
Abstract
Background
The monkey parasite Plasmodium knowlesi is an emerging public health issue in Southeast Asia. In Sabah, Malaysia, P. knowlesi is now the dominant cause of human malaria. Molecular detection methods for P. knowlesi are essential for accurate diagnosis and in monitoring progress towards malaria elimination of other Plasmodium species. However, recent commercially available PCR malaria kits have unpublished P. knowlesi gene targets or have not been evaluated against clinical samples.
Methods
Two real-time PCR methods currently used in Sabah for confirmatory malaria diagnosis and surveillance reporting were evaluated: the QuantiFast™ Multiplex PCR kit (Qiagen, Germany) targeting the P. knowlesi 18S SSU rRNA; and the abTES™ Malaria 5 qPCR II kit (AITbiotech, Singapore), with an undisclosed P. knowlesi gene target. Diagnostic accuracy was evaluated using 52 P. knowlesi, 25 Plasmodium vivax, 21 Plasmodium falciparum, and 10 Plasmodium malariae clinical isolates, and 26 malaria negative controls, and compared against a validated reference nested PCR assay. The limit of detection (LOD) for each PCR method and Plasmodium species was also evaluated.
Results
The sensitivity of the QuantiFast™ and abTES™ assays for detecting P. knowlesi was comparable at 98.1% (95% CI 89.7–100) and 100% (95% CI 93.2–100), respectively. Specificity of the QuantiFast™ and abTES™ for P. knowlesi was high at 98.8% (95% CI 93.4–100) for both assays. The QuantiFast™ assay demonstrated falsely-positive mixed Plasmodium species at low parasitaemias in both the primary and LOD analysis. Diagnostic accuracy of both PCR kits for detecting P. vivax, P. falciparum, and P. malariae was comparable to P. knowlesi. The abTES™ assay demonstrated a lower LOD for P. knowlesi of ≤ 0.125 parasites/µL compared to QuantiFast™ with a LOD of 20 parasites/µL. Hospital microscopy demonstrated a sensitivity of 78.8% (95% CI 65.3–88.9) and specificity of 80.4% (95% CI 67.6–89.8) compared to reference PCR for detecting P. knowlesi.
Conclusion
The QuantiFast™ and abTES™ commercial PCR kits performed well for the accurate detection of P. knowlesi infections. Although the QuantiFast™ kit is cheaper, the abTES™ kit demonstrated a lower LOD, supporting its use as a second-line referral-laboratory diagnostic tool in Sabah, Malaysia.
Similar content being viewed by others

Background
Malaysia has made significant progress towards their World Health Organization (WHO) goal of eliminating human-only malaria by 2020, with no indigenous cases of Plasmodium falciparum or Plasmodium vivax malaria reported in 2018 [1]. However, the emergence of zoonotic transmission of the monkey parasite Plasmodium knowlesi has been less tractable to conventional malaria control efforts [2]. Within Malaysia, P. knowlesi is now the most common cause of malaria in humans, accounting for almost all reported malaria cases [1, 3], including over 2000 notifications in the state of Sabah in 2017 [2]. Confirmed P. knowlesi human infections have now been reported in all areas of Southeast Asia where the primary reservoir macaque hosts and Anopheles leucosphyrus group mosquitoes are present [4,5,6].
Microscopic assessment of Giemsa-stained blood smears remains the appropriate primary point-of-care method for malaria diagnosis in most P. knowlesi endemic countries, including Malaysia [7]. Ideally, differentiation of Plasmodium species via microscopy allows initiation of prompt and appropriate treatment and accurate public health reporting [8]. However, well-established limitations in the use of routine diagnostic malaria microscopy include the inability to differentiate between P. knowlesi and P. malariae due to similar morphology across all life-stages [9, 10]. Plasmodium knowlesi is also commonly misidentified as Plasmodium falciparum due to similarities in the early ring stage [11], and also with Plasmodium vivax in co-endemic areas such as Malaysia [10, 12] and Indonesia [13]. Commercially available pLDH-based rapid diagnostic tests (RDTs) developed for human-only Plasmodium species are known to be cross-reactive for P. knowlesi epitopes [14]. However, RDTs evaluated for P. knowlesi detection to date have demonstrated insufficient sensitivity and specificity to support their use for routine diagnosis [15,16,17,18].
Molecular methods are necessary for accurate diagnostic confirmation of P. knowlesi and other Plasmodium species, and for improved public health malaria surveillance reporting in co-endemic areas in Southeast Asia [11, 19]. In Malaysia, molecular detection methods have been implemented for routine confirmation of all malaria cases since 2014 [7]. In Sabah, the primary molecular detection method at the State Public Health Laboratory (Makmal Kesihatan Awam; MKA) is a multiplex real-time PCR using the QuantiFast™ Multiplex PCR kit (QIAGEN, Germany), which requires addition of previously published primers and probes targeting the SSU rRNA gene of P. knowlesi and other human-only Plasmodium species [20]. The commercially available abTES™ Malaria 5 qPCR II Kit (AITbiotech, Singapore) is used for subsequent validation of any inconclusive results. However, the gene target is undisclosed, and there are no published data evaluating this assay on clinical P. knowlesi samples.
