
Abstract
Background
High FiO2 during one-lung ventilation (OLV) can improve oxygenation, but increase the risk of atelectasis and oxidative stress. The aim of this study was to analyze whether Prostaglandin E1 (PGE1) can improve oxygenation and attenuate oxidative stress during OLV under a lower FiO2.
Method
Ninety patients selectively undergoing thoracotomy for esophageal cancer were randomly divided into three groups (n = 30/group): Group P (FiO2 = 0.6, inhaling PGE1 0.1 μg/kg), Group L (FiO2 = 0.6) and Group C (FiO2 = 1.0). The primary outcomes were oxygenation and pulmonary shunt during OLV. Secondary outcomes included haemodynamics, respiratory mechanics and oxidative stress in serum.
Results
Patients in Group P had significantly higher PaO2 and lower shunt fraction in 30 min of OLV compared with Group L. Compared with Group C, patients in Group P had similar levels of PaO2/FiO2 in 60 min and higher levels of PaO2/FiO2 at 2 h during OLV. The levels of PvO2 and SvO2 in Group P and Group L were significantly lower than Group C. Patients in Group P and Group L had significantly higher levels of superoxide dismutase and lower levels of malondialdehyde than Group C. No significant differences were found in SPO2, ETCO2, PaCO2, Paw, HR and MAP among the three groups. The complications in Group C were significantly higher than another two groups.
Conclusion
PGE1 can maintain adequate oxygenation in patients with low FiO2 (0.6) during OLV. Reducing FiO2 to 0.6 during OLV can decrease the levels of oxidative stress and complications after OLV.
Trial registration
chictr.org.cn identifier: ChiCTR1800017100.
Similar content being viewed by others


Background
Adequate resection of primary lesions and dissection of lymph nodes are important for thoracotomy in treatment of esophageal cancer [1, 2]. One lung ventilation (OLV) technology provides a maneuverable and minimally mobile surgical field. However, the complication, such as intrapulmonary shunt, can lead to a dropping partial pressure of arterial oxygen (PaO2) and threatening hypoxemia [3, 4]. Even though high FiO2 (1.0) improved oxygenation [5], subsequent atelectasis and oxidative stress significantly increased the risk of acute respiratory distress syndrome (ARDS), which were the leading cause of death after surgery [6, 7]. Studies showed that high FiO2, high airway pressure, and prolonged OLV were independent risk factors for ARDS [8,9,10]. The current protective ventilation strategy recommends use of the lowest FiO2 as far as possible in the presence of adequate oxygenation [11].
PGE1 is a selective pulmonary arterial vasodilator. Study had shown that PGE1 could decrease pulmonary shunts and increase PaO2 in a dose-dependent manner during OLV [12]. However, it remains unknown about whether PGE1 nebulization of ventilated lung can reduce pulmonary shunts and maintain adequate oxygenation during OLV under a lower FiO2. The primary objective of this research was to study the effect of preemptive PGE1 nebulization of ventilated lung with a lower FiO2 on maintaining adequate oxygenation during OLV. Our secondary objective was to study the benefits of lower FiO2 during OLV.
Our previous animal study showed that FiO2 (0.6) was safe for OLV and could make a lower lung injury and oxidative stress than FiO2 (1.0). Thus, FiO2 (0.6) was used as lower FiO2 during OLV in this article [13]. Previous studies showed that high FiO2 during OLV was associated with many complications, including lung atelectasis, lung infiltration, lung injury and ARDS [6, 7, 14,15,16]. Reactive oxygen species produced by cells under excessive oxygen were the main reason to this complications [17, 18]. Serum levels of malondialdehyde (MDA) and superoxide dismutase (SOD) are indirect parameters of oxidative stress. Previous studies had shown that MDA was association with lung injury and SOD could attenuate the lung injury [19, 20]. In this article, levels of MDA and SOD and complications after surgery were used to evaluate the benefits of lower FiO2 during OLV.
