
Abstract
Background
Interleukin-4(IL-4) is a critical inflammatory cytokine and has been involved in pathogenesis of cancer. To date, several studies have investigated the association between IL-4 intron 3 variable number of tandem repeats (VNTR) polymorphism and cancer risk in humans; however, the results remain controversial. We performed this meta-analysis to find a more conclusive association between this polymorphism and cancer risk.
Methods
Eight eligible case–control studies were identified through searching electronic databases, including 1583 cases and 1638 controls. Odds ratio (OR) and corresponding 95% confidence interval (CI) were used to estimate the strength of the association.
Results
The results of overall analyses indicated that the variant RP2 allele was associated with a decreased cancer risk compared with the RP1 allele (RP2/RP2 vs. RP1/RP1, OR = 0.64, 95% CI = 0.44-0.94; RP2/RP2 vs. RP1/RP1 + RP1/RP2, OR = 0.75, 95% CI = 0.60-0.92; RP2 vs. RP1, OR = 0.72, 95% CI = 0.56-0.92). In subgroup analyses stratified by ethnicity, there was evidence in the Asian population for an association between this polymorphism and cancer risk (RP2/RP2 vs. RP1/RP1 + RP1/RP2, OR = 0.79, 95% CI = 0.63-0.99; RP2 vs. RP1, OR = 0.77, 95% CI = 0.61-0.97).
Conclusions
IL-4 intron 3 VNTR polymorphism could influence the risk of human cancer. Due to the limitations of this meta-analysis, further well-designed and functional researches should be performed to validate our results.
Similar content being viewed by others


Introduction
Cancer is currently a major health burden in the world which results from complicated interactions between genetic and environmental factors [1],[2]. Epidemiological studies have revealed that chronic inflammation could pose a risk factor for several cancers [3]. Moreover, inflammation has been linked to the pathogenesis of tumors in up to 15% of human cancers [4]. Cytokines are important inflammatory mediators and there is evidence that human predisposition to cancer could be influenced by polymorphisms located in genes encoding cytokines and their receptors [5].
Interleukin-4(IL-4), produced by activated Th2 type CD4+ T cells, represents a key differentiation cytokine that induces development of Th2 subset of lymphocytes, which is responsible for surveillance and clearance of tumor cells by activation of granulocytes and eosinophils, as well as inhibition of angiogenesis [6],[7]. Moreover, Th2 subset is involved in antagonizing IFN-γ function, B cell switching to IgE production, inhibiting macrophage activation and some studies have revealed its anti-tumor activity on several cancers such as colon, breast and renal carcinoma [8],[9]. However, IL-4 plays a bilateral role in the control of tumor growth. It has been reported that IL-4 could promote the initiation, progression and spread of head and neck squamous carcinoma [10]–[13]. Liang et al. [14] have found that there was a significantly higher level of IL-4 mRNA in patients with gastric cancer in stage III and IV than that in stage I and II. In addition, IL-4 also disturbs anti-tumor immunity by down-regulating the expression of Th1 cytokines [10],[15] and impairing the CD8+ T cell immune response in the tumor microenvironment [6],[11].
The gene encoding IL-4 is located on chromosome 5q31.1 [16]. A rapidly growing number of epidemiologic studies have been conducted to investigate the effect of several IL-4 polymorphisms on human cancer risk. One important polymorphism is located in the intron 3 of IL-4 gene and is composed of a 70-bp sequence of variable number of tandem repeats (VNTR) [17],[18]. It has been proved that the IL-4 intron 3 polymorphism might influence the production of IL-4, with the RP1 (two 70-bp repeats) allele enhancing IL-4 expression compared with RP2 (three 70-bp repeats) allele [18],[19].
To date, several case–control studies have been carried out to explore the linkage between IL-4 intron 3 VNTR polymorphism and the risk of several human cancers. However, results from different articles remain controversial. We performed this meta-analysis based on the published studies to make a more conclusive evaluation of the association between this polymorphism and cancer risk.
