
Abstract
Background
The implementation of Electronic Health Record (EHR) systems is a critical challenge, particularly in low-income countries, where behavioral intention plays a crucial role. To address this issue, we conducted a study to extend and apply the Unified Theory of Acceptance and Use of Technology 3 (UTAUT3) model in predicting health professionals' behavioral intention to use EHR systems.
Methods
A quantitative research approach was employed among 423 health professionals in Southwest Ethiopia. We assessed the validity of the proposed model through measurement and structural model statistics. Analysis was done using SPSS AMOS version 23. Hypotheses were tested using structural equation modeling (SEM) analysis, and mediation and moderation effects were evaluated. The associations between exogenous and endogenous variables were examined using standardized regression coefficients (β), 95% confidence intervals, and p-values, with a significance level of p-value < 0.05.
Results
The proposed model outperformed previous UTAUT models, explaining 84.5% (squared multiple correlations (R2) = 0.845) of the variance in behavioral intention to use EHR systems. Personal innovativeness (β = 0.215, p-value < 0.018), performance expectancy (β = 0.245, p-value < 0.001), and attitude (β = 0.611, p-value < 0.001) showed significant associations to use EHR systems. Mediation analysis revealed that performance expectancy, hedonic motivation, and technology anxiety had significant indirect effects on behavioral intention. Furthermore, moderation analysis indicated that gender moderated the association between social influence, personal innovativeness, and behavioral intention.
Conclusion
The extended UTAUT3 model accurately predicts health professionals' intention to use EHR systems and provides a valuable framework for understanding technology acceptance in healthcare. We recommend that digital health implementers and concerned bodies consider the comprehensive range of direct, indirect, and moderating effects. By addressing personal innovativeness, performance expectancy, attitude, hedonic motivation, technology anxiety, and the gender-specific impact of social influence, interventions can effectively enhance behavioral intention toward EHR systems. It is crucial to design gender-specific interventions that address the differences in social influence and personal innovativeness between males and females.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The rise of information communication technology (ICT) globally has given rise to new markets in various industries, including automated health services. Consequently, the utilization of ICT in healthcare systems has been on the rise worldwide [1]. E-health, which refers to the application of ICT in healthcare provision, is crucial for strengthening the healthcare system [2]. One specific ICT solution is the EHR system, designed to capture, store, process, and display patient information [3]. The EHR system facilitates care quality monitoring, electronic alerts, and administrative tasks, thereby enhancing knowledge exchange and decision-making for healthcare professionals [4,5,6,7].
While many countries have invested tremendous effort in integrating e-health initiatives into their healthcare facilities, EHR usage is still lagging behind expectations [8]. The adoption of EHR systems especially in low-income nations remains remarkably low [9], with only 15% successfully implementing such systems [10]. Studies have identified factors contributing to the low adoption of EHR systems in the Sub-Saharan region, including high costs, unreliable power supply, limited internet access, and inadequate computer skills among primary healthcare providers [11, 12].
In Ethiopia, the Federal Ministry of Health (FMOH) has planned various ICT projects, including m-health, human resource information systems, and health management information systems (HMIS) [13]. While the FMOH has made progress in implementing the District Health Information System 2 (DHIS2) and Electronic Community Health Information System (eCHIS), the implementation of a nationwide EHR systems has faced challenges, particularly related to human factors like technical proficiency, negative beliefs, and lack of acceptance [14].
Understanding the factors influencing the adoption of EHR systems is crucial for successful implementation [15], particularly considering the significance of healthcare professionals' adoption behavior [9, 16,17,18]. While studies have been conducted in Ethiopia [19,20,21] and other developing countries [19,20,21,22,23,24,25,26,27,28,29,30] on the intention to use digital health initiatives, the factors influencing the intention to use EHR systems among healthcare providers have not been assessed using the extended UTAUT3 model.
