
Abstract
Background and aims
Atherosclerosis is the main cause of stroke and coronary heart disease (CHD), both leading mortality causes worldwide. Proteomics, as a high-throughput method, could provide helpful insights into the pathological mechanisms underlying atherosclerosis. In this study, we characterized the associations of plasma protein levels with CHD and with carotid intima-media thickness (CIMT), as a surrogate measure of atherosclerosis.
Methods
The discovery phase included 1000 participants from the KORA F4 study, whose plasma protein levels were quantified using the aptamer-based SOMAscan proteomics platform. We evaluated the associations of plasma protein levels with CHD using logistic regression, and with CIMT using linear regression. For both outcomes we applied two models: an age-sex adjusted model, and a model additionally adjusted for body mass index, smoking status, physical activity, diabetes status, hypertension status, low density lipoprotein, high density lipoprotein, and triglyceride levels (fully-adjusted model). The replication phase included a matched case-control sample from the independent KORA F3 study, using ELISA-based measurements of galectin-4. Pathway analysis was performed with nominally associated proteins (p-value < 0.05) from the fully-adjusted model.
Results
In the KORA F4 sample, after Bonferroni correction, we found CHD to be associated with five proteins using the age-sex adjusted model: galectin-4 (LGALS4), renin (REN), cathepsin H (CTSH), and coagulation factors X and Xa (F10). The fully-adjusted model yielded only the positive association of galectin-4 (OR = 1.58, 95% CI = 1.30–1.93), which was successfully replicated in the KORA F3 sample (OR = 1.40, 95% CI = 1.09–1.88). For CIMT, we found four proteins to be associated using the age-sex adjusted model namely: cytoplasmic protein NCK1 (NCK1), insulin-like growth factor-binding protein 2 (IGFBP2), growth hormone receptor (GHR), and GDNF family receptor alpha-1 (GFRA1). After assessing the fully-adjusted model, only NCK1 remained significant (β = 0.017, p-value = 1.39e-06). Upstream regulators of galectin-4 and NCK1 identified from pathway analysis were predicted to be involved in inflammation pathways.
Conclusions
Our proteome-wide association study identified galectin-4 to be associated with CHD and NCK1 to be associated with CIMT. Inflammatory pathways underlying the identified associations highlight the importance of inflammation in the development and progression of CHD.
Similar content being viewed by others


Introduction
Atherosclerosis, which is a cornerstone pathophysiological process of multiple disease forms including coronary heart disease (CHD) and stroke, is the leading cause of mortality worldwide [1]. Epidemiological studies of CHD and stroke have successfully identified major metabolic risk factors such as obesity, diabetes, dyslipidemia, and hypertension, which in turn helped to develop preventive strategies and to identify new drug targets [2].
Atherosclerosis is characterized by thickening of both the media and intima of the arterial wall, followed by plaque formation. Where this process impedes the proper delivery of oxygen-rich blood to the heart, it results in the development of CHD [3]. Specific mechanisms of atherosclerosis involve endothelial dysfunction, lipid accumulation, inflammation, oxidative stress, angiogenesis, matrix degradation, and thrombosis [3]. A marker of early atherosclerosis is carotid intima media thickness (CIMT), an ultrasound-based measurement of arterial wall thickness [4]. CIMT is clinically used to predict risk of atherosclerotic diseases like CHD and stroke [4,5,6,7,8,9]. An increase in CIMT of 0.1 mm has been found to be associated with 15% higher risk for myocardial infarction and 18% higher risk for stroke [10].
Identifying proteins linked to specific atherogenic-mechanisms sheds light onto the molecular pathophysiology of cardiometabolic disturbances. Although there have been multiple studies that found highly expressed proteins within atherosclerotic tissue, only a small number of these findings was replicated when using blood samples [11,12,13].
Proteomics can provide valuable clues to the underlying pathological mechanisms at the molecular level. The plasma proteome has been extensively characterized in cardiovascular disease, because of its availability and proximity to the cardiovascular system. Several studies applying mass spectrometry to quantify plasma proteins in small sample numbers have identified proteins associated with CHD [14,15,16,17,18,19,20]. A study using an aptamer-based platform, capable of profiling more than thousand analytes in plasma, detected many protein changes in the context of myocardial injury in a cohort of the Framingham Heart Studies, thus underscoring the potential of proteomics tools when applied to large human cohorts [21].
In the present study we aim to expand our knowledge of CHD pathophysiology, using quantitative data for 1129 proteins in plasma samples from 1000 individuals of the population-based KORA F4 study from a high-throughput aptamer-based analysis [23]. We explore the association of plasma protein levels with both CHD and CIMT, and additionally validate our findings in an independent sample from the KORA F3 cohort. We further explore possible roles of the associated proteins in the pathogenesis of atherosclerosis and CHD using pathway analysis.
Materials and methods
Study design of the discovery cohort
The KORA (Cooperative health research in the Region of Augsburg) study is an independent population-based cohort study in southern Germany [22]. The study was approved by the ethics committee of the Bavarian Medical Association and was carried out in accordance with the principles of the Declaration of Helsinki. All study participants signed written informed consent prior to their participation in the study.
