
Abstract
Background
Diabetes mellitus (DM) is associated with thrombogenicity, clinically manifested with atherothrombotic events after percutaneous cutaneous intervention (PCI). This study aimed to investigate association between DM status and platelet reactivity, and their prognostic implication in PCI-treated patients.
Methods
The Platelet function and genoType-Related long-term Prognosis-Platelet Function Test (PTRG-PFT) cohort was established to determine the linkage of platelet function test (PFT) with long-term prognosis during dual antiplatelet therapy including clopidogrel in patients treated with drug-eluting stent (DES). We assessed platelet reactivity using VerifyNow and ‘high platelet reactivity (HPR)’ was defined as ≥ 252 P2Y12 reaction unit (PRU). Major adverse cardiac and cerebrovascular event (MACCE) was a composite of all-cause death, myocardial infarction, stent thrombosis or stroke.
Results
Between July 2003 and Aug 2018, DES-treated patients with available PFT were enrolled (n = 11,714). Diabetic patients demonstrated significant higher levels of platelet reactivity (DM vs. non-DM: 225.7 ± 77.5 vs. 213.6 ± 79.1 PRU, P < 0.001) and greater prevalence of HPR compared to non-diabetic patients (38.1% vs. 32.0%, P < 0.001). PRU level and prevalence of HPR were significantly associated with insulin requirement and HbA1c level, as well as diabetic status. DM status and HPR phenotype had a similar prognostic implication, which showed the synergistic clinical impact on MACCE. Association between PRU level and MACCE occurrence seemed higher in diabetic vs. non-diabetic patients. In non-DM patients, HPR phenotype did not significantly increase the risk of MACCE (adjusted hazard ratio [HRadj]: 1.073; 95% confidence interval [CI]: 0.869–1.325; P = 0.511), whereas HPR was an independent determinant for MACCE occurrence among diabetic patients (HRadj: 1.507; 95% CI: 1.193–1.902; P < 0.001).
Conclusion
The levels of on-clopidogrel platelet reactivity are determined by diabetic status and the severity of DM. In addition, HPR phenotype significantly increases the risk of MACCE only in diabetic patients.
Clinical trial registration
URL: https://www.clinicaltrials.gov. Unique identifier: NCT04734028.
Similar content being viewed by others


Introduction
Diabetes mellitus (DM) increases the risk of morbidity and mortality due to atherosclerotic cardiovascular disease (ASCVD). Many studies have shown that DM patients without prior ASCVDs are at the same risk for cardiovascular events as patients without diabetes with a history of earlier cardiovascular events [1, 2]. In patients with diabetes, hyperglycemia, insulin resistance, glucose variability, and systemic inflammation directly or indirectly contribute to the pathogenesis of atherosclerosis and lead to micro- and macro-vascular complications [3,4,5,6]. In addition to atherogenicity, DM is clinically manifested by high rate of acute thromboembolic events, including acute myocardial infarction (AMI), stroke and venous thromboembolism [7, 8]. These findings can be related with increased thrombogenicity owing to platelet hyperreactivity, activation of coagulation factors and hypo-fibrinolysis [9, 10].
High platelet reactivity (HPR) phenotype measured by platelet function test (PFT) is a well-established predictor of major cardiovascular events (MACEs) after percutaneous coronary intervention (PCI) [11,12,13]. Platelet reactivity in diabetic patients can increase according to metabolic abnormalities including hyperglycemia [14], insulin resistance/deficiency [15], oxidative stress, and endothelial dysfunction [16, 17]. Moreover, it can impair the responsiveness to antiplatelet therapy [18, 19]. The present study aimed to investigate the association between diabetic conditions and the level of platelet reactivity, and their clinical implication in a large-scale cohort including patients with significant coronary artery disease (CAD).
Methods
Study design and patients
The PTRG-DES (Platelet function and genoType-Related long-term proGnosis in Drug Eluting Stent-treated patients) consortium is an investigator-initiative nationwide multicenter observational registry endorsed by the Korean Society of Interventional Cardiology, specifically designed to determine the relationship between platelet reactivity/genotype and subsequent clinical events in East Asian patients after uneventful drug-eluting stent (DES) implantation [20].