This study aimed to evaluate the diagnostic accuracy and limit of detection of the two commercially available multiplex real-time PCR methods used in routine molecular diagnosis and surveillance reporting of P. knowlesi and other human-only Plasmodium species in Sabah, Malaysia.
Methods
Study details and ethical approval
Patient demographics, clinical data, and blood samples were collected as part of an ongoing prospective malaria study in Sabah, Malaysia. Patients with positive microscopy for malaria and adult healthy controls, subsequently confirmed malaria-negative via reference PCR [21, 22], were enrolled after informed consent was obtained. The study was approved by the national Medical Research Ethics Committee of Malaysia, and Menzies School of Health Research, Australia.
Blood sample procedures
Venous whole blood was collected from all participants prior to any anti-malarial treatment. Microscopic quantification of Plasmodium species parasitaemia was conducted by an experienced research microscopist in Sabah (parasites per microlitre; calculated from the number of parasites per 200 white blood cells on thick blood film, multiplied by the individual patient’s total white cell count [23] obtained from routine hospital laboratory flow cytometry (Full Blood Count results); in the absence of which, an assumption of an average WBC count of 8000/µL of blood was used). EDTA whole blood samples were stored at -80 °C and transported via liquid nitrogen shipper to Darwin, Australia. Genomic DNA was subsequently extracted from 200 µL of whole blood using QIAamp DNA Blood Mini Kits (Cat. No.: 51,106; QIAGEN) according to the manufacturer’s manual, with a final elution volume of 200 µL.
Detection of Plasmodium species using validated reference nested PCR
For P. knowlesi detection, a previously validated nested PCR targeting the SSU rRNA gene was utilized, which has a reported specificity of 100% against other Plasmodium species infecting humans and/or relevant macaque hosts, and a sensitivity of detection for P. knowlesi of 1–10 parasite genomes per microlitre [22]. A separate validated nested PCR was conducted on clinical malaria samples to identify P. falciparum, P. vivax and P. malariae [21]. Samples were then de-identified and randomly assigned onto duplicated 96-well plates for QuantiFast™ and abTES™ PCR evaluation.
Evaluation of the QuantiFast™ and abTES™ real-time PCR kits
Real-time PCR detection of Plasmodium species was performed by laboratory research members blinded to the reference nested PCR results. Both the QuantiFast™ and abTES™ real-time PCR assays were conducted once for each clinical isolate in accordance with the manufacturers’ and Sabah Public Health Laboratory protocols, using the Bio-Rad CFX96 Touch™ PCR machine (Bio-Rad, USA) and duplicated plates of genomic DNA extracted from the same isolates.
QuantiFast™ primer and probe sequences target the Plasmodium species-specific 18S SSU rRNA gene for P. knowlesi [20] and other human-only Plasmodium species [24] (described in Table 1). QuantiFast™ real-time PCR was carried out over two separate reactions due to overlapping emission wavelengths of the reporter probe (carboxyfluorescein; FAM) used to detect both P. knowlesi and P. malariae. Each final reaction volume of 25 µL consisted of 2 µL DNA template, 12.5 µL master mix, 0.5 µL ROX solution and 1.25 µL 10 × Plasmodium species-specific primer–probe mixture. In the first QuantiFast™ reaction, a monoplex real-time PCR amplification was performed to detect P. knowlesi. Cycling conditions consisted of: initial Taq activation step at 95 °C for 5 min, followed by 45 two-step cycles of denaturation at 95 °C for 30 s, and annealing/extension at 60 °C for 30 s. In the second QuantiFast™ reaction, a triplex amplification was conducted to detect P. falciparum, P. vivax, and P. malariae. Cycling conditions included: Taq activation at 95 °C for 5 min, followed by 45 cycles of denaturation at 95 °C for 45 s, and annealing/extension at 60 °C for 45 s.
The abTES™ reaction was performed using the abTES™ Malaria 5 qPCR II kit, which came with primer–probe mixtures and positive controls for detection of P. knowlesi and four human-only Plasmodium species. The reaction mixture contained 5.0 µL template DNA, 6 µL reaction mix, 2 µL of primer–probe mix, with the final volume adjusted to 25 µL with nuclease-free water. Cycling conditions included: Taq activation at 95 °C for 2 min, followed by 45 cycles of amplification at 95 °C for 5 s, and 60 °C for 20 s. The detection channels used were QUASAR 705 (P. knowlesi), FAM (P. falciparum), ROX (P. vivax), and HEX (P. malariae), with fluorescence measured at the end of each cycle of amplification.
