
Abstract
Background
Use of sodium-glucose-cotransporter-2 (SGLT2) inhibitors often causes an initial decline in glomerular filtration rate (GFR). This study addresses the question whether the initial decline of renal function with SGLT2 inhibitor treatment is related to vascular changes in the systemic circulation.
Methods
We measured GFR (mGFR) and estimated GFR (eGFR) in 65 patients with type 2 diabetes (T2D) at baseline and after 12 weeks of treatment randomized either to a combination of empagliflozin and linagliptin (SGLT2 inhibitor based treatment group) (n = 34) or metformin and insulin (non-SGLT2 inhibitor based treatment group) (n = 31). mGFR was measured using the gold standard clearance technique by constant infusion of inulin. In addition to blood pressure (BP), we measured pulse wave velocity (PWV) under standardized conditions reflecting vascular compliance of large arteries, as PWV is considered to be one of the most reliable vascular parameter of cardiovascular (CV) prognosis.
Results
Both mGFR and eGFR decreased significantly after initiating treatment, but no correlation was found between change in mGFR and change in eGFR in either treatment group (SGLT2 inhibitor based treatment group: r=-0.148, p = 0.404; non-SGLT2 inhibitor based treatment group: r = 0.138, p = 0.460). Noticeably, change in mGFR correlated with change in PWV (r = 0.476, p = 0.005) in the SGLT2 inhibitor based treatment group only and remained significant after adjustment for the change in systolic BP and the change in heart rate (r = 0.422, p = 0.018). No such correlation was observed between the change in eGFR and the change in PWV in either treatment group.
Conclusions
Our main finding is that after initiating a SGLT2 inhibitor based therapy an exaggerated decline in mGFR was related with improved vascular compliance of large arteries reflecting the pharmacologic effects of SGLT2 inhibitor in the renal and systemic vascular bed. Second, in a single patient with T2D, eGFR may not be an appropriate parameter to assess the true change of renal function after receiving SGLT2 inhibitor based therapy.
Trial registration
clinicaltrials.gov (NCT02752113).
Similar content being viewed by others


Introduction
Sodium-glucose-cotransporter-2 (SGLT2) inhibitors have demonstrated remarkable cardiovascular (CV) and renal benefits beyond glycemic control in several trials and emerged as therapeutic agents in the treatment of heart failure and chronic kidney disease [1,2,3,4,5,6,7,8,9,10]. However, it has been repeatedly described that initiation of SGLT2 inhibitor therapy causes an initial decline of estimated glomerular filtration rate (eGFR), which may lead to physician’s concern [1, 6, 7, 11,12,13,14,15]. This initial decline in eGFR with SGLT2 inhibitor treatment is suggested to be related to a reduction in intraglomerular pressure [7, 11,12,13,14,15,16]. The mechanism underlying the reduction of the intraglomerular pressure with SGLT2 inhibitor treatment appears to be different in different cohorts. Previously, we showed in type 2 diabetes (T2D) patients with empagliflozin treatment that this reduction in intraglomerular pressure is caused by a postglomerular vasodilatation, rather than a preglomerular vasoconstriction by tubuloglomerular feedback as demonstrated in patients with type 1 diabetes and experimental studies [16,17,18]. In support to our study, van Bommel et al. observed similar results in T2D patients with dapagliflozin treatment [19]. Although this vasodilatory effect on the efferent arterioles results in an initial drop in eGFR, in the long term it comes to an improvement of kidney function and slows the progression of kidney disease [1, 3, 6, 7].
The predictive and clinical value of the initial eGFR decline remains controversial. While the post-hoc analysis of the EMPA-REG OUTCOME trial did not find any association between the initial “eGFR dip” and the treatment effect of empagliflozin, similar analysis of the DAPA-HF trial showed better clinical outcome in patients with initial eGFR decline after dapagliflozin treatment [11, 14]. In consequence, this controversial results regarding initial decline in eGFR might result in an inappropriate discontinuation of the pharmacotherapy by healthcare providers or patients themselves, out of fear that the medication could harm the kidneys. This may result in a missed opportunity to slow the progression of kidney and CV disease. Thus, there is a crucial need to understand the implications of the initial GFR decline after the beginning of SGLT2 inhibitor treatment.
