
Abstract
Background
Nocturnal desaturation is common in patients with chronic obstructive pulmonary disease (COPD) and impacts disease exacerbation and prognosis. In our previous study, we developed a diagnostic algorithm to classify nocturnal desaturation from SpO2 waveform patterns based on data from patients receiving home oxygen therapy. In this study, we aimed to investigate nocturnal desaturation in patients with COPD based on SpO2 waveform patterns and the associations between the waveforms and clinical data.
Methods
We investigated patients diagnosed with COPD and measured SpO2 and nasal airflow with a type 4 portable long-term recordable pulse oximeter. Then, we classified the SpO2 waveforms with the algorithm and compared the clinical data.
Results
One hundred fifty-three patients (136 male and 17 female) were analysed. One hundred twenty-eight of the 153 (83.7%) patients had nocturnal desaturation, with an intermittent pattern (70.6%), sustained pattern (13.1%) and periodic pattern (68.0%). Intriguingly, desaturation with an intermittent pattern was associated with the apnoea-hypopnea index obtained with the portable monitor, and desaturation with a sustained pattern was associated with the cumulative percentage of time at a SpO2 below 90%.
Conclusions
We found that nocturnal desaturation was frequently observed in patients with COPD and could be classified into 3 types of waveform patterns.
Similar content being viewed by others

Background
Chronic obstructive pulmonary disease (COPD) is a highly prevalent disease worldwide, and sleep-related desaturation in COPD is well known [1, 2]. Even patients with mild to moderate COPD have lower total sleep duration, lower sleep efficacy and worse sleep quality due to insomnia and awakenings at night, leading to a lower quality of life [3]. As COPD progresses, it has been reported that nocturnal desaturations in COPD contribute to the development of daytime respiratory failure, the frequency of acute exacerbations and the development of pulmonary hypertension and are associated with poor survival [4,5,6]. Although nocturnal desaturation may have an important impact on patients with COPD, less research has been focused on the waveform patterns of desaturation.
In our previous study, we analysed nocturnal SpO2 waveforms obtained from patients with chronic respiratory diseases receiving home oxygen therapy (HOT), and we showed that the SpO2 waveforms were very diverse [7]. Then, we found that each waveform was composed of a combination of three desaturation patterns: intermittent pattern, sustained pattern and periodic pattern. Moreover, we developed a diagnostic algorithm to automatically analyse these waveforms.
In clarifying the pathophysiology of desaturation, it is important to classify the desaturation pattern. Therefore, in the present study, we aimed to adapt the algorithm for patients with mild to moderate COPD who were not receiving oxygen therapy and analyse the association between the waveform patterns and the clinical features of COPD.
Methods
Patients
This study was performed between September 2017 and March 2020. The current study was conducted with the approval of the Ethics Committees or Institutional Review Board of Kobe University Hospital (permission number: 160208).
We enrolled 165 outpatients diagnosed with COPD who fulfilled the following inclusion criteria: aged 20 years or older; diagnosed with stable COPD; and daytime PaO2 ≥ 55 Torr (SpO2 ≥ 88%). COPD was diagnosed based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines (post-bronchodilator ratio of forced expiratory volume to forced vital capacity < 70%) [8]. Stable condition was defined as stable disease without reported exacerbations during the previous 3 months without any changes in respiratory medications. Patients were excluded from this study if they were receiving HOT (including positive-pressure ventilation therapy). Written informed consent was obtained from all study participants. The flowchart describing patient recruitment is shown in Fig. 1.

Recruitment of the patients
Measurement and data collection
At registration, a pulmonary function test (PFT) was carried out. The PFT was performed by trained operators in accordance with the international recommendations [9, 10]. Japanese local reference values were used for the predicted values of the PFT [11]. During night, we monitored and evaluated the patients’ oxygenation and breathing with a portable long-term recordable pulse oximeter (SAS2100; Nihon Kohden, Corp., Tokyo, Japan). Recordings with duration of at least 4 h were accepted. Sex, body mass index, daytime SpO2 at rest, and smoking history were extracted from the medical records.
Severity of COPD
Patients with COPD were classified as having GOLD 1 (forced expiratory volume in 1 s (FEV1) ≥ 80% predicted), GOLD 2 (50 ≤ FEV1 < 80% predicted), GOLD 3 (30 ≤ FEV1 < 50% predicted) and GOLD 4 (FEV1 < 30% predicted) disease based on the GOLD guidelines [8].