Methods
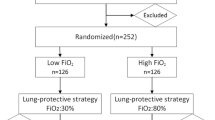
Esophageal cancer patients who were scheduled for elective open radical resection were recruited at the Affiliated Cancer Hospital of Nanjing Medical University between 2015 and 2017. Esophageal cancer was diagnosed on the basis of clinical, laboratory, gastroscopy and pathology. Exclusion Criteria: (1) SpO2 < 90% during trial; (2) severe arrhythmia and hemodynamic instability during surgery; (3) Surgical duration more than 6 h or less than 1 h; (4) immune, endocrine, neurological and cardiovascular diseases, liver dysfunction, kidney dysfunction, glaucoma and psychiatric disorder. Patients were randomly assigned to three groups using random number table (Fig. 1): Group P (FiO2 = 0.6, PGE1 dose = 0.1 μg kg− 1, n = 30) [14], Group L (FiO2 = 0.6, n = 30) and Group C (FiO2 = 1.0, n = 30). All the participants were enrolled after written informed consent was obtained and this study was approval from the Ethics Committee of Nanjing Medical University according to the Helsinki Declaration. This randomized controlled clinical trial was registered at chictr.org.cn (identifier: ChiCTR1800017100).

Flow diagram of study participants
Anesthesia and intervention
All patients were under total intravenous anesthesia with left-sided double-lumen intratracheal intubation. 30 min before being sent into OR, patients were given intramuscular phenobarbital 0.1 g and atropine 0.5 mg. Upon entering the OR, central venous catheter was placed into the right internal jugular vein. Induction was done with sequential intravenous midazolam 0.05 mg kg− 1, fentanyl 3 ~ 4 μg kg− 1, propofol 1 mg kg− 1 and cis-atracurium 0.2 mg kg− 1. Left-sided double-lumen intratracheal tube was then placed, followed with confirmation of position using fiberoptic bronchoscope. Ventilation parameters were set as follows: VT = 6 ~ 8 ml/predicted body weight, RR = 12 ~ 14 /min, I: E = 1:2, ETCO2 = 35 ~ 45 mmHg, FiO2 = 0.6, PEEP = 5cmH2O. During OLV, theses parameters was remained unchanged and nonventilated lung was directly connected with room air. Group P and Group L had FiO2 of 0.6 throughout the surgery, while Group C had FiO2 of 1.0. Continuous intravenous pumps of remifentanil, propofol and cis-atracurium were set up for maintenance of anesthesia. Monitored intraoperative anesthesia depth and maintained bispectral index (BIS) at 40 ~ 60.
After confirming the placement of double-lumen tube with fiberoptic bronchoscope, patient was repositioned to right lateral decubitus and both lungs were ventilated. Group P was given PGE1 [21] (Beijing Tide Pharmaceutical Co., LTD, 10 μg/2 ml, diluted to 10 ml with normal saline) nebulization to the right lung through a reconstructed breathing circuit, while Group L and Group C were given 10 ml normal saline nebulization to the right lung, all nebulization maintained for 10 min. We modified the Yuyue 402A ultrasonic nebulizer by first sealing the bottom of nebulizer tank thus removing the air intake; and then separating the two original nebulizer outlets, so that one outlet was the new intake and the other became the only outlet towards the patient. The system is then connected to the breathing circuit [22].
Observed parameters
An arterial catheter was placed into the radial artery, and a central venous line (two lumens 20 cm long) was introduced via the internal right jugular vein into the right atrium, and its position was confirmed by chest roentgenogram. Artery and venous blood samples were collected for blood gas analyses at post-anesthesia/pre-nebulization (T1), OLV 10 min (T2), OLV 15 min (T3), OLV 30 min (T4), OLV 60 min (T5), OLV 120 min (T6). Meanwhile, mean arterial pressure (MAP), HR and airway pressure (Paw) were recorded. Shunt fraction was calculated using this formula: Qs/Qt = (CcO2-CaO2)/(CcO2-CvO2) [23, 24].