In total, nine prospective registries from 32 Korean academic centers have joined the PTRG-DES consortium, contributing data from 13,160 DES patients treated between July 2003 and August 2018. Consecutive patients who were treated with DES and had been adequately administered both aspirin and clopidogrel were eligible for enrollment, irrespective of patients’ medical conditions or complexity of coronary artery lesions. The major exclusion criteria were the occurrence of a major complication during the procedure, fibrinolytic therapy, and the need for oral anticoagulants. DM was classified by one of the followings: (1) a history of diabetes, regardless of duration of disease, or need for antidiabetic agents; (2) a fasting blood glucose ≥ 126 mg/dl; or (3) glycosylated hemoglobin (HbA1c) ≥ 6.5% [21].
The institutional review board of each participating center approved the registry and waived the requirement for written informed consent for access to an institutional registry. The study was performed in accordance with the Good Clinical Practice Guidelines and the principles of the Declaration of Helsinki.
Platelet function test
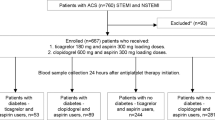
We obtained 11,714 PFT results (PTRG-PFT cohort), in which platelet reactivity was measured after an adequate period to ensure a full antiplatelet effect, using the VerifyNow assay (Accriva, San Diego, CA, USA) [22]. The measurement protocol followed the manufacturer’s recommendations, and the details are described elsewhere [23]. Aspirin was given as either: (1) a coated oral dose of 300 mg for at least 6 h; or (2) a dose of 100 mg at least 5 days before PCI. Clopidogrel was given as either (1) a dose of 600 mg at least 6 h; (2) a dose of 300 mg at least 12 h; or (3) a dose of 75 mg for at least 5 days before PCI. If eptifibatide or tirofiban was used during PCI, a 24-hr washout period was required before VerifyNow testing. No patients receiving abciximab were enrolled because of a long washout period.
The levels of platelet reactivity on clopidogrel and aspirin were reported as ‘P2Y12 reaction unit (PRU)’ and ‘aspirin reaction unit (ARU)’, respectively. We assessed PRUs as continuous and categorical measures. Additionally, the cutoffs of ‘HPR to ADP’ and ‘HPR to arachidonic acid (AA)’ were defined as ‘≥ 252 PRU’ and ‘≥ 414 ARU’ according to our previous report [20].
Clinical outcomes
The primary endpoint was the occurrence of major adverse cardiac and cerebrovascular events (MACCE) including all-cause death, myocardial infarction (MI), definite stent thrombosis (ST) or stroke for 5 years post-PCI. In addition, major bleeding was defined as Bleeding Academic Research Consortium (BARC) bleeding type 3–5 [24].
All deaths were considered to be due to cardiovascular (CV) cause unless a definite non-CV cause could be established. AMI was defined as increased cardiac troponin values with ischemic symptoms or ischemic changes on electrocardiogram or imaging evidence of recent loss of viable myocardium or new regional wall motion abnormalities that were not related to the procedure [25]. Stroke included any new embolic, thrombotic, or hemorrhagic stroke events with neurologic deficits that persisted for at least 24 h. An independent clinical event committee masked to the VerifyNow results adjudicated all clinical events using the original source documents.
Statistical analysis
The Kolmogorov–Smirnov test was performed to analyze the normal distribution of continuous variables. Continuous variables were expressed as mean ± standard deviation (SD) or as median [interquartile range (IQR)], while categorical variables were presented as absolute numbers and frequencies (%). Student’s unpaired t-test and the Mann-Whitney U test were used for evaluating the parametric and the non-parametric continuous variables, respectively. Categorical variables were compared using the Pearson chi-square test or Fisher’s exact test when the Cochran rule was not met. Univariate and multivariate Cox proportional hazard analyses were performed to identify proportional hazard risk for clinical events according to DM status and/or HPR phenotype. To adjust for potential confounders (age, sex, body mass index, index MI presentation, hypertension, dyslipidemia, smoking, DM, chronic kidney disease [CKD], anemia, congestive heart failure, previous PCI, previous stroke, multivessel disease, PCI for left main or left anterior descending artery, and DES generation), variables with P < 0.1 in univariate analysis were then entered into multivariate logistic augmented backwards regression analysis providing odds ratio (OR) and 95% confidence intervals (CIs). Statistical significance was set at P- value < 0.05. All statistical analyses were performed using IBM/SPSSv24.0 (IBM/SPSS, Chicago, IL, USA) and RStudio (Integrated Development Environment for R. RStudio, PBC, Boston, MA, USA).
