
Abstract
Background
Evidence on the role of exogenous female sex steroid hormones in asthma development in women remains conflicting. We sought to quantify the potential causal role of hormonal contraceptives and menopausal hormone therapy (MHT) in the development of asthma in women.
Methods
We conducted a matched case–control study based on the West Sweden Asthma Study, nested in a representative cohort of 15,003 women aged 16–75 years, with 8-year follow-up (2008–2016). Data were analyzed using Frequentist and Bayesian conditional logistic regression models.
Results
We included 114 cases and 717 controls. In Frequentist analysis, the odds ratio (OR) for new-onset asthma with ever use of hormonal contraceptives was 2.13 (95% confidence interval [CI] 1.03–4.38). Subgroup analyses showed that the OR increased consistently with older baseline age. The OR for new-onset asthma with ever MHT use among menopausal women was 1.17 (95% CI 0.49–2.82). In Bayesian analysis, the ORs for ever use of hormonal contraceptives and MHT were, respectively, 1.11 (95% posterior interval [PI] 0.79–1.55) and 1.18 (95% PI 0.92–1.52). The respective probability of each OR being larger than 1 was 72.3% and 90.6%.
Conclusions
Although use of hormonal contraceptives was associated with an increased risk of asthma, this may be explained by selection of women by baseline asthma status, given the upward trend in the effect estimate with older age. This indicates that use of hormonal contraceptives may in fact decrease asthma risk in women. Use of MHT may increase asthma risk in menopausal women.
Similar content being viewed by others


Background
Asthma is a common heterogeneous respiratory disease affecting 1–18% of the population in different countries [1]. In 2019, asthma was estimated to affect approximately 262 million people and cause 461 thousand deaths worldwide, constituting a major global health burden [2]. For decades, age- and sex-related differences in asthma have been reported across different continents [3]. During childhood, asthma is more common in boys than in girls, while from around puberty onwards, it becomes more common in women than in men [3]. Compared to asthma that occurs in childhood, asthma that occurs in adulthood, which mainly affects women, is often more severe and has a faster decline in lung function and a poorer prognosis, representing a distinct clinical phenotype of asthma [4,5,6]. Because the switch in asthma occurs around the onset of puberty, sex steroid hormones (estrogens, progestogens and androgens) have been hypothesized to be implicated in the pathogenesis of adult-onset asthma [3, 7].
In parallel with the hypotheses, mechanistic studies suggest that female sex steroid hormones play an important role in asthma pathogenesis [3, 8]. Meanwhile, a number of epidemiologic studies have investigated the relation of hormonal contraceptives and menopausal hormone therapy (MHT) to the risk of new-onset asthma in adult women [3, 9]. Three cohort studies on hormonal contraceptives and new-onset asthma reported conflicting results [10,11,12]. An umbrella review [13] and a Danish register-based nested case–control study [14] reported an increased risk of new-onset asthma with MHT use in menopausal women, which, however, was contradicted by a UK national cohort study [15]. Overall, the evidence remains uncertain, mostly due to the concerns over potential systematic biases in most existing studies, such as selection bias, inadequate consideration of the full range of potential confounders, and, more essentially, lack of explicit causal reasoning [3, 9, 16, 17]. This makes it challenging, if not impossible, to establish whether the role of exogenous female sex steroid hormones in the development of asthma is causal [17, 18].
In the current study, we sought to determine the association between use of hormonal contraceptives and MHT and new-onset asthma in adult women, accounting for various sources of potential biases, in an attempt to assess whether this association is causal. In doing this, we used causal diagrams to represent and classify potential systematic biases and applied both Frequentist and Bayesian statistical models. The Bayesian model can incorporate our a priori background knowledge on the topic into the analysis and, compared to the conventional Frequentist analysis, is generally more robust to the size and the quality of the sample data [19, 20]. Our a priori hypotheses [3, 21] were that use of hormonal contraceptives, which suppresses the activities of endogenous female sex hormones, would reduce the risk of new-onset asthma, whereas use of MHT, which enhances the levels of endogenous female sex hormones, would increase the risk in menopausal women. To our knowledge, this is the first study that applies the Bayesian approach to investigate the causal role of exogenous female sex steroid hormones in the development of asthma in adult women.
Methods
This study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Additional file 1) [22]. We formulated the research questions according to the PECOS components (Population, Exposure, Comparator, Outcome, and Study design) [23].
Study population
The West Sweden Asthma Study (WSAS) is a population-based, longitudinal study established in West Sweden in 2008, which has been described in detail elsewhere [24]. At study baseline in 2008, the first questionnaire survey was sent to 30,000 randomly selected adults aged 16–75 years in western Sweden, of which 15,003 were women (out of which 9897 (66%) responded) (Fig. 1). Of the respondents, we excluded 1103 women who reported ever had asthma or ever diagnosed with asthma by a doctor. In 2016, the second questionnaire survey was sent to the remaining 8794 women, out of which 6295 (72%) responded. Of the respondents, 114 developed asthma during the 8-year follow-up. For use of hormonal contraceptives, the study population was based on all responding women, including 114 who had new-onset asthma and 6181 who had never had asthma by 2016. For use of MHT, the study population was restricted to 3641 women of menopausal age (\(\ge\) 45 years) at baseline, including 54 who had new-onset asthma and 3587 who had never had asthma by 2016.

Flow diagram for selection of participants in the study. Superscript lowercase letter a (a) indicates the following: in some matched strata, cases had less than 10 controls
Study design
In 2018–2020, the GA2LEN Women’s Questionnaire survey was sent to the 114 cases that had developed asthma during the 8-year follow-up to obtain information on hormonal exposures, out of which 72 (63%) responded. The 72 responding cases were individually matched to 602 controls, out of which 281 (47%) responded to the survey. The matching variables were exact age in years in 2008, place of residence (in or outside Gothenburg), and smoking status (never smoker, former smoker, or current smoker). The choice of a relatively high number of controls per case was to account for potential non-response among the controls. More details on individual matching are provided in Additional file 2 [3, 6, 9, 13, 17, 19, 24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91].
Hormonal exposures
The exposures of interest included ever use of hormonal contraceptives or MHT, which were reported by participants in the Women’s Questionnaire survey in 2018–2020. Use of hormonal contraceptives was measured by “Have you ever taken a treatment which contains hormones to stop you from getting pregnant (e.g., tablets, depot injection, hormonal coil)?” Use of MHT was measured by “Have you ever taken a treatment which contains hormones to reduce the symptoms or effects of menopause (e.g., ‘HRT’ tablets, depot injection, patches, gels, but not vaginal creams or pessaries)?” If participants answered “yes” to either question, they were further asked “How old were you when you first took the treatment?” The respective comparator group was never use of hormonal contraceptives or MHT.