For both QuantiFast™ and abTES™ reactions, samples were considered positive by determining the threshold cycle number (CT) at which normalized reporter dye emission raised above background noise. If the fluorescent signal did not rise above the threshold at 40 cycles (CT 40), the sample was considered negative. Due to the lack of endemic Plasmodium ovale wallikeri or Plasmodium ovale curtisi in Malaysia, detection of these Plasmodium species was not evaluated.
Limit of detection determination for each PCR method and Plasmodium species
The two PCR kits were also systematically evaluated for their respective parasite count limit of detection (LOD) for P. knowlesi, P. falciparum and P. vivax samples. In brief, a single clinical standard isolate for each Plasmodium species with high-quality research microscopic enumeration of parasite counts was utilized after reference PCR-confirmation. Individual quantified whole blood samples were then diluted using fresh malaria-negative blood in order to achieve pre-determined parasite counts, before subsequent genomic DNA extraction. The standardized concentrations included in the final analysis for each isolate were: 200, 20, 2, 0.5, 0.25, and 0.125 parasites/µL. The same clinical isolates at each parasite count concentration were used for both PCR detection kits, enabling a direct comparison of the final measured LOD. Assays were conducted in triplicate at each parasite count concentration, with the LOD defined as the lowest concentration at which a positive result was recorded for all 3 replicates.
Statistical analysis
All statistical analyses were performed using STATA v16 (TX, USA). The primary analysis compared the diagnostic accuracy of the QuantiFast™ and abTES™ kits to detect each Plasmodium species infection against the reference PCR result. Diagnostic tests for sensitivity, specificity, and positive and negative predictive values were evaluated [25], as defined below using the number of true positive (TP), false negative (FN), false positive (FP) and true negative (TN) results:
Sensitivity: proportion of those with the malaria species correctly identified = TP/(TP + FN)
Specificity: proportion of those without the malaria species correctly identified = TN/(FP + TN)
Area under the Receiver Operating Characteristic (ROC) curve: average of sensitivity and specificity
Positive Predictive Value: probability of the patient having malaria following a positive test = TP/(TP + FP)
Negative Predictive Value: probability of the patient having malaria following a negative test = TN/(TN + FN).
Exact binomial confidence intervals of 95% for each of the above diagnostic metrics were calculated and reported. Dependent comparisons between the separate PCR kits diagnostic performance on the same patient’s sample (e.g. QuantiFast™ versus abTES™ for P. knowlesi samples) were conducted using McNemar’s test [26]. Independent comparisons using the same PCR test between patients with different Plasmodium species infections were conducted using Fisher’s exact test for equality of proportions (e.g. QuantiFast™ performance for detecting P. knowlesi versus P. vivax). Overall PCR assay performance was compared by testing equality of the receiver operating characteristic (ROC) areas. Age and parasitaemia were compared across Plasmodium species results using one-way ANOVA after transformation to a normal distribution, followed by Student’s t test for pairwise comparisons; gender was compared using Chi squared test.
Results
A total of 134 samples collected from Dec 2012 to Feb 2016 were included in the primary analysis evaluating the performance of the real-time PCR detection methods, including: 52 P. knowlesi, 21 P. falciparum, 25 P. vivax, and 10 P. malariae monoinfections, and 26 malaria-negative controls. The median age for those with P. knowlesi was 35 years (range 25–47) which was higher than patients infected with other Plasmodium species (p < 0.001) (Table 2). Plasmodium knowlesi-infected patients had a geometric mean parasite count of 9435/µL, similar to those with P. vivax (p = 0.99), higher than the 1023 parasites/µL seen for P. malariae (p < 0.001), and lower than the 24,631 parasites/µL for P. falciparum (p = 0.002). Performance of the screening hospital microscopy result for detecting P. knowlesi compared to the reference PCR demonstrated a sensitivity of 78.8% (95% CI 65.3–88.9) and specificity of 80.4% (95% CI 67.6–89.8), with 21.2% of samples diagnosed as P. malariae.
Diagnostic accuracy of the QuantiFast™ and abTES™ PCR detection methods for P. knowlesi
The 52 clinical samples with confirmed P. knowlesi monoinfections were evaluated by both the QuantiFast™ and abTES™ PCR methods, and compared against the 83 P. knowlesi negative samples (other Plasmodium species and malaria negative controls combined) (Table 3). The sensitivity of the QuantiFast™ assay to detect P. knowlesi was 98.1% (95% CI 89.7–100), with 51 out of 52 samples recording positive results. The single false negative result was recorded from a 59-year old female patient with a parasitaemia of 12,968 parasites/µL. Specificity of the QuantiFast™ test was 98.8% (95% CI 93.4–100), with a single false positive result (mixed P. knowlesi/P. malariae) reported for a P. malariae monoinfection on reference PCR with a low parasite count of 224 parasites/µL. QuantiFast™ demonstrated high diagnostic accuracy with an ROC curve area of 0.98 (95% CI 0.96–1.0), a PPV of 98.1% (95% CI 89.7–100) and a NPV of 98.8% (95% CI 93.4–100).
