
Abstract
Recently, we reported the findings of a randomized controlled trial on the effectiveness of Stepping Stones Triple P (SSTP) compared to Care as Usual (CAU), in BMC Medicine. The study involved parents of 209 children with Borderline to Mild Intellectual Disability (BMID), included following a school-based assessment of psychosocial problems. We found that SSTP had some short-term advantages over CAU, i.e., a reduction of parenting stress and of teacher-reported psychosocial problems, but no long-term advantages, at 6 months after the intervention. Tellegen and Sofronoff criticized that we included a limited amount of studies on the effectiveness of SSTP, and that the interpretation of our findings was inadequate. Regarding available evidence, we confined our summary to published high-quality RCTs regarding individual SSTP on level 4 – our RCT concerned that type of SSTP. Consequently, many studies were excluded but in a very adequate way. Regarding interpretation, Tellegen and Sofronoff criticized that we compared SSTP with CAU, but seem to be unware that this is consonant with current guidelines. Moreover, they noted that 49% of the parents who started SSTP followed less than half of the intended number of sessions. However, our findings on those who completed SSTP showed no more advantages of SSTP in the long term than CAU. We therefore stick to our conclusion that SSTP has some advantages in the short term compared to CAU, but not in the long term. The major burden of psychosocial problems in children with BMID prompts for further improvements.
Please see related articles: http://www.biomedcentral.com/1741-7015/12/191 and http://www.biomedcentral.com/1741-7015/13/25
Similar content being viewed by others


Background
In a recent paper in BMC Medicine, we reported the findings of a randomized controlled trial (RCT) on the effectiveness of Stepping Stones Triple P (SSTP) compared to Care as Usual (CAU) [1]. We appreciate the comments of Tellegen and Sofronoff on this paper [2]. A public debate on the quality of research is the best way to optimize research on what really works for children with psychosocial problems. This is indeed essential to make progress in solving the societal challenge of a high burden of psychosocial problems among children, and holds even more for children with Borderline to Mild Intellectual Disability (BMID) [3,4].
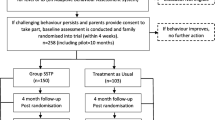
Our findings were based on an RCT, performed and reported following the CONSORT criteria for RCTs [5], and following the design as published in advance in a study protocol [6]. This RCT included 209 parents, 111 of whom were randomized to SSTP and 98 to CAU. In doing so, we followed the same procedure as in a previously published RCT on primary care Triple P (Triple P level 3), that showed no advantages of that variant of Triple P, compared to CAU [7,8]. Our findings were, first, that SSTP had some short-term advantages over CAU, but no long term advantages, i.e., at 6 months after the intervention [1]. Short-term advantages concerned parent-reported parenting stress and teacher-reported child psychosocial problems. Second, we found that 49% of parents dropped before completing at least five sessions, i.e., before half of SSTP [1].
Summary of evidence and interpretation
Tellegen and Sofronoff commented on two issues in particular: the fact that we included a limited amount of studies on the effectiveness of SSTP, and that we did not adequately interpreted our findings. We will respond to these issues consecutively. First, regarding the issue of the existing evidence, we confined the summary of studies in the introduction of our paper to published RCTs regarding individual SSTP on level 4, as our RCT concerned that type of SSTP. As a result, we only cited a limited number of studies. The review of Tellegen and Sanders [9] comprised mostly studies of poor quality. In our paper, we noted some problems associated with the poor quality of those studies, and refer to the extensive discussion of Wilson et al. on that topic [1,10], which had already been published shortly before the submission for publication of Tellegen and Sanders paper [9]. We thus adequately included only studies that fully met criteria regarding having a high-quality design.
Second, regarding our interpretation of the RCT outcomes, Tellegen and Sofronoff criticize two issues. First, they indicate that examination of the mean scores on the measures shows that the lack of long-term effects might be explained by outcomes in the CAU group continuing to improve over the follow-up period. They further indicate that, in contrast, the parents in the SSTP group maintained improvements that were seen at short-term, and hence both groups showed some improvement. These notions are fully consonant with our interpretation of the findings: SSTP may improve the outcomes of children and families somewhat, but in the long term, it does not do that in a better way than the routine Dutch CAU for children with psychosocial problems. SSTP thus has no advantages compared to CAU in the long term.
Tellegen and Sofronoff object to the comparison that we made in our RCT of SSTP with CAU. However, they seem not to unaware that this feature of our RCT reflects the gold standard of research on effectiveness, the CONSORT guideline: a new intervention should be compared to the best care that is available [5]. Withholding that care would lead to an invalid measurement of efficacy, and would also go against ethical guidelines: the control group cannot be withheld the routine care. The new intervention should then simply prove that it is better than routine care – which seems not to be the case in the longer run for SSTP.