CaO2 = (1.36 × hemoglobin ×SaO2) + (0.0031 × PaO2);
CvO2 = (1.36 × hemoglobin ×SvO2) + (0.0031 × PvO2);
CcO2 = ([FiO2 × (PB-PH2O)-PaCO2/Respiratory quotient] × 0.0031) + 1.36 × hemoglobin;
PB,760 mmHg; PH2O, 47 mmHg; respiratory quotient, 0.8.
Measurement of serum malondialdehyde and superoxide dismutase
Venous blood sampling through central line was collected at T1, T4, 30 min after restarting two lung ventilation (TLV) (T7) and 24 h post-operation (T8). After centrifugation at 3000 rpm for 20 min, serum samples were frozen and stored at − 80 °C until biochemical assessment. Human MDA and SOD ELISA Kits were used to measure the concentrations of malondialdehyde (MDA) and superoxide dismutase (SOD) as manual described, respectively.
Statistical analysis
SPSS 20.0 software (IBM Corporation, Armonk, NY, USA) was used to data analysis. At least 25 patients were required in each group to achieve a power of 0.8 and a type I error of 0.05. The data was expressed as mean ± standard deviation (SD) of at least triplicate measurements, and statistical analysis was made by t-test or ANOVA as appropriate. Counting data was tested by chi-square test. P < 0.05 was considered statistically significant.
Results
A total of 90 patients (74 male, 16 female) were enrolled and randomly divided into three groups. Two patients in Group L developed hypoxemia (occurring in 10 min and 15 min during OLV, respectively) and needed to elevate FiO2 during OLV. They were excluded from Group L due to elevating FiO2. Table 1 showed the clinical characteristics of patients in the three groups. There were no significant differences in age, gender, BMI, ASA class, TNM class, lung function, OLV and surgical time (p > 0.05).
PaO2 and PaO2/FiO2 decreased in the first 30 min after initiation of OLV (Fig. 2a and c), while Qs/Qt increased (Fig. 2b). PaO2, PaO2/FiO2 and Qs/Qt in Group L and Group C reached nadir at 30 min, while Group P did at 60 min. Group L and P had significantly lower PaO2 and Qs/Qt than Group C during the whole OLV. Group P had significantly higher levels of PaO2 than Group L, but lower levels of Qs/Qt in first 30 min during OLV (Fig. 2a and b). Group L had significantly lower PaO2/FiO2 than Group P and C in first 30 min, and no significant difference was found between Group P and Group C (Fig. 2c) in first 60 min during OLV. At OLV 120 min, Group P had significantly higher level of PaO2/FiO2 than Group C. Group C had significantly higher levels of PvO2 (Fig. 2d) and SvO2 (Table 2) than Group P and L during OLV. No significant difference was found in SpO2, ETCO2, PaCO2, Paw, HR and MAP among the three groups at each point (Table 2).

PaO2, Qs/Qt, PaO2/FiO2 and PvO2 dynamic changing during OLV in three groups. Comparison of the level of PaO2 (a), Qs/Qt (b), PaO2/FiO2 (c) and PvO2 (d) in Group P, Group L and Group C at post-anesthesia/pre-nebulization (T1), OLV 10 min (T2), OLV 15 min (T3), OLV 30 min (T4), OLV 60 min (T5), OLV 120 min (T6). *p < 0.05 Group L vs. Group C; #p < 0.05 Group P vs. Group L; §p < 0.05 Group P vs. Group C
At 30 min after restarting TLV and 24 h after surgery, the levels of SOD in Group P and L were significantly higher than Group C, while MDA were significantly lower (Fig. 3). No significant difference was found in SOD and MDA levels between Group P and L. After the surgery, there was no significantly difference in the ICU stays and hospital stays among the three groups (p > 0.08). No patients had complications after surgery in Group P and L, while 2 patients had pulmonary infection, 1 patient had pulmonary infection and pulmonary atelectasis and 1 patient had liver dysfunction in Group C (Table 3). The risk of complications was significantly higher in Group C than in Group P and L (p = 0.012).

