
Abstract
Background
Mycobacteria are found in many environmental conditions and infect a variety of species, including rodents and rabbits. Guinea pigs are used experimentally as a model for Mycobacterium tuberculosis, but natural mycobacteriosis in guinea pigs has not been reported.
Case presentation
A 1.5-year-old female guinea pig was found acutely deceased with no premonitory illness. On gross post-mortem examination, multifocal to coalescing, raised, firm, pale tan nodules with discrete, irregular margins were noted over the surfaces of all lung lobes. Histopathology revealed nodules composed of clustered foamy macrophages and multinucleated giant cells containing numerous bacterial rods. Similar bacteria-laden macrophages were noted within sections of the liver, heart, palpebral conjunctiva, duodenum, and cecum. Polymerase chain reaction was performed on tissues collected during post-mortem examination. The 16S rRNA gene product was sequenced and was identical to the Mycobacterium genavense type strain.
Conclusions
To the best of the author’s knowledge, this report details the first documented case of Mycobacterium genvaense infection in a guinea pig and a follow up investigation of close-contact animals. Given their experimental susceptibility and this clinical case report, mycobacteriosis should be considered as a differential in guinea pigs exhibiting weight loss in the absence of other clinical signs. With the potential for zoonotic transmission in immunosuppressed individuals, precautions should be taken to safeguard human health in cases of guinea pigs with suspected M. genavense infection.
Similar content being viewed by others


Background
Mycobacteria are aerobic, non-sporulating bacteria found in many environmental conditions, and these bacteria infect various species, including humans [1,2,3]. Rodents and rabbits can be essential reservoirs of transmission of mycobacteria between wildlife, domestic animals, and humans [4]. Guinea pigs are used experimentally as a human model for M. tuberculosis; however, natural mycobacteriosis has yet to be reported in this species. The following report details the first documented case of Mycobacterium genavense infection in a guinea pig and follow-up investigation of two conspecific guinea pigs and two close-contact domestic pigeons.
Case presentation
A 1.5-year-old female guinea pig (case 1), Cavia porcellus, housed in a zoo was found deceased with no premonitory illness. This individual was part of a public education program, was acquired one year prior from a local rescue organization and lived with two clinically healthy female conspecifics.
Despite a normal appetite, case 1 lost 60 g of body weight (4.6%) over three weeks prior to death based on medical records. On gross examination, over the surfaces of all lung lobes and extending into the parenchyma multifocal to coalescing, raised, firm, pale tan nodules with discrete, irregular margins were observed (Fig. 1). Histopathology revealed nodules composed of clustered foamy macrophages containing numerous bacterial rods. Similar bacteria-laden macrophages were noted within sections of the liver, lungs, heart, palpebral conjunctiva, duodenum, and cecum. The bacterial rods stained strongly with Giemsa, periodic acid-Schiff, and Fite's acid-fast stains, whereas, weakly stained with Ziehl–Neelsen acid-fast stain (Fig. 2). Histology sections were examined using a conventional light microscope (Olympus BX51) equipped with a digital camera (Olympus DP26) and cellSens Standard image analysis software (Olympus, Center Valley, PA 18,034, USA). The spleen and peripheral lymph nodes were considered normal on gross examination and were not examined histologically. Due to high suspicion for mycobacteriosis, a nested polymerase chain reaction (PCR) was performed, first using primers Mb246 and MbR247 with the product from the first amplification used as a template for the second round with primers Mb1 and MbR7 [5]. The product was sequenced using the nested amplification primers. The 16S rRNA gene sequence was 100% identical to 14 strains of M. genavense, including the type strain 2289 identified using a BLAST search of the GenBank database. The next closest match was with Mycobacterium florentinum at 98.7%. Because M. genavense is considered an opportunistic zoonotic pathogen, educational programs with the guinea pigs were ceased, and personal protective equipment (gloves and masks) was required for animal care staff working with the remaining guinea pigs [1].