We used data from the KORA F4 study (n = 3080), which is the follow-up of the KORA S4 survey that was conducted between 2006 and 2008. A subsample of 1000 individuals was randomly selected from the deeply phenotyped KORA F4 participants for plasma protein measurement using the SOMAscan aptamer-based proteomics platform [23]. We included all participants with data for the diagnosis of CHD according to Fig. 1. Exclusion criteria comprised (1) participants with missing data on the outcome or (2) participants with missing data on the model co-variates (BMI, hypertension status, diabetes status, levels of LDL, HDL, and triglycerides, smoking status, and physical activity).
CHD status validation
Stratification of subjects for CHD association was performed according to Fig. 1. We first validated self-reported CHD using self-reported history of myocardial infarction (MI) and characteristic electrocardiogram (ECG) MI changes. The PC-based BioSys system (Hörmann Medizintechnik, Zwönitz, Germany) was used to record ECGs, which were manually assessed by two cardiologists. Infarction-characteristic changes in the ECG were identified by consensus. We used the validated CHD status as a binary variable in subsequent statistical analysis. According to the CHD-status validation, and the inclusion and exclusion criteria, 76 CHD-cases and 906 controls were carried forward to subsequent analysis.

Flow diagram of subjects' stratification for CHD association. Coronary heart disease (CHD) was validated using self-reported history of myocardial infraction (MI) and characteristic electrocardiogram MI changes
CIMT measurement
Ultrasound measurements of the extracranial carotid arteries have been performed in KORA participants as previously described [24, 25]. Briefly, all measurements were conducted by two sonographers according to a standardized protocol [26]. Optimal images of both common carotid arteries (CCA) were identified and stored. Then, CIMT was ascertained over a length of 10 mm beginning at 0–5 mm of the dilatation of the distal CCA using an automated edge detection reading system (Prowin software, Medical Technologies International, USA). The final CIMT value was calculated as the average of the measurements of three frozen images from both the left and right CCA. Measurements of inter-sonographer (n = 30 CIMT measurements) and inter-reader variations (n = 50 CIMT measurements) showed coefficients of variations of 1.9% and 3.0% and Spearman correlation coefficients of ≥ 0.89 (Supplementary information: Supplementary Fig. 1) [25].
Assessment of model covariates
BMI was calculated by dividing each participant’s weight in kilograms by the square of the participant´s height. Participants were categorized as hypertensive if they had a blood pressure measurement (≥ 140/90 mmHg) or if they were receiving medical treatment for hypertension. Diabetes was defined by self-report or current use of glucose-lowering agents. Diabetes status was validated by asking the participant’s responsible physician. Lipid levels included low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglycerides. Self-reported smoking status was categorized as non-, former, or current smoker. Leisure time physical activity was assessed with two separate questions concerning leisure time sport activity in winter and in summer (cycling included). Possible answers were: (1) > 2 h, (2) 1–2 h, (3) < 1 h, and (4) none per week. Participants who had a total score < 5, obtained by summing the numbers (1)– (4) from the winter and summer questions, were classified as physically active.
Proteomics measurements
Plasma samples were sent to SomaLogic Inc. (Boulder Colorado, USA) for proteomics measurement by means of the SOMAscan platform [23, 27]. Samples and bead coupled SOMAmers were mixed in solution. Free proteins were washed out and SOMAmer-protein complexes were photocleaved off the beads. Dextran sulfate was added to the solution as an anionic competitor, allowing non-cognate complexes to dissociate. SOMAmer-protein complexes were captured onto new avidin-coated beads by protein biotin tags. Free SOMAmers were washed out. Afterwards, SOMAmers were released from complexes in a denaturing buffer. Thus, individual protein concentrations were transformed into a corresponding SOMAmer concentration. SOMAmers were hybridized to complementary sequences on a microarray and quantified by fluorescence. The resulting raw intensities were processed using SOMALogic’s data analysis workflow, which utilizes the standard samples included on each plate and entails hybridization normalization, median signal normalization, and signal calibration to control for interplate differences. Protein intensities were reported in relative fluorescence units. One sample failed SOMAscan quality control, leaving a total of 999 samples from 483 males and 516 females. Additionally, we removed 29 aptamers that failed SOMAscan quality control, and 5 additional aptamers as recommended by the SOMAscan assay change log issued on December 22, 2016, leaving 1095 aptamers for further analysis. QC samples had a median intra-assay coefficient of variation (CV) of < 3% and a median inter-assay CV of < 7%. Proteomics data skipping median normalization were used to perform sensitivity analyses to investigate whether the quality control has an influence on the results.
Study design of the replication cohort
For replication analysis, a matched CHD case-control sample was drawn from the KORA F3 cohort, which is a follow-up study from the previous KORA S3 survey, with enrolled German nationals between 25- and 74-years old living in the region of Augsburg, South Germany. The KORA F3 cohort consists of 3988 participants, whose data were collected between 2004 and 2005. 165 CHD-cases were drawn from the study as well as 165 (5-year interval) matched controls. Inclusion criteria for study participants comprised (1) biosample availability and (2) participants with data for the diagnosis of CHD according to the following criteria: self-reported CHD diagnosis, cardiac catheterization, bypass-operation, or myocardial infraction. Exclusion criteria comprised (1) participants with unkown status of CHD and (2) participants with missing data of the model co-variates (BMI, levels of LDL, HDL, triglycerides, diabetes status, hypertension status, smoking status, and physical activity).