New-onset asthma
Women who reported never having had asthma or doctor-diagnosed asthma during the first questionnaire survey in 2008 but later reported that they had asthma or doctor-diagnosed asthma during the second questionnaire survey in 2016 were considered as having developed new-onset asthma. Women who reported asthma were further asked “How old were you when you got asthma?”
Directed acyclic graphs
We used causal directed acyclic graphs (DAGs) to represent potential systematic biases in our study [30, 92]. Details on DAGs are provided in Additional file 2. For confounding bias, we identified potential common causes of each hormonal exposure and new-onset asthma based on previous literature (Additional file 2: Table S1); then, we applied the backdoor criterion to determine a sufficient set of adjustment variables required to minimize confounding (Additional file 2: Figs. S1 and S2) [26]. For use of hormonal contraceptives, the adjusted variables included age, place of residence, level of education, age at menarche, gynecological conditions (including endometriosis, polycystic ovarian syndrome, gynecological acne, and hysterectomy with or without oophorectomy), and tobacco smoking. For use of MHT, the adjusted variables included age, place of residence, level of education, body mass index, tobacco smoking, environmental tobacco smoke, age at menopause, physical exercise, and gynecological conditions. The definitions of the adjusted variables are summarized in Additional file 3 [93]. The DAGs for selection bias and measurement bias are respectively presented in Additional file 2: Figs. S3 and S4. Particularly, for many women, hormonal exposures happened before the study had started; if hormonal exposures had a causal effect on new-onset asthma, restricting the study population to those who had never had asthma at baseline would likely result in differential proportion of susceptible individuals after baseline, thereby introducing selection bias [27].
Statistical analyses
We developed a priori an analysis protocol including justifications for the statistical methods applied in this study (Additional file 2). In brief, for each hormonal exposure we applied Frequentist conditional logistic regression model to adjust for the matching sets and measured confounding variables [38, 49, 51]. We used multiple imputation (MI)—full-conditional specification (FCS) [44, 46]—to impute the missing data and fitted Frequentist conditional logistic regression model to the multiply imputed datasets (\(m=\) 100). Then, we conducted complete-case analysis as a sensitivity analysis, that is, restricting the analysis to individuals with complete data on all variables included in the model. The results were summarized as odds ratio (OR) with 95% confidence interval (CI). We conducted subgroup analyses by baseline age (above or below an age cut-off) to evaluate potential selection bias [94] and calculated E-value [69] to assess the robustness of the estimated causal effects to potential residual confounding.
We applied Bayesian conditional logistic regression model in the multiply imputed datasets (Additional file 2) [64, 66]. The Bayesian model approximated the posterior probability distributions over all possible values of the parameters of interest, conditional on the prior probability distributions, statistical model and observed data [58]. For parameters of hormonal exposure variables, we derived a priori original prior distributions (use of hormonal contraceptives: \(\mathrm{log}OR\sim N(-0.26,{0.20}^{2})\); use of MHT: \(\mathrm{log}OR\sim N(0.17,{0.13}^{2})\)), based on our previous review work [3, 9, 13] as well as newly published studies [11, 14, 15]. In addition, we set three alternative prior distributions to represent our uncertainty about the original prior distribution and used a flat prior distribution (which assigns equal prior plausibility to all possible values of a parameter) to understand the influence of our prior knowledge compared to that of the observed data on the model results [63]. The process of deriving the prior distributions is available in Additional file 4 [3, 10,11,12,13,14,15, 69]. Finally, we used the Markov chain Monte Carlo (MCMC) method to approximate the posterior distributions [64, 66] and calculated the median and the 95% central posterior interval (PI) on OR scale [68]. The 95% central PI means that, given the prior distributions, statistical model, and observed data, the true causal effect has a 95% probability of falling within this range [58]. We estimated the probability that each hormonal exposure would increase the risk of new-onset asthma in women [58].
As asthma is relatively rare in our study population (< 15% by the end of follow-up), the estimated ORs can be approximately interpreted as risk ratios [69]. All statistical analyses were performed using the R software (version 4.0.4) [95]. The R scripts and packages [45, 64, 69, 96,97,98,99,100,101,102,103,104,105,106] are available in Additional files 5 and 6.
Results
Characteristics of the study population
In total, 72 cases and 281 controls responded to the Women’s Questionnaire survey, among which 62 cases (86.1%) and 204 controls (72.6%) had ever used hormonal contraceptives. The median age when starting hormonal contraceptives was 18 years (range: 13–49 years). Thirty-five cases and 150 controls were aged 45 years or older at baseline, among which eight cases (22.9%) and 25 controls (16.7%) had ever used MHT. The median age of starting MHT was 52 years (range: 38–64 years). Forty-two of the 114 cases did not respond to the Women’s Questionnaire survey and were matched with additional 115 controls, resulting in a total of 114 cases and 717 controls. Tables 1 and 2 summarize the background characteristics for all cases and matched controls and for hormone users and never users, respectively. The median age of participants at baseline was 44 years (range: 19–74 years). Cases were more likely to have a BMI of \(\ge\) 30 kg/m2 and a higher level of education (although not statistically significant). Hormonal contraceptive users were more likely to be younger and have a lower BMI and a higher level of education, compared to never user. MHT users were more likely to have a lower BMI, be a former smoker, and live in Gothenburg city, compared to never user. The PECOS components, the results from complete-case analysis, and the MI process are detailed in Additional file 3. Below, we describe the results from both Frequentist and Bayesian analyses based on the multiply imputed datasets.
Use of hormonal contraceptives and new-onset asthma
Frequentist analysis
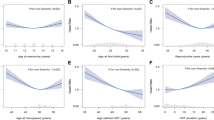
The effect estimate for asthma development with ever use of hormonal contraceptives compared to never use was OR 2.13 (95% CI 1.03–4.38) (Fig. 2a). Subgroup analyses that restricted to participants above a series of age cut-offs showed that the point effect estimate increased consistently with increasing baseline age: OR 2.07 (95% CI 1.00–4.28) among women aged \(\ge\) 25 years, 2.69 (95% CI 1.20–6.03) among \(\ge\) 35 years, 3.07 (95% CI 1.15–8.15) among \(\ge\) 45 years, 4.13 (95% CI 1.13–15.13) among \(\ge\) 55 years, and 4.98 (95% CI 0.63–39.36) among \(\ge\) 65 years. The magnitude of point estimate among women below an age cut-off remained consistently lower than that among those above that cut-off. The E-value for the point estimate among all women was 3.68, which meant that the observed OR of 2.13 could be explained away by unmeasured confounder(s) that were associated with both the exposure and the outcome by a risk ratio of 3.68-fold each, above and beyond the measured confounders, but weaker confounding could not do so.