Results
Baseline characteristics of the study population
From the PTRG-PFT cohort (n = 11,714), the level of platelet reactivity was 217.8 ± 78.7 PRU and prevalence of HPR (≥ 252 PRU) was 34.2% (n = 4,001). Approximately 35% of patients (n = 4,057) had diabetes (Supplement Fig. 1). Table 1 showed the baseline characteristics according to the presence of DM. Compared to non-diabetic patients, diabetic patients were older (DM vs. non-DM: 65.5 ± 10.0 vs. 63.8 ± 11.3, P < 0.001), the proportion of female was higher (34.8% vs. 30.7%, P < 0.001), and the prevalence of hypertension (70.9% vs. 54.5%, P < 0.001) and hyperlipidemia (65.9% vs. 63.7%, P = 0.019) was higher, while the proportion of current smokers was lower (25.7% vs. 29.3%, P < 0.001).

Distribution of PRU according to DM status
DM: diabetes mellitus; PRU: P2Y12 reaction unit
Platelet reactivity and prevalence of HPR according to diabetic condition
The levels of platelet reactivity in diabetic patients were significantly higher than that of non-diabetic patients (DM vs. non-DM: 225.7 ± 77.5 vs. 213.6 ± 79.1 PRU, P < 0.001 and 448.2 ± 72.3 vs. 442.1 ± 67.7 ARU, P < 0.001) (Fig. 1; Table 2). In addition, prevalence of HPR to ADP phenotype was higher in DM patients compared with non-DM subjects (HPR to ADP: 38.1% vs. 32.0%, P < 0.001 and HPR to AA: 53.7% vs. 51.6%, P = 0.090). Even for the diabetic patients, the levels of platelet reactivity and prevalence of HPR phenotypes varied depending on the need for insulin (Table 2); DM patients on insulin (N = 270, 6.7% of DM patients) showed the highest levels of platelet reactivity compared with other groups (DM on insulin vs. DM without insulin vs. non-DM: 44.0% vs. 37.7% vs. 32.0%, P < 0.001) Furthermore, we divided enrolled patients into the three groups according to on-admission HbA1c level (available data: n = 4,095); HbA1c < 6.5% (n = 2,541, 62.1%), 6.5–8.5% (n = 1,192, 29.1%) and > 8.5% (n = 362, 8.8%). HbA1c level showed the weak positive relationship with levels of platelet reactivity (vs. PRU: r = 0.065, P < 0.001 and vs. ARU: r = 0.049, P = 0.101, respectively) (Supplement Fig. 2). Therefore, PRU level proportionally increased across the HbA1c group (216.1 ± 82.2 vs. 226.8 ± 81.6 vs. 229.4 ± 81.4 PRU, P < 0.001). The risk of HPR increased with a significant correlation with HbA1c between HbA1c 6.5% and 8.5%, while there was no significant increase in the HPR risk below 6.5% and above 8.5%.