Materials and methods
Search strategy
Relevant articles indexed in PubMed and Cochrane Library (from inception to July 30, 2014) were independently searched by two authors, using the key words as follows: (“interleukin-4” or “interleukin 4” or “IL-4” or “IL 4”) and (“tumor” or “cancer” or “carcinoma” or “neoplasm” or “malignancy”) and (“polymorphism” or “polymorphisms” or “SNP” or “variant” or “variation”). The retrieved results were filtered to English language papers. An additional manual search was performed among the references of relevant articles and related articles in PubMed.
Study identification
All the retrieved articles were reviewed by two authors independently to select studies for inclusion. As for studies with overlapping data reported by the same investigators, the articles with the most complete data were eligible. Studies included in this meta-analysis should meet the following predetermined criteria: 1) case–control design, 2) evaluation of the IL-4 intron 3 VNTR polymorphism and cancer risk, 3) effective estimation of odd ratio (OR) with 95% confidence interval (CI), or enough data to allow calculation of these two statistics. The major criteria for exclusion were: 1) not relevant to IL-4 polymorphism and cancer risk, 2) not with a case–control design (eg, animal studies, reviews, case reports, letters, and editorials), 3) study on inherited cancers, 4) duplicate data.
Data extraction
Two authors checked each included article independently to extract the necessary data. The following information were collected: first author’s last name, publication year, ethnicity of the study population, country where the study conduct, sample size, source of the control groups (hospital- or population-based), the distribution of variant genotypes of both cases and controls.
Statistical analysis
Pooled analysis was performed to estimate the strength of the association between IL-4 polymorphism and cancer risk using the odds ratio (OR) with 95% confidence interval (CI). The pooled ORs were calculated by a co-dominant model (RP2/RP2 vs. RP1/RP1, RP1/RP2 vs. RP1/RP1), a dominant model (RP2/RP2 + RP1/RP2 vs. RP1/RP1), a recessive model (RP2/RP2 vs. RP1/RP1 + RP1/RP2), and an allelic model (RP2 vs. RP1). The values of the pooled ORs were tested by Z-test [20]. Hardy-Weinberg equilibrium (HWE) was estimated using goodness-of-fit test based on the chi-square test in the control groups of each study [21].
Heterogeneity among the included studies was evaluated using chi-square based on Q-test and I2 statistic [22]. Pooled ORs were calculated using a fixed (Mantel-Haenszel method [23]) or random (DerSimonian-Laird method [24]) effective model according to the absence (I2 < 50%) or presence (I2 > 50%) of heterogeneity. Sensitivity analyses were conducted by removing one study each time to assess the stability of the results. The potential publication bias of the included studies was evaluated by Begg’s funnel plots graphically and Egger’s linear regression test [25].
All the tests were two sides and it is deemed to be statistically significant when P < 0.05. All the statistical analyses were carried out with Stata/SE software version 12.0 (StataCorp LP, College Station, TX, USA).
Results
Literature search and characteristics of eligible studies
Our search in electronic databases identified 444 records. Four hundred and one records were excluded after reviewing titles and abstracts and we gained 43 useful studies. After full-text reviewing, we excluded 35 studies and listed the reasons for their exclusion in Figure 1.

Flow diagram of the study identification process.
There were 8 studies [26]–[33] suitable for this meta-analysis finally, involving a total of 1583 cases and 1638 controls. Seven of the included studies were conducted on an Asian population and the rest one was on a Caucasian population. Characteristics of eligible studies were summarized in Table 1.
Quantitative synthesis
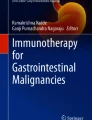
The main results of this meta-analysis were presented in Table 2. In the overall analyses, there was an association between the variant genotypes and cancer risk in several genetic models. Significantly decreased cancer risk was observed in the co-dominant model (RP2/RP2 vs. RP1/RP1, OR = 0.64, 95% CI = 0.44-0.94), recessive model (RP2/RP2 vs. RP1/RP1 + RP1/RP2, OR = 0.75, 95% CI = 0.60-0.92), and allelic model (RP2 vs. RP1, OR = 0.72, 95% CI = 0.56-0.92) (Figure 2). In subgroup analyses stratified by ethnicity, there was evidence in the Asian population for an association between this polymorphism and cancer risk (RP2/RP2 vs. RP1/RP1 + RP1/RP2, OR = 0.79, 95% CI = 0.63-0.99; RP2 vs. RP1, OR = 0.77, 95% CI = 0.61-0.97). According to a specific cancer type, declined risk among studies of bladder cancer was found in all genetic models.