Ever use of hormonal contraceptives (compared to never use) and new-onset asthma in women. a The results were from Frequentist conditional logistic regression. b Posterior probability distribution estimated from Bayesian conditional logistic regression, based on the original prior probability distribution \(\mathrm{log}OR\sim N(-0.26,{0.20}^{2})\) for use of hormonal contraceptives; the vertical bold line indicates the median of the posterior distribution, and the shaded area under the curve indicates the 95% central posterior interval. All analyses were conducted based on the multiply imputed datasets (\(m=\) 100), adjusted for age, place of residence, level of education, age at menarche, gynecological conditions and tobacco smoking. Abbreviations: CI, confidence interval; PI, posterior interval. Superscript lowercase letter a (a) indicates the following: age at baseline in 2008
Bayesian analysis
The posterior distribution for asthma development with ever use of hormonal contraceptives based on the original prior is presented in Fig. 2b. The median of the posterior distribution on OR scale was 1.11 (95% PI 0.79–1.55), and the probability of OR being larger than 1 was 72.3%. Prior sensitivity analysis using three alternative priors showed an upward shift in the median of the posterior distribution: OR 1.22 (95% PI 0.82–1.80), 1.35 (95% PI 0.86–2.12), and 1.51 (95% PI 0.91–2.51), respectively (Additional file 4: Table S1). The respective probabilities of OR being larger than 1 were 84.0%, 90.7%, and 94.4%. The posterior distribution based on flat priors on OR scale had a median of 2.17 (95% PI 1.08–4.64), and the probability of OR being larger than 1 reached up to 98.5%. Additional file 4: Fig. S5 illustrates and compares the posterior distributions based on the different prior distributions.
Use of MHT and new-onset asthma
Frequentist analysis
Among menopausal women, the effect estimate for asthma development with ever use of MHT compared to never use was OR 1.17 (95% CI 0.49–2.82) (Fig. 3a). Subgroup analyses by baseline age did not show any pattern in the point estimates. The E-value for the point estimate among all menopausal women was 1.62, which meant that the observed OR of 1.17 could be explained away by unmeasured confounder(s) that were associated with both the exposure and the outcome by a risk ratio of 1.62-fold each, above and beyond the measured confounders, but weaker confounding could not do so.

Ever use of menopausal hormone therapy (compared to never use) and new-onset asthma in menopausal women. a The results were from Frequentist conditional logistic regression. b Posterior probability distribution estimated from Bayesian conditional logistic regression, based on the original prior probability distribution \(\mathrm{log}OR\sim N(0.17,{0.13}^{2})\) for use of menopausal hormone therapy; the vertical bold line indicates the median of the posterior distribution, and the shaded area under the curve indicates the 95% central posterior interval. All analyses were conducted based on the multiply imputed datasets (\(m=\) 100), adjusted for age, place of residence, level of education, body mass index, tobacco smoking, environmental tobacco smoke, age at menopause, physical exercise and gynecological conditions. Abbreviations: CI, confidence interval; PI, posterior interval. Superscript lowercase letter a (a) indicates the following: age at baseline in 2008
Bayesian analysis
The posterior distribution for asthma development with ever use of MHT based on the original prior is presented in Fig. 3b. The median of the posterior distribution on OR scale was 1.18 (95% PI 0.92–1.52), and the probability of OR being larger than 1 was 90.6%. Prior sensitivity analysis using three alternative priors showed an increase in the width of the 95% PI: OR 1.18 (95% PI 0.87–1.60), 1.18 (95% PI 0.82–1.70), and 1.18 (95% PI 0.76–1.82), respectively (Additional file 4: Table S2). The respective probabilities of OR being larger than 1 were 86.2%, 81.6%, and 77.2%. The posterior distribution based on flat priors on OR scale had a median of 1.17 (95% PI 0.45–2.81), and the probability of OR being larger than 1 dropped down to 62.8%. Additional file 4: Fig. S10 illustrates and compares the posterior distributions based on the different prior distributions.
Discussion
Summary of key findings
In Frequentist analysis, ever use of hormonal contraceptives compared to never use was associated with an increased risk of new-onset asthma in women. Subgroup analyses showed that the association consistently became stronger among women of older age at baseline. Among menopausal women, ever use of MHT compared to never use was statistically non-significantly associated with an increased risk of new-onset asthma. In Bayesian analysis, although the 95% PIs for both use of hormonal contraceptives and MHT included the null value, there was a 72% and 91% probability that the OR was larger than one for hormonal contraceptives and MHT, respectively.
Strengths and limitations
There are several strengths in our study. First, being a case–control study nested within an ongoing prospective cohort, we could ascertain the temporality between the exposure and the outcome and thereby apply models to allow estimation of potential causal effects of exogenous female sex hormones on asthma risk. Second, we built causal DAGs based on published literature and our a priori subject-matter knowledge to identify potential confounding variables for each hormonal exposure [26, 30], which provides an explicit framework to minimize confounding. Third, in order to reduce the potential bias introduced by item non-response, we implemented MI to impute the missing data [39]. Fourth, we applied Bayesian statistical model which incorporated our prior background knowledge into the analysis; in this way, the current analysis provides a solid basis for future analyses. Finally, we adopted open and reproducible research practices [107]—we developed a priori statistical analysis protocol, documented in detail the research process, and made R scripts publicly available.