As a second criticism regarding our interpretation, Tellegen and Sofronoff comment on the fact that, in our RCT, 49% of all parents followed less than half of the intended number of sessions, i.e., they dropped out before completing five sessions. That is a high percentage indeed, and it certainly requires additional study on its reasons. This drop out could be due to many of the included parents having perceived a need for parenting support, and thus provided consent to participate; however, in due course, they decided that SSTP did not adequately meet that need. More importantly, we did not find advantages in the long term compared to CAU for the 51% (i.e., 57) of parents who did complete SSTP adequately, nor did we find more advantages for these 57 parents in the short-term than we did for the full SSTP group. We will address the issue of a high drop-out in additional analyses because of its major importance.
Conclusions
In short, we highly appreciate the willingness of Tellegen and Sofronoff to enter the public debate on the effectiveness of SSTP, but we disagree on their critical reflection regarding the potential weaknesses of our RCT. This RCT, and the previously reported RCT on Primary Care Triple [8,10] have circumvented many of the weaknesses that have been noted regarding the previous research on the effectiveness of Triple P variants [1,10]. It concerned an adequately powered RCT which, compared with CAU (and not with a waiting list condition without care), used questionnaires that were not specifically developed for or used in the SSTP intervention, had an independent data collection process, i.e., parents were asked to complete questionnaires in the absence of the health care professional who was carrying out the intervention, and had a very high retention of participants in all measurements.
Our conclusion is that SSTP has some advantages in the short term compared to CAU, but not in the long term, at least in the Dutch setting. This requires further study, given the major burden of psychosocial problems in children with BMID, as well as for their parents and society.
Abbreviations
- BMID:
-
Borderline to Mild Intellectual Disability
- CAU:
-
Care as Usual
- RCT:
-
Randomized controlled trial
- SSTP:
-
Stepping Stones Triple P
References
Kleefman M, Jansen DEMC, Stewart RE, Reijneveld SA. The effectiveness of Stepping Stones Triple P parenting support in parents of children with borderline to mild intellectual disability and psychosocial problems: a randomized controlled trial. BMC Med. 2014;12:1–19.
Tellegen CL, Sofronoff K. Stepping Stones Triple P: the importance of putting the findings into context. BMC Med. 2015;13:25.
Kaptein S, Jansen DE, Vogels AG, Reijneveld SA. Mental health problems in children with intellectual disability: use of the Strengths and Difficulties Questionnaire. J Intellect Disabil Res. 2008;52:125–31.
Oeseburg B. Prevalence and impact of chronic diseases in adolescents with intellectual disability. PhD thesis. Groningen: University of Groningen; 2010.
Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaboration. Ann Intern Med. 2008;148:295–309.
Kleefman M, Jansen DEMC, Reijneveld SA. The effectiveness of Stepping Stones Triple P: the design of a randomised controlled trial on a parenting programme regarding children with mild intellectual disability and psychosocial problems versus care as usual. BMC Public Health. 2011;11:676–82.
Spijkers W, Jansen DEMC, de Meer G, Reijneveld SA. Effectiveness of a parenting programme in a public health setting: a randomised controlled trial of the positive parenting programme (Triple P) level 3 versus care as usual provided by the preventive child healthcare (PCH). BMC Public Health. 2010;10:131–6.
Spijkers W, Jansen DEMC, Reijneveld SA. Effectiveness of Primary Care Triple P on child psychosocial problems in preventive child healthcare: a randomized controlled trial. BMC Med. 2013;11:1–17.
Tellegen CL, Sanders MR. Stepping Stones Triple P-Positive Parenting Program for children with disability: a systematic review and meta-analysis. Res Dev Disabil. 2013;34:1556–71.
Wilson P, Rush R, Hussey S, Puckering C, Sim F, Allely CS, et al. How evidence-based is an ‘evidence-based parenting program’? A PRISMA systematic review and meta-analysis of Triple P. BMC Med. 2012;10:130–45.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors were involved in the evaluation of Stepping Stones Triple P and of Primary Care Triple P. They declare that they have no other competing interests.
Authors’ contributions
All authors assisted with the conceptualization, drafting, and editing of the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Reijneveld, S.A., Kleefman, M. & Jansen, D.E. Stepping Stones Triple P: the importance of putting the findings into context – a response to Tellegen and Sofronoff. BMC Med 13, 36 (2015). https://doi.org/10.1186/s12916-015-0289-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-015-0289-4