Detection of desaturation
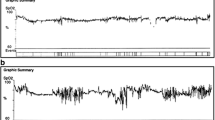
In the present study, desaturation was defined as a more than 3% decrease in SpO2 from baseline. Nocturnal desaturations were divided into three patterns based on the algorithm that Izumi [12]. In brief, when desaturation events lasting longer than 655 s occurred, the events were labelled as the sustained pattern (Fig. 2A). Desaturation events between 30 and 655 s that occurred more than twice were labelled as the periodic pattern (Fig. 2B). We defined the third pattern as the intermittent pattern in which the decrease in and recovery of SpO2 was repeated with a cycle of several minutes (Fig. 2C). Finally, we defined the waveform with limited SpO2 changes other than those described above as the normal pattern.

(adapted from reference with permission)
Characteristics of the nocturnal waveform pattern of SpO2 in COPD patients with nocturnal desaturation. A Sustained pattern, B periodic pattern and C intermittent pattern were classified based on the algorithm (Patients and Methods) ([12]
SpO2 waveforms are diverse; however, we found that each waveform was composed of a combination of three desaturation patterns: S: Sustained, P: Periodic, and I: Intermittent. SpO2 waveforms can be classified into the following eight groups based on the combination of these three patterns: S, P, I, S + P + I, P + I, S + P, S + I and normal.
Apnoea was recorded as the cessation of airflow for at least 10 s, and hypopnea was defined as a ≥ 30% reduction in airflow for at least 10 s associated with an oxygen desaturation ≥ 3%. The apnoea-hypopnea index obtained from the portable monitor (PM-AHI) was defined as the number of apnoeas and hypopneas divided by the total time measured by the portable pulse oximeter. The cumulative percentage of the time spent at a SpO2 less than 90% (CT90) was calculated as the cumulative time spent at a SpO2 less than 90% divided by the total time measured by the portable pulse oximeter.
The 3% oxygen desaturation was defined as a more than 3% decrease in SpO2 from baseline and recover within 120 s. The 3% oxygen desaturation index (ODI) was defined as the number of 3% oxygen desaturations divided by the total time measured by the portable pulse oximeter.
The hypoxic burden was defined as the total area between the baseline and SpO2 waveform divided by the total time measured by the portable pulse oximeter, with the unit of hypoxic burden being (%min)/h [13].
Statistical analysis
Comparisons concerning sex were performed using Fisher’s exact test. Comparisons between two groups other than sex were performed using the Mann–Whitney U-test. Comparison between seven groups was performed Kraskal-Wallis and Mann–Whitney U-test with Bonferroni’s correction. P values reported are 2-sided, and P values less than 0.05 were considered significant unless otherwise specified. P values after Bonferroni’s correction less than 0.0024 were considered significant.
Results
Patients and characteristics
One hundred fifty-three patients (136 male and 17 female) met the inclusion criteria. The median age of the participants was 72 years (interquartile range (IQR): 68–76), and their body mass index was 22.7 (IQR: 20.6–24.4). The numbers of patients with GOLD stages 1, 2, 3 and 4 were 27, 80, 38 and 4, respectively. These patients had a median daytime SpO2 of 97 (IQR: 96–98) %, and all participants had a daytime SpO2 ≥ 90%. The median percent predicted forced expiratory volume in 1 s (%FEV1) was 68.8 (IQR: 16.3–79.7), and the median lowest SpO2 was 85 (IQR: 80–87.5) %. Other patient characteristics, laboratory data and data from the portable oximeters are summarised in Table 1.
Nocturnal desaturation
One hundred twenty-eight of the 153 (83.7%) patients had nocturnal desaturation. The determination of the results with the automatic analysis algorithm for the waveforms is shown below. Desaturation with the intermittent pattern was observed in 108 (70.6%), desaturation with the sustained pattern was observed in 20 (13.1%) and desaturation with the periodic pattern was observed in 104 (68.0%). Intriguingly, there was substantial overlap of the waveforms, especially the intermittent and periodic patterns. A Venn diagram for the waveform patterns is shown in Fig. 3.