Certain limitations need to be taken into account in the interpretation of our findings. First, in our study, women with ever asthma at baseline were excluded, and for many women, hormonal exposures occurred before the study had started. This could have introduced selection bias, especially among older women, only if hormonal exposures had a causal effect on new-onset asthma (Additional file 2: Fig. S3) [27]. For example, if hormonal contraceptives increased the risk of new-onset asthma, the more susceptible individuals would have developed asthma before baseline in the exposed group than in the unexposed group; consequently, restricting to individuals who had not developed asthma by baseline would likely result in less susceptible individuals after baseline in the exposed group than in the unexposed group, thereby attenuating the magnitude of the effect estimate for the true harmful effect or even biasing the effect estimate towards the opposite direction [27]. Contrary to the hypothetical example, in our study, we found that when the age at baseline increased, the magnitude of point estimate for use of hormonal contraceptives consistently increased. We suspect that selection bias due to selection of women based on baseline asthma status may likely be the main explanation for the increase of the point estimate with increasing baseline age. This suggests that use of hormonal contraceptives may in fact have a protective effect on new-onset asthma, as opposed to a harmful effect indicated by our results. Notably, this type of selection bias may arise in any study that attempts to estimate the causal effect of an (lifetime) exposure that occurs before the study has started [27, 94, 108, 109]. Second, because some identified confounding variables were not available in our dataset, we had to rely on proxy variables (e.g., for socioeconomic status), or could not adjust for them at all (e.g., diet, alcohol) for use of MHT and new-onset asthma. Third, the information on hormonal exposures and asthma status was obtained retrospectively by questionnaire survey. Thus, an individual’s ability to recall their medical history may affect the measurement of both hormonal exposures and asthma (Additional file 2: Fig. S4) [92]. In addition, because hormonal exposures were ascertained by recall after asthma had occurred, asthma status might affect the recall of hormonal exposures. However, we expect that the influence was likely to be minimal (if present), because the causal relationship between asthma and hormonal exposures had not been well established. Fourth, more than half of the cases did not report age at asthma onset, which could potentially affect estimation of the temporal relationship between hormonal exposures and new-onset asthma. However, for the cases who reported age at asthma onset, asthma occurred after use of hormonal contraceptives or MHT. Fifth, although WSAS is a population-based study of a representative sample in western Sweden, given the baseline participation rate of 66% and the follow-up rate of 72%, potential selection bias (i.e., bias due to unit non-response) may have arisen, which could potentially affect the estimation of causal effects of exogenous female sex hormones on asthma risk as well as the generalization of our results to the source population. Unfortunately, we were unable to account for this type of bias in our study. Sixth, we could not investigate the potential varying causal effects of use of hormonal contraceptives and MHT by subtypes, doses, durations of use, and routes of administration, because the information on these factors could not be reliably determined from the questionnaire survey. Seventh, the study population for MHT use included women aged \(\ge\) 45 years at baseline, which was used as a proxy measure to identify menopausal women. Since it was not based on the actual menopausal status, this may affect the generalization of our results to the menopausal group of women. Finally, due to data unavailability, we were unable to address the potential modifying effect of BMI for the effects of exogenous female sex hormones on asthma risk.
Comparison to previous studies
To our knowledge [3], three cohort studies have investigated the causal effects of use of hormonal contraceptives on the risk of new-onset asthma, which excluded women with ever asthma at baseline to form the study population [10,11,12]. Interestingly, a similar upward trend existed in the effect estimate with increasing baseline age across or within studies (Additional file 7: Fig. S1 [10,11,12]). Likewise, we suspect that selection bias may likely explain the increase and the reversal of the relative risk with increasing baseline age.
Recently, an umbrella review including five cohort studies [13] and a nested case–control study based on the Danish registers [14] reported that use of MHT was associated with an increased risk of new-onset asthma in menopausal women. In contrast, a UK national cohort study [15], the largest longitudinal study on the topic to date, found that use of MHT was associated with a decreased risk of new-onset asthma and that longer duration of use was associated with a lower asthma risk than shorter duration. It is unclear whether different subtypes of MHT, population characteristics, or asthma phenotypes could explain the heterogeneity in these results.
Implications
First, despite intensive investigations, the epidemiologic evidence on female sex hormones and asthma risk remains equivocal [3, 9, 16]. Future longitudinal studies that account for systematic biases will help advance the evidence. This will benefit from making explicit the causal goals of research [17], and using causal diagrams (e.g., DAGs) to represent and classify systematic biases [25], which formulates a clearer framework for evaluating the proposed causal structures and analytical approaches, thus facilitating explicit causal reasoning of the results. Second, in studies of hormonal exposures that occur early in life (e.g., use of hormonal contraceptives), special attention needs to be paid to potential selection bias [27]. Indeed, for the upward trend in the effect estimate with increasing baseline age observed in our study and across previous studies, other explanations may include effect modification by age (i.e., use of hormonal contraceptives beneficial at younger ages but harmful at older ages) or residual confounding (i.e., the strength of residual confounding varied systematically across different age groups). Future studies that account for different systematic biases will hopefully provide further insights. Third, longitudinal studies that investigate the potential varying causal effects of use of hormonal contraceptives and MHT by subtypes, doses, durations of use, and routes of administration on various phenotypes of asthma are warranted. This can help generate evidence for more individualized asthma prevention strategies for women. Fourth, future studies are needed to investigate the potential modifying effect of BMI for the effects of exogenous female sex hormones on asthma risk. Notably, because BMI can arguably be a mediator along the causal pathway between hormonal contraceptives and new-onset asthma [80,81,82], future studies that carefully collect data on relevant key variables are warranted (e.g., physical activity, alcohol, stress, diet) (Additional file 7: Fig. S2).
Bayesian inference
The Bayesian framework naturally incorporates the investigators’ prior background knowledge about the parameters of interest before observing the data (i.e., prior beliefs) and updates these beliefs about the parameters after observing the data (i.e., posterior beliefs) [19]. This can help improve precision in effect estimate when the sample data is relatively small. For example, the incorporation of our prior knowledge from previous studies of use of MHT and asthma produced an effect estimate with substantially more certainty than that from only relying on the sample data. On the other hand, when the quality of the sample data is not optimal, the Bayesian method can help to some degree mitigate the influence of potential systematic biases on the results; in contrast, the Frequentist method relies only on the sample data and thus is highly dependent on data quality [19]. For example, the inclusion of our prior knowledge on use of hormonal contraceptives and asthma yielded a conservative result as opposed to that from Frequentist analysis; the wide spread of the posterior distribution means that more evidence is needed, which favorably kept us from making an overconfident claim that use of hormonal contraceptives would increase asthma risk in women. Furthermore, Bayesian analysis allows us to make intuitive probabilistic statements about the parameters [19, 110]. We can say that, for example, there was a 91% probability that ever use of MHT would increase asthma risk in menopausal women, conditional on the priors, statistical model and observed data. However, Frequentist estimates are often misinterpreted as Bayesian estimates [19]. A criticism of Bayesian analysis is that the priors are subjective [19]. However, it is noteworthy that this subjectivity creeps into both Frequentist and Bayesian analyses, where in Frequentist analysis, flat priors are implicitly assumed and may not always realistically capture a priori knowledge [19, 20]. The Bayesian framework makes explicit this aspect of subjectivity and uses different distributions to quantify this subjectivity [20].
Conclusions
Although use of hormonal contraceptives was associated with an increased risk of asthma, this may be explained by selection of women by baseline asthma status, given the upward trend in the effect estimate with older age. This indicates that use of hormonal contraceptives may in fact decrease asthma risk in women. Use of MHT may increase asthma risk in menopausal women.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to participant consent.
Change history
05 January 2024
The article was updated to fix omitted Peer Review information.