Previously, we have shown that SGLT2 inhibitor treatment exerts beneficial effects on different vascular parameters, e.g. in the renal and systemic circulation in different cohorts [20,21,22]. The main aim of the current study was to evaluate whether there is a relationship between the initial GFR decline assessed using input steady state input clearance technique with inulin and vascular changes in the systemic circulation. In addition to renal function, we measured pulse wave velocity (PWV) since according to several guidelines [23,24,25] PWV is recommended to most reliably reflect vascular compliance of large arteries in the systemic circulation. Moreover, PWV has been identified to be an independent prognostic marker of CV fatal events [26,27,28,29,30] and its change to improved prognosis [31].
Materials and methods
Study design
This single-center, retrospective study includes 65 patients with T2D who were randomized (1:1) either to receive empagliflozin and linagliptin (SGLT2 inhibitor based treatment) or metformin and insulin (non-SGLT2 inhibitor based treatment) combination therapy. We analyzed the SGLT2 inhibitor based treatment group and the non-SGLT2 inhibitor based treatment group (control group) separately. The rationale for these combination treatments was to compare the renal hemodynamic effects of the timely standard combination T2D treatment (SGLT2 inhibitor + Dipeptidyl peptidase 4 inhibitor) with the combination of insulin and metformin (traditional or old way of treatment). All patients participated in the „Effects of Empagliflozin + Linagliptin vs. Metformin + Insulin Glargine on Renal and Vascular Changes in Type 2 Diabetes (ELMI)“ trial (NCT02752113) between April 2016 and November 2018 in our clinical research center at the University Hospital Erlangen-Nuremberg (www.crc-erlangen.de). The main results of the effects of these two different anti-hyperglycmic treatment strategies have been reported previously [17, 20]. Here we analyzed the prespecified analysis of patients with completed inulin clearance at baseline and after 12 weeks of treatment (The inulin application had to be immediately stopped in our lab after an official warning due to anaphylactic reactions observed during infusions of inulin in France, which ultimately lead to the withdrawal of inulin from the market).
All patients had stable metformin medication for at least 3 months (850 or 1000 mg orally twice daily). Patients that were randomized to the SGLT2inhibitor based treatment study arm received 10 mg empagliflozin and 5 mg linagliptin orally once daily. Empagliflozin was uptitrated to 25 mg if fasting blood glucose was ≥ 100 mg/dl. Patients in the non-SGLT2 inhibitor based treatment group received initially 2–4 units (U) of insulin subcutaneous once daily in addition to their metformin medication. It was adjusted every third day by adding 2 U if fasting blood glucose was not ≤ 125 mg/dl until stable dose was reached.
The respective study was approved by the local Ethical Review Committee (ethics committee of the University of Erlangen-Nuremberg, Germany) and the study was conducted according to the Declaration of Helsinki. Written informed consent was obtained from all patients prior to study inclusion.
Study cohort
A total of 65 patients with T2D aged 18–75 were included in this analysis. Thirty-four patients have been allocated to the SGLT2 inhibitor based treatment group and 31 to the non-SGLT2 inhibitor based treatment group. The eligibility criteria for the study included an glycated haemoglobin (HbA1c) level of ≥ 6.5% for those individuals with antidiabetic monotherapy and ≥ 6.0% for those receiving dual antidiabetic therapy. Main exclusion criteria were the use of insulin, glitazones, dipeptidyl peptidase-4 inhibitor or SGLT2 inhibitor within two months prior to randomization. Patients with congestive heart failure New York Heart Association (NYHA) III/IV were excluded. Furthermore, patients with HbA1c > 10.5% or fasting plasma glucose > 240 mg/dl, urinary albumin to creatinine ratio (UACR) > 300 mg/g, eGFR < 60 ml/min/1.73 m², body-mass-index (BMI) > 40 kg/m² or cardio- and cerebro-vasacular events within the past 6 months were not considered for the study. For female patients, a negative pregnancy test was mandatory before and during the study period.
Assessments
Vascular and renal function measurements were performed at baseline and after 12 weeks of treatment. These measurements have been described in detail previously [17, 20]. Briefly, before attended BP measurement was performed the patient remained seated and relaxed for 3–5 min. An appropriate cuff size was selected according to the arm circumference of each individual. Office BP were calculated from the average of three measurements and were measured with validated devices following the recommendations of the European Society of Hypertension/European Society of Cardiology [32, 33]. . The SphygmoCor™ system (AtCor Medical, Sydney, Australia) was used for the vascular assessment of the compliance of large arteries by measuring pulse wave velocity (PWV) under standardized conditions in our research facility.
