideration
The study is part of a large study titled “malaria control in pregnancy: an evaluation of the effectiveness of IPTp policy on maternal and neonatal health in the Tamale metropolis of Northern Ghana” which was approved by the Committee on Human Research, Publication and Ethics of Kwame Nkrumah University of Science and Technology/Komfo Anokye Teaching Hospital before the commencement of the study (CHRPE/AP/375/16). Informed consent was obtained from each respondent at the beginning of every individual interview. Confidentiality was maintained by the interviewers as records were coded and did not disclose the identity of respondents. The accessed data set were kept on a pass-worded computer.
Results
General characteristics and reported SP use among post-delivery women
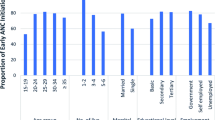
Tables 2 and 3 show the general characteristics of the study respondents and the percentage use of IPTp-SP. Most of the post-delivery women attended ANC clinic at the District Hospital (45.1%), were below 24 years (34.2%) and resided in the urban communities (67.1%). Post-delivery women who had 4 or more antenatal care visits (89.5%) and attended ANC in their second trimester (53.6%) were in the majority. Most of the post-delivery women had anaemia (62.6%), however, 74.1% did not have malaria in pregnancy at 36 weeks of gestation. Post-delivery women who were between the ages of 25–29 (45.2%), had attained a higher level of education (53.4%), enrolled during the first trimester of their pregnancy (52.5%) and had four or more ANC visits (46.3%) reported higher usage of optimal dose of SP.
Place of residence influenced the uptake of SP (p < 0.001). Pregnant women who resided in urban residences had the highest percentage of using the optimal dose during pregnancy (46.7%). Pregnant women who had no malaria infection (47.6%) were found to have used the optimal dose compared to those who had malaria infection (27.6%). There was a higher uptake of the optimal dose of SP among pregnant women who were not anaemic (52.0%) compared to those who were anaemic (36.7%).
Proportion of post-delivery women with reported use of optimal doses of SP
Figure 1 represents the stratification of SP based on the doses. Three or more (≥ 3) doses are considered the optimal dose recommended by the WHO. It could be observed that 42.4% of the post-delivery women reported usage of the optimal dose (Fig. 1) with 20.2% who did not take SP during pregnancy. Among those who reported uptake of SP during pregnancy, a higher proportion of the post-delivery women reported uptake of 2 doses (28.2%) with only 7.1% who reported uptake of 5 doses (Fig. 2).

Stratification of SP doses

Number of doses received by post-delivery
Ordered logistic model for the determinants of optimal SP usage
Tables 4 and 5 are the multivariable ordered logistic regression determining the factors that influenced the reported use of SP among post-delivery women. Women who attended ANC at the District Hospitals were 51% less likely (aOR 0.49 (0.36–0.66), p < 0.001) to take the optimal dose of SP compared to women who attended ANC at the Teaching Hospital. One of the important determinants for the reported use of SP is the number of times the woman attends ANC. Post-delivery women who had 4 or more antenatal care visits were more likely to use 3 or more doses of SP (aOR 1.65(1.11–2.45), p = 0.014) compared to those with less than 4 ANC visits. Post-delivery women who reported and enrolled in the antenatal care services in their second trimester were 37% less likely (aOR 0.63 (0.49–0.80), p < 0.001) to take the optimal doses compared to those who reported in their first trimester of gestation. From the same table, it was observed that post-delivery women who had malaria during their pregnancy were less likely (aOR 0.56(0.43–0.73), p < 0.001) to have taken the optimal dose compared to those who had no malaria infection in pregnancy. This could explain why probably they got infected. Post-delivery women who gave birth to low-birth-weight babies were 53% less likely (aOR 0.47(0.34–0.64), p < 0.001) to take the optimal dose of SP. This means that post-delivery women who reported usage of SP had protection against malaria infection and low birth weight delivery.
Discussion
Though the reported use of SP is expected to prevent malaria in pregnancy and ameliorate the effects on maternal and neonatal health [15, 17], some studies have reported a high prevalence of MiP in some parts of Ghana [27,28,29,30,31,32].
In the current study, pregnant women residents in urban areas were the majority (46.7%) in terms of reported uptake of 3 or more doses of IPTp-SP. This is consistent with other studies which found that urban women are more likely to take three or more doses of SP [33, 34]. However, according to the GMIS women in rural areas (62.0%) were more likely to receive at least three doses, while urban women were more likely not to take SP more than one or two times. The difference could be due to study methodologies: GMIS sampled respondents from across the country, whereas this study’s sample was drawn from a metropolitan area in Ghana’s northern region. There was regional variation in the reported use of three or more doses of SP; Upper West was the highest performing region (78.0%), followed by Upper East (77.4%), Northern (64.5%), and Eastern (42.2%), which is similar to the findings of this study (42.4%) [17]. This suggests that ongoing campaigns to improve malaria prevention methods for expectant mothers should focus especially on rural areas.