Abbreviations
- CI:
-
Confidence interval
- DAGs:
-
Directed acyclic graphs
- FCS:
-
Full-conditional specification
- MCMC:
-
Markov chain Monte Carlo
- MHT:
-
Menopausal hormone therapy
- MI:
-
Multiple imputation
- OR:
-
Odds ratio
- PECOS:
-
Population, Exposure, Comparator, Outcome, and Study design
- PI:
-
Posterior interval
- STROBE:
-
The Strengthening the Reporting of Observational Studies in Epidemiology
- WSAS:
-
West Sweden Asthma Study
References
Global Initiative for Asthma. Global strategy for asthma management and prevention. 2022. http://www.ginasthma.org.
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1204–22.
Zhang GQ, Özuygur Ermis SS, Rådinger M, Bossios A, Kankaanranta H, Nwaru B. Sex disparities in asthma development and clinical outcomes: implications for treatment strategies. J Asthma Allergy. 2022;15:231–47.
Honkamäki J, Piirilä P, Hisinger-Mölkänen H, Tuomisto LE, Andersén H, Huhtala H, et al. Asthma remission by age at diagnosis and gender in a population-based study. J Allergy Clin Immunol Pract. 2021;9:1950–9.
De Marco R, Locatelli F, Cerveri I, Bugiani M, Marinoni A, Giammanco G. Incidence and remission of asthma: a retrospective study on the natural history of asthma in Italy. J Allergy Clin Immunol. 2002;110:228–35.
Ilmarinen P, Tuomisto LE, Kankaanranta H. Phenotypes, risk factors, and mechanisms of adult-onset asthma. Mediators Inflamm. 2015;2015: 514868.
Chowdhury NU, Guntur VP, Newcomb DC, Wechsler ME. Sex and gender in asthma. Eur Respir Rev. 2021;30: 210067.
Keselman A, Heller N. Estrogen signaling modulates allergic inflammation and contributes to sex differences in asthma. Front Immunol. 2015;6:568.
McCleary N, Nwaru BI, Nurmatov UB, Critchley H, Sheikh A. Endogenous and exogenous sex steroid hormones in asthma and allergy in females: a systematic review and meta-analysis. J Allergy Clin Immunol. 2018;141:1510–3.
Wei J, Gerlich J, Genuneit J, Nowak D, Vogelberg C, von Mutius E, et al. Hormonal factors and incident asthma and allergic rhinitis during puberty in girls. Ann Allergy Asthma Immunol. 2015;115:21–7.
Nwaru BI, Pillinger R, Tibble H, Shah SA, Ryan D, Critchley H, et al. Hormonal contraceptives and onset of asthma in reproductive-age women: population-based cohort study. J Allergy Clin Immunol. 2020;146:438–46.
Troisi RJ, Speizer FE, Willett WC, Trichopoulos D, Rosner B. Menopause, postmenopausal estrogen preparations, and the risk of adult-onset asthma. A prospective cohort study. Am J Respir Crit Care Med. 1995;152:1183–8.
Zhang GQ, Chen JL, Luo Y, Mathur MB, Anagnostis P, Nurmatov U, et al. Menopausal hormone therapy and women’s health: an umbrella review. PLoS Med. 2021;18: e1003731.
Hansen ESH, Aasbjerg K, Moeller AL, Gade EJ, Torp-Pedersen C, Backer V. Hormone replacement therapy and development of new asthma. Chest. 2021;160:45–52.
Shah SA, Tibble H, Pillinger R, McLean S, Ryan D, Critchley H, et al. Hormone replacement therapy and asthma onset in menopausal women: national cohort study. J Allergy Clin Immunol. 2021;147:1662–70.
Sheikh A, Mukherjee M. We need a robust evidence base to unravel the relationship between sex hormones and asthma. Thorax. 2020;75:826–7.
Hernán MA. The C-word: scientific euphemisms do not improve causal inference from observational data. Am J Public Health. 2018;108:616–9.
Hernán MA, Robins JM. Chapter 3: Observational studies. In: Hernán MA, Robins JM. Causal Inference: What If. Boca Raton: Chapman & Hall/CRC. 2020.
Greenland S. Bayesian perspectives for epidemiological research: I. Foundations and basic methods. Int J Epidemiol. 2006;35:765–75.
Johnson AA, Ott MQ, Dogucu M. Bayes rules! An introduction to applied Bayesian modeling. 2021. https://www.bayesrulesbook.com.
Zhang GQ, Bossios A, Rådinger M, Nwaru BI. Sex steroid hormones and asthma in women: state-of-the-art and future research perspectives. Expert Rev Respir Med. 2020;14:543–5.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4: e296.
Morgan RL, Whaley P, Thayer KA, Schünemann HJ. Identifying the PECO: a framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int. 2018;121:1027–31.
Nwaru BI, Ekerljung L, Rådinger M, Bjerg A, Mincheva R, Malmhäll C, et al. Cohort profile: the West Sweden Asthma Study (WSAS): a multidisciplinary population-based longitudinal study of asthma, allergy and respiratory conditions in adults. BMJ Open. 2019;9: e027808.
Hernán MA, Robins JM. Chapter 6: Graphical representation of causal effects. In: Hernán MA, Robins JM. Causal Inference: What If. Boca Raton: Chapman & Hall/CRC; 2020.
Hernán MA, Robins JM. Chapter 7: Confounding. In: Hernán MA, Robins JM. Causal Inference: What If. Boca Raton: Chapman & Hall/CRC; 2020.
Hernán MA, Robins JM. Chapter 8: Selection bias. In: Hernán MA, Robins JM. Causal Inference: What If. Boca Raton: Chapman & Hall/CRC; 2020.
Hernán MA, Hernández-Díaz S, Robins JM. A structural approach to selection bias. Epidemiology. 2004;15:615–25.
Hernán MA, Robins JM. Chapter 18: Variable selection for causal inference. In: Hernán MA, Robins JM. Causal Inference: What If. Boca Raton: Chapman & Hall/CRC; 2020.
Hernán MA, Hernández-Díaz S, Werler MM, Mitchell AA. Causal knowledge as a prerequisite for confounding evaluation: an application to birth defects epidemiology. Am J Epidemiol. 2002;155:176–84.
Suttorp MM, Siegerink B, Jager KJ, Zoccali C, Dekker FW. Graphical presentation of confounding in directed acyclic graphs. Nephrol Dial Transplant. 2015;30:1418–23.
Shrier I, Platt RW. Reducing bias through directed acyclic graphs. BMC Med Res Methodol. 2008;8:70.
Williamson EJ, Aitken Z, Lawrie J, Dharmage SC, Burgess JA, Forbes AB. Introduction to causal diagrams for confounder selection. Respirology. 2014;19:303–11.