Kaplan–Meier curves of MACCE and major bleeding rate according to diabetic condition. A 5-year MACCE with and without DM; B 5-year MACCE according to index Hb A1c; C 5-year major bleeding with and without DM; D 5-year major bleeding according to index Hb A1c
Hb A1c: hemoglobin A1c; MACCE: major cardiac and cerebrovascular event
Prognostic impact of platelet reactivity according to diabetic condition
During the median follow-up of 37.6 months (IQR, 12.0–60.8), a total of 709 MACCEs (6.1%) (392 deaths [3.3%], 172 non-fatal MI [1.5%], 62 ST [0.5%] and 181 non-fatal stroke [1.5%]), and 324 cases of major bleeding (2.8%) occurred. During 5-year follow-up, the MACCE rate in diabetic patients was higher than that in non-diabetic patients (7.7% vs. 5.2%, unadjusted hazard ratio [HR] 1.418, 95% CI: 1.233–1.645, P < 0.001), and the index HbA1c levels were also related with the risk of MACCE (Fig. 2A and B). The rate of major bleeding was also higher in DM patients (3.4% vs. 2.4%, unadjusted HR 1.370, 95% CI: 1.100-1.708, P = 0.005) (Fig. 2C and D).
Figure 3 showed relative HR for MACCE occurrence according to PRU level. Among the total cohort, the cutoff of platelet reactivity for increasing the risk of MACCE was observed around HPR (PRU ≥ 252). Association between PRU level and MACCE occurrence appeared closer in DM patients compared with non-DM subjects. The cutoff of PRU for MACCE occurrence seemed to be similar between the groups.

Relative hazard ratio for MACCE according to PRU level by restricted cubic spline curve. A all patients; B non-diabetic patients; C diabetic patients
MACCE: major cardiac and cerebrovascular event; PRU: P2Y12 reaction unit
Prognostic impact of HPR phenotype according to diabetic condition
We categorized patients into the four groups according to presence of DM and HPR phenotype. Both DM and HPR phenotype showed the similar prognostic implication in terms with MACCE occurrence. Figure 4 shows that the highest rates of MACCE and all-cause death were found in DM patients with HPR compared with other groups (vs. non-DM without HPR: unadjusted hazard ratio [HR]: 2.102; 95% CI: 1.723–2.564; P < 0.001). In multivariable analysis, only DM phenotype with HPR significantly increased the risk of MACCE compared to non-DM phenotype without HPR (HR: 1.607; 95% CI: 1.301–1.984; P < 0.001) (Table 3).

Kaplan–Meier curves according to presence of DM and HPR phenotype. A MACCE; B all-cause death; C major bleeding
DM: diabetes mellitus; HPR: high platelet reactivity; HR: hazard ratio; MACCE: major cardiac and cerebrovascular event
We evaluated prognostic impact of HPR according to DM status. In non-DM patients, HPR phenotype did not significantly increase the risk of MACCE (adjusted HR [HRadj]: 1.073; 95% CI: 0.869–1.325; P = 0.511), whereas HPR was an independent determinant for MACCE occurrence among diabetic subjects (HRadj: 1.507; 95% CI: 1.193–1.902; P < 0.001) (Supplement Table 1). In terms with all-cause death, HPR phenotype was significantly associated with the increased risk only in DM patients (HRadj: 1.805; 95% CI: 1.316–2.476; P < 0.001), but not in non-DM subjects (HRadj: 1.082; 95% CI: 0.818–1.430; P = 0.582). HPR phenotype significantly increased the risk of stent thrombosis irrespective of DM status (DM: HRadj, 2.956; 95% CI, 1.280–6.825; P = 0.011 and non-DM: HRadj, 3.259; 95% CI, 1.630–6.515; P < 0.001) (Pinteraction = 0.869). However, there were no differences in the risk of major bleeding across the groups.
Discussion
This study investigated the most extensive clinical data to evaluate the long-term prognostic impact of platelet reactivity according to DM status in CAD patients undergoing DES implantation. The major findings were as below: (1) platelet reactivity during clopidogrel treatment was higher in patients with diabetes than those without diabetes, which was related with insulin treatment and the severity of DM (HbA1c level); (2) HPR enhanced the risks of MACCE and all-cause death, which association appeared significant only in diabetic patients; (3) the risk of major bleeding was not associated with HPR phenotype; and (4) prognostic implication of diabetic status and HPR phenotype appeared similar, and its association showed the synergistic effect on MACCE rate.