In contrast, the abTES™ PCR was positive for all 52 P. knowlesi clinical samples, resulting in 100% sensitivity (95% CI 93.2–100). The specificity of the abTES™ assay was the same as seen for QuantiFast™ at 98.8% (95% CI 93.4–100), with a single false positive result recorded as P. knowlesi from a malaria-negative healthy control. The overall test accuracy was excellent, with a ROC curve area of 0.99 (95% CI 0.98–1.0), and a high PPV of 98.1% (95% CI 89.9–100) and NPV of 100% (95% CI 95.5–100). There were no statistically significant differences in any diagnostic metric between QuantiFast™ and abTES™.
Evaluation of QuantiFast™ and abTES™ for detecting P. vivax, P. falciparum and P. malariae
The detection of P. vivax was identical for both PCR methods, with a sensitivity for both of 100% (95% CI 86.3–100), and a specificity of 100% (95% CI 96.7–100) (Table 4). Both PCR methods had 100% sensitivity and specificity for detecting P. falciparum, including at the lowest tested parasitaemia of 1074 parasites/µL. For detection of P. malariae, the sensitivity of the QuantiFast™ was 90.0% (95% CI 55.5–99.7) due to a single false-negative result. In comparison the abTES™ correctly identified all 10 P. malariae infected samples, resulting in a sensitivity of 100% (95% CI 69.2–100); p = 0.32. The specificity for both PCR methods was 100% (95% CI 97.1–100).
QuantiFast™ and abTES™ performed equally well for detecting other Plasmodium species compared to P. knowlesi, with no statistically significant differences for any measure of diagnostic accuracy (Table 4). There were also no differences in diagnostic accuracy when comparing QuantiFast™ versus abTES™ within each separate Plasmodium species group (Table 5).
Limit of detection evaluation
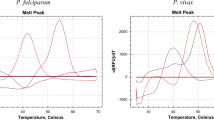
The abTES™ PCR method was shown to have a lower LOD than QuantiFast™ for all Plasmodium species, including a documented LOD at the lowest level of dilution evaluated of 0.125 parasites/µL for both P. knowlesi and P. vivax, and 0.5 parasites/µL for P. falciparum (Fig. 1).

Limit of detection of the QuantiFast™ and abTES™ assays for P. knowlesi, P. falciparum and P. vivax. Limit of detection was defined as the lowest pre-determined parasitaemia required for consistent 100% detection rate based on three replicates at each parasite count level. *False-positive results were recorded (mixed P. falciparum/P. vivax) for P. vivax monoinfections at 2 and 20 parasites/µL
The QuantiFast™ method demonstrated a LOD of 20 parasites/µL for both P. knowlesi and P. falciparum. For P. vivax, although 3 out of 3 replicates were positive at 0.25 parasites/µL, a single replicate remained negative at 0.5 parasites/µL, resulting in a final LOD of 2.0 parasites/µL. The evaluation of P. vivax for QuantiFast™ was also complicated by single replicates reported as mixed P. vivax/P. falciparum at both 2 and 20 parasites/µL.
Discussion
Both the QuantiFast™ and abTES™ real-time PCR assays evaluated in this study demonstrated high diagnostic accuracy in detecting P. knowlesi and other Plasmodium species monoinfections when compared against the reference nested PCR. The experimentally determined LOD for P. knowlesi of 20 parasites/µL for QuantiFast™ and ≤ 0.125 parasites/µL for abTES™ were also both below typical microscopic malaria detection limits [8], further highlighting their utility for confirmatory referral-laboratory diagnostic and surveillance purposes when conducted on point-of-care malaria microscopy-positive samples. Although results suggested a trend towards superior performance of the abTES™ assay and the single reaction required to conduct this assay using current protocols has logistical advantages, abTES™ (~ USD $15.40 per reaction) has a threefold higher cost than QuantiFast™ (~ USD $5.19 per reaction). Therefore, this study supports the use of the current malaria diagnostic and surveillance algorithm used by the Sabah State Public Health Laboratory in an area approaching elimination of human-only Plasmodium species, whereby all microscopy positive malaria patients are tested initially using the QuantiFast™ assay, with abTES™ used for any subsequent negative or mixed Plasmodium species infection results.
