
Abstract
Background
A compromised cardiac autonomic function has been found in subjects with insulin resistance related disorders such as obesity, impaired glucose tolerance (IGT) and type 2 diabetes and confers an increased risk of adverse cardiovascular outcomes. Growing evidence indicate that 1 h plasma glucose levels (1hPG) during an oral glucose tolerance test (OGTT) ≥ 155 mg/dl identify amongst subjects with normal glucose tolerance (NGT) a new category of prediabetes (NGT 1 h-high), harboring an increased risk of cardiovascular organ damage. In this study we explored the relationship between 1 h post-load hyperglycemia and cardiac autonomic dysfunction.
Methods
Presence of cardiac autonomic neuropathy (CAN) defined by cardiovascular autonomic reflex tests (CARTs) and heart rate variability (HRV), assessed by 24-h electrocardiography were evaluated in 88 non-diabetic subjects subdivided on the basis of OGTT data in: NGT with 1 h PG < 155 mg/dl (NGT 1 h-low), NGT 1 h-high and IGT.
Results
As compared to subjects with NGT 1 h-low, those with NGT 1 h-high and IGT were more likely to have CARTs defined CAN and reduced values of the 24 h time domain HVR parameters including standard deviation of all normal heart cycles (SDNN), standard deviation of the average RR interval for each 5 min segment (SDANN), square root of the differences between adjacent RR intervals (RMSSD), percentage of beats with a consecutive RR interval difference > 50 ms (PNN50) and Triangular index. Univariate analyses showed that 1hPG, but not fasting and 2hPG, was inversely associated with all the explored HVR parameters and positively with CARTs determined presence of CAN. In multivariate regression analysis models including several confounders we found that 1hPG was an independent contributor of HRV and presence of CAN.
Conclusion
Subjects with 1hPG ≥ 155 mg/dl have an impaired cardiac autonomic function.
Similar content being viewed by others

Background
Type 2 diabetes mellitus (T2DM) poses a significant health challenge nowadays. It can affect major organ systems, leading to complications including, among others, autonomic dysfunction and cardiac autonomic neuropathy (CAN) [1,2,3]. The prevalence of CAN ranges from 31 to 73% in patients with T2DM and it increases along with disease duration [2,3,4].
Since T2DM is spreading around the world, incidence of CAN is expected to significantly increase among individuals with T2DM in the coming decades [3,4,5]. Longitudinal studies indicate that CAN is a predictor of adverse cardio-cerebrovascular events in diabetic patients [3, 4, 6, 7, 8]. The PROSPERO meta-analysis showed that diabetic patients with CAN have a 3-fold increased risk of future cardiovascular events and death than those without CAN [8]. However, despite its prevalence and negative prognostic value, CAN is still underdiagnosed in patients with diabetes [3, 4, 9].
According to the Toronto Consensus Panel on Diabetic Neuropathy, CAN is defined as impairment of autonomic control of the cardiovascular system in the context of diabetic disease after exclusion of other causes [10]. CAN is usually diagnosed using several cardiovascular autonomic reflex tests (CARTs) [11]. Interestingly, a higher prevalence of CAN defined by CARTs has not only been found in subjects with T2DM, but also in those with impaired fasting glucose (IFG) and/or impaired glucose tolerance (IGT) [12]. These prediabetic conditions are both characterized by intermediate hyperglycemia and are broadly recognized to be associated with an increased risk of future T2DM and adverse cardiovascular events [13, 14].
Additionally, a reduced heart rate variability (HRV), which is an early clinical manifestation of CAN reflecting the autonomic system imbalance with a reduced parasympathetic activity and a relative sympathetic predominance on the heart, has been found in patients with prediabetes and even more in those with T2DM [15,16,17]. This finding shows that cardiac autonomic perturbations occur in subjects with altered glucose homeostasis before the onset of full-blown T2DM and progress with a worsening of glucose tolerance.