DM itself is a well-established risk factor for CV events in patients undergoing PCI. The major pathophysiology of CV events is associated with its atherogenicity, and increased thrombogenicity in diabetic patients is associated with worse clinical outcomes. In addition, DM status has been associated with the level of platelet reactivity and the prevalence of HPR. Their platelets have dysregulated signaling pathways, that lead to a hyperreactive phenotype with enhanced adhesion, aggregation, and activity [26]. Hyperglycemia can increase platelet reactivity by inducing non-enzymatic glycation of proteins on the surface of the platelets. Such glycation decreases membrane fluidity and increases the propensity for platelets activation [14]. Insulin antagonizes the effect of platelet agonists such as collagen, ADP, epinephrine, and platelet-activating factor, which can induce high platelet reactivity [15]. Superoxide may increase platelet reactivity by enhancing intraplatelet release of calcium after activation and limiting the biological activity of nitric oxide (NO) [27, 28] Endothelial dysfunction also increases platelet reactivity by decreased production and the effect of NO and prostacyclin [17]. Because of these pathologic changes, responsiveness to P2Y12 inhibitor was decreased [29, 30] Our data showed that the level of platelet reactivity (i.e., PRU) was correlated with HbA1c level and the proportion of HPR increased according to HbA1c level. In other words, not only presence of diabetes, but also diabetic condition (e.g., HbA1c level or insulin treatment) affected platelet reactivity during P2Y12 inhibitor therapy. Therefore, strict control of diabetic condition (i.e., HbA1c < 6.5%) may affect the effect of antiplatelet regimens and decrease the rate of HPR, which may be related with a better clinical outcome in DES-treated patients.
HPR on antiplatelet therapy is a well-validated risk factor of ischemic events in patients undergoing PCI [13, 31,32,33]. The optimal cut-off values for HPR are different between the East Asian and Western populations, and it is known already that PRU values are higher in East Asian populations (218 PRU in PTRG-DES vs. 188 PRU in ADAPT-DES during clopidogrel treatment) [20, 31]. Although the distribution of PRU was shifted to the right side, the ischemic events rate after PCI was known to be lower in East Asians than Westerners. This was known as “East Asian Paradox” [34]. The present study already validated this concept by presenting ≥ 252 PRU as an optimal cut-off of HPR using time-dependent ROC curve analysis. It is quite higher than 208 PRU, which was suggested in Western population [12, 31]. The PRU values of diabetic patients were higher than those of non-diabetic patients, and PRU values gradually increased according to the severity of DM. In terms of clinical outcomes, this study showed that HPR and DM had a combined prognostic implication following DES implantation. Based on the change of the platelet reactivity in patients with diabetes, the clinical studies of potent P2Y12 inhibitor such as prasugrel [35] and ticagrelor [36] showed a favorable outcome following PCI in diabetic patients. It is interesting to note that in non-DM patients, although the incidence of MACCE is numerically higher in the HPR group, there is no statistically significant difference. This might be because the non-DM group, having fewer co-morbidities, presented fewer events, thus not showing a statistical distinction. Considering that diabetes itself is a strong risk factor for CV events after PCI, the risk of HPR for MACCE occurrence is also quite high even in East Asian patients. Choice of potent P2Y12 inhibitor can be more preferred in DM patients with poorly controlled glucose level or on insulin treatment.
This study had several limitations. First, the PTRG-DES consortium excluded patients treated with potent P2Y12 inhibitors. An added advantage could be that all patients were treated with the same drug (clopidogrel). As a result, it can guarantee the homogeneity of the study population. However, the resulting disadvantage is that the difference in the effect of potent P2Y12 inhibitor therapy for diabetic patients with HPR cannot be evaluated. Second, to assess the status of DM, detailed data on the degree of control, duration, type of medications, and the presence of diabetic complications are essential. Due to the limitations of a large cohort study, we cannot obtain detailed DM-related data for individual patients. However, we believe that HbA1c levels and insulin treatment are appropriate indicators of DM control and long-standing DM at the time of PFT. Finally, platelet function test and HbA1c level were assessed with each other at a single time-point measurement. Platelet reactivity can change according to the phase and may be linked with the status of glycemic control.