Constant-infusion input-clearance technique with inulin (Inutest, Fresenius, Linz, Austria) and sodium p-aminohippurate (PAH) (Daiichi Sankyo, Tokyo, Japan) were used to measure the true renal function (mGFR) and renal plasma flow (RPF), respectively. This method is the most widely used method for the measurement of mGFR since a good correlation between the traditional method with urine collection and the constant infusion technique without urine collection (r = 0.993) has been demonstrated [34]. Based on serum creatinine measurements, the eGFR was calculated according to the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula [17].
Statistical analysis
Statistical analysis was performed using SPSS Statistics 28.0 (IBM, Armonk, New York, USA) and data were expressed as mean ± standard deviation (SD) in text and tables. A two-sided p-value of < 0.05 was considered statistically significant. Paired t-test was applied for the comparison of the end of 12 weeks treatment phase versus baseline within each treatment group. The unpaired Student’s t-test was used to determine the statistical significance of the differences between the SGLT2 inhibitor based and non-SGLT2 inhibitor based treatment arms. Bivariate correlation analyses were assessed by performing Pearson’s test. The correlation analysis of the parameter UACR was assessed by performing Spearman’s test, since UACR was not normally distributed. Since change of PWV is strongly dependent on change in systolic BP, we adjusted our approach to the change of systolic BP and the change of heart rate after 12 weeks by applying covariance analysis. The Bland-Altman Plot was used as a descriptive tool to evaluate the agreement between two methods, showing the relationship between the change of mGFR and eGFR and the mean of the two methods.
Results
Clinical characteristics at baseline and after 12 weeks of treatment
The clinical characteristics of the SGLT2 inhibitor based treatment (n = 34) and non-SGLT2 inhibitor based treatment (n = 31) groups are shown in Table 1. The average age of the patients was 59.4 ± 8.4 years in the SGLT2 inhibitor based treatment group and 59.9 ± 9.7 years in the non-SGLT2 inhibitor based treatment group. 77% of the patients were male with no between group differences. The two groups did not differ in terms of demographic data.
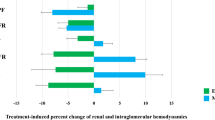
We observed a significant reduction of glycaemic parameters like fasting plasma glucose and HbA1c after 12 weeks in both treatment arms (Table 2). Patients in the SGLT2 inhibitor based treatment arm had a significant reduction in weight and BMI, whereas no change in these parameters was observed in the non-SGLT2 inhibitor based treatment group (Table 2). The effects on renal hemodynamics of the SGLT2 inhibitor based treatment group and non-SGLT2 inhibitor based treatment group have been described previously [17] and are presented in Table 2 for the patients included in the current analysis. Renal function decreased in both treatment groups irrespective whether analysed by mGFR or eGFR. Briefly, in patients with SGLT2 inhibitor based treatment, PWV decreased from 8.2 ± 1.6 to 7.8 ± 1.5 m/s after 12 weeks of treatment (p = 0.028), whereas no change in PWV occurred after 12 weeks of treatment in the non-SGLT2 inhibitor based treatment group (p = 0.169).
Relationship between renal and systemic vascular bed
The change of mGFR in the SGLT2 inhibitor based treatment group correlated with the change of PWV (r = 0.476, p = 0.005, Table 3A, Fig. 1A). Such a correlation could not be shown between the change of eGFR and the change of PWV (r=-0.038, p = 0.834, Table 3A, Fig. 1B). We did not found any correlation between PWV and mGFR or eGFR in the non-SGLT2 inhibitor based treatment group (all p > 0.10, Table 3B). Similarly, we found a correlation between change of mGFR and change of office systolic BP (r = 0.398, p = 0.023; Fig. 2) as well as change of office diastolic BP (r = 0.354, p = 0.040) in the SGLT2 inhibitor based treatment group, but no correlation between change of eGFR and change of office systolic or diastolic BP was observed. Noticeably, the relationship described between change in mGFR and change in PWV remained significant after adjustment for the change of systolic BP and the change of heart rate after 12 weeks (r = 0.422, p = 0.018). In the non-SGLT2 inhibitor based treatment group no such correlations of the changes in systolic and diastolic BP with change in PWV were observed with neither mGFR nor eGFR.