Multiple sensitive molecular methods for P. knowlesi detection have been published to date including nested [4, 22], single-step [27,28,29], and real-time PCR [30, 31], and loop-mediated isothermal amplification (LAMP) [32,33,34,35]. Although these molecular methods are directed against a range of different P. knowlesi gene targets, their reported detection limits are all below that of routine microscopic examination of malaria blood films. Real-time PCR has a number of advantages compared to conventional nested PCR, including the ability to simultaneously detect multiple Plasmodium species in a single amplification round, with higher throughput potential, and does not require manual quantification of end-points using gel electrophoresis [20]. However, real-time PCR requires expensive customized hydrolysis probes in addition to the pre-selected primers for common targets such as P. knowlesi-specific 18S SSU rRNA [36], as utilized by the QuantiFast™ assay. This validated gene target is also commonly used for both real-time and nested PCR methods for other Plasmodium species differentiation [37], due to a unique Plasmodium genus core sequence and a separate highly conserved Plasmodium species-specific region [38], resulting in improved diagnostic specificity. In this study, the target gene sequences of the abTES™ method are undisclosed, however gel electrophoresis visualization of the respective Plasmodium species-specific PCR products showed amplicon lengths consistent with standard Plasmodium 18S SSU rRNA gene sequences [21].
The use of confirmatory molecular detection methods have enabled accurate reporting of malaria trends in Malaysia demonstrating increasing P. knowlesi incidence [3], and have also provided reliable data on national and sub-national progress towards achieving elimination of other human-only Plasmodium species [2]. In other co-endemic settings in Southeast Asia, the incorporation of P. knowlesi detection into existing nucleic acid-based detection protocols would improve their use in targeted malaria surveillance strategies and accuracy of case reporting, particularly on those reported as P. malariae or indeterminate Plasmodium species infections from point-of-care microscopy [13, 19]. Additionally, this would allow improved understanding of regional diversity in the epidemiology of P. knowlesi transmission, and assist in the design of appropriate local preventive public health interventions. The use of molecular detection methods have also enabled evaluation and improvements of local treatment guidelines for knowlesi malaria, including recommending early intravenous artesunate for those with parasitaemia ≥ 20,000/µL [39], and artemisinin-based combination therapy (ACT) for uncomplicated disease in Malaysia [40, 41]. Finally, molecular detection methods may aid surveillance for another zoonotic monkey parasite, Plasmodium cynomolgi, with increasing case-reports highlighting spill-over infections occurring in humans in Sabah [42], Peninsular Malaysia [43] and Cambodia [44]. Plasmodium cynomolgi is morphologically similar to P. vivax on microscopic blood film evaluation [45], and due to being closely genetically related to P. vivax, previous PCR detection methods have also demonstrated cross-reactivity between these Plasmodium species [44]. This may have implications for accuracy of P. vivax case reporting, and potential underestimation of P. cynomolgi incidence in Southeast Asia [19].
The QuantiFast™ assay evaluated in this study is currently favoured by the Sabah State Public Health Laboratory due to its lower cost compared to abTES™, despite requiring two reactions; i.e. one monoplex and one triplex for each clinical isolate. The lengthier run time for QuantiFast™ is further compounded by a more tedious sample preparation. However, the technical issue of requiring two reactions per sample for the current QuantiFast™ laboratory protocol could be overcome by changing one of the FAM reporter dyes currently used for both P. malariae or P. knowlesi probes (Table 1), thus ensuring non-overlapping of emission wavelengths across four probes. As this study replicated the current public health surveillance protocol, the development of a new probe using a fourth colour would require additional validation. Future development of the QuantiFast™ method could, therefore, result in a single quadruplex reaction, further reducing operational cost and time, and minimization of errors, which would ideally include detection of P. cynomolgi if an appropriately validated probe becomes available.
One limitation of this study related to the secondary LOD analysis, where the lowest pre-selected parasitaemia (0.125 parasites/µL) remained above the actual limit of detection for P. knowlesi and P. vivax when using the abTES™ method. Difficulties with the conduct of PCR diagnostics in reference or research laboratory settings are evident for many pathogens, and may not reflect the ideal technical accuracy of the diagnostic assay. It is also not possible to preclude the possibility of abTES™ real-time PCR having greater sensitivity for detection of P. knowlesi as compared to the reference PCR [22]. Although unlikely, the single positive result for abTES recorded from a healthy control in an endemic area may have been a genuine asymptomatic submicroscopic P. knowlesi infection. A single P. knowlesi sample with a parasite count of 12,968/µL, a level well above the documented LOD, was found to be falsely negative on the QuantiFast™ assay, but positive with abTES™, which may have indicated a possible error during sample loading. The specificity of the QuantiFast™ assay for P. knowlesi detection was reduced by a single false-positive mixed P. knowlesi/P. malariae result for a P. malariae monoinfection of 224 parasites/µL, the corresponding abTES™ result was positive for P. malariae only. This anomaly may have been caused by unintended annealing of P. knowlesi-specific probes onto P. malariae genomic DNA [46]; a plausible scenario given primers used for the QuantiFast™ P. knowlesi monoplex are not Plasmodium species-specific. The QuantiFast™ assay also demonstrated a false-positive mixed P. falciparum/P. vivax result from a P. vivax monoinfection during the LOD analysis at low-level parasitaemia (2 and 20 parasites/µL). These findings imply that in routine surveillance in Sabah, mixed Plasmodium species infections using QuantiFast™ may require further validation.