Pearl J. Causal diagrams for empirical research. Biometrika. 1995;82:669–710.
Hernán MA, Robins JM. Chapter 22: Target trial emulation. In: Hernán MA, Robins JM. Causal Inference: What If. Boca Raton: Chapman & Hall/CRC; 2020.
Textor J, van der Zander B, Gilthorpe MS, Liskiewicz M, Ellison GT. Robust causal inference using directed acyclic graphs: the R package ‘dagitty.’ Int J Epidemiol. 2016;45:1887–94.
Kleinbaum DG, Klein M. Chapter 11: Analysis of matched data using logistic regression. In: Kleinbaum DG, Klein M. Logistic Regression: A Self-Learning Text (Third Edition). New York: Springer Science+Business Media, LLC; 2010.
Rose S, Laan MJ. Why match? Investigating matched case-control study designs with causal effect estimation. Int J Biostat. 2009;5:Article 1.
White IR, Carlin JB. Bias and efficiency of multiple imputation compared with complete-case analysis for missing covariate values. Stat Med. 2010;29:2920–31.
Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338: b2393.
White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med. 2011;30:377–99.
Rubin DB. Multiple Imputation for Nonresponse in Surveys. New Jersey: Wiley; 1987.
van Buuren S. Chapter 5: Analysis of imputed data. In: van Buuren S. Flexible Imputation of Missing Data (Second Edition). Boca Raton: Chapman & Hall/CRC; 2018.
Seaman SR, Keogh RH. Handling missing data in matched case-control studies using multiple imputation. Biometrics. 2015;71:1150–9.
van Buuren S, Groothuis-Oudshoorn K. mice: multivariate imputation by chained equations in R. J Stat Softw. 2011;45:1–67.
Azur MJ, Stuart EA, Frangakis C, Leaf PJ. Multiple imputation by chained equations: what is it and how does it work? Int J Methods Psychiatr Res. 2011;20:40–9.
Moons KG, Donders RA, Stijnen T, Harrell FE Jr. Using the outcome for imputation of missing predictor values was preferred. J Clin Epidemiol. 2006;59:1092–101.
Mustillo S, Kwon S. Auxiliary variables in multiple imputation when data are missing not at random. J Math Sociol. 2014;39:73–91.
Pearce N. Analysis of matched case-control studies. BMJ. 2016;352: i969.
Kleinbaum DG, Klein M. Chapter 4: Maximum likelihood techniques: an overview. In: Kleinbaum DG, Klein M. Logistic Regression: A Self-Learning Text (Third Edition). New York: Springer Science+Business Media, LLC; 2010.
Wan F, Colditz GA, Sutcliffe S. Matched versus unmatched analysis of matched case-control studies. Am J Epidemiol. 2021;190:1859–66.
Mansournia MA, Hernán MA, Greenland S. Matched designs and causal diagrams. Int J Epidemiol. 2013;42:860–9.
Brookmeyer R, Liang KY, Linet M. Matched case-control designs and overmatched analyses. Am J Epidemiol. 1986;124:693–701.
Brenner H, Blettner M. Controlling for continuous confounders in epidemiologic research. Epidemiology. 1997;8:429–34.
Austin PC, Brunner LJ. Inflation of the type I error rate when a continuous confounding variable is categorized in logistic regression analyses. Stat Med. 2004;23:1159–78.
Persson E, Waernbaum I. Estimating a marginal causal odds ratio in a case-control design: analyzing the effect of low birth weight on the risk of type 1 diabetes mellitus. Stat Med. 2013;32:2500–12.
McElreath R. Statistical Rethinking: A Bayesian Course with Examples in R and Stan (Second Edition). Boca Raton: Chapman & Hall/CRC; 2020.
Muth C, Oravecz Z, Gabry J. User-friendly Bayesian regression modeling: a tutorial with rstanarm and shinystan. TQMP. 2018;14:99–119.
MacLehose RF, Hamra GB. Applications of Bayesian methods to epidemiologic research. Curr Epidemiol Rep. 2014;1:103–9.
Nicenboim B, Schad D, Vasishth S. Chapter 6: The art and science of prior elicitation. In: Nicenboim B, Schad D, Vasishth S. An introduction to Bayesian data analysis for cognitive science. 2023. https://vasishth.github.io/bayescogsci/book/ch-priors.html.
Mathur MB, VanderWeele TJ. Robust metrics and sensitivity analyses for meta-analyses of heterogeneous effects. Epidemiology. 2020;31:356–8.
Pullenayegum EM. An informed reference prior for between-study heterogeneity in meta-analyses of binary outcomes. Stat Med. 2011;30:3082–94.
Depaoli S, Winter SD, Visser M. The importance of prior sensitivity analysis in Bayesian statistics: demonstrations using an interactive Shiny app. Front Psychol. 2020;11: 608045.
Goodrich B, Gabry J, Ali I, Brilleman S. rstanarm: Bayesian applied regression modeling via Stan. R package version 2.21.1. 2020. https://mc-stan.org/rstanarm.
Lemoine NP. Moving beyond noninformative priors: why and how to choose weakly informative priors in Bayesian analyses. Oikos. 2019;128:912–28.
Zhou X, Reiter JP. A note on Bayesian inference after multiple imputation. Am Stat. 2012;64:159–63.
Zitzmann S, Hecht M. Going beyond convergence in Bayesian estimation: why precision matters too and how to assess it. Struct Equ Modeling. 2019;26:646–61.
Makowski D, Ben-Shachar MS, Lüdecke D. bayestestR: describing effects and their uncertainty, existence and significance within the Bayesian framework. J Open Source Softw. 2019;4:1541.
VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167:268–74.
Velentzis LS, Egger S, Banks E, Canfell K. Menopausal hormone therapy: characterising users in an Australian national cross-sectional study. PLoS ONE. 2021;16: e0253725.
Costanian C, Edgell H, Ardern CI, Tamim H. Hormone therapy use in the Canadian Longitudinal Study on Aging: a cross-sectional analysis. Menopause. 2018;25:46–53.
Manzoli L, Di Giovanni P, Del Duca L, De Aloysio D, Festi D, Capodicasa S, et al. Use of hormone replacement therapy in Italian women aged 50–70 years. Maturitas. 2004;49:241–51.
Nagel G, Lahmann PH, Schulz M, Boeing H, Linseisen J. Use of hormone replacement therapy (HRT) among women aged 45–64 years in the German EPIC-cohorts. Maturitas. 2007;56:436–46.
Skiba MA, Islam RM, Bell RJ, Davis SR. Hormonal contraceptive use in Australian women: who is using what? Aust N Z J Obstet Gynaecol. 2019;59:717–24.