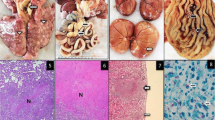
Gross image of post-mortem examination of guinea pig #1. Multifocal to coalescing, raised, firm, pale tan nodules with discrete, irregular margins were noted throughout all lung lobes during the post-mortem examination of guinea pig #1

Histologic image from post-mortem examination of case #1. A Pulmonary parenchyma and pleura are infiltrated and expanded by inflammatory nodules consisting of macrophages, multinucleated giant cells, lymphocytes, and plasma cells. The dashed line delineates the transition between healthy pulmonary parenchyma and a pulmonary lesion at the top of the image. Hematoxylin and eosin (H&E) stain. 4 × magnification. Scale bar represents 300 microns. B Intralesional macrophages (arrow) contain basophilic, rod-shaped bacteria. H&E stain. 40 × magnification. C Macrophages (insert) laden with acid-fast staining bacteria. Fite's acid-fast stain. 40 × magnification. Histology sections were examined using a conventional light microscope (Olympus BX51) equipped with a digital camera (Olympus DP26) and cellSens Standard image analysis software (Olympus, Center Valley, PA 18034, USA). Images were acquired at 300 dpi resolution and were edited for scale bar and white balance in Photoshop 23.1.1 (Adobe, San Jose, CA 95110, USA)
Physical exams and whole-body computed tomography scans were performed on the two conspecific guinea pigs to screen for pulmonary granulomas. Physical examinations were unremarkable. Computed tomography (CT) scans were acquired at a slice thickness of 1 mm, with 139 mA and 120 kV. The raw data were reconstructed in a soft and sharp kernel. Case 2 was anesthetized using isoflurane (Fluriso, MWI Animal Health, Boise ID 83,705 USA) via facemask for induction and maintenance, and the CT scan revealed suspected atelectasis of the entirety of the pulmonary parenchyma within the right hemithorax. To reduce interference with pulmonary atelectasis, CT scans were repeated with the patient awake in a plexiglass chamber (30 cm × 11 cm × 11 cm) approximately one and three hours following the first scan. Both subsequent scans of case 2 revealed focal areas of well-defined, irregular, consolidation of the right pulmonary parenchyma, in the dorsal aspect of the right cranial and right middle lung lobes (Fig. 3). There was no evidence or clinical signs of regurgitation noted. The CT scan of case 3 was performed awake in the same chamber to avoid atelectasis, and the pulmonary parenchyma was within normal limits.

Computed tomography image from case #2. Transverse image at the level of the mid-scapula (*). Within the dorsal aspect of the right cranial lung lobe there are areas of pulmonary consolidation with relatively well-defined margins. ( <) The patient is contained in a fitted box. Image displayed C:320 W2800. Slice thickness 0.69 mm, 120 kV, 139 mA. The pulmonary changes could represent mycobacteriosis as the pulmonary parenchyma was positive on PCR. The distribution of the consolidation, the timeframe of event, and the evolution of the consolidation on the repeat CT would not be considered usual for either aspiration pneumonia nor pulmonary atelectasis
Due to the history of mycobacterial infection in a conspecific and persistent changes within the pulmonary parenchyma identified via cross-sectional imaging, humane euthanasia was elected for case 2. It was re-anesthetized with isoflurane, blood was collected via cardiocentesis, and she was euthanized via intracardiac pentobarbital, and submitted for complete post-mortem examination and PCR of lung tissue for mycobacteria. Based on published reference intervals, a complete blood count (CBC) and chemistry panel were unremarkable [6]. Lung consolidation was noted on gross post-mortem examination. Histopathology revealed evidence of aspiration of gastric contents as well as pulmonary lymphoid hyperplasia (potentially a response to inflammatory disease). Lung tissue was submitted for Mycobacterium PCR, which was positive for Mycobacterium goodii (99.75%), a strain 93.87% homologous to Mycobacterium genavense.
Due to concern for early M. genavense infection, potential of zoonosis, and contagious spread to other public education animals, the third conspecific, case 3, was humanely euthanized in the same manner as case 2. A CBC and chemistry panel were performed, and results were unremarkable. Gross post-mortem examination was unremarkable. Lung tissue was submitted for Mycobacterium PCR and was negative.
Mycobacterium genavense has previously been reported in numerous avian species and is considered one of the most frequent etiologic agents of avian mycobacteriosis in pet birds [7,8,9,10,11,12,13]. Because the guinea pigs in this report were previously housed underneath two domestic pigeons, there was suspicion that the pigeons were a potential source of M. genavense. Pooled fecal material from the pigeons was submitted for PCR sequencing, and the result was negative. Because two guinea pigs had positive lung PCR results and the sensitivity of detecting mycobacterium in the stool samples was low, the two pigeons were euthanized for post-mortem examination and testing for evidence of M. genavense. There was no gross or histologic evidence of mycobacterial infection in either pigeon on postmortem examination. Initial PCR on the pigeon lung tissue revealed Actinomyces spp. in one and Mycobacterium gordonae in the other. Repeat PCRs were performed due to the possibility of contaminants causing false positive results, which were negative. It was concluded that these pigeons were likely not the source of mycobacteriosis in the guinea pigs. It is possible, however, that case 1 may have been harboring the infection upon arrival to the zoo as pre-shipment diagnostics such as bloodwork and imaging were not performed prior to arrival the previous year, and standard pre-shipment tests likely would not have identified a mycobacterial infection.