Forest plot for the overall association between IL-4 intron 3 VNTR polymorphism and cancer risk for an allelic model (RP2 versus RP1).
In addition, we omitted 1 study in which the control group was not in agreement with HWE [30] and repeated the meta-analysis. The result was consist with the overall analyses (RP1/RP2 vs. RP1/RP1, OR = 0.74, 95% CI = 0.49-1.13; RP2/RP2 vs. RP1/RP1, OR = 0.62, 95% CI = 0.41-0.95; RP2/RP2 + RP1/RP2 vs. RP1/RP1, OR = 0.71, 95% CI = 0.46-1.09; RP2/RP2 vs. RP1/RP1 + RP1/RP2, OR = 0.78, 95% CI = 0.61-0.98; RP2 vs. RP1, OR = 0.71, 95% CI = 0.53-0.94).
Test for heterogeneity and sensitivity analysis
There was significant heterogeneity in the overall analyses for the comparison of the allelic model (RP2 vs. RP1: P = 0.002 and I2 = 68.8% for heterogeneity). Sensitivity analyses were carried out to explore the origin of heterogeneity. Two studies [26],[33] were under suspicion and the heterogeneity was remarkably decreased after omitting these two articles (RP2 vs. RP1: OR = 0.87, 95% CI = 0.76-0.99, P = 0.546 and I2 = 0.00% for heterogeneity). Moreover, the pooled ORs in all genetic models were not altered qualitatively when any single study was removed, which indicated the results of the present meta-analysis were relatively stable and credible (Figure 3).

Sensitivity analysis for the overall association between IL-4 intron 3 VNTR polymorphism and cancer risk for an allelic model (RP2 versus RP1).
Publication bias
The publication bias of eligible literatures was assessed by Begg’s funnel plots graphically and Egger’s test statistically. The shapes of funnel plots in all models did not show any evidence of an obvious asymmetry (Figure 4). Meanwhile, the Egger’s test indicated no publication bias either (RP1/RP2 vs. RP1/RP1: P = 0.631, RP2/RP2 vs. RP1/RP1: P = 0.051, RP2/RP2+ RP1/RP2 vs. RP1/RP1: P = 0.462, RP2/RP2 vs. RP1/RP1 + RP1/RP2: P = 0.055, RP2 vs. RP1: P = 0.066).

Begg’s funnel plot for the overall association between IL-4 intron 3 VNTR polymorphism and cancer risk for an allelic model (RP2 versus RP1).
Discussion
Cancer is a heterogeneous disease resulting from genetics, environmental factors, and their interactions, the clinical outcome of which is difficult to predict [34]–[36]. Inflammation has been associated with variant malignancies. Elevated levels of inflammatory cytokines have been linked to inflammatory exacerbation. As a critical anti-inflammatory cytokine, IL-4 has implicated in the pathogenesis of various cancers. Elevated plasma levels of IL-4 were correlated with risk of acute myeloid leukemia, melanoma, head and neck squamous cell carcinoma, non-small-cell lung cancer, prostate, colon, breast, renal cell cancer [37]–[40], and were associated with poor prognosis in non-Hodgkin lymphoma [41]. More specifically, several polymorphisms of the gene encoding IL-4 have been proved to be risk factors for cancer [33],[42]–[45]. Besides the most common polymorphisms, −590C > T(rs2243250) and -33 T > C(rs2070874), the intron 3 VNTR polymorphism also plays an important role in alteration of IL-4 production.
To our knowledge, Li et al. performed a meta-analysis about the association of IL-4 intron 3 VNTR polymorphism and cancer risk [46]. Their results showed that there was no association between this polymorphism and cancer risk. However, some concerns were related to this meta-analysis. First, the sample size was relatively small, involving 791 cases and 772 controls from 5 case–control studies. Second, there was significant heterogeneity and the origin of heterogeneity was not well explored. In addition, several important studies about the association of IL-4 intron 3 VNTR polymorphism and cancer risk have been published recently.