Al SM. Awareness and use of contraceptives among Saudi women attending primary care centers in Al-Qassim. Saudi Arabia Int J Health Sci. 2010;4:11–21.
Costas L, Sequera VG, Quesada P, Altzibar JM, Lope V, Pérez-Gómez B, et al. Hormonal contraception and postmenopausal hormone therapy in Spain: time trends and patterns of use. Menopause. 2015;22:1138–46.
Parazzini F, Progetto Menopausa Italia Study Group. Trends of determinants of hormone therapy use in Italian women attending menopause clinics, 1997–2003. Menopause. 2008;15:164–70.
Lucas R, Barros H. Life prevalence and determinants of hormone replacement therapy in women living in Porto Portugal. Maturitas. 2007;57:226–32.
Lindh I, Hognert H, Milsom I. The changing pattern of contraceptive use and pregnancies in four generations of young women. Acta Obstet Gynecol Scand. 2016;95:1264–72.
Endalifer ML, Diress G, Addisu A, Linger B. The association between combined oral contraceptive use and overweight/obesity: a secondary data analysis of the 2016 Ethiopia Demographic and Health Survey. BMJ Open. 2020;10: e039229.
San-Juan-Rodriguez A, Bes-Rastrollo M, Martinez-Gonzalez MA, Martín-Moreno JM, Rico-Campà A, Gea A. Oral contraceptives use and development of obesity in a Mediterranean cohort: the SUN (Seguimiento Universidad de Navarra) Project. Int J Obes. 2020;44:320–9.
Ulhaq MZ, Pamungkasari EP, Murti B. Meta analysis: effect of oral contraceptives on obesity in fertile age women in Asia. J Matern Child Health. 2020;5:673–82.
Anderson DJ, Chung HF, Seib CA, Dobson AJ, Kuh D, Brunner EJ, et al. Obesity, smoking, and risk of vasomotor menopausal symptoms: a pooled analysis of eight cohort studies. Am J Obstet Gynecol. 2020;222:478.
Noll PRES, Campos CAS, Leone C, Zangirolami-Raimundo J, Noll M, Baracat EC, et al. Dietary intake and menopausal symptoms in postmenopausal women: a systematic review. Climacteric. 2021;24:128–38.
Canário AC, Cabral PU, Spyrides MH, Giraldo PC, Eleutério J Jr, Gonçalves AK. The impact of physical activity on menopausal symptoms in middle-aged women. Int J Gynaecol Obstet. 2012;118:34–6.
McAndrew LM, Napolitano MA, Albrecht A, Farrell NC, Marcus BH, Whiteley JA. When, why and for whom there is a relationship between physical activity and menopause symptoms. Maturitas. 2009;64:119–25.
Dąbrowska-Galas M, Dąbrowska J, Ptaszkowski K, Plinta R. High physical activity level may reduce menopausal symptoms. Medicina. 2019;55:466.
Sabia S, Fournier A, Mesrine S, Boutron-Ruault MC, Clavel-Chapelon F. Risk factors for onset of menopausal symptoms: results from a large cohort study. Maturitas. 2008;60:108–21.
Beasley R, Semprini A, Mitchell EA. Risk factors for asthma: is prevention possible? Lancet. 2015;386:1075–85.
Macsali F, Svanes C, Bjørge L, Omenaas ER, Gómez RF. Respiratory health in women: from menarche to menopause. Expert Rev Respir Med. 2012;6:187–200.
Hernán MA, Robins JM. Chapter 9: Measurement bias. In: Hernán MA, Robins JM. Causal inference: what if. Boca Raton: Chapman & Hall/CRC; 2020.
Hernán MA, Cole SR. Invited commentary: causal diagrams and measurement bias. Am J Epidemiol. 2009;170:959–62.
Coggon D, Rose G, Barker DJP. Chapter 8: Case-control and cross sectional studies. In: Coggon D, Rose G, Barker DJP. Epidemiology for the Uninitiated (Fourth Edition). 1997. https://www.bmj.com/about-bmj/resources-readers/publications/epidemiology-uninitiated/8-case-control-and-cross-sectional.
Hernán MA, Alonso A, Logroscino G. Cigarette smoking and dementia: potential selection bias in the elderly. Epidemiology. 2008;19:448–50.
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. 2021. https://www.R-project.org/.
Gabry J, Mahr T. bayesplot: plotting for Bayesian models. R package version 1.9.0.; 2022. https://mc-stan.org/bayesplot/.
Dogucu M, Johnson A, Ott M. bayesrules: datasets and supplemental functions from Bayes rules! R package version 0.0.2.900. 2021. https://github.com/bayes-rules/bayesrules.
Dowle M, Srinivasan A. data.table: extension of ‘data.frame’. R package version 1.14.2. 2021. https://CRAN.R-project.org/package=data.table.
Wickham H, François R, Henry L, Müller K. dplyr: a grammar of data manipulation. R package version 1.0.8. 2022. https://CRAN.R-project.org/package=dplyr.
Carstensen B, Plummer M, Laara E, Hills M. Epi: a package for statistical analysis in epidemiology. R package version 2.46. 2022. https://CRAN.R-project.org/package=Epi.
Harrison E, Drake T, Ots R. finalfit: quickly create elegant regression results tables and plots when modelling. R package version 1.0.4. 2021. https://CRAN.R-project.org/package=finalfit.
Wickham H. ggplot2: elegant graphics for data analysis. New York: Springer-Verlag; 2016.
Wickham H, Miller E. haven: import and export “SPSS”, “Stata” and “SAS” files. R package version 2.4.3. 2021. https://CRAN.R-project.org/package=haven.
Tierney N, Cook D, McBain M, Fay C. naniar: data structures, summaries, and visualisations for missing data. R package version 0.6.1. 2021. https://CRAN.R-project.org/package=naniar.
Wickham H, Bryan J. readxl: read Excel files. R package version 1.4.0. 2022. https://CRAN.R-project.org/package=readxl.
Stan Development Team. RStan: the R interface to Stan. R package version 2.21.5. 2022. https://mc-stan.org/.
Mathur MB, Fox MP. Toward open and reproducible epidemiology. Am J Epidemiol. 2023;192:658–64.
Stevens J, Cai J, Pamuk ER, Williamson DF, Thun MJ, Wood JL. The effect of age on the association between body-mass index and mortality. N Engl J Med. 1998;338:1–7.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–13.
Goodman SN, Fanelli D, Ioannidis JP. What does research reproducibility mean? Sci Transl Med. 2016;8:341ps12.
