
Abstract
Background
Chronic kidney disease (CKD) and hypertension are chronic diseases affecting a large portion of the population frequently coexistent and interdependent. The inability to produce/use adequate renal dopamine may contribute to the development of hypertension and renal dysfunction. The heterodimeric amino acid transporter LAT2/4F2hc (SLC7A8/SLC3A2 genes) promotes the uptake of L-DOPA, the natural precursor of dopamine. We examined the plausibility that SLC7A8/SLC3A2 gene polymorphisms may contribute to hypertensive CKD by affecting the L-DOPA uptake.
Methods
421 subjects (203 men and 218 women, mean age of 78.9 ± 9.6 years) were recruited and divided in four groups according to presence/absence of CKD, defined as reduced estimated glomerular filtration rate (eGFR < 60 ml/min/m2) calculated using the creatinine-based Berlin Initiative Study–1 (BIS1) equation, and to presence/absence of hypertension (systolic blood pressure ≥ 140 and/or diastolic blood pressure ≥ 90 mmHg). Subjects were analysed for selected SNPs spanning the SLC7A8 and SLC3A2 loci by Sequenom MassARRAY iPLEX platform.
Results
The most significant SNP at the SLC3A2 (4F2hc) locus was rs2282477-T/C, with carriers of the C-allele having a lower chance to develop hypertension among CKD affected individuals [OR = 0.33 (CI 0.14–0.82); p = 0.016]. A similar association with hypertensive CKD was found for the SLC7A8 (LAT2) rs3783436-T/C, whose C-allele resulted associated with decreased risk of hypertension among subjects affected by CKD [OR = 0.56 (95% CI 0.35–0.90; p = 0.017]. The two variants were predicted to be potentially functional.
Conclusions
The association between SLC3A2 and SLC7A8 variants to hypertension development in patients with renal failure could be linked to changes in L-DOPA uptake and consequently dopamine synthesis. Although the associations do not survive correction for Bonferroni multiple testing, and additional research is needed, our study opens new avenues for future basic and translational research in the field of hypertensive CKD.
Similar content being viewed by others


Background
The progressive decline of renal function that accompanies the physiological aging has received considerable attention as it is the leading risk factor for chronic kidney disease (CKD), a condition that can deteriorate further throughout life, potentially resulting in kidney failure or end-stage renal disease (ESRD) [1]. A measure of the kidney’s filtration ability widely used clinically to diagnose and stage CKD is decreased glomerular filtration rate (GFR), which can be estimated from the serum creatinine level (eGFRcrea). eGFR shows a strong heritable component, [2] and recent multi-ethnic genome-wide association studies (GWAS) and meta-analysis identified multiple genetic loci associated with CKD and eGFR, that can explain a portion, albeit, small, of the trait variance. [3, 4].
To date, a huge body of research has consistently found that loss of renal function is a strong risk factor for adverse clinical outcomes and increased mortality in the general population [5]. In particular, numerous evidence indicate that CKD is an important complicating factor for hypertension, a disorder that compromises cardiovascular health, and that is increasing in incidence and prevalence worldwide, becoming a major public problem [6]. The relationship between CKD and hypertension is reciprocal since hypertension is a strong determinant of worse renal function and decline in renal function frequently causes or exacerbates hypertension. This close interconnection is the result of multiple factors, including reduced nephron mass, increased sodium retention, endothelial dysfunction, and activation of hormones [7,8,9].
Dopamine is a natriuretic and diuretic hormone with an important paracrine/autocrine role in the kidney, affecting water and electrolyte balance. Increasing research indicate that the activation of intrarenal dopaminergic pathways, both for dopamine production and signalling, helps prevent or mitigate the development of hypertension, whereas defects in this system are linked to increased susceptibility to hypertension [10,11,12].
The major source of renal dopamine is derived from the decarboxylation of its precursor l-3, 4-dihydroxyphenylalanine (L-DOPA), which is taken up by proximal renal tubules from either the circulation or the glomerular filtrate and is then converted to dopamine by the aromatic L-amino acid decarboxylase (L-AADC), also localized to the renal tubules, the activity of which is upregulated by high-sodium diet and downregulated by low-salt diet [13, 14]. Cell uptake of L-DOPA, which may be the rate-limiting step in the synthesis of renal dopamine, is promoted mainly through the sodium independent and pH-sensitive L-type amino acid transporter type 2 (LAT2), which is present at both apical and basolateral membranes [15]. LAT2 is a non-glycosylated 12-transmembrane-spanning membrane protein, and a member of the solute carrier family 7 (SLC7) of amino acid transporters, coded by the SLC7A8 gene. Functional expression of LAT2 requires association with the 4F2 heavy chain antigen (4F2hc), also known as CD98, to form a heterodimer [16]. 4F2hc belongs to the solute carrier family 3 member 2 and is coded by the SLC3A2 gene. Consistent with a role of LAT2 in transporting L-DOPA, Wu et al. [17] demonstrated that by increasing the expression of SLC7A8 in tubular epithelial cells a corresponding increase in L-DOPA uptake was achieved. LAT2 has been also reported to be expressed at higher levels in renal cortex of spontaneously hypertensive (SHR) than in normotensive rats; its overexpression was associated with enhanced L-DOPA uptake and preceded the onset of hypertension [18, 19].