Correlation between change in mGFR (A; upper part) or change in eGFR (B; lower part) and change in PWV after 12 weeks of treatment in SGLT2 inhibitor based treatment group

Correlation between change in mGFR and change in office systolic blood pressure after 12 weeks of treatment in SGLT2 inhibitor based treatment group
In addition, we observed a correlation between change in mGFR (but not with eGFR) and change in UACR and change in high sensitive C reactive protein (hs-CRP) in patients in the SGLT2 inhibitor based treatment only (r = 0.367, p = 0.033 and r = 0.376, p = 0.031, Fig. 3a and b). We did not observe any correlation between change in mGFR and change in fasting plasma glucose (r = 0.177, p = 0.317) or change in HbA1c (r=-0.235, p = 0.181). No correlation between change in eGFR and change in fasting plasma glucose (r = 0.025, p = 0.889) or change in HbA1c (r = 0.136, p = 0.443) was observed as well.

Correlation between change in in mGFR after 12 weeks of treatment and change in UACR (A; upper part) and change in hs-CRP (B; lower part) in SGLT2 inhibitor based treatment group
Relationship between change in mGFR and change in eGFR
Despite a reduction of mGFR and eGFR, we observed no correlation between the change of mGFR and eGFR (r=-0.148, p = 0.404, Fig. 4). Comparing the decline in eGFR and mGFR in the SGLT2 inhibitor based treatment cohort, we found that the decline of true renal function (mGFR) tended to be lower compared to the decline of eGFR (p = 0.057). In accordance, the Bland-Altman plot shows poor agreement between mGFR and eGFR change with wide limits of agreement ranging from − 33.2 to + 47.0 ml/min/1.73 m² (Fig. 5).

Correlation between change in mGFR and change in eGFR after 12 weeks of treatment in SGLT2 inhibitor based treatment group

Bland-Altman Plot for the agreement between change in mGFR and change in eGFR in the SGLT2 inhibitor based treatment group
Discussion
SGLT2 inhibitor therapy often causes an initial decline of eGFR after starting treatment. The main finding of our study is that the initial decline in true renal function, which is defined as mGFR, with SGLT2 inhibitor treatment is linearly associated with improved vascular compliance of large arteries, thereby reflecting the pharmacologic effects of SGLT2 inhibitors both in the renal and systemic vascular bed. No such relationship was observed in the non-SGLT2 inhibitor based therapy serving as a control group in this retrospective study. Another key message of this study is that the decline in eGFR with SGLT2 inhibitor treatment does not reflect the decline in true renal function. This lack of relationship may explain also the failure to find any correlations between the change in eGFR and change in PWV. Thus, we postulate if renal function is correctly assessed, decline of GFR after starting SGLT2 inhibitor therapy is paralleled by changes of vascular compliance of large arteries in the systemic circulation.
While we observed a decline in eGFR and mGFR for both treatment arms, only patients in the SGLT2 inhibitor based treatment arm had a significant decrease in PWV from 8.2 ± 1.6 to 7.8 ± 1.5 m/s after 12 weeks of treatment. As suggested in the current guidelines of the European Society of Hypertension, PWV is known to be a unique measure of arterial stiffness and an important tool to assess vascular aging [23, 35, 36]. Two large meta-analyses revealed that this parameter is able to classify CV risk more accurately than conventional risk-based scores and that it improves CV event prediction, especially in young and middle-aged patients [26, 27]. Cherney et al. previously reported a decrease in arterial stiffness in 40 subjects with type 1 diabetes after 8 weeks of empagliflozin treatment [37]. In accordance, we previously reported beneficial effects of 12 weeks SGLT2 inhibitor based treatment regarding vascular function [20]. Noticeably, in this study we observed a correlation between the change of mGFR and the change of PWV with SGLT2 inhibitor based treatment, which demonstrates the close relationship between renal and systemic vascular bed. This correlation was only observed in the SGLT2 inhibitor based treatment group and persisted after adjustment for the change of office systolic BP and the change of heart rate after 12 weeks. Moreover, we observed a correlation between change in mGFR and change in office systolic and diastolic BP in the SGLT2 inhibitor based treatment group. Thus, the observed linear relationship between decline of mGFR and PWV indicate that decline of mGFR reflects also vascular changes in the systemic circulation exerted by SGLT2 inhibitors, and the magnitude of the initial decline of renal function is therefore of clinical relevance indicative of the magnitude of improved arterial stiffness.