Recently, several studies have demonstrated that 1-hour plasma glucose (1hPG) levels during an oral glucose tolerance test (OGTT) ≥ 155 mg/dl (8.6 mmol/L) may identify, among subjects with normal glucose tolerance (NGT), those with glucose homeostasis abnormalities, including reduced insulin sensitivity and β cell dysfunction and an increased risk to develop T2DM [18,19,20,21], thus leading International Diabetes Federation (IDF) to recently recommend a value of 1hPG ≥ 155 mg/dl as an additional criterion to identify individuals with prediabetes who may benefit of preventive intervention [22]. Additionally, a large body of evidence has demonstrated that subjects with NGT and 1hPG ≥ 155 mg/dl (NGT 1 h-high) have a cluster of cardio-metabolic abnormalities common to T2DM, including left ventricular hypertrophy and diastolic dysfunction, impaired mechano-energetic myocardial efficiency, vascular atherosclerosis [18, 22,23,24,25,26], making it possible to speculate about an association between higher 1 h-PG and cardiac autonomic dysfunction. In line with this view, Perticone M et al. have described a decline of HRV during the first hour of OGTT in subjects with NGT 1 h-high, which was similar to that observed in those with IGT [27]. However, in this study, HRV was assessed by electrocardiographic (ECG) recordings performed during OGTT, which is not representative of basal resting conditions. Long-term, usually 24-hour HRV recordings, are considered the “gold standard” for clinical HRV assessment [28,29,30], since they are able to detect autonomic nervous responses during normal daily activities, thus providing a more accurate evaluation of cardiac autonomic function than short-term measurements [28,29,30]. To the best of our knowledge, it is still uncertain whether subjects with NGT 1 h-high have a compromised cardiac autonomic function as compared to patients with NGT and 1hPG < 155 mg/dl (NGT 1 h-low). In this study we therefore aimed to verify whether non-diabetic subjects with 1 h post-load hyperglycemia have an altered cardiac autonomic function and a reduced HRV during normal daily activities. To address this issue, we evaluated the presence of CAN defined by using CARTs and HRV assessed by 24-h electrocardiography in a cohort of non-diabetic Caucasian subjects.
Methods
Study population
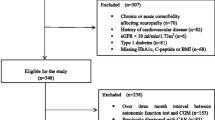
The study population consisted of 88 non-diabetic outpatients, participating to the Catanzaro Metabolic Risk Factors Study (CATAMERIS) [19, 23,24,25,26]. The main exclusion criteria were history or clinical evidence of coronary, valvular heart disease, cardiac arrhythmia, hyperlipidemia, peripheral vascular disease, diabetes, chronic gastrointestinal diseases associated with malabsorption, chronic pancreatitis, history of any malignant disease, history of autoimmune diseases, history of thyroid disorders, liver or kidney failure, treatments able to modify glucose metabolism, antihypertensive treatment with beta-blockers. Patients with pathologies or taking medications capable of causing dysfunction in the autonomic control of the cardiovascular system were excluded from the study as well as subjects with body mass index (BMI) ≥ 35 kg/m2.
All subjects underwent to a detailed medical history recording and physical examination with collection of anthropometric parameters including BMI, waist circumference, and blood pressure values. All study participants reported no significant reduction in body weight within the three months before the visit, and to perform little to no physical activity (less than 30 min of aerobic activity such as walking or running per day). After 12-h fasting, a biochemical characterization including a 75 g OGTT with 0-, 30-, 60-, 90- and 120-minutes sampling for plasma glucose and insulin was performed. Subjects were classified as having NGT when fasting plasma glucose (FPG) was < 110 mg/dL (6.1 mmol/L) and 2 h post-load glucose (2hPG) was < 140 mg/dL (7.77 mmol/L), IGT if they had FPG < 126 mg/dl and 2 h PG 140–199 mg/dl in accordance to World Health Organization (WHO) criteria [31].
Participants with NGT were further subdivided into two groups according to their 1 h PG during the OGTT. Those with a 1 h PG equal or above 155 mg/dL (8.6 mmol/L) were labeled NGT 1 h-high; those with a 1 h PG below 155 mg/dL were defined as NGT 1 h-low.
One week after OGTT, study participants underwent to cardiac autonomic function evaluation as described below.
The study was approved by the institutional ethics committee of the university “Magna Graecia” of Catanzaro (approval code: 2012.63). Written informed consent was obtained from each participant in accordance with the principles of the Declaration of Helsinki. All the investigations were performed according to principles of the Declaration of Helsinki.
Recording of heart rate variability
Cardiac autonomic function was evaluated by HRV parameters, obtained using time domain method according to previous recommendations [15, 30]. The patients were instructed to avoid exercise, smoking, alcohol and caffeinated drinks one day before the test. All subjects underwent ECG monitoring for 24 h by a three-channel (Cardioline Clickholter ® five leads monitoring). Before starting HRV monitoring via ECG we measured the heart rate (HR) after 5 min of rest. During the test, subjects were asked to perform the normal daily activities without engaging in more physical activity than they had already reported. We evaluated the following 24 h-HRV time domain parameters, which have been found associated with CAN [32,33,34]: the standard deviation of all normal heart cycles (RR intervals) (SDNN), the standard deviation of the average RR interval for each 5 min segment (SDANN), root mean square of the difference of successive R-R intervals (RMSSD), the percentage of beats with a consecutive R - R interval difference > 50 ms (pNN50), the Triangular index: Total number of RR intervals divided by the height of the histogram of all RR intervals measured on a discrete scale.