To validate the results of our discovery phase, the replication was performed using ELISA-based measures of the significant proteins obtained with the fully-adjusted model. However, only galectin-4 was assessed to be associated with CHD. Due to the lack of CIMT measures in KORA F3, NCK1 was not tested.
Enzyme-linked immunosorbent assay (ELISA) for galectin-4
An ELISA pre-coated with antibodies against galectin-4 was purchased from MyBiosource (San Diego, CA, U.S.A, MBS9715486) and analyzed according to the manufacturer’s protocol. A standard curve was prepared using recombinant galectin-4 in concentrations ranging from 96 to 3 pg/ml with a measurement error below 12%. Plasma samples were diluted in a 1:5 ratio using the dilution buffer provided by the kit. Absorption at 450 nm was measured with the Fluorostar Omega microplate reader (BMG LabTech, Ortenberg, Germany).
Pre-processing of protein data
All protein values including either SOMAscan- or ELISA-based measures, were log2 transformed and standardized to have a mean of 0 and a standard deviation of 1, to be used for further statistical analysis.
Statistical analysis
Estimated associations between CHD and each plasma protein were calculated by applying iterative multiple logistic regression analysis (dichotomous outcome), while associations between CIMT and each plasma protein were calculated using a linear regression model (continuous outcome). Both CHD and CIMT associations were tested according to the following models: model 1 adjusted by age and sex only; model 2 adjusted for age, sex, body mass index (BMI), smoking status, physical activity, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglyceride levels, diabetes status, and hypertension status.
Subjects with missing values were excluded from the respective analysis. To account for protein multiple testing, we applied Bonferroni correction resulting in a significant threshold of 4.57E-05 (0.05/1095 proteins) for both CHD and CIMT outcomes. To assess the performance of our replicated results as biomarkers, we calculated the area under the receiver operating characteristic curve (ROC-AUC) using the “pROC” R-package version 1.16.2.
Systems biology analysis
Systems biology analysis of CHD- and CIMT-nominally associated proteins (p < 0.05) identified with the fully-adjusted model was performed using the Ingenuity Pathways Knowledge (Qiagen, Redwook City, CA), a database of biological interactions and processes spanning from molecular (proteins, genes) to organism (diseases) levels. Ingenuity Pathway Analysis (IPA) uses enrichment analysis-approaches to calculate the significance of observing a candidate protein/gene set within the context of biological systems. IPA calculates the p-value for enrichment or overlap between the test set and the IPA knowledge base using Fisher´s Exact test. Significant activation was considered at z-score > 2 and significant inhibition at z-score < − 2. Pathway analyzes included causal networks and identification of upstream regulators.
Results
Baseline characteristics of the study population are described in Table 1. Stratification of participants in our discovery cohort KORA F4 for CHD association is displayed in Fig. 1. There were 982 individuals included in the fully-adjusted model of which 76 had CHD. Non-CHD participants were younger with a mean age of 58.7 years and comprised more women (53.2%), compared to participants with CHD who had a mean age of 64.8 years and comprised less women (31.6%). Participants with CHD had a higher mean of CIMT (0.91) as compared to those without (0.87, p-value: 0.017). As expected, participants with CHD showed higher consumption rates of statins, platelet aggregation inhibitors, aspirin, antihypertensive medication, beta-blockers, and cardiac glycosides. However, anti-diabetic medication showed no significant differences.
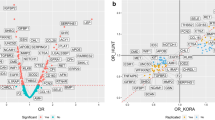
In total, five proteins were found to be significantly associated with CHD in the sex-age adjusted model (Table 2; Fig. 2, Supplementary Table 1). Two of these proteins showed a protective effect namely, coagulation factor X (OR = 0.66, 95% CI = 0.55–0.80) and its activated form coagulation factor Xa (OR = 0.65, 95% CI = 0.53–0.79) and three showed negative effects namely, cathepsin H (OR = 1.64, 95% CI = 1.3–2.09), galectin-4 (OR = 1.70, 95% CI = 1.41–2.08) and renin (OR = 1.73, 95% CI = 1.38–2.17). Only galectin-4 remained significantly associated with CHD in the fully-adjusted model (OR = 1.58, 95% CI = 1.30–1.93) (Table 2; Fig. 2, Supplementary Table 2)

Volcano plot showing the association between plasma proteins and CHD. (A) Age-sex adjusted model. (B) Fully-adjusted model: age, sex, body mass index (BMI), physical activity, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglyceride levels, diabetes status, hypertension status and smoking status included as covariates. Each dot on the figure represents the odds ratio of a single protein with Bonferroni significant proteins labelled. OR: odds ratio
For CIMT, four proteins in total were found to be significantly associated in the age-sex adjusted model after Bonferroni adjustment, these were GDNF family receptor alpha-1 (GFRA1) (β = 0.017, p-value = 1.91E-06), cytoplasmic protein NCK1 (NCK1) (β = 0.017, p-value = 3.59E-06), insulin-like growth factor-binding protein 2 (IGFBP2) (β = − 0.015, p-value = 4.47E-05), and growth hormone receptor (GHR) (β = 0.016, p-value = 2.46E-05) (Table 3; Fig. 3, Supplementary Table 3). In the fully-adjusted model, only NCK1 (β = 0.017, p-value = 1.39E-06) remained significantly associated with CIMT after Bonferroni adjustment (Table 3; Fig. 3, Supplementary Table 4).