Conclusion
The QuantiFast™ and abTES™ methods for detection of P. knowlesi infections both performed to an appropriately high standard in the primary evaluation of this study, supporting their continued usage for confirmatory malaria diagnosis and accurate malaria surveillance reporting in Sabah, Malaysia. The QuantiFast™ kit is a cost-effective initial method, with the abTES™ kit appropriate for second-line confirmation of negative or mixed Plasmodium species infections due to potentially improved sensitivity and specificity.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding authors upon reasonable request.
References
WHO. World malaria report 2019. Geneva: World Health Organization; 2019.
Cooper DJ, Rajahram GS, William T, Jelip J, Mohammad R, Benedict J, et al. Plasmodium knowlesi malaria in Sabah, Malaysia, 2015–2017: ongoing increase in incidence despite near-elimination of the human-only Plasmodium species. Clin Infect Dis. 2020;70:361–7.
Hussin N, Lim YA-L, Goh PP, William T, Jelip J, Mudin RN. Updates on malaria incidence and profile in Malaysia from 2013 to 2017. Malar J. 2020;19:55.
Singh B, Sung LK, Matusop A, Radhakrishnan A, Shamsul SS, Cox-Singh J, et al. A large focus of naturally acquired Plasmodium knowlesi infections in human beings. Lancet. 2004;363:1017–24.
Shearer FM, Huang Z, Weiss DJ, Wiebe A, Gibson HS, Battle KE, et al. Estimating geographical variation in the risk of zoonotic Plasmodium knowlesi infection in countries eliminating malaria. PLoS Negl Trop Dis. 2016;10:e0004915.
Iwagami M, Nakatsu M, Khattignavong P, Soundala P, Lorphachan L, Keomalaphet S, et al. First case of human infection with Plasmodium knowlesi in Laos. PLoS Negl Trop Dis. 2018;12:e0006244.
Ministry of Health Malaysia: Management guidelines of malaria in Malaysia. 2014.
WHO. Microscopy for the detection, identification and quantification of malaria parasites on stained thick and thin blood films in research settings. Geneva: World Health Organization; 2015. http://www.who.int/tdr/publications/microscopy_detec_ident_quantif/en.
Lee K-S, Cox-Singh J, Singh B. Morphological features and differential counts of Plasmodium knowlesi parasites in naturally acquired human infections. Malar J. 2009;8:73.
Barber BE, William T, Grigg MJ, Yeo TW, Anstey NM. Limitations of microscopy to differentiate Plasmodium species in a region co-endemic for Plasmodium falciparum, Plasmodium vivax and Plasmodium knowlesi. Malar J. 2013;12:8.
Singh B, Daneshvar C. Human infections and detection of Plasmodium knowlesi. Clin Microbiol Rev. 2013;26:165–84.
William T, Jelip J, Menon J, Anderios F, Mohammad R, Mohammad TAA, et al. Changing epidemiology of malaria in Sabah, Malaysia: increasing incidence of Plasmodium knowlesi. Malar J. 2014;13:390.
Coutrier FN, Tirta YK, Cotter C, Zarlinda I, González IJ, Schwartz A, et al. Laboratory challenges of Plasmodium species identification in Aceh Province, Indonesia, a malaria elimination setting with newly discovered P. knowlesi. PLoS Negl Trop Dis. 2018;12:e0006924.
McCutchan TF, Piper RC, Makler MT. Use of malaria rapid diagnostic test to identify Plasmodium knowlesi infection. Emerg Infect Dis. 2008;14:1750.
Kawai S, Hirai M, Haruki K, Tanabe K, Chigusa Y. Cross-reactivity in rapid diagnostic tests between human malaria and zoonotic simian malaria parasite Plasmodium knowlesi infections. Parasitol Int. 2009;58:300–2.
Barber BE, William T, Grigg MJ, Piera K, Yeo TW, Anstey NM. Evaluation of the sensitivity of a pLDH-based and an aldolase-based rapid diagnostic test for diagnosis of uncomplicated and severe malaria caused by PCR-confirmed Plasmodium knowlesi, Plasmodium falciparum, and Plasmodium vivax. J Clin Microbiol. 2013;51:1118–23.