Cardiac autonomic function evaluation
To assess the prevalence of CAN in the study population we performed CARTs as suggested by Toronto Consensus Conference [10, 11, 35, 36]. As reported in Sudo et al. [36], the standard CARTs recommended for diagnosis of CAN include: Heart rate response to deep inspiration and expiration (3 inhale/exhale cycles with 6 breathing cycles per minute rate (5 s inhale and 5 s exhale phases); Heart rate response to Valsalva maneuver (exhaling against 40 mmHg for 15 s); 30:15 ratio: heart rate response upon standing up; Decrease in systolic blood pressure upon standing up; Handgrip strength test: rise in diastolic blood pressure upon sustained tension of hand muscles. Diagnosis of CAN was defined as presence of three abnormal results among the autonomic cardiovascular indices [35, 36].
Laboratory determinations
Glucose, triglycerides, and total and high-density lipoprotein (HDL) cholesterol concentrations were determined by enzymatic methods (Roche, Basel, Switzerland). Plasma insulin concentration was measured with a chemiluminescence-based assay (Immulite, Siemens Healthcare Diagnostics Inc., Marburg, Germany). Glycated haemoglobin (HbA1c) values were determined by high performance liquid chromatography with a National Glycohemoglobin Standardization Program certified automated analyzer (Adams HA-8160 HbA1C analyzer, Menarini, Italy).
Calculations
Insulin sensitivity was assessed by the Matsuda index calculated as: 10,000/square root of [fasting glucose (mmol/L) × fasting insulin (mU/L)] × [mean glucose x mean insulin during OGTT] [37].
Statistical analysis
Variables with a skewed distribution (i.e., triglycerides, fasting and post-laod insulin) were log-transformed to meet the normality assumption for statistical purposes. The results for the continuous variables are given as means ± SD. A general linear model with post hoc Fisher’s least significant difference correction was employed to test pairwise differences in anthropometric and cardio-metabolic parameters among the different glucose tolerance groups. The chi-square test was used for the comparisons of categorical variables. Relationships between HRV related parameters, CAN prevalence and clinical parameters were determined by Pearson’s correlation coefficient or Spearman’s correlation coefficient for categorical variables. A multivariable linear regression analysis was carried out to test the independent relationship between 1hPG levels and HRV parameters. Moreover, a multivariable logistic regression model was built to identify the independent contributors of CAN diagnosis. A p value < 0.05 was considered statistically significant. All statistical analyses were performed using the statistical package SPSS 22.0 for Windows (SPSS, IBM, Chicago, IL, USA).
Results
Of the 88 study participants, having a mean age and BMI of 50 ± 15 years and 27.6 ± 4.0 kg/m2, respectively, 57 had NGT and 31 had IGT. Individuals with NGT were divided into two groups based on their 1hPG: 26 subjects with 1hPG < 155 mg/dl (NGT 1 h-low) and 31 individuals with 1hPG ≥ 155 mg/dl (NGT 1 h-high). No differences in term of sex and age were detected among the three study groups, whereas subjects with NGT 1 h-high and IGT presented higher BMI than those with NGT 1 h-low (Table 1). Where available waist circumference measurements were obtained as a marker of abdominal adiposity (N = 75; 93 ± 16, 103 ± 16, 105 ± 14, respectively for NGT 1 h-low, NGT 1 h-high and IGT). Subjects with NGT 1 h-high and IGT displayed higher waist circumference (p = 0.01) consistent with an higher BMI.
After adjusting for BMI, we found that subjects with NGT 1 h-high and IGT displayed a worse metabolic profile as compared to NGT 1 h-low group, having increased levels of total cholesterol, triglycerides, HbA1c, FPG, 1hPG, 2hPG, fasting, 1 h and 2 h post-load insulin, and lower levels of HDL and insulin sensitivity estimated by Matsuda index (Table 1). No significant difference in systolic and diastolic blood pressure, and HR was observed between the study groups (Table 1).
Notably, we found that all the computed 24 h time domain parameters of HVR such as SDNN, SDANN, RMSSD, PNN50 and Triangular index were significantly decreased in subjects with NGT 1 h-high and IGT as compared to those with NGT 1 h-low (Table 2). Accordingly, the proportion of subjects with CARTs diagnosed CAN was significantly higher amongst subjects having NGT 1 h-high or IGT than those with NGT 1 h-low (Table 2).