Volcano plot showing the association between plasma proteins and CIMT. (A) Age-sex adjusted model. (B) Fully-adjusted model: age, sex, body mass index (BMI), physical activity, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglyceride levels, diabetes status, hypertension status and smoking status included as covariates. Each dot on the figure represents the β-coefficients of a single protein with Bonferroni significant proteins labelled
To investigate possible effects of the quality control of the proteomics data on the results [28], we performed a sensitivity analysis based on proteomics data skipping median normalization. No effect on our main CHD or CIMT findings was detected (Supplementary results: Sensitivity analyses; Supplementary Tables 6–7).
To validate our results, we tested our fully-adjusted model findings in an independent cohort of KORA F3 using ELISA-measured levels of galectin-4. Characteristics of participants are shown in Supplementary Table 5. The association between galectin-4 and CHD was successfully replicated in the fully-adjusted case-control study (OR = 1.40, 95% CI = 1.09–1.88, p-value = 1.37E-02; Supplementary Table 5).
To test galectin-4 as a biomarker, we run ROC-AUC tests in both KORA F3 and F4. A potential role of galectin-4 as a biomarker can be inferred from our results (Supplementary results: Assessment of Galectin-4 as a biomarker of CHD; Supplementary Figs. 2–3).
Finally, to gain insights into enriched signaling pathways and biological mechanisms, Ingenuity Pathway Analysis was performed using nominally associated proteins (p-value < 0.05) identified with the fully-adjusted model including 106 CHD-associated proteins or 66 CIMT-associated proteins. For CHD, the unique significant causal network (z-score = − 2.11) including galectin-4 and 43 CHD-associated proteins, predicted the activation of peroxisome proliferator activated receptor alpha (PPARA), which might directly increase the expression of galectin-4. This finding was also predicted by the causal network with the lowest p-value (FDR = 5.37E-02), which included 68 CHD-associated proteins. Figure 4A shows the summary of PPARA-predicted activation via the two networks. For CIMT, the unique significant causal network (z-score = − 2.0) including NCK1 and four CIMT-associated proteins, identified interleukin-9 as an inhibited upstream regulator (Fig. 4B). Due to the prediction of inflammation pathways as upstream regulators of galectin-4 and NCK1, we further run the two models adjusting for high sensitivity C-reactive protein (CRP) in KORA F4 as a sensitivity analysis (Supplementary results: Sensitivity analyses; Supplementary Tables 8–9). No effect was observed on our main CHD or CIMT findings.

Predicted upstream regulators of galectin-4 or NCK1 and associated proteins. Results obtained when analyzing nominally significant (p < 0.05) CHD-associated proteins using the fully-adjusted model. (A) PPARA was predicted to directly increase expression of galectin-4 (LGALS4): selected pathways of the two significant causal networks predicting the activation of peroxisome proliferator activated receptor alpha (PPARA). Activation of P38 mitogen-activated protein kinase (P38MAPK) leads to activation and phosphorylation of PPARA. Interleukin-1 beta (IL1B) usually decreases the activity of PPARA; however, IL1B is predicted to be inhibited. (B) Unique significant inhibited causal network including NCK1: predicted inhibition of interleukin-9 (IL9) could indirectly increase expression of NCK1, SPTAN1 and CFL1, and indirectly decrease expression of CMA1. Full line: direct interaction; segmented line: indirect interaction. Black arrows: associated proteins identified by the fully-adjusted model in the discovery phase
Discussion
The main aim of the present study was to identify protein associations with CHD and CIMT, to provide understanding of the pathophysiology of CHD and atherosclerosis risk. In the age-sex adjusted model, proteomic analysis showed differential abundance of five proteins with CHD and four with CIMT. Following further adjustment of the model for BMI, smoking status, lipid measurements, hypertension, and diabetes status, the quantitative difference of galectin-4 for CHD and NCK1 for CIMT remained significant. Moreover, the association of galectin-4 with CHD was further validated using ELISA-based measurements in an independent study.