Discussion and conclusions
This is the first documented case of natural Mycobacterium genavense infection in a guinea pig. M. genavense infection has been reported in numerous small mammal species, including chinchillas, ferrets, rabbits, and squirrels, and avian species including doves, budgerigars, zebra finches, African penguins, and canaries, among others [7,8,9,10,11, 14,15,16,17,18].
Similarities between this and previously reported cases of Mycobacterium genavense infection in ferrets and a chinchilla include conjunctivitis, weight loss, and poor body condition [14, 15, 19]. In addition, infection with M. tuberculosis has been associated with weight loss in experimentally infected guinea pigs [20]. No organisms were detected via Ziehl–Neelsen acid-fast staining in case 2, which is similar to a ferret diagnosed with M. genavense [19]. While case 2 was positive on PCR, it also had evidence of aspiration and pulmonary inflammation; it is unknown if the positive M. goodii result was a false positive due to contamination, or evidence of true infection, since it was closely related to M. genavense. M. goodii is considered an emerging pathogen, commonly associated with nosocomial infections in humans [21, 22]. In animal species, M. goodii has been reported in canine patients, a leopard, as well as a spotted hyena with pyogranulomatous pneumonia [23,24,25,26].
Prior to presentation, the animals in this report were allowed to be in close contact with the public as educational ambassadors. For human health reasons, strict and thorough diagnostic procedures of close-contact animals, including full post-mortem examinations were performed, as false negative results from other diagnostics (i.e. skin testing, imaging, tracheal washes) would not be acceptable in this situation. In cases of non-tuberculosis mycobacterial pulmonary disease in humans, diagnosis depends on compatible clinical and radiographic findings along with positive sputum samples or positive culture results from bronchial lavage [27, 28]. Unfortunately, tracheobronchial lavage is not considered a routine procedure in guinea pigs due to their small size and laryngeal anatomy, limiting our diagnostic capabilities to non-invasive diagnostics such as CT [29]. While other non-invasive diagnostics, such as tuberculin skin testing, have been reported in guinea pigs for Mycobacterium tuberculosis in laboratory settings, the diagnostic sensitivity of this test is unreliable [30]. Further, while bacterial culture was not performed in these cases, culture of mycobacterial organisms could be considered as described in previous reports of M. genavense infections in animals [9, 31].
It was concluded that the pigeons in this report were likely not the source of mycobacteriosis in the guinea pigs. It is possible, however, that case 1 may have been harboring the infection upon arrival to the zoo as pre-shipment diagnostics such as bloodwork and imaging were not performed prior to arrival the previous year, and standard pre-shipment tests likely would not have identified an active mycobacterial infection. Future pre-shipment diagnostics to be considered include testing for anti-mycobacterial antibodies to evaluate for potential previous exposure to mycobacterial pathogens.
This is the first documented case of Mycobacterium genavense in a guinea pig, with a follow-up investigation unable to determine the source of infection. Mycobacteria can be found in the environment and incidentally in subclinical animals but can also cause severe disease and be difficult to diagnose antemortem. These characteristics made identifying the source of infection challenging. Mycobacteriosis should be included as a differential in guinea pigs presenting with weight loss despite lack of other clinical signs, especially with their high susceptibility to M. tuberculosis in experimental settings. Finally, given the potential for zoonotic transmission, precautions should be taken to safeguard health of immunocompromised humans in cases of suspected infection with M. genavense.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available in the GenBank repository, accession number OM760044.
Abbreviations
- CBC:
-
Complete blood count
- CT:
-
Computed tomography
- H&E:
-
Hematoxylin and eosin
- PCR:
-
Polymerase chain reaction
References
Bottger EC, Hirschel B, Coyle MB. Mycobacterium genavense sp. nov. Int J Syst Bacteriol. 1993;43(4):841–3.
Rastogi N, Legrand E, Sola C. The mycobacteria: an introduction to nomenclature and pathogenesis: -EN- -FR- -ES-. Rev Sci Tech. 2001;20(1):21–54. https://doi.org/10.20506/rst.20.1.1265.
Schrenzel MD. Molecular Epidemiology of Mycobacteriosis in Wildlife and Pet Animals. Vet Clin North Am Exot Anim Pract. 2012;15(1):1–23. https://doi.org/10.1016/j.cvex.2011.11.001.