Next, in an attempt to identify clinical variables associated with cardiac autonomic dysfunction, we performed univariate analyses. As shown in Table 3, both SDNN and SDANN were inversely related with age, HbA1c, FPG, 1hPG, 1 h and 2 h post-load insulin levels, but not with 2hPG, and positively associated with insulin sensitivity assessed by Matsuda index. RMSSD was negatively associated with BMI, diastolic blood pressure, total cholesterol, 1hPG, 1 h and 2 h post-load insulin levels and positively related with Matsuda index of insulin sensitivity. We found that PNN50 was negatively associated with total cholesterol, 1hPG, 1 h post-load insulin levels and positively with Matsuda index of insulin sensitivity, whereas Triangular index was inversely related with age, HR, triglycerides, HbA1c, 1hPG and 1 h post-load insulin but not with 2hPG. Moreover, we observed that presence of CARTs defined CAN was associated with age, HR, HbA1c, 1hPG, 1 h and 2 h post-load insulin levels and lower insulin sensitivity, but not with 2hPG (Table 3).
Furthermore, we carried out multivariate regression analyses in order to explore whether 1hPG was an independent predictor of cardiac autonomic dysfunction (Table 4). In a linear regression model including gender, age, BMI, HbA1c, FPG and 1hPG, we found that 1hPG was the strongest determinant of SDNN and SDANN. This result was retained even when waist circumference replaced BMI in the model (data not shown). Similar results were found when 2hPG levels were inserted in the model (β=−0.43, P = 0.007 for SDNN, β=−0.44, P = 0.006 for SDANN) (Table 4).
In a linear regression model including gender, age, BMI, blood pressure, lipid profile, HbA1c, fasting and 1 h PG, we found that 1hPG was an independent predictor of RMSSD. The independent relationship between RMSSD and 1hPG was retained even when BMI was replaced by waist circumference in the model, and also when 2hPG was added in the model (β=-0.33, P = 0.045) (Table 4). Additionally, 1hPG levels were an independent contributor of Triangular index in a linear regression model including age, gender, BMI, HR, lipid profile, HbA1c, fasting and 1 h PG (Table 4). Similar results were found when BMI was replaced by waist circumference in the model. When 2hPG were added in the model, 1hPG value remained to be independently associated with Triangular index (β=-0.46, P = 0.004) (Table 4). Conversely, no independent relationship was observed between 1hPG and PNN50 (Table 4).
Moreover, in a logistic regression model including age, gender, BMI, HR, HbA1c, FPG, 1hPG and 2hPG, we found that age and 1hPG values were independent contributor of CARTs defined presence of CAN (Table 5). We found a positive association between higher levels of 1hPG and increased risk of CAN even when waist circumference replaced BMI in the model (data not shown).
Discussion
Several studies have demonstrated the association between cardiac autonomic dysfunction and disorders associated with insulin resistance, including obesity, metabolic syndrome, prediabetes, and T2DM [12, 16, 32, 38,39,40]. It has been postulated that several mechanisms, which are not completely understood, contribute to cardiac autonomic dysfunction, including aging, insulin resistance, and the consequent hyperinsulinemia and hyperglycemia [3, 4, 32, 40]. Indeed, both hyperinsulinemia and hyperglycemia have been found to directly cause sympathetic excitation, through peripheral and central mechanisms [41, 42], thus leading to an autonomic imbalance toward a sympathetic predominance, which in turn may contribute to increase, on the one hand, the risk of insulin resistance and glucose tolerance, and on the other hand, the risk of ventricular arrhythmias and cardiovascular events.
It is now widely recognized that subjects with NGT 1 h-high are characterized by skeletal muscle insulin resistance, as confirmed by observations from hyperinsulinemic euglycemic clamp studies and OGTT-derived indexes of insulin sensitivity and reduced insulin clearance; all these factors lead to sustained hyperinsulinemia after an oral glucose load [18, 19, 22].
Moreover, it has been demonstrated that individuals with NGT 1 h-high show an unfavorable cardiovascular risk profile and organ damage [18, 22,23,24,25,26]. Furthermore, a recent retrospective study conducted on an elderly Chinese population has demonstrated that subjects with higher levels of 1hPG have a significant increase in CVD risk and all-cause mortality regardless of the onset of diabetes at follow-up [43].
Based on this evidence, our aim was to investigate whether subjects with NGT 1 h-high have autonomic cardiac dysfunction as well as those with IGT and to evaluate whether early post-prandial elevation of glucose levels provide an independent contribution to HRV parameters.