Galectin-4 is a member of the beta-galactoside-binding proteins, and has important functions in lipid raft stabilization, protein apical trafficking, cell adhesion, as well as wound healing [29]. Galectin-4 may be involved in atherosclerosis by enhancing lipid raft stabilization, which may subsequently affect redox signaling pathways [30]. Schroder et al. reported galectin-4 to be correlated with myocardial blood flow reserve, a gold standard diagnostic to clinically assess coronary microvascular dysfunction, in women with angina pectoris and non-obstructive CHD [31]. The authors conjectured that galectin-4’s promotion of cell adhesion contributed to the association [31]. A Swedish population-based study found galectin-4 to be significantly associated with incident coronary events (hazard ratio (HR) = 1.34, 95% confidence interval (CI) = 1.14–1.57) and incident heart failure (HR = 1.26, 95% CI 1.03–1.54) [32]. Another study compared heart failure patients to controls both recruited in the outpatient clinic at Karolinska University Hospital, finding galectin-4 to be significantly associated with heart failure (HR = 2.6; FDR adjusted p-value 0.005) [33]. In addition, galectin-4 has been reported to be associated with hospitalization linked to obesity [34] and ST-segment elevation myocardial infarction [35]. All listed reports are in line with our finding of galectin-4’s association with CHD. The pathway analysis of CHD-associated proteins suggests that the interplay of galectin-4 and the predicted activated status of both p38 MAPk signaling and interleukin-1B, representatives of inflammation pathways [36], takes place via the peroxisome proliferator activated receptor alpha (PPARA). PPARG-deficient macrophages have been found to display an elevated production of pro-inflammatory cytokines including interleukin-1B [37].
Among the five CHD-associated proteins using the age-sex adjusted model, two were found to be associated with a higher- and two with a lower-CHD risk. Our reported association of renin with higher CHD-risk might have been lost when using the fully-adjusted model due to the adjustment for hypertension [38]. However, renin has been reported to be positively associated with CHD [39, 40]. Renin is a member of the renin-angiotensin-aldosterone system, which, via its active peptide angiotensin II, contributes to atherosclerosis development, not only by promoting hypertension but also through multiple direct actions on vessels [41].
Cathepsin H was an additional protein associated with a higher CHD-risk in the age-sex adjusted model. Cathepsin H is a lysosomal cysteine protease important in the overall degradation of lysosomal proteins [42]. Its atherogenic role could lead the transformation of LDL to an atherogenic moiety, which in turn induces macrophage foam cell formation [43].
Proteins associated with lower-CHD risk associations included coagulation factor X as well as its active form coagulation factor Xa. A pathogenetic mechanism of CHD includes thrombotic vessel occlusion followed by rupture of an atherosclerotic plaque [3]. It is therefore not surprising that constituents and a regulating protein of the coagulation cascade were found significantly associated with CHD in the present study. Factor Xa exerts also non-hemostatic effects by activation of protease-activated receptors-1 (PAR-1) and PAR-2, which have been associated with atherosclerosis, inflammation, and fibrosis [44]. Such counterintuitive associations were reported before: where the concentrations of coagulation factor X and prothrombin were lower in blood from patients with CHD having more than 50% stenosis compared with those without CHD [45]. Brummel-Ziedins et al. hypothesized that despite the depletion of coagulation factors, the balance between tissue factor and tissue factor pathway inhibitor is the primary driver of a hypercoagulable state in patients with CHD [45].
We also identified proteins to be associated with CIMT. NCK1 was the unique significant protein positively associated with CIMT in the fully-adjusted model. NCK1 is reported to be involved in different pathways leading to the progression of atherosclerosis [46]. For instance, it is associated with vascular permeability, which allows the uptake of low-density lipoproteins (LDL) and thereby stimulates inflammation [46, 47]. The resulting oxidative stress increase in endothelial cells decreases nitric oxide and thereby supports endothelial cell dysfunction [48]. Alfaidi et al. showed in an in-vivo study that NCK1-knockdown reduced NF-κB signaling and thereby inflammation in endothelial cells [46]. Additionally, pathway analysis revealed interleukin-9 to indirectly inhibit expression of NCK1, SPTAN1, and CFL1, while the opposite effect was predicted for CMA1. Interleukin-9 has been reported to decrease expression of human NCK1 in MDA-MB-231 human breast cells, and to differentially regulate actin cytoskeleton-related proteins such as NCK1 [49]. Interestingly, both SPTAN1 and CFL1 are filamentous cytoskeletal and actin-related proteins, while CMA1 could participate in extracellular matrix degradation [50]. We were unable to validate the NCK1 findings using ELISA-measurements due to the lack of CIMT measurements in the validation sample.
We were able to confirm three additional proteins associated with CIMT using our age-sex adjusted model namely GFRA1, IGFBP2 and GHR, which have been all reported to be linked to CVD, mortality, and atherosclerosis [51, 52]. IGFBP2 was the unique obtained negative association. The same direction effect has been reported as a strong association with type 2 diabetes in a comparison study of incident type 2 diabetes and coronary heart disease in the KORA cohort [53].
In this study, we identified proteins specifically associated with either CHD or CIMT. Previous reports on KORA F4 have already stated a non-linear relation between CIMT and CHD risk [54]. Thus, this complex relationship amongst the two phenotypes could help to explain the specificity of our findings. In a sensitivity analysis additionally adjusting for CRP, the results of our full models did not change. Thus, our reported associations are independent from CRP, an inflammation marker of the acute phase response.