The impairment of renal dopaminergic system functionality in hypertension has been extensively studied at various levels both in human and in experimental animals [11, 20]. However, to our knowledge, no studies to date have examined the effect of genetic variants of SLC7A8 and SLC3A2 genes on the relationship between CKD and hypertension. Therefore, the purpose of this exploratory study is to addresses this knowledge gap by investigating this effect in a sample population of elderly subjects.
Methods
Study participants
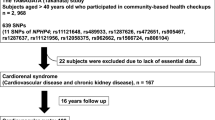
For this study we analysed 421 unrelated subjects (203 men and 218 women) whose ages ranged from 64 to 90 years. All subjects were born in Calabria (South Italy) and ancestry ascertained by requiring up to the grandparents' generation to be in the same region. Sample recruitment was undertaken across the whole territory through several recruitment campaigns carried out for monitoring the quality of aging in the whole Calabria region (21). The recruitment strategies consisted in contacting the family physicians and nursing home and examining population registers. Subjects who were eligible for the study were contacted and invited to participate in the study. Each subject underwent a medical visit carried out by a geriatrician who also conducted an interview including the administration of a structured questionnaire. The questionnaire collected socio-demographic information, evaluated physical and cognitive status, and self-reported health status. Subjects with cancer, dementia and/or neurologic disorders were not included. Before the visit, an informed consent was signed by each subject for the permission to collect blood samples and usage of register-based information for research purposes. The recruitment flow chart of the study participants is reported in the Additional file 1.
Biochemical measurements
At the time of enrolment, a peripheral blood sample was drawn after an overnight fast of 12 h in the morning for clinical and laboratory screening. Serum samples were immediately stored at -80 °C until assayed. The general laboratory panel included serum creatinine measured using the standardized Jaffe method calibrated to isotope dilution mass spectrometry using the automated analyser (RX-30, Nihon Denshi Inc., Tokyo, Japan).
Estimated Glomerular Filtration Rate Equation and blood pressure measurement
The GFR was estimated by the creatinine-based Berlin Initiative Study – 1 (BIS1) equation specially used to estimate GFR in older adults [22]. The equation was the following: eGFR BIS1 = 3736 × creatinine−0.87 × age−0.95 × 0.82 (if female).
Blood pressure was measured by a trained physician using a standard mercury sphygmomanometer. All measurements were performed three times after at least 5 min of rest from the left arm in a sitting posture.
Definition of study phenotypes
We defined a participant with CKD as an individual with eGFR < 60 mL/min/1.73m2 based on the BIS1 equation, and a participant with hypertension as an individual with elevated systolic blood pressure (SBP) or diastolic blood pressure (DBP) (SBP/DBP ≥ 140/90 mm Hg or taking antihypertensive medications). According to these criteria, study participants were categorised into one of four groups: [G1] healthy individual without CKD and hypertension (CKD-/Hyper-); [G2] individual without CKD and with hypertension (CKD-/Hyper +); [G3] individual with CKD and without hypertension (CKD + /Hyper-); [G4] individual with CKD and hypertension (CKD + /Hyper +).
Single nucleotide polymorphisms (SNPs) selection
SNPs within the SLC7A8 and SLC3A2 gens were selected based on a tagging approach to cover most of the genetic variability of these genes, using the Haploview Tagger Program software (https://www.broadinstitute.org/haploview/haploview, version 4.2). The criteria for the selection of tagging SNPs were minor allele frequency (MAF) higher than 0.05 and r2 higher than 0.8. A total of fifteen SNPs were selected for genotyping, eight of which were in the SLC7A8 gene and seven in the SLC3A2 genes. For each SNP, information related to the chromosome, position, minor allele frequency (MAF) detected in the control subjects of this study and in the 1000 Genomes TSI (Tuscany, Italy) population, and functional annotation of the SNP (missense, synonymous, intronic, and noncoding) is given in Additional file 2.
DNA extraction and genotyping
Genomic DNA was isolated from whole blood or buffy coats according to the salting out procedure.
