
Abstract
Background
Hemoglobin A1C (HbA1c) is a form of glycated hemoglobin used to estimate glycemic control in diabetic patients. Data regarding the prognostic significance of HbA1c levels in contemporary intensive cardiac care unit (ICCU) patients is limited.
Methods
All patients admitted to the ICCU at a tertiary care medical center between January 1, 2020, and June 30, 2021, with documented admission HbA1c levels were included in the study. Patients were divided into 3 groups according to their HbA1c levels: < 5.7 g% [no diabetes mellitus (DM)], 5.7–6.4 g% (pre-DM), ≥ 6.5 g% (DM).
Results
A total of 1412 patients were included. Of them, 974 (69%) were male with a mean age of 67(± 15.7) years old. HbA1c level < 5.7 g% was found in 550 (39%) patients, 5.7–6.4 g% in 458 (32.4%) patients and ≥ 6.5 g% in 404 (28.6%) patients. Among patients who did not know they had DM, 81 (9.3%) patients had high HbA1c levels (≥ 6.5 g%) on admission. The crude mortality rate at follow-up (up to 1.5 years) was almost twice as high among patients with pre-DM and DM than in patients with no DM (10.6% vs. 5.4%, respectively, p = 0.01). Interestingly, although not statistically significant, the trend was that pre-DM patients had the strongest association with mortality rate [HR 1.83, (95% CI 0.936–3.588); p = 0.077].
Conclusions
Although an HbA1c level of ≥ 5.7 g% (pre-DM & DM) is associated with a worse prognosis in patients admitted to ICCU, pre-DM patients, paradoxically, have the highest risk for short and long-term mortality rates.
Similar content being viewed by others

Background
Type 2 diabetes mellitus (DM) is a known risk factor for cardiovascular diseases [1], and patients with DM and cardiovascular disease suffer from higher morbidity and mortality as compared with non-diabetic patients [2,3,4]. Moreover, studies have shown a progressive relationship between plasma glucose levels and cardiovascular risk, and even pre-DM patients are at increased risk for cardiovascular diseases [5]. Also, in patients hospitalized due to acute coronary syndrome (ACS), a higher plasma glucose level at admission is associated with higher mortality risk. This association is seen both in patients with and without a diagnosis of DM [6, 7].
Glycated hemoglobin A1c (HbA1c), the major fraction of glycated hemoglobin, is formed by irreversible non-enzymatic glycation. Its concentration depends only on the red blood cell life span and blood glucose level [8]. Thus, it is an indicator for blood glucose concentrations in the preceding 2–3 months. It is of great significance for monitoring the regulation of diabetes and the risk for complications. Furthermore, the American Diabetes Association (ADA) and World Health Organization (WHO) recommend using HbA1c for the diagnosis of DM [9, 10].
Data regarding HbA1c and outcomes in contemporary intensive coronary care units (ICCUs) is limited. An observational study performed in a medical intensive care unit (MICU) found that HbA1c testing in patients with stress hyperglycemia during hospitalization reveals undiagnosed diabetes in 14% of patients. Moreover, hyperglycemia with lower baseline HbA1c was associated with increased mortality as well [11]. Furthermore, in patients with ACS, acute glycemic control, as estimated by plasma glucose levels, rather than the chronic pre-existing glycemic state as estimated by HbA1c affects prognosis [12, 13]. Hence, we aimed to investigate the prognostic significance of admission HbA1c levels among contemporary ICCU patients in a tertiary care medical center.
Methods
Study population
We performed a prospective single-center observational cohort study at the Shaare Zedek Medical Center, a tertiary referral hospital and one of the 2 largest medical centers in Jerusalem. The study population consisted of non-selected consecutive patients admitted to the ICCU between 1 January 2020 and 30 June 2021. We included only patients for whom HbA1c levels on admission were documented. Patients were divided into 3 groups according to their HbA1c levels: < 5.7 g% [no diabetes mellitus (no-DM)], 5.7–6.4 g% (pre-DM) and ≥ 6.5 g% (DM). The division into groups was done according to the position paper of the ADA: Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2019 [10]. Obesity was defined by a body mass index (BMI) > 30. Demographic data, comorbid conditions, medications, physical examination, laboratory findings, in-hospital complications, length of stay (LOS), and in-hospital mortality were systematically recorded. In-hospital complications were defined as the occurrence of acute heart failure, left ventricular thrombus, shock, recurrent myocardial infarction or stent thrombosis, malignant arrhythmias, mechanical complication (free wall rupture or ventricular septal rupture), acute renal failure, severe bleeding requiring blood transfusion, vascular complication, cerebrovascular accident, anoxic brain damage and sepsis.