Conducting this study in Ethiopia is crucial for examining the adoption of the EHR within a distinct healthcare context. The insights gained will inform the development of customized approaches for successful EHR implementation, not only in Ethiopia but also in similar resource-constrained settings worldwide. Extending the UTAUT3 model will deepen the understanding of factors influencing EHR adoption, potentially enabling improved predictions and guidance for researchers and digital health implementers in developing customized strategies. Therefore, this study aims to propose an alternative theoretical model, the extended UTAUT3 model, and examine the potential predictors of healthcare professionals' intention to use EHR systems based on this extended model. The study seeks to address the following research questions:
-
I)
How effective is our proposed model, the extended UTAUT3, in explaining the intention of healthcare professionals to use the EHR system?
-
II)
What are the potential factors that can predict the intention of healthcare professionals to use the EHR system, according to the extended UTAUT3 model?
Theoretical background and the proposed research model
Over the past few decades, there has been a noticeable focus on comprehending how newly introduced technologies will be adopted and embraced by end-users. This emphasis aims to predict levels of acceptance and address any resistance to change that may arise. To achieve these goals, several models have been developed, two of which have gained significant recognition: the Technology Acceptance Model (TAM) [31] and the UTAUT [32] model. The UTAUT model, in particular, has garnered considerable attention from researchers since its development, inspiring many to delve into its intricacies [23, 29, 33].
In the following subsections, we conducted a review of both the original and extended models of UTAUT and proposed a potential extension of the model for our study.
Unified theory of acceptance and use of technology (UTAUT)
The UTAUT model, originally formulated by Venkatesh et al., 2003 [32], is considered more comprehensive and predictive than earlier models. It was developed by integrating and synthesizing eight earlier models in the field. It initially consisted of four core constructs: effort expectancy, performance expectancy, social influence, and facilitating conditions. In addition, Venkatesh et al. considered four moderator variables such as age, gender, experience, and voluntariness of use in the original UTAUT model [32].
The four core constructs of the original UTAUT model were derived by merging constructs with similar behavior from the earlier eight models of technology acceptance and use. During this process, they identified five constructs perceived usefulness, extrinsic motivation, job fit, relative advantage, and outcome expectations from different models that exhibited similar behavior. These constructs were then integrated into the UTAUT model to explore the concept of effort expectancy [32].
The creators of the original UTAUT model also integrated three constructs perceived ease of use, complexity, and ease of use from the existing models to capture the concept of effort expectancy within the UTAUT model. Similarly, the concept of social influence was addressed by integrating three constructs from the existing models: subjective norm, social factors, and image. Furthermore, facilitating conditions were represented in the UTAUT model by integrating three distinct constructs: perceived behavioral control, facilitating conditions, and compatibility [32].
Extended theory of acceptance and use of technology (UTAUT2)
Venkatesh et al., 2012 [34] extended the UTAUT model to UTAUT2 by incorporating three additional constructs: hedonic motivation, price value, and habit. UTAUT2 demonstrated greater predictive power in explaining the intention to use new technologies compared to the original UTAUT model [32, 34]. The authors also made modifications to the model by considering age, gender, and experience of use as moderator variables, while dropping voluntariness as a moderator, to make the revised model more applicable to voluntary behavior.
The constructs of hedonic motivation, price value, and habit, which were incorporated into the UTAUT2 model, have distinct origins and were derived from different theoretical perspectives. While the concept of hedonic motivation traced back to the earlier concept of psychological hedonism, the significance of hedonic factors, such as enjoyment and pleasure, in shaping consumers' acceptance and use of technology was recognized by Childers et al. in 2001 [35]. The inclusion of the second construct, price value, in UTAUT2 was based on economic and rational decision-making theory [36], which emphasizes individuals' evaluation of the costs and benefits associated with adopting a technology.
The inclusion of the concept of "habit" in the UTAUT2 model was inspired by the understanding that people develop automatic patterns of behavior over time. This recognition was influenced by two perspectives: the Habit/Automaticity Perspective (HAP) [37] and the Instant Activation Perspective (IAP) [38] as highlighted by Venkatesh et al, 2012 [34]. The HAP suggests that habits formed through repeated actions can lead to automatic behavior, while the IAP views automatic use as a faster version of conscious use [37, 38].