A Venn diagram of the waveform patterns
Associations between waveforms and clinical data
We conducted an exploratory analysis to clarify the clinical data and desaturation parameters in each group. The results are shown in Figs. 4 and 5. In the groups with overlapping waveforms, especially the S + P + I group, the CT90 tended to be higher, and the lowest SpO2 tended to be lower (Fig. 4).

Association between the waveforms and the clinical data. *: Statistically significance with Bonferroni’s correction of multiple testing. N: Normal, S: Sustained, P: Periodic, I: Intermittent

Association between the waveforms and desaturation parameters. *: Statistically significance with Bonferroni’s correction of multiple testing. N: Normal, S: Sustained, P: Periodic, I: Intermittent
We assumed that the algorithm, which was developed based on data from patients with severe disease receiving HOT, was still indicative of the pathophysiological aspects in the current study population. Therefore, we compared the patients’ characteristics between the groups with or without each desaturation pattern.
The patients with the intermittent pattern had a significantly higher PM-AHI (19.5, IQR: 13.1–41.9 vs. 5.7, IQR: 3.5–9.3) and higher 3% ODI (7.4, IQR: 4.0–11.8 vs. 2.0, IQR: 1.3–3.3) than patients without the intermittent pattern (Table 2). And, in patients with intermittent pattern, 107 of 108 (99.1%) patients showed PM-AHI ≥ 5. The patients with high PM-AHI (≥ 15) were 75 (69.4%). These patients were relatively severe in the point of airway obstruction showing lower %FEV1, although not statistically significant (49.6, IQR: 28.1–75.8 vs 53.4, IQR: 24.9–76.6, P = 0.387). In addition, the hypoxic burden was significantly higher in patients with intermittent pattern than patients without intermittent pattern.
The patients with the sustained pattern had a significantly higher CT90 than those without the sustained pattern (16.4, IQR: 1.9–37.1 vs. 2.1, IQR: 0.35–6.3). On the other hand, PM-AHI was significantly lower in the patients with the sustained pattern (8.4, IQR: 4.3–18.2 vs. 19.2, IQR: 12.1–28.7) (Table 3).
Comparisons between the patients with and without the periodic pattern revealed that there were no significant differences in the PM-AHI. %FEV1 was significantly lower in the patients with the periodic pattern (59.8, IQR: 50–66.1 vs. 73.9, IQR: 59.9–81.3) (Table 4).
Contrary to the hypothesis, the strength of the correlation between the desaturation pattern and the index of respiratory function was low.
Discussion
In the present study, we investigated nocturnal desaturation in patients with COPD who did not have daytime hypoxemia with an automatic analysis algorithm we previously reported [7].
Even in patients with COPD without daytime desaturation, nocturnal desaturation was common. Sleep affects breathing in various ways, such as through a decrease in ventilator responses to both hypoxia and hypercapnia, a decrease in tidal volume due to the diminished tone and activity of the accessory muscles of respiration, and an increase in upper airway resistance [14, 15].
Although these changes also occur in healthy subjects in an unknown manner [16], the effect of these changes on PaO2 can be negligible because of the high oxygen reserve in the lung. On the other hand, patients with COPD have pathological changes such as airflow limitation, respiratory muscle fatigue, hyperinflation of the lungs, and ventilation/perfusion ratio mismatch caused by the destruction of the pulmonary capillary beds [17], which can lead to lower baseline PaO2. In patients whose daytime PaO2 levels are on the steep portion of the oxyhaemoglobin dissociation curve, even small physiological changes in respiration can lead to greater desaturation [17, 18]. These might be the reasons many patients with COPD have nocturnal desaturation.
In the S + P + I group, there was no trend in %FEV1. In other words, it is possible that patients in this group might be exposed to severe hypoxemia regardless of the severity of COPD. Even in patients with COPD without daytime hypoxemia, it has been reported that desaturations can occur due to complications such as obstructive sleep apnoea (OSA) and rapid eye movement (REM) sleep-related hypoventilation [19, 20]. It is suggested that there is a population exposed to severe hypoxemia due to overlap of pathophysiologies, such as apnoea and hypoventilation.