Maternal education (college/tertiary; 53.4%) and being resident in the urban (46.7%) and peri-urban (40.3%) were impactful in higher uptake of IPTp-SP. This is consistent with findings from previous studies [34,35,36,37]. Education helps women to read literature, as well as listen to the radio and watch TV to understand the effects of malaria in pregnancy. It also helps people be inquisitive and to be open to new ideas [36, 38, 39] which in turn builds women's knowledge of health issues which helps them to make well-informed healthcare choices during pregnancy [40]. Educated women are better subscribers of malarial interventions and often complete their IPTp-SP dosage course [41, 42]. Studies conducted in Yendi and Chereponi in the Northern and the North-East Regions observed that women without formal education had difficulty in understanding health information during clinical counselling due to the language barrier and format of the information. Hence, they are unable to translate health information into practice [43]. Similarly, less educated women might come from poorer families and live in homes that lack electricity which makes it difficult to access the media easily [44, 45]. This might be the reason for the higher uptake compared to women without education. Facility-based health information should be based on needs assessment to effect relative change in women’s behaviour towards maternity care.
In this study, 42.4% of participants used the optimal dose (three or more doses), with 28.0%, 18.1%, and 7.1% using 3 doses, 4 doses, and 5 doses, respectively. The percentage of pregnant women who received three or more doses of SP is similar to previous studies [34, 39, 46, 47] but lower than the findings of a study conducted in southern Ghana (71.0%) [26] and the 2019 GMIS findings (61.0%) [48]. However, the percentage recorded in this study is an improvement over the percentage (39.0%) reported by the 2014 Ghana Demographic and Health Survey [15] and the NMCP (24.6%) in 2014. Pregnant women who took 3 or more doses of IPTp-SP increased significantly between 2014 (39.0%) and 2019 (61.0%) but remained unchanged between 2016 (60.0%) and 2019 (61.0%) [48]. The proportion of post-delivery women who used IPTp-SP 4 and 5 were 18.1% and 7.1%, respectively, which were higher than the national rates of 4.2% and 1.2%, respectively [16]. The low uptake of IPT 4 and 5 might be due to the late reporting for ANC services in Ghana as studies show that irrespective of the nationwide progress in ANC coverage, timing and number of visits remain a maternal health concern [15, 49, 50]. This observation is further sustained by the results from Table 5 which found that early initiation of ANC and 4 or more ANC (aOR 1.65(1.11–2.45), p = 0.014) visits increased the likelihood of taking three or more doses of SP which corroborates the findings of a study done in Malawi and confirms the WHO updated guidance on ANC[46].
Most of the post-delivery women visited ANC at least four times (89.5%), however, less than half (46.3%) of women reported uptake of three or more doses of SP which is consistent with the findings of a study conducted in Kumasi [35], Gushegu [52], Ghana and Tanzania [53, 54].
In Table 5, pregnant women who initiated their first ANC during the second (aOR 0.63 (0.49–0.80), p < 0.001) and third trimester (aOR 0.38 (0.19–0.75), p = 0.006) were less likely to take three or more doses of SP compared to those who initiated it during the first trimester. This re-affirms the need to place more emphasis on early ANC initiation [9, 21, 34, 49, 50].
The NMCP should step up efforts to promote early ANC initiation and raise awareness about the importance of IPTp-SP and other malaria prevention measures. If they understand the benefits of IPTp, they will seek it out or request it at ANC [34], resulting in optimal IPTp-SP uptake [54]. The updated WHO ANC recommendations stress on early promotion of ANC interaction at either the facility or community level [51, 55].
It was discovered that pregnant women who had malaria at 36 weeks of gestation [aOR 0.56(0.43–0.73), p < 0.001] and gave birth to low-birth-weight babies [aOR 0.47(0.34–0.64), p < 0.001] were less likely to have taken the optimal dose than those who had no malaria in pregnancy and gave birth to normal weight babies. These findings support the argument that using an optimal dose of SP is still effective in preventing malaria in pregnancy [14, 27] and improving birth weight [13]. As a result, the NMCP and the Ghana Health Service, Ghana, should implement interventions aimed at increasing the uptake of at least three doses of SP.