Conclusions
This analysis from the PTRG-DES consortium including a large-scale East Asian patients demonstrated that glucose control affected the level of platelet reactivity during clopidogrel treatment. HPR phenotype and DM status showed the similar prognostic implication after DES implantation, and HPR was significantly associated with ischemic risk only in diabetic patients.
Data Availability
PTRG-PFT data sets are not publicly available because of data protection agreements but can be available from the corresponding author on reasonable request.
Abbreviations
- AA:
-
Arachidonic acid
- AMI:
-
Acute myocardial infarction
- ARU:
-
Aspirin reaction units
- ASCVD:
-
Atherosclerotic cardiovascular disease
- BARC:
-
Bleeding Academic Research Consortium
- CAD:
-
Coronary artery disease
- CKD:
-
Chronic kidney disease
- CI:
-
Confidence intervals
- CV:
-
Cardiovascular
- DES:
-
Drug-eluting stent
- DM:
-
Diabetes mellitus
- Hb:
-
Hemoglobin
- HPR:
-
High platelet reactivity
- HR:
-
Hazard ratio
- IQR:
-
Interquartile range
- MACCE:
-
Major adverse cardiac and cerebrovascular events (MACCE)
- MACE:
-
Major cardiovascular event
- MI:
-
Myocardial infarction
- NO:
-
Nitric oxide
- OR:
-
Odds ratio
- PCI:
-
Percutaneous coronary intervention
- PFT:
-
Platelet function test
- PRU:
-
P2Y12 reaction unit
- SD:
-
Standard deviation
- ST:
-
Stent thrombosis
References
Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339:229–34.
Schramm TK, Gislason GH, Kober L, Rasmussen S, Rasmussen JN, Abildstrom SZ, et al. Diabetes patients requiring glucose-lowering therapy and nondiabetics with a prior myocardial infarction carry the same cardiovascular risk: a population study of 3.3 million people. Circulation. 2008;117:1945–54.
American Diabetes A. 9. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018;41:S86-S104.
O’Keefe JH, Bell DS. Postprandial hyperglycemia/hyperlipidemia (postprandial dysmetabolism) is a cardiovascular risk factor. Am J Cardiol. 2007;100:899–904.
DeFronzo RA. Insulin resistance, lipotoxicity, type 2 diabetes and atherosclerosis: the missing links. The Claude Bernard Lecture 2009 Diabetologia. 2010;53:1270–87.
Intensive blood-glucose. Control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK prospective diabetes study (UKPDS) Group. Lancet. 1998;352:837–53.
Furie B, Furie BC. Mechanisms of thrombus formation. N Engl J Med. 2008;359:938–49.
Gariani K, Mavrakanas T, Combescure C, Perrier A, Marti C. Is diabetes mellitus a risk factor for venous thromboembolism? A systematic review and meta-analysis of case-control and cohort studies. Eur J Intern Med. 2016;28:52–8.
Colwell JA, Nesto RW. The platelet in diabetes: focus on prevention of ischemic events. Diabetes Care. 2003;26:2181–8.
Boden G, Vaidyula VR, Homko C, Cheung P, Rao AK. Circulating tissue factor procoagulant activity and thrombin generation in patients with type 2 diabetes: effects of insulin and glucose. J Clin Endocrinol Metab. 2007;92:4352–8.
Gurbel PA, Bliden KP, Samara W, Yoho JA, Hayes K, Fissha MZ, et al. Clopidogrel effect on platelet reactivity in patients with stent thrombosis: results of the CREST Study. J Am Coll Cardiol. 2005;46:1827–32.
Price MJ, Angiolillo DJ, Teirstein PS, Lillie E, Manoukian SV, Berger PB, et al. Platelet reactivity and cardiovascular outcomes after percutaneous coronary intervention: a time-dependent analysis of the gauging responsiveness with a VerifyNow P2Y12 assay: impact on thrombosis and safety (GRAVITAS) trial. Circulation. 2011;124:1132–7.
Park KW, Jeon KH, Kang SH, Oh IY, Cho HJ, Lee HY, et al. Clinical outcomes of high on-treatment platelet reactivity in Koreans receiving elective percutaneous coronary intervention (from results of the CROSS VERIFY study). Am J Cardiol. 2011;108:1556–63.