In accordance, the DAPA-HF results showed an association between the initial decline in eGFR after dapagliflozin treatment and better CV outcome [11]. Compared to patients without initial eGFR decline, patients with an initial eGFR decline also had a slower long term eGFR decline [11]. Van Bommel et al. previously reported a reduction in pulse pressure in patients with T2D after 12 weeks of dapagliflozin treatment and a correlation between the reduction in pulse pressure and the reduction in mGFR [38]. Similar to PWV, pulse pressure is an indirect marker of arterial stiffness. Noticeably, in our study we observed the association between the change of mGFR and improvement of arterial stiffness independent of BP changes. In contradiction to these results a post hoc analysis of the EMPA-REG OUTCOME trial could not find any impact of the initial eGFR dip and the treatment effect of empagliflozin on CV outcome [14].
In accordance to our main results, we observed a correlation between change in mGFR and change in UACR in the SGLT2 inhibitor based treatment group. Increased urinary albumin excretion is considered as a marker of impaired permeability of the endothelium in the renal circulation. Likewise, transcapillary escape of radioactively marked albumin has been observed in the systemic circulation [39], thus suggesting that increased albumin escape from the blood stream (which can be easily measured in the renal vascular bed by UACR) is a marker not restricted to indicate renal prognosis. In several prospective clinical studies, albuminuria has been found to be an independent risk marker for CV events in various CV high risk populations, including T2D [40,41,42,43,44,45]. Our finding regarding the relationship of change in UACR and change in mGFR in the SGLT2 inhibitor based treatment group again support the link between the renal and systemic vascular bed.
Porrini E. et al. previously discussed the reliability of eGFR equations and concluded them to be unreliable tools to assess renal function in individual patients [46]. In accordance, we did not observe any correlation between the change of eGFR and mGFR after initiating SGLT2 inhibitor based treatment. Similarly, we have shown in a study with 190 T2D patients in the early stage of their disease that change of renal function after various short-term pharmacological intervention is not accurately and precisely reflected by the change of eGFR.
There is no doubt that carefully conducted pharmacological studies documented that SGLT2 inhibitors decrease renal function in several study cohorts. The inaccuracy of eGFR to measure renal function may be dependent on the sample size of study populations. In large-scale populations there is a consistent decrease of eGFR and individual variations of eGFR may be offset by large number of patients [2, 9, 47]. Nevertheless, from a clinical perspective, eGFR may not be an appropriate parameter to assess the true change of renal function in a given patient or small study cohorts after receiving a SGLT2 inhibitor therapy, since according to our data any decline in eGFR with SGLT2 inhibitor treatment does not necessarily reflect a decline in true renal function .
In our study, we not only observed a decline in GFR in patients with SGLT2 inhibitor based treatment, but also in patients receiving the non- SGLT2 inhibitor based treatment with insulin + metformin. Our group previously reported a decrease in renal plasma flow and renal blood flow paralleled by an increase in renal vascular resistance in patients with insulin + metformin treatment, which may explain the decline in GFR in this treatment group [17].
Limitations
Our study has several limitations. It is a single-center analysis with a small sample size due to the forced by the lack of availability of inulin due to its withdrawal from the market. However, it is a prespecified analysis and in contrast to the large controlled randomized trials [2, 9, 11, 14], we measured GFR in our patients with the “gold standard”, which is a reliable tool to assess true renal function. Patients were randomized to receive either empagliflozin and linagliptin or metformin and insulin. For our present analysis this combination treatment is a limitation, since it is not possible to attribute the association between vascular improvement and mGFR decline only to empagliflozin treatment. However, we previously showed that linagliptin treatment does not cause any decline in mGFR or eGFR or any other renal hemodynamic parameter [48]. Thus, we believe that the GFR decline in our trial and its correlation to the change in PWV is attributed to the initiation of empagliflozin treatment. Our study cohort include only patients with T2D and our findings cannot be necessarily transferred to other cohorts like patients with type 1 diabetes, chronic kidney disease or heart failure.
Conclusion
In conclusion, we found that initial decline in true renal function with SGLT2 inhibitor based treatment goes in parallel with improved vascular stiffness of large arteries, thereby reflecting the pharmacologic effects of SGLT2 inhibitors both in the renal and systemic vascular bed. Thus, our data indicate that decline of renal function reflects also changes in vascular function in the systemic circulation, i.e. improvement of arterial stiffness. According to our observations, eGFR may not be an appropriate parameter to assess the true change in renal function after receiving SGLT2 inhibitor based treatment in an individual patient and potentially may lead to the inappropriate decision to discontinue SGLT2 inhibitor therapy.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SGLT2:
-
Sodium–glucose–cotransporter–2
- CV:
-
cardiovascular
- GFR:
-
glomerular filtration rate
- mGFR:
-
measured GFR
- eGFR:
-
estimated GFR
- T2D:
-
type 2 diabetes
- BP:
-
blood pressure
- PWV:
-
pulse wave velocity
- U:
-
units
- UACR:
-
urinary albumin to creatinine ratio
- BMI:
-
body–mass–index
- CKD:
-
EPI–Chronic Kidney Disease Epidemiology Collaboration
- SD:
-
standard deviation
- Hs:
-
CRP–high sensitive C reactive protein
- HbA1c:
-
glycated haemoglobin
References
Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou F-F, Mann JFE, McMurray JJV, Lindberg M, Rossing P, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–46.
McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, Ponikowski P, Sabatine MS, Anand IS, Bělohlávek J, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008.
Mosenzon O, Wiviott SD, Cahn A, Rozenberg A, Yanuv I, Goodrich EL, Murphy SA, Heerspink HJL, Zelniker TA, Dwyer JP, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019;7(8):606–17.
Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W, Law G, Desai M, Matthews DR. Canagliflozin and Cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–57.
Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, Januzzi J, Verma S, Tsutsui H, Brueckmann M, et al. Cardiovascular and renal outcomes with Empagliflozin in Heart failure. N Engl J Med. 2020;383(15):1413–24.
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, Edwards R, Agarwal R, Bakris G, Bull S, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–306.
Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, Johansen OE, Woerle HJ, Broedl UC, Zinman B. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323–34.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, et al. Dapagliflozin and Cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–57.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, et al. Empagliflozin, Cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–28.
Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, Emberson JR, Preiss D, Judge P, Mayne KJ, Ng SYA, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2023;388(2):117–27.
Adamson C, Docherty KF, Heerspink HJL, de Boer RA, Damman K, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, Petrie MC, et al. Initial decline (dip) in estimated glomerular filtration rate after initiation of Dapagliflozin in patients with heart failure and reduced ejection fraction: insights from DAPA-HF. Circulation. 2022;146(6):438–49.
Heerspink HJ, Desai M, Jardine M, Balis D, Meininger G, Perkovic V. Canagliflozin slows progression of renal function decline independently of Glycemic effects. J Am Soc Nephrol. 2017;28(1):368–75.
Heerspink HJ, Johnsson E, Gause-Nilsson I, Cain VA, Sjöström CD. Dapagliflozin reduces albuminuria in patients with diabetes and hypertension receiving renin-angiotensin blockers. Diabetes Obes Metab. 2016;18(6):590–7.
Kraus BJ, Weir MR, Bakris GL, Mattheus M, Cherney DZI, Sattar N, Heerspink HJL, Ritter I, von Eynatten M, Zinman B, et al. Characterization and implications of the initial estimated glomerular filtration rate ‘dip’ upon sodium-glucose cotransporter-2 inhibition with empagliflozin in the EMPA-REG OUTCOME trial. Kidney Int. 2021;99(3):750–62.
Oshima M, Jardine MJ, Agarwal R, Bakris G, Cannon CP, Charytan DM, de Zeeuw D, Edwards R, Greene T, Levin A, et al. Insights from CREDENCE trial indicate an acute drop in estimated glomerular filtration rate during treatment with canagliflozin with implications for clinical practice. Kidney Int. 2021;99(4):999–1009.
Cherney DZ, Perkins BA, Soleymanlou N, Maione M, Lai V, Lee A, Fagan NM, Woerle HJ, Johansen OE, Broedl UC, von Eynatten M. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation. 2014;129(5):587–97.
Ott C, Jung S, Korn M, Kannenkeril D, Bosch A, Kolwelter J, Striepe K, Bramlage P, Schiffer M, Schmieder RE. Renal hemodynamic effects differ between antidiabetic combination strategies: randomized controlled clinical trial comparing empagliflozin/linagliptin with metformin/insulin glargine. Cardiovasc Diabetol. 2021;20(1):178.
Kidokoro K, Cherney DZI, Bozovic A, Nagasu H, Satoh M, Kanda E, Sasaki T, Kashihara N. Evaluation of glomerular hemodynamic function by Empagliflozin in Diabetic mice using in vivo imaging. Circulation. 2019;140(4):303–15.
van Bommel EJM, Muskiet MHA, van Baar MJB, Tonneijck L, Smits MM, Emanuel AL, Bozovic A, Danser AHJ, Geurts F, Hoorn EJ, et al. The renal hemodynamic effects of the SGLT2 inhibitor dapagliflozin are caused by post-glomerular vasodilatation rather than pre-glomerular vasoconstriction in metformin-treated patients with type 2 diabetes in the randomized, double-blind RED trial. Kidney Int. 2020;97(1):202–12.