Unified theory of acceptance and use of technology 3 (UTAUT3)
UTAUT3 was adapted from UTAUT2 by Farook et al., 2017 [25]. This model includes eight constructs: effort expectancy, performance expectancy, social influence, facilitating conditions, hedonic motivation, price value, habit, and a newly added variable called personal innovativeness [25]. The original UTAUT3 model was tested among business students in Malaysia and explained 58.1% of the variance in behavioral intention to use a lecture capture system [25].
The concept of personal innovation in information technology (IT) has long been acknowledged, with scholars like Agarwal and Prasad [39] recognizing its significance in technology adoption. Expanding on this, Farook et al., 2017 [25] extended the UTAUT model by incorporating personal innovativeness as a variable. Their empirical research aimed to provide insights into how personal innovativeness influences individuals' behavioral intentions and acceptance of technology, specifically focusing on the usage of a lecture capture system.
The proposed research model: identify constructs to extend and modify UTAUT3
Our research aimed to extend the UTAUT3 model by identifying additional constructs and modifying them to our specific research context. Building on previous studies that explored ways to expand the UTAUT model, such as introducing new variables and incorporating moderation and mediation mechanisms [26], we conducted a comprehensive literature review to address the limitations of previous UTAUT models. Our primary focus was on the intention to use, specifically excluding use behavior during the pre-implementation phase of EHR in our study area, as use behavior cannot be studied at this stage. Consequently, we extended the UTAUT3 model by incorporating additional constructs and making necessary adjustments. To achieve this, we drew upon the UTAUT3 model proposed by Farook et al. in 2017 [25] and refined it to better suit our research context.
To bridge the gap observed in the original UTAUT, UTAUT2, and UTAUT3 models, we conducted a comprehensive review of the literature that examined various extensions and theories associated with those models. Through this review, we identified individual behavioral factors and integrated them into our proposed model. In line with the TAM model [40], which considered attitude as a fundamental construct, and previous UTAUT extensions that utilized attitude as a mediating variable [21,22,23, 41,42,43,44], we incorporated attitude as a mediator variable in our study. While the original UTAUT model did not include attitude based on empirical findings [32], we argue that its exclusion does not necessarily invalidate its potential relevance as a mediator in specific research contexts.
By considering different theoretical perspectives [45] and our specific research context, we argue that including attitude as a mediator can provide a more comprehensive understanding of the underlying mechanisms involved in technology acceptance and use. We aimed to contribute to the existing literature by uncovering the specific psychological processes that drive individuals' decision-making and behavioral intention formation in technology adoption. This perspective aligns with the Cognitive Evaluation Theory (CET) proposed by Deci and Ryan [45], which emphasize the impact of perceptions on intrinsic motivation.
In our study, we propose including technology anxiety and digital technology self-efficacy as exogenous variables in the context of digital health technologies, building upon the findings of researchers who have extended the UTAUT models [27, 46]. Specifically, Guo et al., 2013 [42] recommended considering inhibiting factors in technology acceptance, with technology anxiety being one such factor. Additionally, previous studies have examined the impact of technology anxiety and technology self-efficacy in various domains of information system development [27, 46,47,48].
Technology anxiety initially recognized and explored by researchers and scholars in the fields of psychology and human–computer interaction, represents the fear or apprehension individuals may experience when using new technologies [48]. On the other hand, technology self-efficacy, introduced by psychologist Albert Bandura, refers to an individual's belief in their ability to successfully perform tasks using technology [49].
While price value was a construct in UTAUT2, we excluded it from our model based on the recommendation of a previous study [19], particularly when participants were not direct purchasers of the system. Even though UTAUT3 is the extension of UTAUT2, it doesn’t consider the moderation effect. We argue that including mediators and moderation can enhance the viability of the models, and therefore, we incorporated the moderator variables of the UTAUT2 model such as gender [7], age [7, 50], and experience [7].
Although UTAUT is not new, the specific UTAUT3 model has not been extensively tested in previous research, particularly in the context of digital health. Additionally, our extended version of UTAUT3 provides a foundation for future researchers examining the behavioral intention and acceptance of to use of new technology. By incorporating additional relevant constructs, our study addressed calls from scholars to enhance the applicability of the UTAUT model [34, 51, 52].