Limitations
The study used a cross-sectional study design, which has the disadvantage of making it impossible to infer causation. Again, there was the possibility of the women reporting the usage of IPTp inaccurately. However, these women were interviewed while they were still on admission and the information given was double-checked from their maternal health care records as well as the ANC register book at the various facilities.
Conclusion
According to the findings of the study, early initiation of ANC and four or more ANC visits during pregnancy increased the uptake of the optimal dose of SP. Postpartum women who had late gestational malaria and had low birth weight babies reported low SP uptake. Women with a primary education who were enrolled in ANC during the second and third trimesters reported less use of SP as an intermittent malaria preventive treatment in Northern Ghana. This study emphasizes the importance of expanding general education beyond primary school and encouraging early ANC visits to increase coverage of the recommended IPTp-SP uptake among pregnant women, thereby preventing gestational malaria infection and improving birth weight.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ANC:
-
Antenatal care
- aOR:
-
Adjusted odd ratio
- DOT:
-
Directly observed therapy
- GMIS:
-
Ghana Malaria Indicator Survey
- IPTp:
-
Intermittent preventive treatment of malaria in pregnancy
- Mip:
-
Malaria in pregnancy
- NMCP:
-
National Malaria Control Programme
- OPD:
-
Out-patient departments
- OR:
-
Odd ratio
- PPS:
-
Probability proportional to size
- SDG:
-
Sustainable development Goal
- SP:
-
Sulfadoxine-pyrimethamine
- UNICEF:
-
United Nations Children’s Fund
- WHO:
-
World Health Organization
References
Sohail M, Shakeel S, Kumari S, Bharti A, Zahid F, Anwar S, et al. Prevalence of malaria infection and risk factors associated with anaemia among pregnant women in semiurban community of Hazaribag, Jharkhand. India Biomed Res Int. 2015;2015:740512.
WHO. World malaria report 2019. Geneva: World Health Organization; 2019.
WHO. World malaria report 2021. Geneva: World Health Organization; 2021.
Steketee RW, Campbell CC. Impact of national malaria control scale-up programmes in Africa: magnitude and attribution of effects. Malar J. 2010;9:299.
WHO. World Malaria Report 2017. Geneva: World Health Organization; 2017.
WHO. Policy brief for the implementation of intermittent preventive treatment of malaria in pregnancy. Geneva: World Health Organization; 2014.
Desai M, ter Kuile FO, Nosten F, McGready R, Asamoa K, Brabin B, et al. Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis. 2007;7:93–104.
Guyatt HL, Snow RWR. Impact of malaria during pregnancy on low birth weight in sub-Saharan Africa. Clin Microbiol Rev. 2004;17:760–9.
NMCP. 2015 Annual Report National Malaria Control Centre for Health Information Management. Accra, Ghana, 2016;1–70.
Berry I, Walker P, Tagbor H, Bojang K, Coulibaly SO, Kayentao K, et al. Seasonal dynamics of malaria in pregnancy in West Africa: evidence for carriage of infections acquired before pregnancy until first contact with antenatal care. Am J Trop Med Hyg. 2018;98:534–42.
WHO. Evidence review group: intermittent preventive treatment of malaria in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP). Geneva: World Health Organization; 2012.
Ghana Health Service. 2017 Annual Report National Malaria Control Programme. Accra, Ghana, 2018.
Mosha D, Chilongola J, Ndeserua R, Mwingira F, Genton B. Effectiveness of intermittent preventive treatment with sulfadoxine-pyrimethamine during pregnancy on placental malaria, maternal anaemia and birthweight in areas with high and low malaria transmission intensity in Tanzania. Trop Med Int Health. 2014;19:1048–56.
USAID. Improving uptake of intermittent preventive therapy in pregnancy (IPTp) at Rachuonyo sub county hospital in Homa Bay County. https://pdf.usaid.gov/pdf_docs/PA00TC57.pdf.
GSS; GHS; ICF Int. Ghana demographic health survey. DHS Program, 2014. 2015. https://dhsprogram.com/pubs/pdf/FR307/FR307.pdf.
NMCP. 2014 Annual Report National Malaria Control. Accra, Ghana, 2015.
Ghana Statistical Service. Ghana Malaria Indicator Survey 2019 Final Report. 2020. www.DHSprogram.com.
Fact sheet on Sustainable Development Goals (SDGs): health targets.
Armah P, Kicha D. Primary health care in Ghana: the structure and functions in relation to preventing neglected tropical diseases. Archiv Euromed. 2020;10:12–7.