We have found, in line with prior studies [18, 19, 22], that subjects with NGT 1 h-high and IGT show a worse cardiometabolic profile than those with NGT 1 h-low, with increased abdominal adiposity, fasting and post-load glucose and insulin levels, an unfavorable lipid profile and a lower insulin sensitivity. Interestingly, after adjusting for BMI, we observed a significant reduction in HRV parameters in both subjects with NGT 1 h-high and IGT as compared to NGT 1 h-low group. These data are relevant, especially in terms of SDNN, which is a commonly used parameter to evaluate HRV, especially in patients with diabetic neuropathy; furthermore, SDNN is able to predict worse cardiovascular outcomes in patients with dysglycemia [44]. Accordingly, when we assessed the presence of CAN by using CARTs, we observed that subjects with NGT 1 h-high as well as those with IGT were more likely to have CAN than those with NGT 1 h-low. Moreover, by performing univariate analysis, we found that elevated 1hPG levels were associated with a decrease in all of the assessed HRV time domain measures and with diagnosis of CAN defined by CARTs. We also found that other glucose parameters such FPG and HbA1c, but not 2PG values, were associated with HVR measures (i.e. SDNN, SDANN, and triangular index) and the presence of CAN (only for HbA1c). By performing multiple regression analysis, we demonstrated that 1hPG contribute to HRV changes and to predict the presence of CAN independently of adiposity measures (BMI or waist circumference) and HbA1c, FPG and 2hPG. These results support the pathogenic role of early post-prandial elevation of glucose levels in affecting cardiac autonomic balance. This view is also supported by the evidence that acute hyperglycemia with an octreotide-induced suppression of insulin secretion may directly trigger sympathetic activity in euglycemic subjects [42]. Moreover, preclinical studies have demonstrated that exposure to high glucose levels may activate several pathways with deleterious effects on neuronal cells, including oxidative stress, mitochondrial dysfunction, polyol and AGEs pathways, which in turn may affect cardiac autonomic function [3, 4]. On the other hand, taking into account the negative association between 1 h post-load insulin levels and the HVR measures, and the positive relationship between insulin sensitivity estimated using the Matsuda index and cardiac autonomic function, we cannot exclude that the relationship between 1 h post-load hyperglycemia and cardiac autonomic dysfunction is mediated, at least in part, by elevation of post-prandial insulin levels and insulin resistance, which are mutually related and found to promote a shift of autonomic balance towards increased sympathetic regulation of the heart [13, 32, 41, 45]. In agreement with the view that both hyperglycemia and hyperinsulinemia/insulin resistance contribute to increase the adrenergic burden, Rodrigues S et al. reported a higher muscle sympathetic nerve activity in subjects with metabolic syndrome, particularly in those with elevated plasma glucose levels [45].
From a purely clinical point of view, our data show a higher prevalence of cardiac autonomic dysfunction amongst subjects with NGT 1 h-high and IGT, thus supporting the importance of early diagnosis of CAN in individuals with prediabetes who are characterized by elevated post-load glucose levels, in order to minimize the cardiovascular risk in non-diabetic patients.
However, caution is needed in interpreting results. In an attempt to obtain a well-characterized study population free of confounding factors or other causes of cardiac autonomic dysfunction (i.e., history or clinical evidence of coronary heart disease, cardiac arrhythmia, any malignant disease, autoimmune diseases, thyroid disorders, hepatic or renal insufficiency, treatments capable of modifying glucose metabolism), we enrolled a small number of subjects in our study. All participants were Caucasian which is why it is not possible to apply our findings to other racial and ethnic groups. Another limitation of our study is that participants underwent a single 75 g OGTT to assess glucose tolerance. Although this approach is common both in clinical practice and in epidemiological studies, it was not possible to evaluate the intra-individual variability of 1hPG and 2hPG, thus possibly leading to some inaccuracies in the classification of the recruited participants into groups of glucose tolerance. Subjects with NGT 1 h-high and IGT were older (although not significantly) and had higher values of BMI than NGT 1 h-low group. Even if statistical analyses were adjusted for these confounders we cannot firmly exclude their effects on the reported findings. No quantitative data regarding physical activity and body composition was recorded. However, given the sedentary life style reported by our study participants it is plausible that the low physical activity had a negligible effect on our results. Furthermore, we recruited participants in a referral university hospital; therefore, our findings cannot be extended to the general population. Finally, the cross-sectional design of the study reflects only an association of 1hPG with cardiac autonomic dysfunction and prevents us from drawing any conclusions about the causal relationship between dysglycemia and the development of CAN in non-diabetic patients. This first report on the topic should be considered hypothesis generating: prospective studies are needed to determine whether early postprandial hyperglycemia contributes to determining cardiac autonomic dysfunction. Moreover, future investigations are warranted to investigate the effects of weight loss and/or glucose lowering interventions on cardiac autonomic dysfunction.
Conclusions
In conclusion, our results demonstrate that elevated levels of 1hPG may identify, amongst NGT subjects, those with an impairment of cardiac autonomic function similar to that observed in patients with IGT. Our findings are consistent with the proposal to include the 1hPG ≥ 155 mg/dl to the current OGTT based criteria for the diagnosis of prediabetes [22], in order to identify a subgroup of subjects with normal levels of FPG and 2hPG who display an unfavorable cardiometabolic profile, with an increased risk of cardiovascular organ damage, including CAN. Due to the considerable socioeconomic burden associated with the development of cardiovascular clinical manifestations of decompensated T2DM, the implementation of a more sensitive strategy for early identification of high-risk subjects could be important to reduce the increasing prevalence of complications of dysglycemia and bring benefits to global health.