Overall, our study contributes to the theory of health information technology (HIT) use behavior by extending UTAUT3 after a comprehensive review of previous models and literature. Through this process, we introduced two exogenous variables, technology anxiety, and technology self-efficacy, and also the mediator variable of attitude, as well as moderation variables of the UTAUT2 model were introduced, to extend the recent UTAUT3 model by Farook et al., 2017 [25].
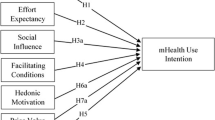
Overall, our extended model includes core constructs such as performance expectancy, effort expectancy, social influence, facilitating conditions, hedonic motivation, habit, technology self-efficacy, technology anxiety, and the mediator variable attitude. Furthermore, the model encompasses three moderator variables: age, sex, and experience. The hypotheses were developed based on a thorough review of existing literature and are supported by relevant studies, as summarized in Table 1. Figure 1 provides a visual representation of our proposed research model.

The proposed research model. NB: TSE = technology self-efficacy, EE = effort expectancy, PE = performance expectancy, PI = personal innovativeness, FC = facilitating condition, SI = social influence, HM = Hedonic motivation, TAN = technology anxiety, EHR = Electronic health record
Methods
Study design and setting
Between September 1 and October 14, 2022, a cross-sectional quantitative study was conducted at governmental hospitals in Illu Aba Bora and Buno Bedele Zones, which are situated in the Oromia regional state of southwest Ethiopia. Previously, the two zones were considered a single administrative zone, but they have since been demarcated separately. Mettu and Bedele are the respective capital cities of Illu Aba Bora and Buno Bedele, located approximately 600 km and 580 km away from Addis Ababa, the capital city of Ethiopia, respectively.
Study participants, sample size, and sampling procedure
The study population for this research consisted of all health professionals permanently working in the Illu Aba Bora and Buno Bedele zones in southwest Ethiopia. The sample size was calculated using a single population proportion formula, as follows:
In this study, a prevalence (P) of 50% (P = 0.5) was assumed for health professionals' behavioral intention to use EHR, as previous studies in a similar setting did not reveal the exact prevalence. The researchers also used a 95% confidence level (Z = 1.96) and a margin of error (d) of 5% (d = 0.05).
Based on these assumptions and the aforementioned formula, a sample size of 384 was calculated. To account for the expected non-response rate of 10%, the total sample size was increased by 10% of the initial sample size, resulting in a final total sample size of 423.
In Illu Aba Bora and Buno Bedele Zones, there were a total of five fully functional public hospitals, employing 1,398 healthcare providers. To ensure representation, the sample size of 423 was proportionally allocated among the five public hospitals. Subsequently, health professionals were randomly selected from each hospital to participate in the study.
Measurement instrument
Data collection was conducted using a self-administered questionnaire that had undergone pretesting. The questionnaire was specifically developed for this study, taking into consideration an extensive review of previous UTAUT models, theories, and studies conducted elsewhere [27, 43, 48, 55, 58, 59, 66, 69,70,71]. It consisted of three parts, with a total of 47 items. Part one assessed socio-demographic factors using five items. Part two focused on UTAUT-based behavioral predictors with 39 items. Part three addressed the behavioral intention to use EHR with three items (See Supportive file 1 for additional information).
Statistical analysis
For statistical analysis, the data were entered into EpiData version 4.6 and then exported to SPSS AMOS 23. Descriptive statistics, including frequencies and percentages, were used to summarize the variables. The assumptions of linearity and normality were checked and found to be fulfilled. Scatterplots were examined and tests such as the Shapiro–Wilk test were conducted to assess these assumptions. The results confirmed that the data exhibited a relatively linear pattern and approximated a normal distribution.