Acknowledgements
We would like to thank the participants for their valuable contributions in the study. We also thank Daniil Lisik, Helén Törnqvist, Helen Friberg, Lina Rönnebjerg, Louise Olausson, and Maryanne Raneklint at Krefting Research Centre for their assistance with data collection and/or the study flow diagram. We thank the anonymous reviewers for their constructive comments, which greatly improved the quality of this manuscript. GZ thanks the Frictionless Data for Reproducible Research Fellows Programme for the mentoring and support and the Stockholm University library for providing the inspiring study environment during the revision of the manuscript.
Funding
Open access funding provided by University of Gothenburg. GZ was supported by the VBG Group Herman Krefting Foundation on Asthma and Allergy, and Sahlgrenska Academy, University of Gothenburg, Sweden. MBM was supported by R01 LM013866, UL1TR003142, P30CA124435, and P30DK116074. BIN was supported by the VBG Group Herman Krefting Foundation on Asthma and Allergy, Knut and Alice Wallenberg Foundation, and the Wallenberg Centre for Molecular and Translational Medicine, University of Gothenburg, Sweden. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
BIN conceived the study. GZ and BIN collected the data. GZ and RB visualized and cleaned the data. GZ, RB, MBM, HK, and BIN developed the statistical analysis protocol. GZ, RB, and MBM wrote the R scripts. GZ performed the statistical analyses and drafted the initial manuscript. GZ, RB, MBM, CL, RM, LE, GW, MR, BL, HK, and BIN interpreted the results and critically revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the regional ethical board at the University of Gothenburg (DNR: 052/16, 906/16). Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Competing interests
MBM is a member of the research advisory boards of Sentience Institute and Greener by Default. All other authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
STROBE checklist for reports of case–control studies.
Additional file 2:
Table S1. Potential common causes of use of hormonal contraceptives or menopausal hormone therapy and new-onset asthma in women. Figure S1. A causal directed acyclic graph for potential common causes of use of hormonal contraceptives and new-onset asthma in women. Figure S2. A causal directed acyclic graph for potential common causes of use of menopausal hormone therapy and new-onset asthma in menopausal women. Figure S3. A causal directed acyclic graph for potential selection bias of hormonal exposures and new-onset asthma in women. Figure S4. A causal directed acyclic graph for potential measurement bias of hormonal exposures and new-onset asthma in women.
Additional file 3:
Section 1. Supplementary methods and results for the Frequentist analysis of hormonal contraceptives and new-onset asthma in women. Table S1. Background characteristics of the responded new-onset asthma cases and matched controls in WSAS in 2009–2016. Figure S1. Age distribution at baseline in 2008 among the responded women (N = 353). Figure S2. Age at first use of hormonal contraceptives in 261 women. Figure S3. Age at asthma diagnosis among 32 cases. Figure S4. Ever use of hormonal contraceptives (compared to never use) and new-onset asthma in women. Figure S5. Comparison between women who had data on the incomplete variables and those who did not with respect to auxiliary variables. Figure S6. Healthy convergence for the incomplete variables. Figure S7. The distribution of use of hormonal contraceptives in the observed data and in the m = 100 imputed datasets. Figure S8. Kernel density estimates for the marginal distributions of the observed data for age at menarche and the m = 100 densities calculated from the imputed data. Figure S9. The distribution of gynecological condition in the observed data and in the m = 100 imputed datasets. Figure S10. The distribution of level of education in the observed data and in the m = 100 imputed datasets. Figure S11. Odds ratios for ever use of hormonal contraceptives (compared to never use) and new-onset asthma among all women (N = 831) across the m = 100 imputed datasets. Section 2. Supplementary methods and results for the Frequentist analysis of menopausal hormone therapy and new-onset asthma in menopausal women. Figure S12. Age at first use of menopausal hormone therapy in 32 women. Figure S13. Age at asthma diagnosis among 13 cases. Figure S14. Ever use of menopausal hormone therapy (compared to never use) and new-onset asthma in menopausal women. Figure S15. Comparison between women who had data on the incomplete variables and those who did not with respect to auxiliary variables. Figure S16. Healthy convergence for the incomplete variables. Figure S17. The distribution of use of menopausal hormone therapy in the observed data and in the m = 100 imputed datasets. Figure S18. Kernel density estimates for the marginal distributions of the observed data for age at menopause and the m = 100 densities calculated from the imputed data. Figure S19. The distribution of physical exercise in the observed data and in the m = 100 imputed datasets. Figure S20. Kernel density estimates for the marginal distributions of the observed data for body mass index and the m = 100 densities calculated from the imputed data. Figure S21. The distribution of level of education in the observed data and in the m = 100 imputed datasets. Figure S22. The distribution of environmental smoke in the observed data and in the m = 100 imputed datasets. Figure S23. The distribution of gynecological condition in the observed data and in the m = 100 imputed datasets. Figure S24. Odds ratios for ever use of menopausal hormone therapy (compared to never use) and new-onset asthma among all menopausal women (N = 409) across the m = 100 imputed datasets.
Additional file 4:
Section 1. Supplementary methods and results for the Bayesian analysis of hormonal contraceptives and new-onset asthma in women. Table S1. Posterior estimates for the original and alternative priors for use of hormonal contraceptives and new-onset asthma in women. Figure S1. The original and alternative prior distributions. Figure S2. Posterior distributions estimated from each multiply imputed dataset (m = 100). Figure S3. Posterior distributions estimated from each Markov chain in the first imputed dataset. Figure S4. Trace plot from the first imputed dataset. Figure S5. Posterior distributions for the original and alternative priors. Section 2: Supplementary methods and results for the Bayesian analysis of menopausal hormone therapy and new-onset asthma in menopausal women. Table S2. Posterior estimates for the original and alternative priors for use of menopausal hormone therapy and new-onset asthma in menopausal women. Figure S6. The original and alternative prior distributions. Figure S7. Posterior distributions estimated from each multiply imputed dataset (m = 100). Figure S8. Posterior distributions estimated from each Markov chain in the first imputed dataset. Figure S9. Trace plot from the first imputed dataset. Figure S10. Posterior distributions for the original and alternative priors.
Additional file 5.
R scripts for use of hormonal contraceptives and new-onset asthma in women.
Additional file 6.
R scripts for use of menopausal hormone therapy and new-onset asthma in menopausal women.
Additional file 7:
Figure S1. Previous cohort studies on use of hormonal contraceptives and new-onset asthma in women. Figure S2. Simplified causal directed acyclic graphs to represent the role of body mass index for the effect of use of hormonal contraceptives on new-onset asthma in women.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, G., Basna, R., Mathur, M.B. et al. Exogenous female sex steroid hormones and new-onset asthma in women: a matched case–control study. BMC Med 21, 337 (2023). https://doi.org/10.1186/s12916-023-03038-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-023-03038-8