Multiplex Genotyping was performed using the iPLEX assay on MassArray system (Sequenom Inc., San Diego, CA, USA). Sequenom MassARRAY Assay Designer software (version 3) was used to design primers for PCR and for single base extension against the candidate SNPs selected from analysis. PCR products were processed following the manufacturer’s instructions, and unincorporated nucleotides deactivated with the shrimp alkaline phosphatase (SAP). A primer extension reaction was then used to generate allele-specific products, which were subsequently desalted on resin and spotted onto the 384-element SpectroCHIP (Sequenom) for matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry analysis using SpectroACQUIRE v3.3.1.3 (Sequenom). The MassARRAY Typer v3.4 software (Sequenom). was used to call genotypes, and the individual spectrograms were inspected to check for calling errors.
To assess the reliability of the genotype identification protocols, about 10% of the analyzed samples were re-genotyped. For all SNPs polymorphisms concordance among duplicates was about 100%.
Quality Control
After genotyping, samples were subjected to a battery of quality control (QC) tests. At sample level, subjects with a proportion of missing genotypes higher than 10% were excluded from the analysis. At SNP level, SNPs were excluded if they had a missing frequency (MiF) higher than 20%, a minor allele frequency (MAF) lower than 5%, or a significant deviation from Hardy–Weinberg equilibrium (HWE, p < 0.05).
Statistical analysis
Continuous variables are expressed as mean ± SDs while categorical variables as percentages. Kolmogrov-Simirnov and Shapiro–Wilk tests were used to evaluate the normal distribution of the variables. One-way Analysis of Variance (ANOVA) with the Bonferroni post-hoc test, and chi-square test were applied to assess differences in biochemical, clinical, and anthropometric variables among groups, where appropriate. Allele and genotype frequencies were calculated by direct counting from the observed genotypes. HWE was tested by Fisher’s exact test. Odd ratios (OR) and 95% confidence interval (95% CI) based on logistic regression models were estimated to evaluate the effect of genotypes (independent variables) on the probability of belonging to different groups (dependent variable) including age and sex as covariates. For each SNP, data were coded with respect to a dominant, a recessive, and an additive model of inheritance. The dominant model compares homozygous carriers for the less common allele and heterozygous subjects (grouped together) with the group of homozygous for the more common allele. The recessive model compares individuals homozygous for the minor allele with the combined group of heterozygous and major allele homozygous carriers. The additive model assumes that there is a linear gradient in risk between the three genotypes. The most likely genetic model was estimated based on minimum level of statistical significance (Wald test p-value).
A conditional analysis was performed by including associated SNPs in the model to test their independent effect.
All statistical data were analyzed by the SPSS software version 28.0 (SPSS, Inc., Chicago, IL, USA). The significance level of the association test was set at 5%. Bonferroni correction was performed to correct for multiple comparisons, setting the significant P-value at 2E-04 for the genetic analyses (0.05/13*3*6, where 13 represents the number of SNPs analyzed, 3 represents the genetic models and 6 the number of comparisons as reported in Table 2.
Functional characterization of the single nucleotide polymorphisms
Several tools were used to investigate the functional effect of the associated SNPs. HaploReg v4.2 (https://pubs.broadinstitute.org/mammals/haploreg/haploreg.php) and RegulomeDB 2.2 (http://regulome.stanford.edu/) were used to investigate the potential influence of the SNPs on DNA regulatory elements. Specifically, HaploReg provides data in relation to the effect of the SNPs on chromatin state and regulatory motifs, while RegulomeDB provides a predictive score which reflect the probability for the SNP to be functionally active, and a rank score that depends on the amount of experimental evidence supporting the SNP to be functionally active. The rank ranges from 1 to 6 with a low score representing strong evidence of regulatory function. Genotype-Tissue Expression (GTEx) portal (https://gtexportal.org/home/) was interrogated to identify potential expression quantitative trait loci (eQTLs), which are genetic variants with an effect on gene expression levels.
Results
Characteristics of study subjects
The study population consisted of 421 subjects with a sex ratio of approximately 1:1 and a mean age of 78.9 ± 9.6 years. Overall, 59.14% had chronic kidney disease (CKD), defined by low eGFR (< 60 ml/min/m2), while 56.77% had hypertension, defined as systolic blood pressure ≥ 140 and/or diastolic blood pressure ≥ 90 mmHg. We divided the subjects into four phenotypic groups according to the presence/absence of CKD and/or hypertension. Group 1 included healthy individuals with no CKD and no hypertension (G1, CKD-/hyper-), group 2 persons without CKD with hypertension (G2, CKD-/hyper +), group 3 included persons with CKD without hypertension (G3, CKD + /hyper-), and group 4 persons with CKD and hypertension (G4, CKD + /hyper +).
The main demographic, clinical and biochemical characteristics of the whole sample are presented in Additional file 3, while Table 1 reports the characteristics of the four groups studied and the results of the comparisons among the four phenotypic groups.