To ensure measurement validity, the outer loadings, cross-loadings, and item loadings of each item were assessed. The reliability of the measurement model was evaluated using Construct Composite Reliability (CR) and Cronbach's alpha (Cα) for each construct. Convergent validity was assessed using the Average Variance Extracted (AVE), while discriminant validity was examined using the Heterotrait-Monotrait Ratio (HTMT). Common method bias was evaluated using Harman's single-factor test. Multicollinearity between predictor constructs was checked using the Variance Inflation Factor (VIF).
To evaluate the structural model, R2, standardized estimates, and model fit indices were utilized. Model fit was assessed using indices such as the Root Mean Square of Standardized Residual (RMSEA), Adjusted Goodness of Fit Index (AGFI), Goodness of Fit Index (GFI), Comparative Fit Index (CFI), and Normal Fit Index (NFI). The associations between exogenous and endogenous variables, as well as significant moderation and mediation effects, were examined using standardized regression coefficients (β), 95% confidence intervals, and p-values with a significance level of p-value < 0.05.
The explanatory power of UTAUT2, UTAUT3, and the proposed model of Extended UTAUT3 were compared using R2. Statistical mediation analysis was employed to estimate the strength of mediator-outcome effects, while moderation analysis was used to observe whether moderator variables influenced the association between independent and dependent variables. In the analysis of the moderating effect of experience, experience was treated as a continuous variable to capture the potential variation in the relationship between predictors and the outcome variable as experience increases. Direct, indirect, and total effects were reported, and mean-centered values were used for moderation effect analysis.
Results
Socio-demographic characteristics
Out of the 423 respondents, 394 participants (93.1%) responded during the data collection period. The largest proportion of participants fell within the age range of 31 to 40 (49.5%), identified as male (67.8%), worked as nurses (30.9%), and held a degree (66.2%). Additionally, the majority of respondents (43.7%) reported having 6 to 10 years of experience (refer to Table 2).
Evaluating the measurement model
In the measurement model, we evaluated reliability, convergent validity, and discriminant validity. Reliability was assessed by examining the Construct Composite Reliability (CR) and the internal consistency reliability (Cα) for each construct. Our findings indicated that Cα values ranged from 0.727 to 0.94, while CR values ranged from 0.906 to 0.989. These values exceeded the suggested threshold of 0.7 [72] (Refer to Table 3).
We assessed convergent validity using the Average Variance Extracted (AVE). The AVE is calculated as the sum of the squared loadings divided by the number of indicators. Prior researchers in this field have suggested that a factor loading above 0.7 is generally considered sufficient for establishing convergent validity [73]. While a factor loading of 0.7 is commonly considered indicative of a strong association between indicators and constructs, it is widely accepted among scholars to use a cut-off point of 0.5 as acceptable [31, 74]. Therefore, we included indicators with factor loadings above 0.5 to ensure a comprehensive assessment of convergent validity. Items below this threshold were excluded to maintain the reliability and validity of the measurement model.
Based on Table 3, it can be inferred that the AVE values for all variables, except for effort expectancy, habit, and technology anxiety, were above 0.7. The AVE values for effort expectancy, habit, and technology anxiety were 0.685, 0.653, and 0.602, respectively, falling below the threshold of 0.7. However, these AVE values still demonstrate reasonable convergent validity according to the argument put forth by certain scholars, who stated that an AVE value above 0.5 might be acceptable [75, 76].
The concept of discriminant validity aims to assess the distinctiveness and individual existence of each unobservable latent variable [77]. This evaluation can be performed using criteria such as the Fornell-Larcker criterion and the HTMT method. Notably, recent studies have highlighted that the HTMT approach is a superior and more contemporary method [78]. When the HTMT value falls below 0.90, it indicates the presence of discriminant validity between two related constructs. As shown in Table 4, the HTMT values ranged from 0.208 to 0.864, which is below the recommended threshold for establishing discriminant validity [79].
Common method bias (CMB) arises when respondents' answers to behavioral, opinion, and perception measurements are influenced by their situation and context. In our study, we employed Harman's single-factor test [80] to examine the presence of CMB. The results of Harman's one-component test indicated a dispersion of 41.7%, which falls below the acceptable threshold of 50% for this test [80]. Based on these findings, we concluded that there was no evidence of CMB in our study.