Study outcomes
The primary outcome of our study was overall mortality, with a follow-up of up to 1.5-year from the time of index hospitalization. Every death in Israel is documented in a central database of the Israeli Ministry of the Internal Affairs and is updated in the hospitals’ medical records. We used these records to examine the overall mortality rates among the study participants. The study’s secondary outcomes included: (a) comparison of patients’ characteristics among the different HbA1c levels; and (b) in-hospital interventions and complications during the index hospitalization among the different HbA1c levels.
Statistical methods
Patients’ characteristics were presented as numbers (%) for categorical variables and as means (SD) or medians (IQR) for normal and non-normal distributed continuous variables, respectively.
A chi-square test was used for the comparison of categorical variables. Analysis of variance (ANOVA) test and Kruskal–Wallis test were performed for comparison of normally and non-normally distributed continuous variables, respectively. For the post-hoc analyses, we used the Bonferroni correction method.
Hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) for the association between the HbA1c group and mortality were estimated using a Cox proportional-hazards model. The model included the following potential confounders: age, gender, hypertension, hyperlipidemia, diabetes mellitus diagnosis, in-hospital complication, prior intervention, heart failure, and chronic kidney disease. Data were censored at death or at the end of the study period. Kaplan Meier survival curves were compared using the log-rank test. Then, the pre-DM and DM were grouped together and the same analyses were performed.
All tests were conducted with a two-sided overall 5% significance level (α = 0.05). All analyses were performed using R software (R Development Core Team, version 4.0.3, Vienna, Austria).
Results
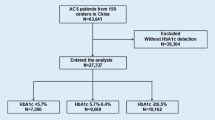
A total of 1739 patients were included in the study. HbA1c on admission was documented in 1412 (81%) patients. Of them, 550 (39%) patients were defined as no-DM, 458 (32.4%) were defined as pre-DM and 404 (28.6%) were defined as DM patients (Table 1).
Interestingly, 81/870 (9.3%) patients had high HbA1c levels ≥ 6.5 g% on admission, but did not know they had DM.
Patients characteristics
Patients in the no-DM group were younger as compared with patients in the other groups [mean age 63.6 (95% CI 62.1–65.1) vs. 70.3 (95% CI 69.1–71.6) in the pre-DM group and 68.6 (95% CI 67.5–69.8) in the DM group; p < 0.001]. The percentage of patients in the pre-DM group increased with patients' age, while for the DM group, it peaks in the seventh decade of life and was then declines (Fig. 1). A higher proportion of men was observed in the DM group as compared with the no-DM and pre-DM groups (74% vs. 66.9% and 67%, respectively; p = 0.035). Obesity rates were higher in the pre-DM (34.1%) and DM (34.9%) groups vs. the no-DM group (24.5%) (p < 0.001). Lastly, patients in the pre-DM and DM groups had higher rates of hypertension, hyperlipidemia, chronic kidney disease, coronary artery disease, heart failure and cardiomyopathy, pulmonary hypertension, atrial fibrillation/flutter, cerebrovascular disease and peripheral artery disease as seen in Table 1.

Percentage of patients in the diabetes mellitus (DM) groups stratified by age
In-hospital complications and mortality rates
Iֹn-hospital complications rates were similar between the groups (32.6% in the no-DM group vs. 28.0%, and 26.9% in the pre-DM and DM group, respectively; p = 0.313) (Table 2). Crude in-hospital mortality rates were higher in the pre-DM and DM groups as compared with the no-DM group (3.7% and 3.0% vs. 1.5%, respectively; p = 0.072). The combined group of pre-DM and DM patients had a higher crude mortality rate when compared with no-DM patients (12.6% versus 8.2%; p = 0.01).
Follow-up mortality rate
The mortality rates during the follow-up period were 8.2% in the no-DM group vs. 12.5% and 12.8% in the pre-DM and DM group, respectively (p = 0.035). Interestingly, although in a multivariate analysis, pre-DM and DM states were associated with higher mortality rates [HR 1.84, (95% CI 0.81–2.97); p = 0.184], the Pre-DM patients had the strongest association with mortality rate [HR 1.83, (95% CI 0.936–3.588); p = 0.077]. (Tables 3 and 4; Figs. 2 and 3). Other factors found to be independently associated with mortality were: age; a history of heart failure; structural heart disease and valvular disease, and in-hospital complications (Table 3).

Kaplan–Meier plot for mortality by HbA1c group assignment

Kaplan–Meier plot for mortality by HbA1c group assignment. Pre-DM and DM are grouped together. DM, diabetes mellitus
Discussion
In this large prospective trial in a tertiary care medical center ICCU, the prevalence of pre-DM (32.4%) and DM (28.6%) patients were similar to several other studies involving cardiac and ICCU patients [14, 15]. Around 9% of patients with no previous diagnosis of DM had HbA1c levels on admission in the diabetic range. Our data show that in non-selected consecutive ICCU patients the highest risk for in-hospital and overall mortality rate is among the pre-DM and DM subgroups. Surprisingly, we found that the highest mortality risk tends to be among patients with pre-DM and not in the patients with DM.