The present meta-analysis, including 1583 cases and 1638 controls from 8 case–control studies, comprehensively assessed the association between IL-4 intron 3 VNTR polymorphism and risk of human cancers. We found an association between IL-4 intron 3 VNTR polymorphism and cancer risk. Our results indicated the RP1 allele might be a risk factor for malignancies. The results were robust because the pooled ORs did not alter in sensitivity analyses. Stratified analyses suggested that the association was mainly in Asian populations and in bladder cancer. Since there was significant heterogeneity in several genetic models, two studies were founded out by sensitivity analyses. We re-checked these 2 studies and found that 1 study [26] was the only population-based design in the 8 included studies and the other one [33] was the only one that conducted on a Caucasian population. In addition, we pooled the data from studies on diverse cancer types, which might contribute to some extent of the heterogeneity. Different cancer types might give rise to different host responses, and the interactions between different environmental factors and host might also influence the susceptibility to different cancer types. Because of the limited study number, we could not perform a meta-regression analysis to estimate the extent of heterogeneity from different cancer types.
Some limitations of our meta-analysis should be pointed out. First, the pooled outcomes were calculated based on unadjusted estimates, which limited a more precise evaluation on adjusted estimates by several important factors like age, sex, lifestyle and etc. Only one study reported that IL-4 intron 3 VNTR polymorphism was associated with oral and pharyngeal carcinoma risk, which interacted with alcohol drinking [32]. Thus, lacking of these original information limited supplementary assessment of the potential interactions because gene-gene, gene-environment interactions and other polymorphisms of the same gene might influence cancer predisposition. Second, most of the studies included in the present meta-analysis only focused on the relationship between IL-4 intron 3 VNTR polymorphism and cancer risk, which made it hard to assess the effects of IL-4 haplotypes composed of different IL-4 polymorphisms on carcinogenesis. There was evidence that IL-4 -590C > T(rs2243250), −33 T > C(rs2070874) polymorphisms were associated with cancer risk [42],[43],[45]. Thus, the status of other IL-4 polymorphisms might cover up the impact of intron 3 VNTR polymorphism on carcinogenesis. Third, limited study number restricted us to perform additional subgroup analyses. Forth, although there was no publication bias statistically, the potential publication bias might exist because some studies with negative results were not published. Moreover, there was only one study conducted on the Caucasian population and no study on the African population in this meta-analysis.
Despite these limitations, advantages in our meta-analysis should be also acknowledged. First, the statistical power was definitely increased by pooling a substantial number of cases and controls. Second, all the eligible studies met the inclusion and exclusion criteria strictly and completely. Third, no publication bias was detected through Begg’s funnel plots and Egger’s test, which indicated that the pooled results should be unbiased.
In conclusion, the results of this meta-analysis were statistically credible. The relationship between IL-4 intron 3 VNTR polymorphism and cancer risk was assessed and this polymorphism was associated with cancer risk, mainly in Asians. To draw a more precise conclusion, further studies should be carried out with more detailed individual information, concerning the effects of other polymorphisms and haplotypes, enrolling larger sample size of cases and well-matched controls, especially in Caucasians and Africans, to validate the role of IL-4 polymorphism in carcinogenesis.
References
Hoeijmakers JH: Genome maintenance mechanisms for preventing cancer. Nature. 2001, 411 (6835): 366-374. 10.1038/35077232.
Bredberg A: Cancer: more of polygenic disease and less of multiple mutations? A quantitative viewpoint. Cancer. 2011, 117 (3): 440-445. 10.1002/cncr.25440.
Wang S, Liu Z, Wang L, Zhang X: NF-kappaB signaling pathway, inflammation and colorectal cancer. Cell Mol Immunol. 2009, 6 (5): 327-334. 10.1038/cmi.2009.43.
Kuper H, Adami HO, Trichopoulos D: Infections as a major preventable cause of human cancer. J Intern Med. 2000, 248 (3): 171-183. 10.1046/j.1365-2796.2000.00742.x.