To evaluate multicollinearity among predictor constructs, we conducted an assessment. The results indicated that all constructs had VIF values below 4.0 and tolerance levels above 0.2. These findings suggest that there is no evidence of multicollinearity among the predictor constructs, indicating that they are independent of each other.
Evaluating the structural model
We assessed the structural model using R2 values, standardized estimates, and model fit indices. To evaluate the model fit, we considered popular indices such as RMSEA, AGFI, GFI, CFI, and NFI. Table 5 shows that all model fit indices indicated an acceptable level of fit.
In terms of explanatory power, we analyzed the R2 values of the endogenous constructs. The results revealed that the modified UTAUT3 constructs explained 84.5% (0.845) of the variance in attitude towards EHR and 86.2% (0.862) of the variance in intention to use EHR. When compared to earlier UTAUT models, UTAUT3 explained 66.9% (0.669) of the variance in intention to use EHR, while UTAUT2 explained 62.9% (0.629). These findings suggest that the proposed model (Extended UTAUT3) has a stronger explanatory power than the earlier UTAUT3 and UTAUT2 models (See Supportive File 1).
Furthermore, the evaluation of the structural model revealed significant direct effects. Specifically, personal innovativeness (β = 0.468, p-value < 0.001), hedonic motivation (β = 0.135, p-value < 0.016), technology anxiety (β = -0.083, p-value < 0.027), and performance expectancy (β = 0.782, p-value < 0.001) had significant direct effects on attitude towards EHR. Similarly, personal innovativeness (β = 0.215, p-value < 0.018), performance expectancy (β = 0.245, p-value < 0.001), and attitude (β = 0.611, p-value < 0.001) had significant direct effects on the intention to use EHR (See Table 6).Table 5
Mediation analysis
We used mediation analysis to examine whether attitude plays a mediating role. Mediation occurs when the independent variable's impact on the dependent variable is partially or completely transmitted through the mediator. Complete mediation happens when the predictor's influence is entirely transmitted through the mediator, while partial mediation occurs when the predictor's influence is partially transmitted through the mediator.
Our findings reveal that attitude mediates the relationship between hedonic motivation (β = 0.512, p-value < 0.01), technology anxiety (β = -0.360, p-value < 0.05), and performance expectancy (β = 0.701, p-value < 0.01) with the intention to use EHR, as shown in Table 7.
Moderation analysis
The moderating effect of age
According to the results presented in Table 8, the moderation analysis indicated that age does not have a moderating effect on the relationship between the independent variables and behavioral intention.
The moderating effect of gender
The results from the moderation analysis, as presented in Table 9, indicate that gender moderates the association between social influence (χ2 = 14.630, p-value < 0.001) and personal innovativeness (χ2 = 5.011, p-value < 0.001) with behavioral intention. Specifically, being male (β = -0.784, p-value < 0.001) strengthens the association between social influence and behavioral intention compared to being female (β = -0.086, p-value > 0.05). Conversely, being female (β = 0.407, p-value < 0.001) strengthens the association between personal innovativeness and behavioral intention compared to being male (β = 0.199, p-value < 0.05).
The moderating effect of experience
According to the information presented in Table 10, no moderation effect was observed. The moderating variable did not have any effect on either strengthening or weakening the association between the independent and dependent variables.
Discussion
In this study, we proposed an extended UTAUT3 model to analyze the predictors of behavioral intention to use EHR among health professionals in public hospitals in southwest Ethiopia. The model exhibited strong explanatory power and explained 84.5% (R2 = 0.845) of the variance in behavioral intention to use EHR. Following Leguina et al., 2015 [86] classification of models as weak, moderate, and strong based on their explanatory power, we can confidently classify the proposed model as strong.
In our analysis, we compared the explanatory power of recent UTAUT models, utilizing the current data, with the extended UTAUT3 model. Our findings revealed that UTAUT3 explained 66.9% of the variance in intention to use EHR, while UTAUT2 explained 62.9%. These results indicate that the newly proposed model exhibits a higher level of explanatory power compared to the earlier models, suggesting its effectiveness in understanding behavioral intention.