A major strength of our study is the proteome-wide approach, which covers proteins at low abundance levels in plasma. By conducting a hypothesis-free analysis, we were able to analyze the association of a wide array of plasma proteins with CHD and CIMT. An additional strength is the availability of an independent sample, which we could use to validate initial results with an alternative measurement technique that provides absolute concentrations. Our study also has limitations. The lack of patient differentiation by CHD severity could, for instance, be attenuating some associations. Manifestations of early-stage CHD differ from the late-stage CHD. In the latter, protein levels change due to myocardial injury and physiological compensation. Additionally, the difference in plaque vulnerability and extent of atherosclerosis between stable and unstable CHD [55], may also impact the plasma proteome. Finally, due to the cross-sectional nature of our study, temporal relations cannot be inferred.
In summary, our proteome-wide study identified a new association of galectin-4 with CHD. Galectin-4 may be involved in atherosclerosis by enhancing lipid raft stabilization, which subsequently affects redox signaling pathways. Moreover, we report the association of NCK1 with CIMT.
Availability of data and materials
The informed consent given by KORA study participants does not cover data posting in public databases. However, data are available upon request by means of a project agreement from KORA (https://helmholtz-muenchen.managed-otrs.com/external).
References
Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart Disease and Stroke Statistics-2018 update: a Report from the American Heart Association. Circulation. 2018;137(12):e67–492.
Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109–14.
Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and rupture. Circ Res. 2014;114(12):1852–66.
Ravani A, Werba JP, Frigerio B, Sansaro D, Amato M, Tremoli E, et al. Assessment and relevance of carotid intima-media thickness (C-IMT) in primary and secondary cardiovascular prevention. Curr Pharm Des. 2015;21(9):1164–71.
Inaba Y, Chen JA, Bergmann SR. Carotid intima-media thickness and cardiovascular events. N Engl J Med. 2011;365(17):1640–1. author reply 1641-2.
Polak JF, O’Leary DH. Carotid intima-media thickness as surrogate for and predictor of CVD. Glob Heart. 2016;11(3):295–e3123.
van den Oord SCH, Sijbrands EJG, ten Kate GL, van Klaveren D, van Domburg RT, van der Steen AFW, et al. Carotid intima-media thickness for cardiovascular risk assessment: systematic review and meta-analysis. Atherosclerosis. 2013;228(1):1–11.
Doneen AL, Bale BF. Carotid intima-media thickness testing as an asymptomatic cardiovascular disease identifier and method for making therapeutic decisions. Postgrad Med. 2013;125(2):108–23.
Darabian S, Hormuz M, Latif MA, Pahlevan S, Budoff MJ. The role of carotid intimal thickness testing and risk prediction in the development of coronary atherosclerosis. Curr Atheroscler Rep. 2013;15(3):306.
Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis. Circulation. 2007;115(4):459–67.
Verwer MC, Mekke J, Timmerman N, Waissi F, Boltjes A, Pasterkamp G, et al. Comparison of cardiovascular biomarker expression in extracellular vesicles, plasma and carotid plaque for the prediction of MACE in CEA patients. Sci Rep. 2023;13(1):1010.
Herrington DM, Mao C, Parker SJ, Fu Z, Yu G, Chen L, et al. Proteomic Architecture of Human Coronary and aortic atherosclerosis. Circulation. 2018;137(25):2741–56.
Stakhneva EM, Striukova EV, Ragino YI. Proteomic studies of blood and vascular wall in atherosclerosis. Int J Mol Sci. 2021;22(24):13267.
Dardé VM, de la Cuesta F, Dones FG, Alvarez-Llamas G, Barderas MG, Vivanco F. Analysis of the plasma proteome associated with acute coronary syndrome: does a permanent protein signature exist in the plasma of ACS patients? J Proteome Res. 2010;9(9):4420–32.
Kristensen LP, Larsen MR, Mickley H, Saaby L, Diederichsen ACP, Lambrechtsen J, et al. Plasma proteome profiling of atherosclerotic disease manifestations reveals elevated levels of the cytoskeletal protein vinculin. J Proteom. 2014;101:141–53.
Yin X, Subramanian S, Hwang SJ, O’Donnell CJ, Fox CS, Courchesne P, et al. Protein biomarkers of new-onset cardiovascular disease: prospective study from the systems approach to biomarker research in cardiovascular disease initiative. Arterioscler Thromb Vasc Biol. 2014;34(4):939–45.
Májek P, Reicheltová Z, Suttnar J, Malý M, Oravec M, Pečánková K, et al. Plasma proteome changes in cardiovascular disease patients: novel isoforms of apolipoprotein A1. J Transl Med. 2011;9:84.
Cubedo J, Padró T, García-Moll X, Pintó X, Cinca J, Badimon L. Proteomic signature of Apolipoprotein J in the early phase of new-onset myocardial infarction. J Proteome Res. 2011;10(1):211–20.
Cubedo J, Padró T, Cinca J, Mata P, Alonso R, Badimon L. Retinol-binding protein 4 levels and susceptibility to ischaemic events in men. Eur J Clin Invest. 2014;44(3):266–75.