With respect to individuals without CKD, both with and without hypertension, those with CKD, both with and without hypertension, were older. Also, there was a lower proportion of males in all groups compared to the proportion of males in the control (G1) group. Moreover, significant differences among groups in some disease-related quantitative metabolic variables were observed. As shown in Table 1 and as expected, the means for both systolic and diastolic blood pressure were found significantly higher in subjects with hypertension both with and without CKD, when compared with normotensive subjects. On the other hand, higher levels of creatinine, urea and uric acid were found among subjects with CKD, both hypertensive and normotensive when compared with the other groups. Finally, compared with the control group CKD + /hyper + subjects showed higher levels of triglycerides.
Genetic association of LAT2 and 4F2hc SNPs to chronic kidney disease and hypertension
The complete list of the selected SNPs is reported in Additional file 2. No deviations from HWE among the controls were observed, except for rs489381 (SLC3A2), rs1015089 (SLC7A8). Therefore, these two SNPs were excluded from further analysis.
The potential implication of the selected variants on the probability of belonging to a specific phenotypic group was tested by logistic regression analyses comparing each group with every other group. Results are summarized in Table 2.
After adjustments for age and sex, the most significant result at the SLC3A2/4F2hc locus was found at rs2282477-T/C. In particular, by comparing group G1 to group G4, that is the comparison between subjects with no CKD and no hypertension and subjects with CKD and hypertension, we observed a dominant genetic effect of rs2282477-C allele on the chance to belong to the G4 group with an odds ratio (OR) of 0.27 (CI 0.18–0.91; p = 0.035), meaning that that the presence of the minor allele C associates with reduced chance to have both CKD and hypertension in comparison to healthy controls. For rs2282477 in SLC3A2/4F2hc we also found association in a dominant model when comparing group G3 to group G4, that is the comparison between CKD subjects without versus those with hypertension, [OR = 0.33 (CI 0.14–0.82); p = 0.016]. This means that among CKD affected individuals, those carrying the rs2282477-C allele have a lower chance to develop hypertension relative to homozygotes for the T allele. A similar result was found for the marker of SLC7A8/LAT2 rs3783436-T/C, whose minor allele C resulted associated with reduced risk of hypertension when the G3 group was compared to the G4 in an additive model [OR = 0.56 (95% CI 0.35–0.90; p = 0.017]. It should be noted, however, that these associations did not meet the Bonferroni correction threshold for multiple testing (pcorrected = 0.0002). No associations were identified in the other comparisons.
To test whether the two SNPs (rs2282477 and rs3783436) have independent effect when considered together, we performed a conditional logistic regression analysis of each SNP with the other SNP as covariate and adjusting for age and sex. This analysis showed that the significant association of rs3783436 with the chance to belong to the G4 phenotype (comparison G3 versus G4) disappeared (p > 0.1) after adjusting for rs2282477, which is consistent with a non-independent effect of the two SNPs.
Possible functional effects
The rs2282477 lies in the 3' untranslated region of 4F2hc gene while rs3783436 is located in intron 4 of LAT2 gene, so we checked whether there could be differences in gene expression due to these polymorphisms, to provide a rationale for the association found. To this aim, we used several online resources. First, we queried the Haploreg database for the presence of proxy SNPs in linkage disequilibrium (LD) (r2 > = 0.8) with these variants. Rs2282477 resulted not in LD with any other polymorphisms, while rs3783436 was in LD with 5 intronic SNPs in the same gene. Further analysis of these SNPs using Haploreg indicated that they are in regions of active chromatin, as indicated by a DNASE I hypersensitivity site. Data from RegulomeDB support these observations, as both SNPs showed a score of 1f, which indicates they are affecting different DNA regulatory elements and are linked to the expression of target genes. To gain more insight in the possible regulatory roles of rs2282477 and rs3783436 on gene expression, Genotype-Tissue Expression project database (http://www.gtexportal.org/home/) was used. For both variants, no eQTL effect in renal tissue is reported in GTEx portal. However, both SNPs were expression quantitative trait (eQTL) and splicing quantitative trait (sQTL) loci in multiple tissues and cell types. Rs2282477 was an eQTL for TMEM223 (Transmembrane Protein 223) gene in blood with a decreasing expression effect of the minor allele C. This variant was additionally demonstrated to represent a sQTL for SLC3A2 in several cultured cell lines with the C allele associated with significantly decreased intron excision ratios. As for the rs3783436, we found that the less common C allele increased the expression of SLC7A8 in several brain regions, and also resulted a sQTL of SLC7A8 with tissue-specific splicing effects of the genotypes.