Serum SOD activities and MDA levels in three groups. Comparison of Serum SOD activities (a) and MDA levels (b) in Group P, L and C at T1 (post-anesthesia/pre-nebulization), T5 (OLV 60 min), T7 (30min after switching back to TLV), T8 (24h post-operation). *p < 0.05 vs. Group C
Discussion
Although previous study had shown that PGE1 could decrease pulmonary shunt and increase PaO2 in a dose-dependent manner during OLV [12], it remains unclear whether PGE1 can help to maintain adequate oxygenation with a low FiO2 during OLV. Our article showed that low FiO2 (0.6) led to lower levels of PaO2, PaO2/FiO2, Qs/Qt and PvO2 than high FiO2 (1.0). PGE1 can increase the levels of PaO2 and PaO2/FiO2 in first 30 min during OLV. More importantly, PGE1 can even make patients with low FiO2 (0.6) have a higher level of PaO2/FiO2 than high FiO2 (1.0) at 2 h during OLV. Meanwhile, the low FiO2 (0.6) did not influence the levels of ETCO2, PaCO2, Paw, HR and MAP during OLV. In addition, low FiO2 (0.6) can also decrease oxidative stress and complications after surgery.
Yang M et al. showed that 58% of patients with protective strategy (FiO2 = 0.5, PEEP = 5cmH2O, VT = 6 mL/kg) during OLV developed hypoxemia and needed to elevate FiO2 to maintain an SpO2 > 95% [14]. While, our result showed that only 6.7% (2/30) of patients (FiO2 = 0.6, PEEP = 5cmH2O, VT = 6 ~ 8 mL/kg) developed hypoxemia and needed to elevate FiO2. In addition, no patients in Group P developed hypoxemia. We speculated that FiO2 (0.6) was the lower limit for studying the benefits of low FiO2.
Hypoxic pulmonary vasoconstriction (HPV) is a reflex contraction of vascular smooth muscle in the pulmonary circulation in response to low regional partial pressure of oxygen (Po2) [25]. Due to higher PaO2 (> 100 mmHg), HPV did not occur in the ventilated lung. The pulmonary vascular resistance (PVR) of HPV in non-ventilated lung would redistribute pulmonary blood flow to the ventilated lung. Lumb Andrew B et al. showed that PVR was determined by PvO2 in non-ventilated lung during OLV [25]. Lower levels of PvO2 in Group P and L (Fig. 2d) would lead to higher levels of PVR in non-ventilated lung, which would increase blood flow to the ventilated lung and decrease shunt fraction. As anticipated, we detected lower levels of Qs/Qt (Fig. 2b) in Group P and L. PGE1 could dilate pulmonary artery in ventilated lung [21], whic h could also increase blood flow to the ventilated lung and decrease shunt fraction. We also detected lower levels of Qs/Qt (Fig. 2b) in Group P. In conclusion, low FiO2 and PGE1 could increase blood flow to the ventilated lung and decrease shunt fraction during OLV.
Previous studies showed that HPV had two distinct phases [26,27,28]. Phase 1 began within a few seconds and was maximal at 15 min. When moderate hypoxia (Po2 30 to 50 mmHg) was sustained for more than 30 to 60 min, phase 2 of HPV began and a further increase in PVR was seen, reaching a peak at 2 h. In clinical practice, PaO2 reached its lowest level 20 to 30 min after the start of OLV and then gradually increased during the next 1 to 2 h [29]. Here, our results showed that PaO2 decreased and reached nadir in the first 30 min during OLV and 2 hypoxemias occurred in Group L at 10 min and 15 min during OLV, respectively. More importantly, our results further showed that PGE1 delayed the nadir time of PaO2 to 60 min, during which PVR began the second increasing. Overall, PGE1 was beneficial for patients to go through hypoxic period in the first 30 min during OLV. No patients in Group P had hypoxemia during OLV, supporting the conclusion.