WHO. New WHO recommendations for IPTp-SP. Geneva, World Health Organization, 2014. http://whqlibdoc.who.int/publications/2010/9789241599412_eng.pdf
Ghana Statistical Service. Ghana Multiple Indicator Cluster Survey with an Enhanced Malaria Module and Biomarker. Final Report. 2 Accra, Ghana, 011.
WHO. Intermittent preventive treatment in pregnancy (IPTp). Geneva: World Health Organization; 2019.
Fethney J. Statistical and clinical significance, and how to use confidence intervals to help interpret both. Aust Crit Care. 2010;23:93–7.
Ranganathan P, Pramesh CS, Buyse M. Common pitfalls in statistical analysis: clinical versus statistical significance. Perspect Clin Res. 2015;6:169–70.
Nwaefuna EK, Afoakwah R, Orish VN, Egyir-Yawson A, Boampong JN. Effectiveness of intermittent preventive treatment in pregnancy with sulphadoxine-pyrimethamine against submicroscopic falciparum malaria in central region. Ghana J Parasitol Res. 2015;2015:959427.
Ibrahim H, Maya ET, Issah K, Apanga PA, Bachan EG, Noora CL. Factors influencing uptake of intermittent preventive treatment of malaria in pregnancy using sulphadoxine pyrimethamine in sunyani municipality. Ghana Pan Afr Med J. 2017;28:122.
Agyeman YN, Newton SK, Annor RB, Owusu-Dabo E. the effectiveness of the revised intermittent preventive treatment with sulphadoxine pyrimethamine (IPTp-SP) in the prevention of malaria among pregnant women in Northern Ghana. J Trop Med. 2020;2020:2325304.
Wilson NO, Ceesay FK, Obed SA, Adjei AA, Gyasi RK, Rodney P, et al. Intermittent preventive treatment with sulfadoxine-pyrimethamine against malaria and anemia in pregnant women. Am J Trop Med Hyg. 2011;85:12–21.
Anto F, Agongo IH, Asoala V, Awini E, Oduro AR. Intermittent preventive treatment of malaria in pregnancy: assessment of the sulfadoxine-pyrimethamine three-dose policy on birth outcomes in rural Northern Ghana. J Trop Med. 2019;2019:6712685.
Ofori MF, Ansah E, Agyepong I, Hviid L, Akanmori BD. Pregnancy-associated malaria in a rural community of Ghana. Ghana Med J. 2009;43:13–8.
Kweku M, Ofori M, Takramah W, Axame WK, Owusu R, Adjuik M, et al. Prevalence of malaria and anaemia among pregnant women attending antenatal care clinic in the Hohoe municipality of Ghana. Int J Nursing Didactics. 2017;7:21–30.
Darko AG, Adoba P, Edzemeah FJ, Ephraim RK, Sampong BB, Gborgblorvor D, et al. Asymptomatic malaria and its effect on parturients who received intermittent preventive treatment, a cross sectional study of the Bekwai district Ghana. GSC Biol Pharm Sci. 2018;4:7–16.
Amoran OE, Ariba AA, Iyaniwura CA. Determinants of intermittent preventive treatment of malaria during pregnancy (IPTp) utilization in a rural town in Western Nigeria. Reprod Health. 2012;9:12.
Arnaldo P, Rovira-Vallbona E, Langa JS, Salvador C, Guetens P, Chiheb D, et al. Uptake of intermittent preventive treatment and pregnancy outcomes: Health facilities and community surveys in Chókwè district, southern Mozambique. Malar J. 2018;17:109.
Addai-Mensah O, Annani-Akollor ME, Fondjo LA, Sarbeng K, Anto EO, Owiredu EW, et al. Regular antenatal attendance and education influence the uptake of intermittent preventive treatment of malaria in pregnancy: a cross-sectional study at the university hospital, Kumasi. Ghana J Trop Med. 2018;2018:5019215.
Okethwangu D, Opigo J, Atugonza S, Kizza CT, Nabatanzi M, Biribawa C, et al. Factors associated with uptake of optimal doses of intermittent preventive treatment for malaria among pregnant women in Uganda: analysis of data from the Uganda demographic and health survey, 2016. Malar J. 2019;18:250.
Ayubu MB, Kidima WB. Monitoring compliance and acceptability of intermittent preventive treatment of malaria using sulfadoxine pyrimethamine after ten years of implementation in Tanzania. Malar Res Treat. 2017;2017:9761289.
Basha GW. Factors affecting the utilization of a minimum of four antenatal care services in Ethiopia. Obstet Gynecol Int. 2019;2019:5036783.
Kumah E, Duvor F, Otchere G, Ankomah SE, Fusheini A, Kokuro C, et al. Intermittent preventive treatment of malaria in pregnancy with sulphadoxine-pyrimethamine and its associated factors in the Atwima Kwanwoma district. Ghana Ann Glob Health. 2022;88:27.