Pre-DM is an intermediate stage of glycemic control with glycemic parameters above normal but below the diabetes threshold. It is a state with a high risk of conversion to overt DM (5–10% per year) and is associated with various complications of DM, including cardiovascular complications [16]. A recent meta-analysis including more than 10-million individuals has shown that a pre-DM state is associated with an increased risk of all-cause mortality and cardiovascular disease in the general population and in patients with atherosclerotic cardiovascular disease [17]. However, despite the association between pre-DM and adverse cardiovascular outcomes, the recommended treatment remains focused on changing lifestyles and only suggests considering pharmacotherapy with metformin. This is in contrast to the given medical treatment and growing use of newer anti-glycemic treatments, such as sodium-glucose co-transporter-2 (SGLT2) inhibitors and glucagon-like peptide-1 (GLP1) agonists in patients with overt DM.
The pre-DM paradox, in which the highest mortality risk tends to be among patients with pre-DM, is consistent with data presented in a number of recent studies. Yahyavi et al. showed that among ambulatory patients, the 12-month risk of major adverse cardiovascular events was highest in subjects with HbA1c just below the diagnostic threshold for diabetes—the pre-DM patients [18]. They found an adjusted hazard ratio of 2.53 in the pre-DM group as compared with 2.46 in the DM group. Importantly, they also found a lower cumulative incidence of initiation of cardioprotective and glucose-lowering medications among patients just below the diagnostic threshold for DM, as compared with patients with a DM diagnosis. This might explain why those patients are at increased risk for mortality. They are less likely to receive self-management and lifestyle modification education compared with DM patients. These findings will mainly affect the long-term prognosis, as in our study. However, several other trials have shown similar findings with regard to the short-term prognosis, among a diverse group of patients. Kim et al. have found that pre-DM condition, unlike DM, was a significant predictor of short-term neurological outcomes and in-hospital mortality among patients with acute ischemic stroke [15]. It should be mentioned that in this study, the initial glucose measurement was higher in the DM group as compared with the pre-DM and normoglycemic groups. Hence, the higher complication rate cannot be attributed to stress hyperglycemia as demonstrated in previous studies [12]. This study also shows that pre-DM patients had a significantly lower rate of preadmission statin treatment (19.3% vs. 30%) and also lower rates of antiplatelet treatment. This, again, suggests that pre-DM patients may have been alienated from appropriate medical measures despite their cardiovascular risk. Furthermore, a recently published study investigated the impact of pre-DM and DM on the 3-year outcome of patients treated with new-generation drug-eluting stents using post-hoc analyses of two large-scale randomized clinical trials (the BIO-RESORT and BIONYX trials). This study has shown that after treatment with new-generation drug-eluting stents, both patient groups had higher risks of ischemic and bleeding events compared with non-DM patients. Differences in major bleeding were mainly attributable to dissimilarities in baseline characteristics [19].
Our findings further support the findings of these previous studies that a pre-DM state is a significant risk factor for cardiovascular complications and mortality. Moreover, our study population were patients admitted to a tertiary care medical center ICCU with an acute cardiovascular disease, hence, had a higher risk for cardiovascular complications and mortality during follow-up. In light of the findings, the need arises for research regarding the effects of current diabetes treatments in patients with pre-DM state and whether the treatment recommendations for primary and secondary prevention should be changed accordingly.
Study limitations
Our study has several limitations: First, the study was an observational study and, as such, is subjected to confounding factors. Second, it is a single-center study. Lastly, we did not have data comparing medications on admission to the different groups in the study. However, this fact is less likely to affect the external validity of the study as long as pre-DM treatment is not significantly different from what is common elsewhere. Nevertheless, our study includes a large sample size of consecutive non-selected ICCU patients and includes real-world data about patients with various cardiac diseases who required hospitalization in the ICCU, which contributes to the external validity of the study.
Conclusion
Pre-DM and DM are common among ICCU patients. Among these patients, an HbA1c level of ≥ 5.7 g% (pre-DM & DM) is associated with a worse prognosis. Moreover, pre-DM patients probably have the highest risk for mortality following admission to the ICCU. Further studies are needed to better understand the reasons for this pre-DM paradox.
Availability of data and materials
The data that support the findings of this study are available from the authors [EA] upon reasonable request.
Abbreviations
- HbA1c:
-
Hemoglobin A1C
- ICCU:
-
Intensive cardiac care unit
- DM:
-
Diabetes mellitus
- ACS:
-
Acute coronary syndrome
- BMI:
-
Body mass index
References
Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis epidemiology, pathophysiology, and management. JAMA. 2002;287(19):2570–81.