Grubb TL et al. showed that PGE1 increased the level of PaO2/FiO2 and decreased the level of Qs/Qt at 15 min during OLV. Meanwhile, the level of PaO2/FiO2 and Qs/Qt returned after PGE1 withdrawal [21]. Our results further showed that PGE1 increased the level of PaO2/FiO2 in patients with low FiO2 (0.6) to the level in patients with high FiO2 (1.0) in 60 min during OLV, indicating that PGE1 could maintain adequate oxygenation in patients with low FiO2 (0.6) in 60 min during OLV. More importantly, PGE1 made a higher PaO2/FiO2 in patients with low FiO2 (0.6) than in patients with high FiO2 (1.0) at 2 h during OLV, indicating that PGE1 was beneficial to a prolong surgery.
Ultrasonic nebulizer utilizes 50 Hz AC electricity, converts it into high frequency electricity of more than 1.45 MHz and then into same frequency sound waves (ultrasonic wave). This wave generates mechanical oscillation to the drug solution, creating aerosols of 1–5 μm diameter that are of similar diameter as alveoli. Therefore, medications can enter the alveoli with airflow [22], accumulate in the lower respiratory tract and exert a fast and localized effect with minimal systemic impact [30]. As anticipated, the three groups had similar levels of MAP and HR in our study.
Although higher levels of oxidative stress in patients with higher FiO2 after the surgery had been demonstrated by previous studies [14, 31, 32], the levels of oxidative stress during OLV were little studied. In our article, we studied the levels of MDA and SOD at post-anesthesia/pre-nebulization, 60 min during OLV, 30 min after restarting TLV and 24 h after surgery. Our results showed that the higher oxidative stress in patients with higher FiO2 occurred only after the OLV. Olivant et al. [32] showed similar levels of pro-inflammatory cytokines in the plasma during OLV. However, higher levels of pro-inflammatory cytokines were detected in lung tissue after surgery. Our results explained this paradox phenomenon.
Our previous animal study showed that FiO2 (0.6) decreased the levels of oxidative stress and lung injury after OLV [13]. Here, our results further showed that FiO2 (0.6) can decrease the levels of oxidative stress and complications in esophageal cancer patients after OLV. In this article, we not only studied the benefits of lower FiO2 in human, but also the benefits of PGE1. However, there are still some limitations in this study. Firstly, the sample size was small to study the role of PGE1 in some rare complications, such as ARDS. Secondly, we did not study the safe dose range of PGE1. Thirdly, our study subjects were limited to patients with normal pulmonary function. Even though a case report had shown that epoprostenol improve oxygenation in a patient with severe interstitial lung disease during OLV [33], more articles are needed to study the role of PGE1 in patients with impaired pulmonary function. Finally, whether PGE1 had similar effects in elderly, obesity and pediatric patients needed to study.
Conclusions
PGE1 can maintain adequate oxygenation in patients with low FiO2 (0.6) in during OLV. Reducing FiO2 to 0.6 during OLV can decrease the levels of oxidative stress and complications after OLV.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- OLV:
-
One-lung ventilation
- PGE1 :
-
Prostaglandin E1
- FiO2 :
-
Fraction of inhaled oxygen
- SOD:
-
Superoxide dismutase
- MDA:
-
Malondialdehyde
- ARDS:
-
Acute respiratory distress syndrome
- PaO2 :
-
Partial pressure of arterial oxygen
- BIS:
-
Bispectral index
- MAP:
-
Mean arterial pressure
- Paw:
-
Airway pressure
- HPV:
-
Hypoxic pulmonary vasoconstriction
- PVR:
-
Pulmonary vascular resistance
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90.
McGuire S. World Cancer report 2014. Geneva, Switzerland: World Health Organization, International Agency for Research on Cancer, WHO press 2015. Adv Nutr. 2016;7:418–9.