Bidwell J, Keen L, Gallagher G, Kimberly R, Huizinga T, McDermott MF, Oksenberg J, McNicholl J, Pociot F, Hardt C, D’Alfonso S: Cytokine gene polymorphism in human disease: on-line databases. Genes Immun. 1999, 1 (1): 3-19. 10.1038/sj.gene.6363645.
Olver S, Apte S, Baz A, Kienzle N: The duplicitous effects of interleukin 4 on tumour immunity: how can the same cytokine improve or impair control of tumour growth?. Tissue Antigens. 2007, 69 (4): 293-298. 10.1111/j.1399-0039.2007.00831.x.
Swain SL, Weinberg AD, English M, Huston G: IL-4 directs the development of Th2-like helper effectors. J Immunol. 1990, 145 (11): 3796-3806.
Toi M, Bicknell R, Harris AL: Inhibition of colon and breast carcinoma cell growth by interleukin-4. Cancer Res. 1992, 52 (2): 275-279.
Yu SJ, Kim HS, Cho SW, Sohn J: IL-4 inhibits proliferation of renal carcinoma cells by increasing the expression of p21WAF1 and IRF-1. Exp Mol Med. 2004, 36 (4): 372-379. 10.1038/emm.2004.49.
Myers JN, Yasumura S, Suminami Y, Hirabayashi H, Lin W, Johnson JT, Lotze MT, Whiteside TL: Growth stimulation of human head and neck squamous cell carcinoma cell lines by interleukin 4. Clin Cancer Res. 1996, 2 (1): 127-135.
Manchanda P, Sharma SC, Das SN: Differential regulation of IL-2 and IL-4 in patients with tobacco-related oral squamous cell carcinoma. Oral Dis. 2006, 12 (5): 455-462. 10.1111/j.1601-0825.2005.01220.x.
Agarwal A, Rani M, Saha GK, Valarmathi TM, Bahadur S, Mohanti BK, Das SN: Disregulated expression of the Th2 cytokine gene in patients with intraoral squamous cell carcinoma. Immunol Investig. 2003, 32 (1–2): 17-30. 10.1081/IMM-120019205.
Yamamoto T, Yoneda K, Ueta E, Hirota J, Osaki T: Serum cytokine levels in patients with oral mucous membrane disorders. J Oral Pathol Med. 1991, 20 (6): 275-279. 10.1111/j.1600-0714.1991.tb00927.x.
Liang J, Li Y, Liu X, Xu X, Zhao Y: Relationship between cytokine levels and clinical classification of gastric cancer. Asian Pac J Cancer Prev. 2011, 12 (7): 1803-1806.
Goto T, Nishizono A, Fujioka T, Ikewaki J, Mifune K, Nasu M: Local secretory immunoglobulin A and postimmunization gastritis correlate with protection against Helicobacter pylori infection after oral vaccination of mice. Infect Immun. 1999, 67 (5): 2531-2539.
Serefoglou Z, Yapijakis C, Nkenke E, Vairaktaris E: Genetic association of cytokine DNA polymorphisms with head and neck cancer. Oral Oncol. 2008, 44 (12): 1093-1099. 10.1016/j.oraloncology.2008.02.012.
Rosenwasser LJ, Klemm DJ, Dresback JK, Inamura H, Mascali JJ, Klinnert M, Borish L: Promoter polymorphisms in the chromosome 5 gene cluster in asthma and atopy. Clin Exp Allergy. 1995, 25 (Suppl 2): 74-78. 10.1111/j.1365-2222.1995.tb00428.x. discussion 95–76
Mout R, Willemze R, Landegent JE: Repeat polymorphisms in the interleukin-4 gene (IL4). Nucleic Acids Res. 1991, 19 (13): 3763-10.1093/nar/19.13.3763.
Nakashima H, Miyake K, Inoue Y, Shimizu S, Akahoshi M, Tanaka Y, Otsuka T, Harada M: Association between IL-4 genotype and IL-4 production in the Japanese population. Genes Immun. 2002, 3 (2): 107-109. 10.1038/sj.gene.6363830.