McClure DE. Mycobacteriosis in the Rabbit and Rodent. Vet Clin North Am Exot Anim Pract. 2012;15(1):85–99. https://doi.org/10.1016/j.cvex.2011.11.002.
Carter IWJ, Schuller M, James GS, Sloots TP, Halliday CL, editors. PCR for Clinical Microbiology: An Australian and International Perspective. 10th ed. New York: Springer; 2010. https://doi.org/10.1007/978-90-481-9039-3.
Carpenter JW, Marion CJ. Exotic animal formulary. 5th ed. St. Louis (MO): Elsevier; 2018.
Haridy M, Fukuta M, Mori Y, Ito H, Kubo M, Sakai H, Yanai T. An Outbreak of Mycobacterium genavense Infection in a Flock of Captive Diamond Doves (Geopelia cuneata). Avian Dis. 2014;58(3):383–90. https://doi.org/10.1637/10775-011714-Reg.1.
Schmitz A, Korbel R, Thiel S, Worle B, Gohl C, Rinder M. High prevalence of Mycobacterium genavense within flocks of pet birds. Vet Microbiol. 2018;218:40–4. https://doi.org/10.1016/j.vetmic.2018.03.026.
Portaels F, Realini L, Bauwens L, Hirschel B, Meyers WM, de Meurichy W. Mycobacteriosis caused by Mycobacterium genavense in birds kept in a zoo: 11-year survey. J Clin Microbiol. 1996;34(2):319–23. https://doi.org/10.1128/jcm.34.2.319-323.1996.
Krause KJ, Reavill D, Weldy SH, Bradway DS. Mycobacterium genavense in an African penguin (Spheniscus demersus). J Zoo Wildl Med. 2015;46(4):971–5. https://doi.org/10.1638/2012-0205.1.
Ramis A, Ferrer L, Aranaz A, Liebana E, Mateos A, Dominguez L, Pascual C, Fdez-Garayazabal J, Collins MD. Mycobacterium genavense infection in canaries. Avian Dis Jan-Mar. 1996;40(1):246–51.
Bercovier H, Vincent V. Mycobacterial infections in domestic and wild animals due to Mycobacterium marinum, M. fortuitum, M. chelonae, M. porcinum, M. farcinogenes, M. smegmatis, M. scrofulaceum, M. xenopi, M. kansasii, M. simiae and M. genavense: -EN- -FR- -ES-. Rev Sci Tech. 2001;1:265–90. https://doi.org/10.20506/rst.20.1.1269.
Reavill DR, Schmidt RE. Mycobacterial Lesions in Fish, Amphibians, Reptiles, Rodents, Lagomorphs, and Ferrets with Reference to Animal Models. Vet Clin North Am Exot Anim Pract. 2012;15(1):25–40. https://doi.org/10.1016/j.cvex.2011.10.001.
Huynh M, Pingret J-L, Nicolier A. Disseminated Mycobacterium genavense Infection in a Chinchilla (Chinchilla lanigera). J Comp Pathol. 2014;151(1):122–5. https://doi.org/10.1016/j.jcpa.2014.03.003.
Lucas J, Lucas A, Furber H, James G, Hughes MS, Martin P, Chen SC, Mitchell DH, Love DN, Malik R. Mycobacterium genavense infection in two aged ferrets with conjunctival lesions. Aust Vet J. 2000;78(10):685–9. https://doi.org/10.1111/j.1751-0813.2000.tb10406.x.
Ludwig E, Reischl U, Janik D, Hermanns W. Granulomatous Pneumonia Caused by Mycobacterium genavense in a Dwarf Rabbit ( Oryctolagus cuniculus ). Vet Pathol. 2009;46(5):1000–2. https://doi.org/10.1354/vp.08-VP-0190-L-BC.
Theuss T, Aupperle H, Eulenberger K, Schoon H-A, Richter E. Disseminated Infection with Mycobacterium genavense in a Grizzled Giant Squirrel (Ratufa macroura) Associated with the Isolation of an Unknown Mycobacterium. J Comp Pathol. 2010;143(2–3):195–8. https://doi.org/10.1016/j.jcpa.2010.01.007.
Gomez G, Saggese MD, Weeks BR, Hoppes SM, Porter BF. Granulomatous encephalomyelitis and intestinal ganglionitis in a spectacled Amazon parrot (Amazona albifrons) infected with Mycobacterium genavense. J Comp Pathol. 2011;144(2–3):219–22. https://doi.org/10.1016/j.jcpa.2010.08.007.