Data availability
Clinical data of study participants are available upon reasonable request to the Corresponding Author.
Abbreviations
- BMI:
-
Body mass index
- CAN:
-
Cardiac autonomic neuropathy
- CATAMERIS:
-
Catanzaro Metabolic Risk Factors Study
- CARTs:
-
Cardiovascular autonomic reflex tests
- ECG:
-
Clectrocardiography
- FPG:
-
Fasting plasma glucose
- IDF:
-
International Diabetes Federation
- IFG:
-
Impaired fasting glucose
- IGT:
-
Impaired glucose tolerance
- HbA1c:
-
Glycated haemoglobin
- HDL:
-
High-density lipoprotein
- HRV:
-
Heart rate variability
- NGT:
-
Normal glucose tolerance
- OGTT:
-
Oral glucose tolerance test
- PNN50:
-
Percentage of beats with a consecutive RR interval difference > 50 ms
- 1hPG:
-
1 h post-load glucose
- 2hPG:
-
2 h post-load glucose
- RMSSD:
-
Root mean square of the difference of successive R-R intervals
- SDNN:
-
Standard deviation of all normal heart cycle
- SDANN:
-
Standard deviation of the average RR interval for each 5 min segment
- T2DM:
-
Type 2 diabetes mellitus
- WHO:
-
World Health Organization
References
Avogaro A, Fadini GP. Microvascular complications in diabetes: a growing concern for cardiologists. Int J Cardiol. 2019;291:29–35.
Zoppini G, Cacciatori V, Raimondo D, Gemma M, Trombetta M, Dauriz M, et al. Prevalence of cardiovascular autonomic neuropathy in a cohort of patients with newly diagnosed type 2 diabetes: the Verona newly diagnosed type 2 diabetes study (VNDS). Diabetes Care. 2015;38(8):1487–93.
Williams S, Raheim SA, Khan MI, Rubab U, Kanagala P, Zhao SS, Marshall A, Brown E, Alam U. Cardiac autonomic neuropathy in type 1 and 2 diabetes: Epidemiology, Pathophysiology, and management. Clin Ther. 2022;44(10):1394–416.
Fisher VL, Tahrani AA. Cardiac autonomic neuropathy in patients with diabetes mellitus: current perspectives. Diabetes Metab Syndr Obes. 2017;10:419–34.
Zimmet PZ. Diabetes and its drivers: the largest epidemic in human history? Clin Diabetes Endocrinol. 2017;3:1.
Valensi P, Sachs RN, Harfouche B, Lormeau B, Paries J, Cosson E, Paycha F, Leutenegger M, Attali JR. Predictive value of cardiac autonomic neuropathy in diabetic patients with or without silent myocardial ischemia. Diabetes Care. 2001;24(2):339–43.
Ko SH, Song KH, Park SA, Kim SR, Cha BY, Son HY, Moon KW, Yoo KD, Park YM, Cho JH, Yoon KH, Ahn YB. Cardiovascular autonomic dysfunction predicts acute ischaemic stroke in patients with type 2 diabetes mellitus: a 7-year follow-up study. Diabet Med. 2008;25(10):1171–7.
Chowdhury M, Nevitt S, Eleftheriadou A, Kanagala P, Esa H, Cuthbertson DJ, Tahrani A, Alam U. Cardiac autonomic neuropathy and risk of cardiovascular disease and mortality in type 1 and type 2 diabetes: a meta-analysis. BMJ Open Diabetes Res Care. 2021;9(2):e002480.
Vinik AI, Ziegler D. Diabetic cardiovascular autonomic neuropathy. Circulation. 2007;115(3):387–97.
Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, Lauria G, Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P, Toronto Diabetic Neuropathy Expert Group. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010;33(10):2285–93.
Assessment. Clinical autonomic testing report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Neurology. 1996;46(3):873–80.
Eleftheriadou A, Williams S, Nevitt S, Brown E, Roylance R, Wilding JPH, Cuthbertson DJ, Alam U. The prevalence of cardiac autonomic neuropathy in prediabetes: a systematic review. Diabetologia. 2021;64(2):288–303.
Levitan EB, Song Y, Ford ES, Liu S. Is nondiabetic hyperglycemia a risk factor for Cardiovascular Disease? A Meta-analysis of prospective studies. Arch Intern Med. 2004;164(19):2147–55.
Huang Y, Cai X, Mai W, Li M, Hu Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. BMJ. 2016;355:i5953.