Grigg MJ, William T, Barber BE, Parameswaran U, Bird E, Piera K, et al. Combining parasite lactate dehydrogenase-based and histidine-rich protein 2-based rapid tests to improve specificity for diagnosis of malaria due to Plasmodium knowlesi and other Plasmodium species in Sabah, Malaysia. J Clin Microbiol. 2014;52:2053–60.
Foster D, Cox-Singh J, Mohamad DS, Krishna S, Chin PP, Singh B. Evaluation of three rapid diagnostic tests for the detection of human infections with Plasmodium knowlesi. Malar J. 2014;13:60.
Anstey NM, Grigg MJ. Zoonotic malaria: the better you look, the more you find. J Infect Dis. 2019;219:679–81.
Divis PC, Shokoples SE, Singh B, Yanow SK. A TaqMan real-time PCR assay for the detection and quantitation of Plasmodium knowlesi. Malar J. 2010;9:344.
Padley D, Moody A, Chiodini P, Saldanha J. Use of a rapid, single-round, multiplex PCR to detect malarial parasites and identify the species present. Ann Trop Med Parasitol. 2003;97:131–7.
Imwong M, Tanomsing N, Pukrittayakamee S, Day NP, White NJ, Snounou G. Spurious amplification of a Plasmodium vivax small-subunit RNA gene by use of primers currently used to detect P knowlesi. J Clin Microbiol. 2009;47:4173–5.
WHO. Guidelines for the treatment of malaria. Geneva: World Health Organization; 2015.
Rougemont M, Van Saanen M, Sahli R, Hinrikson HP, Bille J, Jaton K. Detection of four Plasmodium species in blood from humans by 18S rRNA gene subunit-based and species-specific real-time PCR assays. J Clin Microbiol. 2004;42:5636–43.
McNeil BJ, Keeler E, Adelstein SJ. Primer on certain elements of medical decision making. N Engl J Med. 1975;293:211–5.
Hawass N. Comparing the sensitivities and specificities of two diagnostic procedures performed on the same group of patients. Br J Radiol. 1997;70:360–6.
Lucchi NW, Poorak M, Oberstaller J, DeBarry J, Srinivasamoorthy G, Goldman I, et al. A new single-step PCR assay for the detection of the zoonotic malaria parasite Plasmodium knowlesi. PLoS One. 2012;7:e31848.
Haanshuus CG, Mohn SC, Mørch K, Langeland N, Blomberg B, Hanevik K. A novel, single-amplification PCR targeting mitochondrial genome highly sensitive and specific in diagnosing malaria among returned travellers in Bergen, Norway. Malar J. 2013;12:26.
Stanis CS, Song BK, Chua TH, Lau YL, Jelip J. Evaluation of new multiplex PCR primers for the identification of Plasmodium species found in Sabah, Malaysia. Turkish J Med Sci. 2016;46:207–18.
Reller ME, Chen WH, Dalton J, Lichay MA, Dumler JS. Multiplex 5′ nuclease quantitative real-time PCR for clinical diagnosis of malaria and species-level identification and epidemiologic evaluation of malaria-causing parasites, including Plasmodium knowlesi. J Clin Microbiol. 2013;51:2931–8.
Lee PC, Chong ETJ, Anderios F, Lim YA, Chew CH, Chua KH. Molecular detection of human Plasmodium species in Sabah using PlasmoNex™ multiplex PCR and hydrolysis probes real-time PCR. Malar J. 2015;14:28.
Lau Y-L, Fong M-Y, Mahmud R, Chang P-Y, Palaeya V, Cheong F-W, et al. Specific, sensitive and rapid detection of human Plasmodium knowlesi infection by loop-mediated isothermal amplification (LAMP) in blood samples. Malar J. 2011;10:197.
Britton S, Cheng Q, Grigg MJ, William T, Anstey NM, McCarthy JS. A sensitive, colorimetric, high-throughput loop-mediated isothermal amplification assay for the detection of Plasmodium knowlesi. Am J Trop Med Hyg. 2016;95:120–2.
Iseki H, Kawai S, Takahashi N, Hirai M, Tanabe K, Yokoyama N, et al. Evaluation of a loop-mediated isothermal amplification method as a tool for diagnosis of infection by the zoonotic simian malaria parasite Plasmodium knowlesi. J Clin Microbiol. 2010;48:2509–14.
Piera KA, Aziz A, William T, Bell D, González IJ, Barber BE, et al. Detection of Plasmodium knowlesi, Plasmodium falciparum and Plasmodium vivax using loop-mediated isothermal amplification (LAMP) in a co-endemic area in Malaysia. Malar J. 2017;16:29.