Winocour PD, Watala C, Kinglough-Rathbone RL. Membrane fluidity is related to the extent of glycation of proteins, but not to alterations in the cholesterol to phospholipid molar ratio in isolated platelet membranes from diabetic and control subjects. Thromb Haemost. 1992;67:567–71.
Westerbacka J, Yki-Jarvinen H, Turpeinen A, Rissanen A, Vehkavaara S, Syrjala M, et al. Inhibition of platelet-collagen interaction: an in vivo action of insulin abolished by insulin resistance in obesity. Arterioscler Thromb Vasc Biol. 2002;22:167–72.
Spinetti G, Kraenkel N, Emanueli C, Madeddu P. Diabetes and vessel wall remodelling: from mechanistic insights to regenerative therapies. Cardiovasc Res. 2008;78:265–73.
Schafer A, Bauersachs J. Endothelial dysfunction, impaired endogenous platelet inhibition and platelet activation in diabetes and atherosclerosis. Curr Vasc Pharmacol. 2008;6:52–60.
Schneider DJ. Factors contributing to increased platelet reactivity in people with diabetes. Diabetes Care. 2009;32:525–7.
Angiolillo DJ, Bernardo E, Sabate M, Jimenez-Quevedo P, Costa MA, Palazuelos J, et al. Impact of platelet reactivity on cardiovascular outcomes in patients with type 2 diabetes mellitus and coronary artery disease. J Am Coll Cardiol. 2007;50:1541–7.
Her AY, Jeong YH, Kim BK, Joo HJ, Chang K, Park Y, et al. Platelet function and genotype after DES Implantation in East Asian Patients: Rationale and characteristics of the PTRG-DES Consortium. Yonsei Med J. 2022;63:413–21.
ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 2. Classification and diagnosis of diabetes: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46:19–S40.
Sibbing D, Aradi D, Alexopoulos D, Ten Berg J, Bhatt DL, Bonello L, et al. Updated Expert Consensus Statement on platelet function and genetic testing for guiding P2Y12 receptor inhibitor treatment in percutaneous coronary intervention. JACC Cardiovasc Interv. 2019;12:1521–37.
Jeong YH, Bliden KP, Antonino MJ, Park KS, Tantry US, Gurbel PA. Usefulness of the VerifyNow P2Y12 assay to evaluate the antiplatelet effects of ticagrelor and clopidogrel therapies. Am Heart J. 2012;164:35–42.
Mehran R, Rao SV, Bhatt DL, Gibson CM, Caixeta A, Eikelboom J, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the bleeding Academic Research Consortium. Circulation. 2011;123:2736–47.
Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Executive Group on behalf of the joint european Society of Cardiology /American College of Cardiology /American Heart Association /World Heart Federation Task Force for the Universal Definition of Myocardial I. Fourth Universal Definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72:2231–64.
Davi G, Patrono C. Platelet activation and atherothrombosis. N Engl J Med. 2007;357:2482–94.
Schaeffer G, Wascher TC, Kostner GM, Graier WF. Alterations in platelet Ca2 + signalling in diabetic patients is due to increased formation of superoxide anions and reduced nitric oxide production. Diabetologia. 1999;42:167–76.
Freedman JE. Oxidative stress and platelets. Arterioscler Thromb Vasc Biol. 2008;28:11–6.
Angiolillo DJ, Jakubowski JA, Ferreiro JL, Tello-Montoliu A, Rollini F, Franchi F, et al. Impaired responsiveness to the platelet P2Y12 receptor antagonist clopidogrel in patients with type 2 diabetes and coronary artery disease. J Am Coll Cardiol. 2014;64:1005–14.
Angiolillo DJ, Bernardo E, Ramirez C, Costa MA, Sabate M, Jimenez-Quevedo P, et al. Insulin therapy is associated with platelet dysfunction in patients with type 2 diabetes mellitus on dual oral antiplatelet treatment. J Am Coll Cardiol. 2006;48:298–304.