Heart rate variability.: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation. 1996;93(5):1043–65.
Coopmans C, Zhou TL, Henry RMA, Heijman J, Schaper NC, Koster A, Schram MT, van der Kallen CJH, Wesselius A, den Engelsman RJA, Crijns HJGM, Stehouwer CDA. Both prediabetes and type 2 diabetes are Associated with Lower Heart Rate Variability: the Maastricht Study. Diabetes Care. 2020;43(5):1126–33.
Hadad R, Akobe SF, Weber P, Madsen CV, Larsen BS, Madsbad S, Nielsen OW, Dominguez MH, Haugaard SB, Sajadieh A. Parasympathetic tonus in type 2 diabetes and pre-diabetes and its clinical implications. Sci Rep. 2022;12(1):18020.
Fiorentino TV, Marini MA, Succurro E, Andreozzi F, Perticone M, Hribal ML, Sciacqua A, Perticone F, Sesti G. One-hour postload hyperglycemia: implications for Prediction and Prevention of type 2 diabetes. J Clin Endocrinol Metab. 2018;103(9):3131–43.
Fiorentino TV, Marini MA, Andreozzi F, Arturi F, Succurro E, Perticone M, Sciacqua A, Hribal ML, Perticone F, Sesti G. One-hour postload hyperglycemia is a stronger predictor of type 2 diabetes than impaired fasting glucose. J Clin Endocrinol Metab. 2015;100:3744–51.
Abdul-Ghani MA, Abdul-Ghani T, Ali N, Defronzo RA. One-hour plasma glucose concentration and the metabolic syndrome identify subjects at high risk for future type 2 diabetes. Diabetes Care. 2008;31(8):1650–5.
Bergman M, Chetrit A, Roth J, Jagannathan R, Sevick M, Dankner R. One-hour post-load plasma glucose level during the OGTT predicts dysglycemia: observations from the 24year follow-up of the Israel Study of Glucose Intolerance, obesity and hypertension. Diabetes Res Clin Pract. 2016;120:221–8.
Bergman M, Manco M, Satman I, Chan J, Schmidt MI, Sesti G, Vanessa Fiorentino T, Abdul-Ghani M, Jagannathan R, Kumar Thyparambil Aravindakshan P, Gabriel R, Mohan V, Buysschaert M, Bennakhi A, Pascal Kengne A, Dorcely B, Nilsson PM, Tuomi T, Battelino T, Hussain A, Ceriello A, Tuomilehto J. International diabetes federation position statement on the 1-hour post-load plasma glucose for the diagnosis of intermediate hyperglycaemia and type 2 diabetes. Diabetes Res Clin Pract. 2024;209:111589.
Sciacqua A, Miceli S, Carullo G, Greco L, Succurro E, Arturi F, Sesti G, Perticone F. One-hour postload plasma glucose levels and left ventricular mass in hypertensive patients. Diabetes Care. 2011;34:1406–11.
Sciacqua A, Miceli S, Greco L, Arturi F, Naccarato P, Mazzaferro D, Tassone EJ, Turano L, Martino F, Sesti G, Perticone F. One-hour postload plasma glucose levels and diastolic function in hypertensive patients. Diabetes Care. 2011;34:2291–6.
Succurro E, Marini MA, Arturi F, Grembiale A, Lugarà M, Andreozzi F, Sciacqua A, Lauro R, Hribal ML, Perticone F, Sesti G. Elevated one-hour post-load plasma glucose levels identifies subjects with normal glucose tolerance but early carotid atherosclerosis. Atherosclerosis. 2009;207:245–9.
Fiorentino TV, Miceli S, Succurro E, Sciacqua A, Andreozzi F, Sesti G. Depressed myocardial mechano-energetic efficiency in subjects with dysglycemia. Diabetes Res Clin Pract. 2021;177:108883.
Perticone M, Tassone EJ, Scarpino PE, Naccarato P, Addesi D, di Cello S, et al. Sympathovagal balance and 1-h postload plasma glucose in normoglucose tolerant hypertensive patients. Acta Diabetol. 2016;53(1):41–7.
Julario R, Mulia EPB, Rachmi DA, A’yun MQ, Septianda I, Dewi IP, Juwita RR, Dharmadjati BB. Evaluation of heart rate variability using 24-hour Holter electrocardiography in hypertensive patients. J Arrhythm. 2020;37(1):157–64.
Shaffer F, McCraty R, Zerr CL. A healthy heart is not a metronome: an integrative review of the heart’s anatomy and heart rate variability. Front Psychol. 2014;5:1040.
Kleiger RE, Stein PK, Bigger JT. Heart rate variability: measurement and clinical utility. Ann Noninvasive Electrocardiol. 2005;10(1):88–101.