Link L, Bart A, Verhaar N, van Gool T, Pronk M, Scharnhorst V. Molecular detection of Plasmodium knowlesi in a Dutch traveler by real-time PCR. J Clin Microbiol. 2012;50:2523–4.
Li J, Wirtz RA, Mcconkey GA, Sattabongkot J, Waters AP, Rogers MJ, et al. Plasmodium: genus-conserved primers for species identification and quantitation. Exp Parasitol. 1995;81:182–90.
Waters A, McCutchan T. Partial sequence of the asexually expressed SU rRNA gene of Plasmodium vivax. Nucleic Acids Res. 1989;17:2135.
Barber BE, William T, Grigg MJ, Menon J, Auburn S, Marfurt J, et al. A prospective comparative study of knowlesi, falciparum, and vivax malaria in Sabah, Malaysia: high proportion with severe disease from Plasmodium knowlesi and Plasmodium vivax but no mortality with early referral and artesunate therapy. Clin Infect Dis. 2013;56:383–97.
Grigg MJ, William T, Barber BE, Rajahram GS, Menon J, Schimann E, et al. Age-related clinical spectrum of Plasmodium knowlesi malaria and predictors of severity. Clin Infect Dis. 2018;67:350–9.
Grigg MJ, William T, Menon J, Dhanaraj P, Barber BE, Wilkes CS, et al. Artesunate–mefloquine versus chloroquine for treatment of uncomplicated Plasmodium knowlesi malaria in Malaysia (ACT KNOW): an open-label, randomised controlled trial. Lancet Infect Dis. 2016;16:180–8.
Grignard L, Shah S, Chua TH, William T, Drakeley CJ, Fornace KM. Natural human infections with Plasmodium cynomolgi and other malaria species in an elimination setting in Sabah, Malaysia. J Infect Dis. 2019;220:1946–9.
Ta TH, Hisam S, Lanza M, Jiram AI, Ismail N, Rubio JM. First case of a naturally acquired human infection with Plasmodium cynomolgi. Malar J. 2014;13:68.
Imwong M, Madmanee W, Suwannasin K, Kunasol C, Peto TJ, Tripura R, et al. Asymptomatic natural human infections with the simian malaria parasites Plasmodium cynomolgi and Plasmodium knowlesi. J Infect Dis. 2018;219:695–702.
Coatney GR, Collins WE, Warren M, Contacos PG. The primate malarias. Bethesda MD: US Department of Health Education and Welfare; 1971.
Chua KH, Lim SC, Ng CC, Lee PC, Lim YAL, Lau TP, et al. Development of high resolution melting analysis for the diagnosis of human malaria. Sci Rep. 2015;5:15671.
Acknowledgements
We thank the study participants, the IDSKKS malaria research team nursing and laboratory staff, Malaysian Ministry of Health hospital directors and clinical staff at Queen Elizabeth Hospital and Keningau and Ranau District Hospitals as well as the Sabah State Public Health Laboratory. We also recognise the support from Dato’ Dr. Goh Pik Pin and the Clinical Research Centre, Queen Elizabeth Hospital, Kota Kinabalu, Sabah. We would like to thank the Director General of Health Malaysia for permission to publish this article.
Funding
This work was supported by the National Health and Medical Research Council, Australia (Grant Numbers 1037304 and 1045156; fellowships to NMA [1042072], BEB [1088738]; MJG [1138860]); ‘Improving Health Outcomes in the Tropical North: A Multidisciplinary Collaboration (HOT NORTH)’ [grant number 1131932]; the National Institutes of Health, USA (Grant Number R01AI116472-01); and the Australian Centre of Research Excellence in Malaria Elimination. This work was partly supported by FRGS0388 awarded to THC. NAN was supported by FRGS0388 awarded to THC. AFT is supported via a Malaysia Australia Colombo Plan Commemoration (MACC) and Australian Government Research Training Program (RTP) Scholarship at Charles Darwin University.
Author information
Authors and Affiliations
Contributions
TW, GSR, DJC, BEB, NMA, THC and MJG led the conception, study design and data collection. NAN, KAP, AFT and YLL performed laboratory testing. AFT, NAN, YLL, THC and MJG interpreted and analysed the data, wrote and revised the manuscript. NAN was supervised by THC. THC and MJG co-supervised this work. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Medical Research and Ethics Committee, Ministry of Health, Malaysia (NMRR-10-754-6684), and Menzies School of Health Research, Australia (HREC-2010-1431).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nuin, N.A., Tan, A.F., Lew, Y.L. et al. Comparative evaluation of two commercial real-time PCR kits (QuantiFast™ and abTES™) for the detection of Plasmodium knowlesi and other Plasmodium species in Sabah, Malaysia. Malar J 19, 306 (2020). https://doi.org/10.1186/s12936-020-03379-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-020-03379-2