Dequéant B, Pascal Q, Bilbault H, Dagher E, Boschiroli M-L, Cordonnier N, Reyes-Gomez E. Identification of Mycobacterium genavense natural infection in a domestic ferret. J Vet Diagn Invest. 2019;31(1):133–6. https://doi.org/10.1177/1040638718812137.
Clark S, Hall Y, Williams A. Animal Models of Tuberculosis: Guinea Pigs. Cold Spring Harb Perspect Med. 2014;5(5):a018572.
Salas NM, Klein N. Mycobacterium goodii: An Emerging Nosocomial Pathogen. Infect Dis Clin Pract (Baltim MD). 2017;25(2):62–5.
Shelton A, Giurgea L, Moshgriz M, Siegel M, Akselrod H. A case of Mycobacterium goodii infection related to an indwelling catheter placed for the treatment of chronic symptoms attributed to Lyme disease. Infect Dis Rep. 2019;11(2):8108. https://doi.org/10.4081/idr.2019.8108.
Bryden SL, Burrows AK, O’hara AJ. Mycobacterium goodii infection in a dog with concurrent hyperadrenocorticism. Vet Dermatol. 2004;15(5):331–8. https://doi.org/10.1111/j.1365-3164.2004.00383.x.
Krimer PM, Phillips KM, Miller DM, Sanchez S. Panniculitis attributable to Mycobacterium goodii in an immunocompetent dog in Georgia. J Am Vet Med Assoc. 2010;237(9):1056–9. https://doi.org/10.2460/javma.237.9.1056.
Gcebe N, Hlokwe TM. Non-tuberculous Mycobacteria in South African Wildlife: Neglected Pathogens and Potential Impediments for Bovine Tuberculosis Diagnosis. Front Cell Infect Microbiol. 2017;30(7):15. https://doi.org/10.3389/fcimb.2017.00015.
van Helden PD, van GeyPittius NC, Warren R, Michel A, Hlokwe T, Morar D, Godfroid J, du Plessis EC, Bengis R. Pulmonary infection due to Mycobacterium goodii in a spotted hyena (Crocuta crocuta) from South Africa. J Wildl Dis. 2008;44(1):151–4. https://doi.org/10.7589/0090-3558-44.1.151.
Anjos LRBD, Parreira PL, Torres PPTS, Kipnis A, Junqueira-Kipnis AP, Rabahi MF. Non-tuberculous mycobacterial lung disease: a brief review focusing on radiological findings. Rev Soc Bras Med Trop. 2020;11(53):e20200241.
Musaddaq B, Cleverley JR. Diagnosis of non-tuberculous mycobacterial pulmonary disease (NTM-PD): modern challenges. Br J Radiol. 2020;93(1106):20190768. https://doi.org/10.1259/bjr.20190768.
ArdiacaGarcía M, Montesinos Barceló A, BonvehíNadeu C, Jekl V. Respiratory Diseases in Guinea Pigs, Chinchillas and Degus. Vet Clin North Am Exot Anim Pract. 2021;24(2):419–57. https://doi.org/10.1016/j.cvex.2021.02.001.
Gao J, Guo M, Teng L, Bao R, Xian Q, Wang X, HO W. Guinea pig infected with Mycobacterium tuberculosis via oral consumption. J Appl Anim Res. 2018;46:1323–8. https://doi.org/10.1080/09712119.2018.1505622.
Kiehn TE, Hoefer H, Bottger EC, Ross R, Wong M, Edwards F, et al. Mycobacterium genavense infections in pet animals. J Clin Microbiol. 1996;34(7):1840–2.
Acknowledgements
We would like to acknowledge the animal care staff at Zoo Knoxville for their care of the animals described in this report.
Funding
No funding was provided for this manuscript.
Author information
Authors and Affiliations
Contributions
DJM was involved in case management and was a major contributor in preparing this manuscript. AA participated in the post-mortem examinations of the animals described in this report and provided Figs. 1 and 2. SK directed the microbiological analysis of samples described in this report. AMH directed the computed tomography scans and interpretations of the animals described in this report and provided Fig. 3. AC was involved in case management of the animals described in this report. DM was involved in manuscript preparation. JS directed case management of the animals described in this report, mentored DM in manuscript preparation, and was a major contributor to preparing the manuscript. All authors read, edited, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Minich, D.J., Agrawal, A., Kania, S.A. et al. Disseminated Mycobacterium genavense infection in a guinea pig (Cavia porcellus): a case report. BMC Vet Res 18, 93 (2022). https://doi.org/10.1186/s12917-022-03198-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12917-022-03198-4