Cubedo J, Padró T, Badimon L. Coordinated proteomic signature changes in immune response and complement proteins in acute myocardial infarction: the implication of serum amyloid P-component. Int J Cardiol. 2013;168(6):5196–204.
Ngo D, Sinha S, Shen D, Kuhn EW, Keyes MJ, Shi X, et al. Aptamer-based proteomic profiling reveals novel candidate biomarkers and pathways in Cardiovascular Disease. Circulation. 2016;134(4):270–85.
Holle R, Happich M, Löwel H, Wichmann HE, MONICA/KORA Study Group. KORA–a research platform for population based health research. Gesundheitswesen. 2005;67(Suppl 1):S19–25.
Suhre K, Arnold M, Bhagwat AM, Cotton RJ, Engelke R, Raffler J, et al. Connecting genetic risk to disease end points through the human blood plasma proteome. Nat Commun. 2017;8:14357.
Kowall B, Ebert N, Then C, Thiery J, Koenig W, Meisinger C, et al. Associations between blood glucose and carotid intima-media thickness disappear after adjustment for shared risk factors: the KORA F4 study. PLoS ONE. 2012;7(12):e52590.
Then C, Kowall B, Lechner A, Meisinger C, Heier M, Koenig W, et al. Plasma MR-proANP levels are associated with carotid intima-media thickness in the general community: the KORA F4 study. Atherosclerosis. 2013;230(2):235–41.
Bots ML, Mulder PG, Hofman A, van Es GA, Grobbee DE. Reproducibility of carotid vessel wall thickness measurements. The Rotterdam Study. J Clin Epidemiol. 1994;47(8):921–30.
Gold L, Ayers D, Bertino J, Bock C, Bock A, Brody EN, et al. Aptamer-based multiplexed proteomic technology for biomarker discovery. PLoS ONE. 2010;5(12):e15004.
Candia J, Cheung F, Kotliarov Y, Fantoni G, Sellers B, Griesman T, et al. Assessment of Variability in the SOMAscan Assay. Sci Rep. 2017;7(1):14248.
Cao ZQ, Guo XL. The role of galectin-4 in physiology and diseases. Protein Cell. 2016;7(5):314–24.
Catalgol B, Kartal Ozer N. Lipid rafts and redox regulation of cellular signaling in cholesterol induced atherosclerosis. Curr Cardiol Rev. 2010;6(4):309–24.
Schroder J, Zethner-Moller R, Bové KB, Mygind ND, Hasbak P, Michelsen MM, et al. Protein biomarkers and coronary microvascular dilatation assessed by rubidium-82 PET in women with angina pectoris and no obstructive coronary artery disease. Atherosclerosis. 2018;275:319–27.
Molvin J, Jujić A, Melander O, Pareek M, Råstam L, Lindblad U, et al. Proteomic exploration of common pathophysiological pathways in diabetes and cardiovascular disease. ESC Heart Fail. 2020;7(6):4151–8.
Rullman E, Melin M, Mandić M, Gonon A, Fernandez-Gonzalo R, Gustafsson T. Circulatory factors associated with function and prognosis in patients with severe heart failure. Clin Res Cardiol. 2020;109(6):655–72.
Korduner J, Holm H, Jujic A, Melander O, Pareek M, Molvin J, et al. Galectin-4 levels in hospitalized versus non-hospitalized subjects with obesity: the Malmö Preventive Project. Cardiovasc Diabetol. 2022;21(1):125.
Fernández Cisnal A, García-Blas S, Valero E, Miñana G, Núñez J, Sanchis Forés J. Trefoil factor-3 and galectin-4 as new candidates for prognostic biomarkers in ST-segment elevation myocardial infarction. Rev Esp Cardiol (Engl Ed). 2020;73(5):418–20.
Zarubin T, Han J. Activation and signaling of the p38 MAP kinase pathway. Cell Res. 2005;15(1):11–8.
Heming M, Gran S, Jauch SL, Fischer-Riepe L, Russo A, Klotz L, et al. Peroxisome proliferator-activated Receptor-γ modulates the response of macrophages to Lipopolysaccharide and glucocorticoids. Front Immunol. 2018;9:893.
Sayer G, Bhat G. The renin-angiotensin-aldosterone system and heart failure. Cardiol Clin. 2014;32(1):21–32. vii.
Alderman MH, Madhavan S, Ooi WL, Cohen H, Sealey JE, Laragh JH. Association of the renin-sodium profile with the risk of myocardial infarction in patients with hypertension. N Engl J Med. 1991;324(16):1098–104.
Katsiki N, Mikhailidis DP, Banach M. Leptin, cardiovascular diseases and type 2 diabetes mellitus. Acta Pharmacol Sin. 2018;39(7):1176–88.
Gonçalves I, Edsfeldt A, Colhoun HM, Shore AC, Palombo C, Natali A, et al. Association between renin and atherosclerotic burden in subjects with and without type 2 diabetes. BMC Cardiovasc Disord. 2016;16(1):171.
Fuchs R, Gassen HG. Nucleotide sequence of human preprocathepsin H, a lysosomal cysteine proteinase. Nucleic Acids Res. 1989;17(22):9471.