Jung S, Bosch A, Kannenkeril D, Karg MV, Striepe K, Bramlage P, Ott C, Schmieder RE. Combination of empagliflozin and linagliptin improves blood pressure and vascular function in type 2 diabetes. Eur Heart J Cardiovasc Pharmacother. 2020;6(6):364–71.
Kolwelter J, Kannenkeril D, Linz P, Jung S, Nagel AM, Bosch A, Ott C, Bramlage P, Nöh L, Schiffer M, et al. The SGLT2 inhibitor empagliflozin reduces tissue sodium content in patients with chronic heart failure: results from a placebo-controlled randomised trial. Clin Res Cardiol. 2023;112(1):134–44.
Striepe K, Jumar A, Ott C, Karg MV, Schneider MP, Kannenkeril D, Schmieder RE. Effects of the selective sodium-glucose cotransporter 2 inhibitor empagliflozin on vascular function and Central Hemodynamics in patients with type 2 diabetes Mellitus. Circulation. 2017;136(12):1167–9.
Mancia Chairperson G, Kreutz Co-Chair R, Brunström M, Burnier M, Grassi G, Januszewicz A, Muiesan ML, Tsioufis K, Agabiti-Rosei E, Algharably EAE et al. 2023 ESH guidelines for the management of arterial hypertension the Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J Hypertens 2023.
Townsend RR, Wilkinson IB, Schiffrin EL, Avolio AP, Chirinos JA, Cockcroft JR, Heffernan KS, Lakatta EG, McEniery CM, Mitchell GF et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66(3):698–722.
Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588–605.
Ben-Shlomo Y, Spears M, Boustred C, May M, Anderson SG, Benjamin EJ, Boutouyrie P, Cameron J, Chen CH, Cruickshank JK, et al. Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects. J Am Coll Cardiol. 2014;63(7):636–46.
Ohkuma T, Ninomiya T, Tomiyama H, Kario K, Hoshide S, Kita Y, Inoguchi T, Maeda Y, Kohara K, Tabara Y, et al. Brachial-ankle pulse Wave Velocity and the risk prediction of Cardiovascular Disease: an Individual Participant Data Meta-Analysis. Hypertension. 2017;69(6):1045–52.
Laurent S, Katsahian S, Fassot C, Tropeano AI, Gautier I, Laloux B, Boutouyrie P. Aortic stiffness is an independent predictor of fatal stroke in essential hypertension. Stroke. 2003;34(5):1203–6.
Sutton-Tyrrell K, Najjar SS, Boudreau RM, Venkitachalam L, Kupelian V, Simonsick EM, Havlik R, Lakatta EG, Spurgeon H, Kritchevsky S, et al. Elevated aortic pulse wave velocity, a marker of arterial stiffness, predicts cardiovascular events in well-functioning older adults. Circulation. 2005;111(25):3384–90.
Vlachopoulos C, Aznaouridis K, Terentes-Printzios D, Ioakeimidis N, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with brachial-ankle elasticity index: a systematic review and meta-analysis. Hypertension. 2012;60(2):556–62.
Cardoso CRL, Salles GF. Prognostic value of changes in aortic stiffness for Cardiovascular outcomes and Mortality in resistant hypertension: a Cohort Study. Hypertension. 2022;79(2):447–56.
O’Brien E, Parati G, Stergiou G, Asmar R, Beilin L, Bilo G, Clement D, de la Sierra A, de Leeuw P, Dolan E, et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31(9):1731–68.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens. 2018;36(10):1953–2041.
Cole BR, Giangiacomo J, Ingelfinger JR, Robson AM. Measurement of renal function without urine collection. A critical evaluation of the constant-infusion technic for determination of inulin and para-aminohippurate. N Engl J Med. 1972;287(22):1109–14.
Munakata M. Brachial-ankle pulse wave velocity in the measurement of arterial stiffness: recent evidence and clinical applications. Curr Hypertens Rev. 2014;10(1):49–57.
Climie RE, Alastruey J, Mayer CC, Schwarz A, Laucyte-Cibulskiene A, Voicehovska J, Bianchini E, Bruno RM, Charlton P, Grillo A et al. Vascular ageing - moving from Bench towards Bedside. Eur J Prev Cardiol 2023.