Discussion
Chronic kidney disease (CKD) and hypertension are two common chronic diseases that often coexist and can have a bidirectional cause-effect relationship. Their coexistence has serious implications for human health increasing morbidity and mortality, especially from cardiovascular disease [23]. Several factors contribute to the concurrent presence of hypertension and kidney disease [24], including the contribution of a genetic component, as suggested by recent studies highlighting genes involved in both hypertension and kidney disease [25, 26]. In the present study, to increase the understanding of the genetic connection in between, we investigated the genetic variability of the SLC7A8/SLC3A2 genes, coding for the heteromeric transporter LAT2/4F2hc which mediates the cell-uptake of L-DOPA in kidney, in subjects stratified according to presence/absence of CKD and presence/absence of hypertension. CKD was evaluated by estimated glomerular filtration rate (eGFR) according to the BIS1 equation, the most reliable for assessing renal function in older white patients and reported to perform relatively better than other equations in older adults [22, 27, 28].
Although not holding Bonferroni correction for multiple testing, our results provided suggestive evidence,, that the minor alleles of two variants, rs2282477-C within SLC3A2/4F2hc- and rs3783436-C within SC7A8/LAT2, were nominally associated with lower odds of hypertension in presence of CKD. The two SNPs seems to have no independent effect in reducing the risk of hypertension, most likely reflecting the functional linkage of the two genes.
Both SNPs lie in non-coding regions, specifically rs2282477 in the 3'-UTR and rs3783436 in intron 4 of the respective genes, thus having no obvious direct effect on the structure and function of the affected proteins. The in-silico analysis showed that these variants could alter the binding ability of some specific transcription factors that could alter gene expression. According to the GTEx data, both polymorphisms act as eQTL and sQTL with different genotype effects across different cell types/tissues. In particular, the SLC3A2-rs2282477 was identified as a cis-eQTL for the gene TMEM223 in blood, with homozygous subjects for the protective C allele showing lower gene expression levels. TMEM223 encodes for an inner mitochondrial membrane protein involved in the assembly process of the mitochondrial- encoded COX-1 and required for the biogenesis of cytochrome c oxidase (complex IV) [29].
As for the rs3783436-C allele, eQTL analysis found it associated with increased expression of SLC7A8 mRNA in several brain regions. This is quite interesting considering that the brain and kidney act in concert to maintain normal body homeostasis by controlling sodium and water balance [30]. Unfortunately, no eQTL data from kidney tissue were available for these variants or their proxies in linkage disequilibrium. Nevertheless, based on available data, a plausible explanation for our results could be that an increase in LAT2 and/or 4F2hc gene expression owing to the presence of these genetic variants determines an increase of the uptake of L-DOPA and consequently of dopamine synthesis, which may lead decreased systemic blood pressure. This hypothesis is supported by Jacinto et al. [31], who reported reduced urinary dopamine/sodium excretion in some forms of human primary hypertension. Furthermore, hypertension has been reported in mice with intrarenal deletion of dopamine due to the aromatic L-amino acid decarboxylase (AADC) deficiency [32] or lacking dopamine receptors [33]. On the other hand, it has been reported that the expression of SLC7A8 is increased in renal tissue of spontaneously hypertensive rats [17,18,19], which might contribute to enhanced L-DOPA uptake and increased dopamine production. It is tempting to speculate that in this setting the increased expression of SLC7A8 may represent an adaptive compensatory mechanism, possibly caused by the deficiency in dopamine-mediated natriuresis, tending to limit the progressive rise blood pressure.
It is difficult, however, to establish a clear correlation between dopamine levels, LAT2/4F2hc expression, and the risk of hypertension in the context of CKD, even in view of the pleiotropic effects that dopamine and the SLC7A8/SLC3A2 genes exert. In fact, besides its important role in in helping to regulate blood pressure, dopamine enhances renal blood flow, an important determinant of glomerular filtration rate; low-dose dopamine represents a therapeutic choice to increase renal blood flow in patients, thus limiting or preventing renal failure [11]. Evidence shows that dopamine has also anti-inflammatory and antioxidant potential to prevent or ameliorate renal dysfunction [10, 11]. Mice with intrarenal dopamine deficiency have increased oxidative stress and inflammatory cells infiltration [32]. Furthermore, recent evidence has highlighted a relationship between the renal dopaminergic system and oxidative stress in the development of hypertension [20]. To this regard, it is worthwhile mentioning that rs2282477 SNP in SLC3A2 acts as a cis-eQTL to modulate the expression of the TMEM223 gene, which is involved in complex IV biogenesis whose dysfunction often leads to increased production of reactive oxygen species [29]. This suggests a plausible biological basis for the relationship among dopamine, oxidative stress, hypertension, and renal failure.