Lohser J. Managing hypoxemia during minimally invasive thoracic surgery. Anesthesiol Clin. 2012;30(4):683–97.
Karzai W, Schwarzkopf K. Hypoxemia during one-lung ventilation: prediction, prevention, and treatment. Anesthesiology. 2009;110(6):1402–11.
Lytle FT, Brown DR. Appropriate ventilatory settings for thoracic surgery: intraoperative and postoperative. Semin Cardiothorac Vasc Anesth. 2008;12(2):97–108.
García-de-la-Asunción J, García-Del-Olmo E, Perez-Griera J, Marti F, Galan G, Morcillo A, et al. Oxidative lung injury correlates with one-lung ventilation time during pulmonary lobectomy: a study of exhaled breath condensate and blood. Eur J Cardiothorac Surg. 2015;48(3):e37–44.
Rothen HU, Sporre B, Engberg G, Wegenius G, Reber A, Hedenstierna G. Prevention of atelectasis during general anaesthesia. Lancet. 1995;345(8962):1387–91.
Misthos P, Katsaragakis S, Theodorou D, Milingos N, Skottis I. The degree of oxidative stress is associated with major adverse effects after lung resection: a prospective study. Eur J Cardiothorac Surg. 2006;29(4):591–5.
Blank RS, Colquhoun DA, Durieux ME, Kozower BD, et al. Management of one-lung Ventilation: impact of tidal volume on complications after thoracic surgery. Anesthesiology. 2016;124(6):1286–95.
Jeon K, Yoon JW, Suh GY, Kim J, Kim K, Yang M, et al. Risk factors for post-pneumonectomy acute lung injury/acute respiratory distress syndrome in primary lung cancer patients. Anaesth Intensive Care. 2009;37(1):14–9.
Brassard Charles L, Lohser J, Donati F, Bussières Jean S. Step-by-step clinical management of one-lung ventilation: continuing professional development. Can J Anaesth. 2014;61(12):1103–21.
Chen TL, Lee YT, Wang MJ, Lee JM, Lee YC, Chu SH. Endothelin-1 concentrations and optimisation of arterial oxygenation and venous admixture by selective pulmonary artery infusion of prostaglandin E1 during thoracotomy. Anaesthesia. 1996;51(5):422–6.
Xu Z, Gu L, Bian Q, Li P, Wang L, Zhang J, et al. Oxygenation, inflammatory response and lung injury during one lung ventilation in rabbits using inspired oxygen fraction of 0.6 vs. 1.0. J Biomed Res. 2016;31(1):56–64.
Yang M, Ahn HJ, Kim K, Kim JA, Yi CA, Kim MJ, et al. Does a protective ventilation strategy reduce the risk of pulmonary complications after lung cancer surgery?: a randomized controlled trial. Chest. 2011;139(3):530–7.
Magnusson L, Spahn DR. New concepts of atelectasis during general anaesthesia. Br J Anaesth. 2003;91(1):61–72.
Licker M, Fauconnet P, Villiger Y, Tschopp JM. Acute lung injury and outcomes after thoracic surgery. Curr Opin Anaesthesiol. 2009;22(1):61–7.
Kellner M, Noonepalle S, Lu Q, Srivastava A, Zemskov E, Black SM. ROS signaling in the pathogenesis of acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). Adv Exp Med Biol. 2017;967:105–37.
Zewu D, Yufang Y. Accelerated inflammation and oxidative stress induced by LPS in acute lung injury: Ιnhibition by ST1926. Int J Mol Med. 2018;41:3405–21.
Williams EA, Quinlan GJ, Anning PB, Goldstraw P, Evans TW. Lung injury following pulmonary resection in the isolated, blood-perfused rat lung. Eur Respir J. 1999;14(4):745–50.
Tekinbas C, Ulusoy H, Yulug E, Erol MM, Alver A, Yenilmez E, Geze S, Topbas M. One-lung ventilation: for how long? J Thorac Cardiovasc Surg. 2007;134(2):405–10.