Cherney DZ, Perkins BA, Soleymanlou N, Har R, Fagan N, Johansen OE, Woerle HJ, von Eynatten M, Broedl UC. The effect of empagliflozin on arterial stiffness and heart rate variability in subjects with uncomplicated type 1 diabetes mellitus. Cardiovasc Diabetol. 2014;13:28.
van Bommel EJM, Smits MM, Ruiter D, Muskiet MHA, Kramer MHH, Nieuwdorp M, Touw DJ, Heerspink HJL, Joles JA, van Raalte DH. Effects of dapagliflozin and gliclazide on the cardiorenal axis in people with type 2 diabetes. J Hypertens. 2020;38(9):1811–9.
Knudsen ST, Bek T, Poulsen PL, Hove MN, Rehling M, Mogensen CE. Macular edema reflects generalized vascular hyperpermeability in type 2 diabetic patients with retinopathy. Diabetes Care. 2002;25(12):2328–34.
Gerstein HC, Mann JF, Yi Q, Zinman B, Dinneen SF, Hoogwerf B, Hallé JP, Young J, Rashkow A, Joyce C, et al. Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA. 2001;286(4):421–6.
Hillege HL, Fidler V, Diercks GF, van Gilst WH, de Zeeuw D, van Veldhuisen DJ, Gans RO, Janssen WM, Grobbee DE, de Jong PE. Urinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general population. Circulation. 2002;106(14):1777–82.
Ng WY, Lui KF, Thai AC. Evaluation of a rapid screening test for microalbuminuria with a spot measurement of urine albumin-creatinine ratio. Ann Acad Med Singap. 2000;29(1):62–5.
Deckert T, Feldt-Rasmussen B, Borch-Johnsen K, Jensen T, Kofoed-Enevoldsen A. Albuminuria reflects widespread vascular damage. The Steno hypothesis. Diabetologia. 1989;32(4):219–26.
Feldt-Rasmussen B. Microalbuminuria, endothelial dysfunction and cardiovascular risk. Diabetes Metab. 2000;26(Suppl 4):64–6.
Pedrinelli R, Giampietro O, Carmassi F, Melillo E, Dell’Omo G, Catapano G, Matteucci E, Talarico L, Morale M, De Negri F, et al. Microalbuminuria and endothelial dysfunction in essential hypertension. Lancet. 1994;344(8914):14–8.
Porrini E, Ruggenenti P, Luis-Lima S, Carrara F, Jiménez A, de Vries APJ, Torres A, Gaspari F, Remuzzi G. Estimated GFR: time for a critical appraisal. Nat Rev Nephrol. 2019;15(3):177–90.
Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, Brunner-La Rocca HP, Choi DJ, Chopra V, Chuquiure-Valenzuela E, et al. Empagliflozin in Heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451–61.
Ott C, Kistner I, Keller M, Friedrich S, Willam C, Bramlage P, Schmieder RE. Effects of linagliptin on renal endothelial function in patients with type 2 diabetes: a randomised clinical trial. Diabetologia. 2016;59(12):2579–87.
Acknowledgements
We gratefully acknowledge the expert technical assistance of Dorothea Bader-Schmieder, Ingrid Fleischmann, Kerstin Fröhlich-Endreß, Ulrike Heinritz, Simone Pejkovic, Wiebke Maurer and Theresa Federlein.
Funding
No funding received.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Merve Günes-Altan collected data, analyzed data and wrote the manuscript.
Agnes Bosch, Kristina Striepe, Mario Schiffer and Peter Bramlage collected data, contributed to the discussion and reviewed the manuscript.
Roland E. Schmieder analyzed data, contributed to the discussion and reviewed/edited the manuscript.
Dennis Kannenkeril collected data, designed the study, analyzed data, contributed to the discussion and reviewed/edited the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from each patient before study inclusion. The study protocol was approved by the Local Ethics Committee (University of Erlangen- Nuremberg), and the studies were conducted in accordance with the Declaration of Helsinki and the principles of good clinical practice guidelines.
Consent for publication
All authors gave full consent for publication.
Competing interests
MGA and other authors except RES declare that they have no conflict of interest with respect to this study. RES has conflict of interests with respect to this study: Boehringer Ingelheim, AstraZeneca (grants to the institution, speaker and adviser bureau).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Günes-Altan, M., Bosch, A., Striepe, K. et al. Is GFR decline induced by SGLT2 inhibitor of clinical importance?. Cardiovasc Diabetol 23, 184 (2024). https://doi.org/10.1186/s12933-024-02223-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02223-0