Hill J, Hoyt J, van Eijk AM, D’Mello-Guyett L, ter Kuile FO, Steketee R, et al. Factors affecting the delivery, access, and use of interventions to prevent malaria in pregnancy in sub-Saharan Africa: a systematic review and meta-analysis. PLoS Med. 2013;10:e1001488.
Dionne-Odom J, Westfall AO, Apinjoh TO, Anchang-Kimbi J, Achidi EA, Tita ATN. Predictors of the use of interventions to prevent malaria in pregnancy in Cameroon. Malar J. 2017;16:132.
Agomo CO, Oyibo WA. Factors associated with risk of malaria infection among pregnant women in Lagos. Nigeria Infect Dis Poverty. 2013;2:19.
Bassoumah B, Mohammed AA. The socio-cultural challenges to maternal and neonatal care: the views of women with disabilities receiving maternity care in the Chereponi district of the Northern Ghana. Sci Afr. 2020;7:e00258.
Winther T, Matinga MN, Ulsrud K, Standal K. Women’s empowerment through electricity access: scoping study and proposal for a framework of analysis. J Dev Effect. 2017;9:389–417.
UNDESA: Electricity and education: the benefits, barriers, and recommendations for achieving the electrification of primary and secondary schools. https://sustainabledevelopment.un.org/index.php?page=view&type=400&nr=1608&menu=1515.
Azizi SC. Uptake of intermittent preventive treatment for malaria during pregnancy with sulphadoxine-pyrimethamine in Malawi after adoption of updated World Health Organization policy: an analysis of demographic and health survey 2015–2016. BMC Public Health. 2020;20:335.
Ameh S, Owoaje E, Oyo-Ita A, Kabiru CW, Akpet OEO, Etokidem A, et al. Barriers to and determinants of the use of intermittent preventive treatment of malaria in pregnancy in cross river state, Nigeria: a cross-sectional study. BMC Pregnancy Childbirth. 2016;16:99.
GSS, NMCP, DHS Program. 2019 Ghana Malaria Indicator Survey (GMIS). Accra, Ghana; Rockville, USA. 2020. https://dhsprogram.com/pubs/pdf/MIS35/MIS35.pdf.
GSS, GHS, ICF. 2017 Ghana Maternal Health Survey Key Findings. Accra, Ghana; Rockville, USA. 2017. https://dhsprogram.com/pubs/pdf/SR251/SR251.pdf.
GSS, NMCP. Malaria indicator survey 2016. Accra, Ghana; 2016.
Lattof SR, Moran AC, Kidula N, Moller AB, Jayathilaka CA, Diaz T, et al. Implementation of the new WHO antenatal care model for a positive pregnancy experience: a monitoring framework. BMJ Glob Health. 2020;5:e002605.
Stephen AAI, Wurapa F, Afari EA, Sackey SO, Malm KL, Nyarko KM. Factors influencing utilization of intermittent preventive treatment for pregnancy in the Gushegu district, Ghana, 2013. Pan Afr Med J. 2016;25:4.
Sigalla GN, Mushi D, Meyrowitsch DW, Manongi R, Rogathi JJ, Gammeltoft T, et al. Intimate partner violence during pregnancy and its association with preterm birth and low birth weight in Tanzania: a prospective cohort study. PLoS ONE. 2017;12:e0172540.
Protas J, Tarimo D, Moshiro C. Determinants of timely uptake of ITN and SP (IPT) and pregnancy time protected against malaria in Bukoba. Tanzania BMC Res Notes. 2016;9:318.
WHO. Recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization; 2016.
Acknowledgements
We are grateful to all women who participated in this study, Dr. Bani Bannison, the Biomedical scientist at the Tamale Teaching Hospital, and the hardworking research assistants especially Rita Neindow and Alhassan Bukari
Funding
The authors received no funding.
Author information
Authors and Affiliations
Contributions
YNA contributed to the management of the study; was responsible for conceptualization of the project, research design; interpretation of the data, wrote the first draft of the manuscript and coordinated its multiple revisions. BB, contributed to the research design, and revisions of the manuscript. JOM contributed to the research design and proofread the final version. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Agyeman, Y.N., Bassoumah, B. & Owusu-Marfo, J. Predictors of optimal uptake of intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine and outcome of pregnancy in selected health facilities: a cross-sectional study in Northern Ghana. Malar J 22, 80 (2023). https://doi.org/10.1186/s12936-023-04501-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-023-04501-w