Della Rocca G, Coccia C, Pompei L, Costa MG, Di Marco P, Pietropaoli P. Inhaled aerosolized prostaglandin E1, pulmonary hemodynamics, and oxygenation during lung transplantation. Minerva Anestesiol. 2008;74(11):627–33.
Xu X, Wang X, Weihong G, et al. The pharmacokinetics of inhaled morphine delivered by an ultrasonic nebulizer in ventilated dogs. J Aerosol Med Pulm Drug Deliv. 2012;25(1):41–6.
Walley KR. Use of central venous oxygen saturation to guide therapy. Am J Respir Crit Care Med. 2011;184(5):514–20.
Hardman JG, Bedforth NM, Ahmed AB, Mahajan RP, Aitkenhead AR. A physiology simulator: validation of its respiratory components and its ability to predict the patient's response to changes in mechanical ventilation. Br J Anaesth. 1998;81(3):327–32.
Lumb Andrew B, Slinger P. Hypoxic pulmonary vasoconstriction: physiology and anesthetic implications. Anesthesiology. 2015;122(4):932–46.
Benumof JL. Intermittent hypoxia increases lobar hypoxic pulmonary vasoconstriction. Anesthesiology. 1983;58(5):399–404.
Lohser J, Slinger P. Lung injury after one-lung ventilation: a review of the pathophysiologic mechanisms affecting the ventilated and the collapsed lung. Anesth Analg. 2015;121(2):302–18.
Burrowes KS, Clark AR, Wilsher ML, Miline DG, Tawhai MH. Hypoxic pulmonary vasoconstriction as a contributor to response in acute pulmonary embolism. Ann Biomed Eng. 2014;42(8):1631–43.
Ishikawa S. Oxygenation may improve with time during one-lung ventilation. Anesth Analg. 1999;89(1):258–9.
Bund M, Henzler D, Walz R, Piepenbrock S, Kuhlen R. Aerosolized and intravenous prostacyclin during one-lung ventilation hemodynamic and pulmonary effects. Anaesthesist. 2004;53(7):612–20.
Cheng YD, Gao Y, Zhang H, , Duan CJ, Zhang CF. Effects of OLV preconditioning and postconditioning on lung injury in thoracotomy. Asian J Surg 2014;37(2):80–85.
Olivant FA, Husain K, Wolfson MR, Hubert TL, Rodriguez E, Shaffer TH, et al. Hyperoxia during one lung ventilation: inflammatory and oxidative responses. Pediatr Pulmonol. 2012;47(10):979–86.
Raghunathan K, Connelly NR, Robbins LD, Ganim R, Hochheiser G, DiCampli R. Inhaled epoprostenol during one-lung ventilation. Ann Thorac Surg. 2010;89(3):981–3.
Acknowledgements
Not applicable.
Funding
This work was supported by grants from The talents program of Jiangsu Cancer Hospital (YC201805), The program of Health Department of Jiangsu Province (BJ16028) and The program of Jiangsu Cancer Hospital (ZN201607).
Author information
Authors and Affiliations
Contributions
Lijun Wang, Pengyi Li and Lianbing Gu designed the study. Pengyi Li and Lianbing Gu contributed to manuscript writing and manuscript revision. Qingming Bian, Jing Tan and Dian Jiao collected the data. Fei Wu and Zeping Xu analyzed and interpreted the data. Lijun Wang critically reviewed, edited and approved the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All the participants were enrolled after written informed consent was obtained and this study was approval from the Ethics Committee of Nanjing Medical University according to the Helsinki Declaration. This randomised controlled clinical trial was registered at chictr.org.cn (identifier: ChiCTR1800017100).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, P., Gu, L., Bian, Q. et al. Effects of prostaglandin E1 nebulization of ventilated lung under 60%O2 one lung ventilation on patients’ oxygenation and oxidative stress: a randomised controlled trial. Respir Res 21, 113 (2020). https://doi.org/10.1186/s12931-020-01380-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-020-01380-6