It is also worth noting that the LAT2/4F2hc complex, in addition to transport L-DOPA, also mediates the transport and reabsorption in proximal tubules of almost all neutral amino acids. Dysfunctions of this process may impact on maintaining amino acids concentration both in kidney and plasma [34]. This is of relevance considering the documented casual association of circulating amino acids with hypertension [35, 36] and with alteration in kidney function [37, 38]. For instance, glutamine, one of the amino acids transported by the LAT2/4F2hc complex, has been reported to significantly decrease kidney damage and improve kidney function by modulating oxidative stress and apoptosis in murine tubular epithelial cells [39].
We are aware that our work presents some limitations that merit consideration. First, the significance of our results did not survive correction for multiple testing. This is likely because the sample size within the subgroups is rather small, limiting statistical power to detect associations with likely moderate effects of SNPs. Since this is an exploratory study, findings must be interpreted with caution. Nevertheless, the results will be helpful for future confirmatory research conducted with larger population samples. A limitation is also that the consequences of these variants on gene expression in kidney is unknown and, hence, the biological mechanisms hypothesized to drive the associations are speculative. Further experimental studies are required to validate the findings. Lastly, considering that CKD includes various renal diseases, for future work, it would be interesting to consider whether the relationships we found differ according to specific kidney disorders.
Conclusions
In conclusion, our preliminary findings derived from a hypothesis-driven candidate gene study offers suggestive evidence to support the role of SLC3A2 /SLC7A8 function to the development of hypertension in patients with renal failure. This association most probably reflect important pleiotropic effects of both dopamine and SLC7A8/SLC3A2 genes. Given the prevalence and rising incidence rates of hypertensive CKD, understanding of pathogenic mechanisms and of potential determinants of these two associated conditions should be of utmost importance. Therefore, despite some limitations, we believe that our study has the important value of opening a novel avenue for future basic and translational research in the field of hypertensive CKD.
Availability of data and materials
The dataset supporting the conclusions of this article is included in Additional file 4.
Abbreviations
- 4F2hc :
-
4F2 heavy chain antigen
- AADC :
-
Aromatic L-amino acid decarboxylase
- BIS1 :
-
Berlin Initiative Study–1
- CD98 :
-
CD98 heavy chain
- CKD :
-
Chronic kidney disease
- COX-1 :
-
Cytochrome c oxidase I
- DBP :
-
Diastolic blood pressure
- eGFR :
-
Estimated glomerular filtration rate
- eGFRcrea :
-
Estimated glomerular filtration rate from creatinine
- eQTLs :
-
Expression quantitative trait loci
- ESRD :
-
End-stage renal disease
- GTEx :
-
Genotype-Tissue Expression
- GWAS :
-
Genome-wide association studies
- HWE :
-
Hardy–Weinberg equilibrium
- L-AADC :
-
L-Amino Acid Decarboxylase)
- LAT2 :
-
L-type amino acid transporter 2
- LD :
-
Linkage disequilibrium
- L-DOPA :
-
L-3, 4-dihydroxyphenylalanine
- MAF :
-
Minor allele frequency
- MALDI-TOF :
-
Matrix-assisted laser desorption/ionization-time of flight
- MiF :
-
Missing frequency
- PCR :
-
Polymerase chain reaction
- QC :
-
Quality control
- SBP :
-
Systolic blood pressure
- SHR :
-
Spontaneously hypertensive rats
- SLC3A2 :
-
Solute carrier family 3 member 2
- SLC7A8 :
-
Solute Carrier Family 7 Member 8
- SNPs :
-
Single nucleotide polymorphisms
- sQTL :
-
Splicing quantitative trait
- TMEM223 :
-
Transmembrane Protein 223
- TSI :
-
Tuscany Italy
- WKY :
-
Wistar-Kyoto rats
References
Denic A, Glassock RJ, Rule AD. The Kidney in Normal Aging: A Comparison with Chronic Kidney Disease. Clin J Am Soc Nephrol. 2022;17(1):137–9.
Arpegård J, Viktorin A, Chang Z, de Faire U, Magnusson PK, Svensson P. Comparison of heritability of Cystatin C- and creatinine-based estimates of kidney function and their relation to heritability of cardiovascular disease. J Am Heart Assoc. 2015;4(1): e001467.
Köttgen A, Pattaro C. The CKDGen Consortium: ten years of insights into the genetic basis of kidney function. Kidney Int. 2020;97(2):236–42.
Wuttke M, Li Y, Li M, Sieber KB, Feitosa MF, Gorski M, et al. A catalog of genetic loci associated with kidney function from analyses of a million individuals. Nat Genet. 2019;51(6):957–72.