In this study, PM-AHI was significantly higher in desaturation with the intermittent pattern. However, this was not observed in the comparison of patients with and without the sustained or periodic pattern. This might indicate a correlation between the intermittent pattern and PM-AHI. So, we assume this intermittent pattern reflects SAS. Moreover, it is suggested that 99.1% of patients in this pattern were suffering from COPD and SAS.
In each desaturation group, the results of PM-AHI and ODI were not necessarily similar. Because PM-AHI needs to evaluate with both airflow and 3% desaturation, whereas ODI is evaluated only with oxygen desaturation. Assumingly, this difference occurred the dissociation between PM-AHI and ODI results.
In intermittent pattern, the hypoxic burden may be more suitable than CT90 for evaluation the impacts of hypoxic exposure, because it evaluates not only duration of desaturation but also the depth of desaturation [13]. And it is also expected to be applied to other waveforms.
In our previous study, among patients with COPD receiving HOT, the lower %FEV1 was, the less desaturation with an intermittent pattern [7]. However, in this study, there was no significant difference. There is growing evidence that lung hyperinflation associated with emphysema reduces the likelihood of OSA [21]. It might be speculated that patients with mild to moderate COPD have mild lung hyperinflation, leading to few effects on desaturation with the intermittent pattern.
In this study, we revealed that there were many overlaps of patients with COPD and intermittent pattern. This made it difficult to evaluate periodic and sustained patterns independently from intermittent pattern. However, we believe it is important to find sleep breathing disorder in COPD is not a single pathophysiology, but often complex.
From the results of the comparison based on the sustained pattern, it could be suggested that patients with the sustained pattern had greater hypoxemic exposure. The characteristic of this sustained pattern is that the SpO2 does not recover for a long time, so it is a plausible result. Although there have been reports on the impacts of sustained hypoxic load during sleep [22, 23], the pathophysiology of sustained nocturnal desaturation is not clear. These results suggested that at least this pattern was not involved in apnoea and hypopnea. It has been reported that sustained hypoxemia impairs the arousal response [24, 25], and this arousal response might be involved in sustained desaturation. Nocturnal hypoxemia is generally defined as a SpO2 ≤ 88% for more than 5 min [26], among them, there may be a population of patients that we defined as having the sustained pattern.
We assume that the clinical condition of the periodic pattern is REM sleep-related hypoventilation which correlated with elevated PaCO2, COPD exacerbation, pulmonary hypertension [20] and poor prognosis [27]. Previous study showed that REM sleep-related hypoventilation is seen in patients with severe COPD and type II respiratory failure [20, 28]. Our result in periodic group is consistent with previous reports in the point that %FEV1 was lower in the periodic pattern group. During REM sleep, there are marked diminished in the activity of the accessory muscles of respiration and decrease in ventilator responses in the respiratory center, which can easily lead to alveolar hypoventilation. Based on such speculation, desaturation due to these changes would be more likely to occur in patients with more severe COPD whose pulmonary dysfunction is more severe. On the other hand, Kitajima et al. suggested that NPPV therapy decrease daytime PaCO2 and COPD exacerbation frequency, and may improve PH in patients with REM sleep-related hypoventilation [20]. NPPV therapy is also expected to improve prognosis of these of these patients. Therefore we believed that detecting the periodic pattern is clinically important. Although our study observation found no significant association with clinical specific parameters, further studies associating sleep studies and waveform patterns are needed to clarify the clinical utility.
In this study, we evaluated the nocturnal SpO2 waveforms and found them to be very diverse. We also classified these waveforms and clarified some of the pathogenesis and the patient backgrounds of each waveform. This might be useful because it helps clarify the pathogenesis of sleep disorders, and warrants further clinical study to lead to provide more appropriate treatment in COPD patients.
The limitations of the present study are the lack of data on polysomnography and overnight transcutaneous carbon dioxide tension. In this study, we used a type 4 portable long-term recordable pulse oximeter to measure SpO2 and nasal airflow. According to the classification of the American Sleep Disorder Association, type 4 is determined by the continuous measurement of single or dual bioparameters, for example, oxygen saturation or airflow [29]. This type 4 portable monitor tends to underestimate PM-AHI because the PM-AHI index is defined as the number of apnoeas and hypopneas divided by the total measured time, which is longer than the total sleep time, and the PM-AHI index does not include hypopnea associated with arousal.