Breslow NE, Day NE: Statistical methods in cancer research. Volume II--The design and analysis of cohort studies.IARC Sci Publ 1987, (82):1–406.,
Haber M: Exact significance levels of goodness-of-fit tests for the Hardy-Weinberg equilibrium. Hum Hered. 1981, 31 (3): 161-166. 10.1159/000153199.
Higgins JP, Thompson SG, Deeks JJ, Altman DG: Measuring inconsistency in meta-analyses. BMJ. 2003, 327 (7414): 557-560. 10.1136/bmj.327.7414.557.
Mantel N, Haenszel W: Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959, 22 (4): 719-748.
DerSimonian R, Laird N: Meta-analysis in clinical trials. Control Clin Trials. 1986, 7 (3): 177-188. 10.1016/0197-2456(86)90046-2.
Sterne JA, Gavaghan D, Egger M: Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. 2000, 53 (11): 1119-1129. 10.1016/S0895-4356(00)00242-0.
Tsai FJ, Chang CH, Chen CC, Hsia TC, Chen HY, Chen WC: Interleukin-4 gene intron-3 polymorphism is associated with transitional cell carcinoma of the urinary bladder. BJU Int. 2005, 95 (3): 432-435. 10.1111/j.1464-410X.2005.05315.x.
Tsai MH, Chen WC, Tsai CH, Hang LW, Tsai FJ: Interleukin-4 gene, but not the interleukin-1 beta gene polymorphism, is associated with oral cancer. J Clin Lab Anal. 2005, 19 (3): 93-98. 10.1002/jcla.20060.
Lai KC, Chen WC, Jeng LB, Li SY, Chou MC, Tsai FJ: Association of genetic polymorphisms of MK, IL-4, p16, p21, p53 genes and human gastric cancer in Taiwan. Eur J Surg Oncol. 2005, 31 (10): 1135-1140. 10.1016/j.ejso.2005.07.005.
Kesarwani P, Ahirwar DK, Mandhani A, Mittal RD: Association between −174 G/C promoter polymorphism of the interleukin-6 gene and progression of prostate cancer in North Indian population. DNA Cell Biol. 2008, 27 (9): 505-510. 10.1089/dna.2008.0742.
Konwar R, Chaudhary P, Kumar S, Mishra D, Chattopadhyay N, Bid HK: Breast cancer risk associated with polymorphisms of IL-1RN and IL-4 gene in Indian women. Oncol Res. 2009, 17 (8): 367-372. 10.3727/096504009788428442.
Shekari M, Kordi-Tamandani DM, MalekZadeh K, Sobti RC, Karimi S, Suri V: Effect of anti-inflammatory (IL-4, IL-10) cytokine genes in relation to risk of cervical carcinoma. Am J Clin Oncol. 2012, 35 (6): 514-519. 10.1097/COC.0b013e31822d9c12.
Yang CM, Chen HC, Hou YY, Lee MC, Liou HH, Huang SJ, Yen LM, Eng DM, Hsieh YD, Ger LP: A high IL-4 production diplotype is associated with an increased risk but better prognosis of oral and pharyngeal carcinomas. Arch Oral Biol. 2014, 59 (1): 35-46. 10.1016/j.archoralbio.2013.09.010.
Bozdogan ST, Erol B, Dursun A, Bozdogan G, Donmez I, Mungan NA, Seydaoglu G: The IL-1RN and IL-4 gene polymorphisms are potential genetic markers of susceptibility to bladder cancer: a case–control study.World J Urol 2014, [Epub ahead of print].,
Zhang H, Xu Y, Zhang Z, Liu R, Ma B: Association between COX-2 rs2745557 polymorphism and prostate cancer risk: a systematic review and meta-analysis. BMC Immunol. 2012, 13: 14-10.1186/1471-2172-13-14.
Zhang H, Qi C, Li L, Luo F, Xu Y: Clinical significance of NUCB2 mRNA expression in prostate cancer. J Exp Clin Cancer Res. 2013, 32 (1): 56-10.1186/1756-9966-32-56.