World Health Organization. Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia: report of a WHO/IDF consultation. Geneva: World Health Organization; 2006.
Svensson MK, Lindmark S, Wiklund U, Rask P, Karlsson M, Myrin J, Kullberg J, Johansson L, Eriksson JW. Alterations in heart rate variability during everyday life are linked to insulin resistance. A role of dominating sympathetic over parasympathetic nerve activity? Cardiovasc Diabetol. 2016;15:91.
May O, Arildsen H. Long-term predictive power of heart rate variability on all-cause mortality in the diabetic population. Acta Diabetol. 2011;48(1):55–9.
Shaffer F, Ginsberg JP. An overview of Heart Rate Variability Metrics and norms. Front Public Health. 2017;5:258.
Spallone V, Ziegler D, Freeman R, Bernardi L, Frontoni S, Pop-Busui R, Stevens M, Kempler P, Hilsted J, Tesfaye S, Low P, Valensi P. Toronto consensus panel on diabetic neuropathy. Cardiovascular autonomic neuropathy in diabetes: clinical impact, assessment, diagnosis, and management. Diabetes Metab Res Rev. 2011;27(7):639–53.
Sudo SZ, Montagnoli TL, Rocha B, de Santos S, de Sá AD, Zapata-Sudo MPL. Diabetes-Induced Cardiac Autonomic Neuropathy: impact on heart function and prognosis. Biomedicines. 2022;10(12):3258.
Matsuda M, De Fronzo RA. Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care. 1999;22:1462–70.
Ziegler D, Voss A, Rathmann W, Strom A, Perz S, Roden M, Peters A, Meisinger C, KORA Study Group. Increased prevalence of cardiac autonomic dysfunction at different degrees of glucose intolerance in the general population: the KORA S4 survey. Diabetologia. 2015;58(5):1118–28.
Stein PK, Barzilay JI, Domitrovich PP, Chaves PM, Gottdiener JS, Heckbert SR, Kronmal RA. The relationship of heart rate and heart rate variability to non-diabetic fasting glucose levels and the metabolic syndrome: the Cardiovascular Health Study. Diabet Med. 2007;24(8):855–63.
Dimova R, Tankova T, Guergueltcheva V, Tournev I, Chakarova N, Grozeva G, Dakovska L. Risk factors for autonomic and somatic nerve dysfunction in different stages of glucose tolerance. J Diabetes Complications. 2017;31(3):537–43.
Anderson EA, Hoffman RP, Balon TW, Sinkey CA, Mark AL. Hyperinsulinemia produces both sympathetic neural activation and vasodilation in normal humans. J Clin Invest. 1991;87(6):2246–52.
Hoffman RP, Hausberg M, Sinkey CA, Anderson EA. Hyperglycemia without hyperinsulinemia produces both sympathetic neural activation and vasodilation in normal humans. J Diabetes Complications. 1999;13(1):17–22.
Rong L, Cheng X, Yang Z, Gong Y, Li C, Yan S, Sun B. One-hour plasma glucose as a long-term predictor of cardiovascular events and all-cause mortality in a Chinese older male population without diabetes: a 20-year retrospective and prospective study. Front Cardiovasc Med. 2022;9:947292.
Cha SA, Park YM, Yun JS, Lee SH, Ahn YB, Kim SR, Ko SH. Time- and frequency-domain measures of heart rate variability predict cardiovascular outcome in patients with type 2 diabetes. Diabetes Res Clin Pract. 2018;143:159–69.
Rodrigues S, Cepeda FX, Toschi-Dias E, Dutra-Marques ACB, Carvalho JC, Costa-Hong V, Alves MJNN, Rondon MUPB, Bortolotto LA, Trombetta IC. The role of increased glucose on neurovascular dysfunction in patients with the metabolic syndrome. J Clin Hypertens (Greenwich). 2017;19:840–7.
Funding
This work was supported, in part, by PNRR PRIN P2022E5WSF to F.A., PNRR − 2022-12376731 to F.A., and PRIN 2022F2NMAL to F.A.
Author information
Authors and Affiliations
Contributions
GM collected and analyzed the data, RJ, LS, MR, MM collected the data and edited the manuscript, MP reviewed the manuscript and contributed to the discussion, GCM contribute to write and review the manuscript, AS, ES contributed to the discussion, and reviewed the manuscript, TVF analyzed the data, write and edited the manuscript, FA conceived the study, and reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All study subjects gave their written informed consent to be enrolled in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Monea, G., Jiritano, R., Salerno, L. et al. Compromised cardiac autonomic function in non-diabetic subjects with 1 h post-load hyperglycemia: a cross-sectional study. Cardiovasc Diabetol 23, 295 (2024). https://doi.org/10.1186/s12933-024-02394-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02394-w