Abbud ZA, Shindler DM, Wilson AC, Kostis JB. Effect of diabetes mellitus on short- and long-term mortality rates of patients with acute myocardial infarction: a statewide study. Myocardial infarction data acquisition system study group. Am Heart J. 1995;130(1):51–8.
Abbott RD, Donahue RP, Kannel WB, Wilson PW. The impact of diabetes on survival following myocardial infarction in men vs women. The Framingham Study. JAMA. 1988;260(23):3456–60.
Lehrke M, Marx N. Diabetes mellitus and heart failure. Am J Cardiol. 2017;120(1S):S37-47.
Coutinho M, Gerstein HC, Wang Y, Yusuf S. The relationship between glucose and incident cardiovascular events. A metaregression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 years. Diabetes Care. 1999;22(2):233–40.
Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet. 2000;355(9206):773–8.
Stranders I, Diamant M, van Gelder RE, Spruijt HJ, Twisk JWR, Heine RJ, et al. Admission blood glucose level as risk indicator of death after myocardial infarction in patients with and without diabetes mellitus. Arch Intern Med. 2004;164(9):982–8.
KojićDamjanov S, Đerić M, Eremić KN. Glycated hemoglobin A1c as a modern biochemical marker of glucose regulation. Med Pregl. 2014;67(9–10):339–44.
WHO Guidelines Approved by the Guidelines Review Committee. Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus: abbreviated report of a WHO consultation. Geneva: World Health Organization. 2011. http://www.ncbi.nlm.nih.gov/books/NBK304267/. Accessed 16 July 2021.
American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2019. Diabetes Care. 2019;42(Suppl 1):S13-28.
Hoang QN, Pisani MA, Inzucchi S, Hu B, Honiden S. The prevalence of undiagnosed diabetes mellitus and the association of baseline glycemic control on mortality in the intensive care unit: a prospective observational study. J Crit Care. 2014;29(6):1052–6.
Hadjadj S, Coisne D, Mauco G, Ragot S, Duengler F, Sosner P, et al. Prognostic value of admission plasma glucose and HbA in acute myocardial infarction. Diabet Med J Br Diabet Assoc. 2004;21(4):305–10.
Timmer JR, Ottervanger JP, Bilo HJG, Dambrink JHE, Miedema K, Hoorntje JCA, et al. Prognostic value of admission glucose and glycosylated haemoglobin levels in acute coronary syndromes. QJM Int J Med. 2006;99(4):237–43.
Ishikawa Y, Lewis RD, Laing EM, Anderson AK, Zhang D, Quyyumi AA, et al. Prevalence and trends of type 2 diabetes mellitus and prediabetes among community-dwelling heart failure patients in the United States. Diabetes Res Clin Pract. 2022;15(184): 109191.
Kim BG, Kim GY, Cha JK. Pre-diabetes is a predictor of short-term poor outcomes after acute ischemic stroke using IV thrombolysis. BMC Neurol. 2021;21(1):72.
Bansal N. Prediabetes diagnosis and treatment: a review. World J Diabetes. 2015;6(2):296–303.
Cai X, Zhang Y, Li M, Wu JH, Mai L, Li J, et al. Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis. BMJ. 2020;15(370): m2297.
Yahyavi SK, Snorgaard O, Knop FK, Schou M, Lee C, Selmer C, et al. Prediabetes defined by first measured HbA1c predicts higher cardiovascular risk compared with HbA1c in the diabetes range: a cohort study of nationwide registries. Diabetes Care. 2021;21:dc211062.
Ploumen EH, Pinxterhuis TH, Zocca P, Roguin A, Anthonio RL, Schotborgh CE, et al. Impact of prediabetes and diabetes on 3-year outcome of patients treated with new-generation drug-eluting stents in two large-scale randomized clinical trials. Cardiovasc Diabetol. 2021;20(1):217.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
EA is the guarantor of this study and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. LL and EA researched data and wrote the manuscript; MK, YS, FFS, NP, KH, NL, TM, HK, NA contributed to data curation. LT, RF, FB—statistics; GL, DG and MG contributed to the discussion and reviewed and edited the manuscript. All authors reviewed and provided edits and comments on the manuscript and agreed to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Institutional review board approved the study on the basis of strict maintenance of participants’ anonymity by de-identifying during database analysis. No individual consent was obtained.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lupu, L., Taha, L., Farkash, R. et al. Hemoglobin A1C as a prognostic factor and the pre-diabetic paradox in patients admitted to a tertiary care medical center intensive cardiac care unit. Cardiovasc Diabetol 21, 86 (2022). https://doi.org/10.1186/s12933-022-01529-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-022-01529-1