Abaza MS, Bahman AM, Al-Attiyah RJ, Kollamparambil AM: Synergistic induction of apoptosis and chemosensitization of human colorectal cancer cells by histone deacetylase inhibitor, scriptaid, and proteasome inhibitors: potential mechanisms of action. Tumour Biol. 2012, 33 (6): 1951-1972. 10.1007/s13277-012-0456-6.
Sanchez-Correa B, Bergua JM, Campos C, Gayoso I, Arcos MJ, Banas H, Morgado S, Casado JG, Solana R, Tarazona R: Cytokine profiles in acute myeloid leukemia patients at diagnosis: survival is inversely correlated with IL-6 and directly correlated with IL-10 levels. Cytokine. 2013, 61 (3): 885-891. 10.1016/j.cyto.2012.12.023.
Porter GA, Abdalla J, Lu M, Smith S, Montgomery D, Grimm E, Ross MI, Mansfield PF, Gershenwald JE, Lee JE: Significance of plasma cytokine levels in melanoma patients with histologically negative sentinel lymph nodes. Ann Surg Oncol. 2001, 8 (2): 116-122. 10.1007/s10434-001-0116-3.
Lathers DM, Young MR: Increased aberrance of cytokine expression in plasma of patients with more advanced squamous cell carcinoma of the head and neck. Cytokine. 2004, 25 (5): 220-228. 10.1016/j.cyto.2003.11.005.
Shurin MR, Lu L, Kalinski P, Stewart-Akers AM, Lotze MT: Th1/Th2 balance in cancer, transplantation and pregnancy. Springer Semin Immunopathol. 1999, 21 (3): 339-359. 10.1007/BF00812261.
Mellgren K, Hedegaard CJ, Schmiegelow K, Muller K: Plasma cytokine profiles at diagnosis in pediatric patients with non-hodgkin lymphoma. J Pediatr Hematol Oncol. 2012, 34 (4): 271-275. 10.1097/MPH.0b013e3182431e02.
Pan XF, Wen Y, Loh M, Wen YY, Yang SJ, Zhao ZM, Tian Z, Huang H, Lan H, Chen F, Soong R, Yang CX: Interleukin-4 and −8 gene polymorphisms and risk of gastric cancer in a population in Southwestern China. Asian Pac J Cancer Prev. 2014, 15 (7): 2951-2957. 10.7314/APJCP.2014.15.7.2951.
Jin T, Li X, Zhang J, Wang H, Geng T, Li G, Gao G, Chen C: Genetic association between selected cytokine genes and glioblastoma in the Han Chinese population. BMC Cancer. 2013, 13: 236-10.1186/1471-2407-13-236.
Monroy CM, Cortes AC, Lopez MS, D’Amelio AM, Etzel CJ, Younes A, Strom SS, El-Zein RA: Hodgkin disease risk: role of genetic polymorphisms and gene-gene interactions in inflammation pathway genes. Mol Carcinog. 2011, 50 (1): 36-46. 10.1002/mc.20688.
Olson SH, Orlow I, Simon J, Tommasi D, Roy P, Bayuga S, Ludwig E, Zauber AG, Kurtz RC: Allergies, variants in IL-4 and IL-4R alpha genes, and risk of pancreatic cancer. Cancer Detect Prev. 2007, 31 (5): 345-351. 10.1016/j.cdp.2007.10.002.
Zhenzhen L, Xianghua L, Qingwei W, Zhan G, Ning S: Three common polymorphisms in the IL-4 gene and cancer risk: a meta-analysis involving 5,392 cases and 6,930 controls. Tumour Biol. 2013, 34 (4): 2215-2224. 10.1007/s13277-013-0761-8.
Acknowledgements
This work was granted by National Natural Science Foundation of China (Grant No.91229104).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
YD and SZ conceived and designed the experiments; YD and HC performed the experiments; YD and CP analyzed the data; YD and JS wrote the paper. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Duan, Y., Pan, C., Shi, J. et al. Association between interleukin-4 gene intron 3 VNTR polymorphism and cancer risk. Cancer Cell Int 14, 131 (2014). https://doi.org/10.1186/s12935-014-0131-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12935-014-0131-7