Conclusions
We found that even in patients with COPD without daytime desaturation, nocturnal desaturation was common. We found that the algorithm, which was developed based on data from patients receiving HOT, could be adapted to some extent to patients with COPD, and it captured aspects of the pathogenesis of each desaturation pattern in this study.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COPD:
-
Chronic obstructive pulmonary disease
- GOLD:
-
Global Initiative for Chronic Obstructive Disease
- HOT:
-
Home oxygen therapy
- PET:
-
Pulmonary function test
- FEV1 :
-
Forced expiratory volume in 1 s
- PM-AHI:
-
Apnoea-hypopnea index from portable monitor
- CT90:
-
Cumulative percentage time at SpO2 below 90%
- ODI:
-
Oxygen desaturation index
- IQR:
-
Interquartile range
- %FEV1 :
-
Percent predicted forced expiratory volume in 1 s
- OSA:
-
Obstructive sleep apnoea
- REM:
-
Rapid eye movement
References
Fletcher EC, Miller J, Divine GW, Fletcher JG, Miller T. Nocturnal oxyhemoglobin desaturation in COPD patients with arterial oxygen tensions above 60 mm Hg. Chest. 1987;92:604–8.
Sharafkhaneh A, Jayaraman G, Kaleekal T, Sharafkhaneh H, Hirshkowitz M. Sleep disorders and their management in patients with COPD. Ther Adv Respir Dis. 2009;3:309–18.
Valipour A, Lavie P, Lothaller H, Mikulic I, Burghuber OC. Sleep profile and symptoms of sleep disorders in patients with stable mild to moderate chronic obstructive pulmonary disease. Sleep Med. 2011;12:367–72.
McEvoy RD, Pierce RJ, Hillman D, Esterman A, Ellis EE, Catcheside PG, O’Donoghue FJ, Barnes DJ, Grunstein RR. Nocturnal non-invasive nasal ventilation in stable hypercapnic COPD: a randomised controlled trial. Thorax. 2009;64:561–6.
Owens RL, Malhotra A: Sleep-disordered breathing and COPD: the overlap syndrome. Respir Care 2010, 55:1333–1344 (discussion 1344–1336).
Agusti A, Hedner J, Marin JM, Barbe F, Cazzola M, Rennard S. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20:183–94.
Yoshizaki A, Nagano T, Izumi S, Funada Y, Nakata K, Nishiuma T, Takatsuki K, Ohnishi H, Hazeki N, Yasuda Y, et al. Prospective study of nocturnal desaturation in patients receiving home oxygen therapy. Intern Med. 2021;60:3071–9.
Gupta N, Agrawal S, Chakrabarti S, Ish P. COPD 2020 Guidelines - what is new and why? Adv Respir Med. 2020;88:38–40.
Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten CP, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J. 2005;26:720–35.
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CP, Gustafsson P, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–38.
Kubota M, Kobayashi H, Quanjer PH, Omori H, Tatsumi K, Kanazawa M. Reference values for spirometry, including vital capacity, in Japanese adults calculated with the LMS method and compared with previous values. Respir Investig. 2014;52:242–50.
Izumi S, Nagano T, Yoshizaki A, Nishimura Y. Classification algorithm for nocturnal hypoxemia using nocturnal pulse oximetry. Conf Proc IEEE Eng Med Biol Soc. 2019;2019:3662–5.
Azarbarzin A, Sands SA, Stone KL, Taranto-Montemurro L, Messineo L, Terrill PI, Ancoli-Israel S, Ensrud K, Purcell S, White DP, et al. The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the Osteoporotic Fractures in Men Study and the Sleep Heart Health Study. Eur Heart J. 2019;40:1149–57.
Krachman S, Minai OA, Scharf SM. Sleep abnormalities and treatment in emphysema. Proc Am Thorac Soc. 2008;5:536–42.
Becker HF, Piper AJ, Flynn WE, McNamara SG, Grunstein RR, Peter JH, Sullivan CE. Breathing during sleep in patients with nocturnal desaturation. Am J Respir Crit Care Med. 1999;159:112–8.
Douglas NJ, White DP, Pickett CK, Weil JV, Zwillich CW. Respiration during sleep in normal man. Thorax. 1982;37:840–4.