Al-Aly Z, Zeringue A, Fu J, Rauchman MI, McDonald JR, El-Achkar TM, et al. Rate of kidney function decline associates with mortality. J Am Soc Nephrol. 2010;21(11):1961–9.
Tedla FM, Brar A, Browne R, Brown C. Hypertension in chronic kidney disease: Navigating the evidence. Int J Hypertens. 2011;2011(1):132405.
Ku E, Lee BJ, Wei J, Weir MR. Hypertension in CKD: Core Curriculum 2019. Am J Kidney Dis. 2019;74(1):120–31.
Tian Z, Liang M. Renal metabolism and hypertension Nat Commun. 2021;12:963.
Ameer OZ. Hypertension in chronic kidney disease: What lies behind the scene. Front Pharmacol. 2022;13: 949260.
Armando I, Villar VA, Jose PA. Dopamine and renal function and blood pressure regulation. Compr Physiol. 2011;1(3):1075.
Choi MR, Kouyoumdzian NM, Rukavina Mikusic NL, Kravetz MC, Rosón MI, Rodríguez Fermepin M, et al. Renal dopaminergic system: Pathophysiological implications and clinical perspectives. World J Nephrol. 2015;4(2):196–212.
Vaz de Castro PAS, Jose PA, Simões e Silva AC. Interactions between the intrarenal dopaminergic and the renin–angiotensin systems in the control of systemic arterial pressure. Clin Sci (Lond). 2022;136(16):120–7.
Hayashi M, Yamaji Y, Kitajima W, Saruta T. Aromatic L-amino acid decarboxylase activity along the rat nephron. Am J Physiol Renal. 1990;258:F28-33.
Seri I, Kone BC, Gullans SR, Aperia A, Brenner BM, Ballerman BJ. Influence of sodium intake on dopamine-induced inhibition of renal cortical Na+, K+-ATPase. Am J Physiol. 1990;258:F52–60.
Quinoñes H, Collazo R, Moe OW. The dopamine precursor L-dihydroxyphenylalanine is transported by the amino acid transporters rBAT and LAT2 in renal cortex. Am J Physiol Renal Physiol. 2004;287:F74-80.
Pineda M, Fernández E, Torrents D, Estévez R, López C, Camps M, et al. Identification of a membrane protein, LAT-2, that Co-expresses with 4F2 heavy chain, an L-type amino acid transport activity with broad specificity for small and large zwitterionic amino acids. J Biol Chem. 1999;274(28):19738–44.
Wu Y, Yin Q, Lin S, Huang X, Xia Q, Chen Z, et al. Increased SLC7A8 expression mediates L-DOPA uptake by renal tubular epithelial cells". Mol Med Rep. 2017;16(1):887–93.
Pinho MJ, Gomes P, Serrāo MP, Bonifācio MJ, Soares-da-Silva P. Organ-specific overexpression of renal LAT2 and enhanced tubular L-DOPA uptake precede the onset of hypertension. Hypertension. 2003;42:613–8.
Pinho MJ, Serrao MP, Gomes P, Hopfer U, Jose PA, Soares-da-Silva P. Over-expression of renal LAT1 and LAT2 and enhanced L-DOPA uptake in SHR immortalized renal proximal tubular cells. Kidney Int. 2004;66:216–26.
Qaddumi WN, Jose PA. The Role of the Renal Dopaminergic System and Oxidative Stress in the Pathogenesis of Hypertension. Biomedicines. 2021;9(2):139.
De Rango F, Montesanto A, Berardelli M, Mazzei B, Mari V, Lattanzio F, Corsonello A, Passarino G. To grow old in Southern Italy: a comprehensive Description of the old and oldest old in Calabria. Gerontology. 2011;57:327–34.
Schaeffner ES, Ebert N, Delanaye P, Frei U, Gaedeke J, Jakob O, et al. Two novel equations to estimate kidney function in persons aged 70 years or older. Ann Intern Med. 2012;157:471–81.
Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382:339–52.
Pugh D, Gallacher PJ, Dhaun N. Management of hypertension in chronic kidney disease. Drugs. 2019;79:365–79.
Kim HR, Jin HS, Eom YB. A Genome-Wide Association Study for Hypertensive Kidney Disease in Korean Men. Genes (Basel). 2021;12(5):751.
Zhang C, Fang X, Zhang H, Gao W, Hsu HJ, Roman RJ, et al. Genetic susceptibility of hypertension-induced kidney disease. Physiol Rep. 2021;9(1): e14688.
Koppe L, Klich A, Dubourg L, Ecochard R, Hadj-Aissa A. Performance of creatinine-based equations compared in older patients. J Nephrol. 2013;26:716–23.
Ma Y, Shen X, Yong Z, Wei L, Zhao W. Comparison of glomerular filtration rate estimating equations in older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2023;114: 105107.