Han SR, Momeni A, Strach K, Suriyaphol P, Fenske D, Paprotka K, et al. Enzymatically modified LDL induces cathepsin H in human monocytes: potential relevance in early atherogenesis. Arterioscler Thromb Vasc Biol. 2003;23(4):661–7.
Papadaki S, Tselepis AD. Nonhemostatic activities of factor xa: are there Pleiotropic effects of Anti-FXa. Direct Oral Anticoagulants? Angiol. 2019;70(10):896–907.
Brummel-Ziedins KE, Lam PH, Gissel M, Gauthier E, Schneider DJ. Depletion of systemic concentrations of coagulation factors in blood from patients with atherosclerotic vascular disease. Coron Artery Dis. 2013;24(6):468–74.
Alfaidi M, Acosta CH, Wang D, Traylor JG, Orr AW. Selective role of Nck1 in atherogenic inflammation and plaque formation. J Clin Invest. 2020;130(8):4331–47.
Chen J, Leskov IL, Yurdagul A, Thiel B, Kevil CG, Stokes KY, et al. Recruitment of the adaptor protein nck to PECAM-1 couples oxidative stress to canonical NF-κB signaling and inflammation. Sci Signal. 2015;8(365):ra20.
Gimbrone MA, García-Cardeña G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res. 2016;118(4):620–36.
Das S, Surve V, Marathe S, Wad S, Karulkar A, Srinivasan S, et al. IL-9 abrogates the metastatic potential of breast Cancer by Controlling Extracellular Matrix Remodeling and Cellular Contractility. J Immunol. 2021;206(11):2740–52.
Kanefendt F, Thuß U, Becka M, Boxnick S, Berse M, Schultz A, et al. Pharmacokinetics, Safety, and tolerability of the novel chymase inhibitor BAY 1142524 in healthy male volunteers. Clin Pharmacol Drug Dev. 2019;8(4):467–79.
Wang W, Yu K, Zhao SY, Mo DG, Liu JH, Han LJ, et al. The impact of circulating IGF-1 and IGFBP-2 on cardiovascular prognosis in patients with acute coronary syndrome. Front Cardiovasc Med. 2023;10:1126093.
Ngo LH, Austin Argentieri M, Dillon ST, Kent BV, Kanaya AM, Shields AE, et al. Plasma protein expression profiles, cardiovascular disease, and religious struggles among South asians in the MASALA study. Sci Rep. 2021;11(1):961.
Huth C, Bauer A, Zierer A, Sudduth-Klinger J, Meisinger C, Roden M, et al. Biomarker-defined pathways for incident type 2 diabetes and coronary heart disease-a comparison in the MONICA/KORA study. Cardiovasc Diabetol. 2020;19(1):32.
Simonetto C, Heier M, Rospleszcz S, Meisinger C, Then C, Seißler J, et al. Risk for cardiovascular events responds nonlinearly to carotid intima-media thickness in the KORA F4 study. Atherosclerosis. 2020;296:32–9.
Agewall S. Acute and stable coronary heart disease: different risk factors. Eur Heart J. 2008;29(16):1927–9.
Acknowledgements
We thank Ulrike Lissner for technical support in ELISA measurements and Dr. Pamela Matías-García for data analysis support in PCA plots for quality control.
Funding
Open Access funding enabled and organized by Projekt DEAL. The KORA study was initiated and financed by the Helmholtz Zentrum München– German Research Center for Environmental Health, which is funded by the German Federal Ministry of Education and Research (BMBF) and by the State of Bavaria. Data collection in the KORA study is done in cooperation with the University Hospital of Augsburg. Furthermore, KORA research was supported within the Munich Center of Health Sciences (MC Health), Ludwig-Maximilians-Universität, as part of LMUinnovativ. This research received funding from the German Centre for Cardiovascular Research (DZHK) under grant number DZHK B 19−017 SE and 81×2400136. This project is also funded by the Bavarian State Ministry of Health and Care through the research project DigiMed Bayern (www.digimed-bayern.de).
Author information
Authors and Affiliations
Contributions
MAE, MCGA, CWC and SN interpreted the data, wrote, and revised the manuscript. CWC and MAE participated in the design of the study and analyzed the data. MW conceived the research question, participated in its design and revised the manuscript. EH participated in the design and measurement of the protein replication and revised the manuscript. AP, MW, CG, JG, KS, SK, WR, JS, WK, MN, UV, EH, TD, CM were involved in the data collection, data management, and preparation of their respective cohorts. All authors contributed to the writing of the article, critically reviewed it, and approved the final version for submission.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The KORA (Cooperative health research in the Region of Augsburg) study is an independent population-based cohort study in southern Germany [22]. The study was approved by the ethics committee of the Bavarian Medical Association and was carried out in accordance with the principles of the Declaration of Helsinki. All study participants signed written informed consent prior to their participation in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Elhadad, M.A., del C. Gómez-Alonso, M., Chen, CW. et al. Plasma proteome association with coronary heart disease and carotid intima media thickness: results from the KORA F4 study. Cardiovasc Diabetol 23, 181 (2024). https://doi.org/10.1186/s12933-024-02274-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02274-3