Stone GW, Witzenbichler B, Weisz G, Rinaldi MJ, Neumann FJ, Metzger DC, et al. Platelet reactivity and clinical outcomes after coronary artery implantation of drug-eluting stents (ADAPT-DES): a prospective multicentre registry study. Lancet. 2013;382:614–23.
Brar SS, ten Berg J, Marcucci R, Price MJ, Valgimigli M, Kim HS, et al. Impact of platelet reactivity on clinical outcomes after percutaneous coronary intervention. A collaborative meta-analysis of individual participant data. J Am Coll Cardiol. 2011;58:1945–54.
Suh JW, Lee SP, Park KW, Lee HY, Kang HJ, Koo BK, et al. Multicenter randomized trial evaluating the efficacy of cilostazol on ischemic vascular complications after drug-eluting stent implantation for coronary heart disease: results of the CILON-T (influence of CILostazol-based triple antiplatelet therapy ON ischemic complication after drug-eluting stenT implantation) trial. J Am Coll Cardiol. 2011;57:280–9.
Kang J, Park KW, Palmerini T, Stone GW, Lee MS, Colombo A, et al. Racial differences in Ischaemia/Bleeding Risk Trade-Off during Anti-Platelet Therapy: individual patient Level Landmark Meta-Analysis from seven RCTs. Thromb Haemost. 2019;119:149–62.
Wiviott SD, Braunwald E, Angiolillo DJ, Meisel S, Dalby AJ, Verheugt FW, et al. Greater clinical benefit of more intensive oral antiplatelet therapy with prasugrel in patients with diabetes mellitus in the trial to assess improvement in therapeutic outcomes by optimizing platelet inhibition with prasugrel-thrombolysis in myocardial infarction 38. Circulation. 2008;118:1626–36.
James S, Angiolillo DJ, Cornel JH, Erlinge D, Husted S, Kontny F, et al. Ticagrelor vs. clopidogrel in patients with acute coronary syndromes and diabetes: a substudy from the PLATelet inhibition and patient outcomes (PLATO) trial. Eur Heart J. 2010;31:3006–16.
Acknowledgements
The study was designed by the principal investigator and executive committee and was sponsored by the Platelet-Thrombosis Research Group under the Korean Society of Intervention Cardiology.
Funding
This study was sponsored by the Platelet-Thrombosis Research Group under the Korean Society of Intervention Cardiology.
Author information
Authors and Affiliations
Consortia
Contributions
KHJ and JWS: Study design, collection of data, statistical analyses, drafting of the manuscript. BKK, HJJ, KC, YP, YBS, SGA, SYL. JRC, AYH, HSK, MHK, DSL, ESS: Collection of data, statistical analyses. YHJ, IHC, JWS: Study conception and design, critical revision for important intellectual content and final approval of the submitted manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The institutional review board of each participating center approved the registry and waived the requirement for written informed consent for access to an institutional registry. The study was performed in accordance with the Good Clinical Practice Guidelines and the principles of the Declaration of Helsinki.
Consent for publication
All authors approved submission of the paper.
Competing interests
Dr. Jeong has received honoraria for lectures from AstraZeneca, Daiichi Sankyo, Sanofi-Aventis, Han-mi Pharmaceuticals, and Yuhan Pharmaceuticals, as well as research grants or support from Yuhan Pharmaceuticals and U&I Corporation. Dr. Song has received honoraria for lectures from AstraZeneca, Daiichi Sankyo, Sanofi-Aventis, Bayer Korea, and Samjin Pharmaceutical. Dr. Joo has received honoraria for lectures from AstraZeneca, Hanmi, Samjin, Dong-A, HK inno. N Pharmaceuticals, and DIO Medical Ltd. The other authors have no potential conflicts of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jeon, KH., Jeong, YH., Chae, IH. et al. Implication of diabetic status on platelet reactivity and clinical outcomes after drug-eluting stent implantation: results from the PTRG-DES consortium. Cardiovasc Diabetol 22, 245 (2023). https://doi.org/10.1186/s12933-023-01976-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-01976-4