McNicholas WT, Verbraecken J, Marin JM. Sleep disorders in COPD: the forgotten dimension. Eur Respir Rev. 2013;22:365–75.
McNicholas WT, Hansson D, Schiza S, Grote L. Sleep in chronic respiratory disease: COPD and hypoventilation disorders. Eur Respir Rev. 2019;28:1.
D’Cruz RF, Murphy PB, Kaltsakas G. Sleep disordered breathing and chronic obstructive pulmonary disease: a narrative review on classification, pathophysiology and clinical outcomes. J Thorac Dis. 2020;12:S202-s216.
Kitajima T, Marumo S, Shima H, Shirata M, Kawashima S, Inoue D, Katayama Y, Itotani R, Sakuramoto M, Fukui M. Clinical impact of episodic nocturnal hypercapnia and its treatment with noninvasive positive pressure ventilation in patients with stable advanced COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:843–53.
McNicholas WT. COPD-OSA overlap syndrome: evolving evidence regarding epidemiology, clinical consequences, and management. Chest. 2017;152:1318–26.
Orr RS, Jordan AS, Catcheside P, Saunders NA, McEvoy RD. Sustained isocapnic hypoxia suppresses the perception of the magnitude of inspiratory resistive loads. J Appl Physiol. 1985;2000(89):47–55.
Eckert DJ, Catcheside PG, McDonald R, Adams AM, Webster KE, Hlavac MC, McEvoy RD. Sustained hypoxia depresses sensory processing of respiratory resistive loads. Am J Respir Crit Care Med. 2005;172:1047–54.
Eckert DJ, Catcheside PG, Smith JH, Frith PA, McEvoy RD. Hypoxia suppresses symptom perception in asthma. Am J Respir Crit Care Med. 2004;169:1224–30.
Hlavac MC, Catcheside PG, McDonald R, Eckert DJ, Windler S, McEvoy RD. Hypoxia impairs the arousal response to external resistive loading and airway occlusion during sleep. Sleep. 2006;29:624–31.
Budhiraja R, Siddiqi TA, Quan SF. Sleep disorders in chronic obstructive pulmonary disease: etiology, impact, and management. J Clin Sleep Med. 2015;11:259–70.
Fletcher EC, Donner CF, Midgren B, Zielinski J, Levi-Valensi P, Braghiroli A, Rida Z, Miller CC. Survival in COPD patients with a daytime PaO2 greater than 60 mm Hg with and without nocturnal oxyhemoglobin desaturation. Chest. 1992;101:649–55.
O’Donoghue FJ, Catcheside PG, Ellis EE, Grunstein RR, Pierce RJ, Rowland LS, Collins ER, Rochford SE, McEvoy RD. Sleep hypoventilation in hypercapnic chronic obstructive pulmonary disease: prevalence and associated factors. Eur Respir J. 2003;21:977–84.
Flemons WW, Littner MR, Rowley JA, Gay P, Anderson WM, Hudgel DW, McEvoy RD, Loube DI. Home diagnosis of sleep apnea: a systematic review of the literature. An evidence review cosponsored by the American Academy of Sleep Medicine, the American College of Chest Physicians, and the American Thoracic Society. Chest. 2003;124:1543–79.
Acknowledgements
We would like to thank all investigators who recruited patients and all the patients who participated.
Funding
This work was supported by a joint research Grant from Teijin Pharma Limited to Yoshihiro Nishimura.
Author information
Authors and Affiliations
Contributions
AY, TN and MY conceptualized the study and wrote the manuscript. SI, AY, TN and MY conducted data analysis and statistical analysis. TN, KN, MY, YY, DH, KU, NK, MT and KK collected data. YN and KK supervised the work and were responsible for the project administration. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted with the approval of the Ethics Committees or Institutional Review Board of Kobe University Hospital (Permission Number: 160208). Witten informed consent was obtained from all patients.
Consent for publication
Not applicable.
Competing interests
This work was supported by a joint research grant from Teijin Pharma Limited to Yoshihiro Nishimura.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yoshizaki, A., Nagano, T., Izumi, S. et al. Characteristics of the nocturnal desaturation waveform pattern of SpO2 in COPD patients: an observational study. Respir Res 22, 276 (2021). https://doi.org/10.1186/s12931-021-01868-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-021-01868-9