Dennerlein S, Poerschke S, Oeljeklaus S, Wang C, Richter-Dennerlein R, Sattmann J, et al. Defining the interactome of the human mitochondrial ribosome identifies SMIM4 and TMEM223 as respiratory chain assembly factors. Elife. 2021;10: e68213.
Tanaka S, Okusa D. Crosstalk between the nervous system and the kidney. Kidney Int. 2020;97(3):466–76.
Jacinto SM, Lokhandwala MF, Jandhyala BS. Studies on the pharmacological intervention to prevent oxygen free radical mediated toxicity: effects of dopexamine, a DA1 receptor and β2-adrenoceptor agonist. Naunyn Schmiedebergs Arch Pharmacol. 1994;350:277–83.
Zhang MZ, Yao B, Wang S, Fan X, Wu G, Yang H, et al. Intrarenal dopamine deficiency leads to hypertension and decreased longevity in mice. J Clin Invest. 2011;121:2845–54.
Asico LD, Fuchs S, Accili D, Carey RM, Eisner GM, Jose PA. Disruption of the dopamine D3 receptor gene produces renin-dependent hypertension. J Am Soc Nephrol. 1997;8:295A.
Rossier G, Meier C, Bauch C, Summa V, Sordat B, Verrey F, et al. LAT2, a new basolateral 4F2hc/4F2hc-associated amino acid transporter of kidney and intestine. J Biol Chem. 1999;274(49):34948–54.
Poggiogalle E, Fontana M, Giusti AM, Pinto A, Iannucci G, Lenzi A, et al. Amino acids and hypertension in adults. Nutrients. 2019;11:1459.
Lin C, Sun Z, Mei Z, Zeng H, Zhao M, Hu J, et al. The causal associations of circulating amino acids with blood pressure: a Mendelian randomization study. BMC Med. 2022;20:414.
Duranton F, Lundin U, Gayrard N, Mischak H, Aparicio M, Mourad G, et al. Plasma and urinary amino acid metabolomic profiling in patients with different levels of kidney function. Clin J Am Soc Nephrol. 2014;9:37–45.
Mahbub MH, Yamaguchi N, Nakagami Y, Hase R, Takahashi H, Ishimaru Y, et al. Association of Plasma Branched-Chain and Aromatic Amino Acids with Reduction in Kidney Function Evaluated in Apparently Healthy Adults. J Clin Med. 2021;10(22):5234.
Thomas K, Zondler L, Ludwig N, Kardell M, Lüneburg C, Henke K, et al. Glutamine prevents acute kidney injury by modulating oxidative stress and apoptosis in tubular epithelial cells. JCI Insight. 2022;7(21): e163161.
Acknowledgements
We acknowledge co-funding from Next Generation EU, in the context of the National Recovery and Resilience Plan, Investment PE8 – Project Age-It: “Ageing Well in an Ageing Society”. This resource was co-financed by the Next Generation EU [DM 1557 11.10.2022].
The work has been made possible by the collaboration with Gruppo Baffa (Sadel Spa, Sadel San Teodoro srl, Sadel CSsrl, Casa di Cura Madonna dello Scoglio, AGI srl, Casa di Cura Villa del Rosario srl, Savelli Hospital srl,) and Casa di Cura Villa Ermelinda in the frame of the agreements TECNOLOGIE AVANZATE PER IL MIGLIORAMENTO DEI SERVIZI ALLA PERSONA and TECNOLOGIE AVANZATE PER L'INDAGINE DELLE RELAZIONI TRA UOMO ED AMBIENTI DI VITA.
Funding
This research was supported by “SI.F.I.PA.CRO.DE.–Sviluppo e industrializzazione farmaci innovativi per terapia molecolare personalizzata PA.CRO.DE.” PON ARS01_00568 granted by MIUR (Ministry of Education, University and Research) Italy to G.P.
Author information
Authors and Affiliations
Contributions
Conceptualization, G.R. and P.C.; methodology, P.C., S.D., RLG; formal analysis, G.R., and P.C.; writing—original draft preparation, G.R.; writing—review and editing, G.R., P.C., S.D., and G.P; funding acquisition, G.P. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the Declaration of Helsinki, and it was approved by the local Ethics Committee “Comitato Etico Regione Calabria-Sezione Area Nord” on 2017–10-31 (code n. 25/2017). A written informed consent was obtained from all participants included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Crocco, P., Dato, S., La Grotta, R. et al. Evidence for a relationship between genetic polymorphisms of the L-DOPA transporter LAT2/4F2hc and risk of hypertension in the context of chronic kidney disease. BMC Med Genomics 17, 163 (2024). https://doi.org/10.1186/s12920-024-01935-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12920-024-01935-2