Our study demonstrated a superior level of explanatory power compared to the original UTAUT model of Venkatesh et al., 2003 [32], the UTAUT2 model of Venkatesh et al., 2012 [34], and the UTAUT3 model of Farooq et al., 2017 [25]. These models originally reported explanatory powers of 69%, 74%, and 58.1% of the variance in intention to use, respectively. The strong explanatory capacity of our extended UTAUT3 model could be attributed to various factors. Firstly, the inclusion of individual factors in the model allows for a more comprehensive understanding of the specific determinants of behavioral intention. Additionally, the specific technology type being studied, the characteristics of the study participants, and the sample size may have contributed to the model's strong performance in explaining behavioral intention.
Based on our comprehensive literature review, we found that many scholars who utilized modified and extended UTAUT models across various disciplines reported lower levels of explanatory power compared to our study [13, 19,20,21,22,23, 27, 28, 30, 56, 58, 66, 68, 87, 88]. This suggests that the inclusion of new constructs in the modified UTAUT3 model may have contributed to achieving a higher level of explanatory power. Furthermore, upon examining the measurement model, we found that all of the constructs demonstrated commendable levels of validity and reliability. This indicates the robustness and reliability of the constructs used in our study.
The study's structural model analysis revealed a significant relationship between performance expectancy and the behavioral intention to use EHR. This finding is consistent with previous research conducted in various regions [19,20,21, 23, 24, 27, 42, 58]. Additionally, our mediation analysis indicated that performance expectancy indirectly influenced intention through the mediator variable of attitude, which is consistent with a previous finding [30].
These results implied that an individual's expectation of the desired outcome plays a crucial role in shaping their positive or negative feelings. These feelings, in turn, impact their motivation to engage in a specific task. The expectancy theory of motivation supports this finding, as it proposes that an individual's perception of the desirability of the consequences directly influences their motivation to choose a particular course of action [89].
The study found a clear and positive link between personal innovativeness and the intention to use EHR. This finding is consistent with previous research conducted in various regions [25, 28, 56, 57]. The possible reason behind this connection is that individuals who are open to trying out new digital health solutions are more likely to have a strong desire to use and benefit from these technologies. In simpler terms, being willing to embrace innovation in the field of digital health enhances people's motivation to adopt and utilize digital health tools.
The study findings revealed that individuals' attitude significantly influences their intention to use EHR, which is consistent with previous research conducted in various regions [19, 21, 68]. Building upon prior studies, this research identifies several pivotal factors, including personal innovativeness [61], hedonic motivation, technology anxiety [47], and performance expectancy [41, 42, 44], that play a crucial role in shaping individuals' attitudes towards EHR. These findings highlight the critical importance of comprehending and addressing these factors, as they directly impact individuals' attitudes. To effectively influence individuals' attitudes, healthcare organizations can promote personal innovativeness, emphasize the positive aspects of EHR, alleviate technology anxiety, and enhance performance expectations. By doing so, healthcare organizations can significantly enhance individuals' intention to adopt and utilize EHR in their healthcare practices.
The mediation analysis conducted in this study revealed that hedonic motivation and technology anxiety had a complete mediation effect. While the structural model analysis indicated that the direct effect of hedonic motivation on behavioral intention was not significant, the mediation analysis demonstrated that the effect of hedonic motivation on behavioral intention occurs through attitude, which is referred to as an indirect effect. This finding is reasonable as the level of pleasure or satisfaction influences individuals' positive or negative feelings and strengthens their inclination towards a particular behavior. It is worth noting that previous studies on behavioral aspects of digital health technology did not extensively explore mediation analysis, and thus we did not find significant mediation effects consistent with our findings. However, unlike our study, a few studies reported that attitude mediates the relationship between effort expectancy and behavioral intention [21, 41, 43].
The mediation analysis conducted in this study revealed that technology anxiety had a significant indirect negative effect on behavioral intention. This implies that individuals' fear or anxiety towards technology creates negative emotions, which in turn hinder their willingness to engage in the desired behavior. Interestingly, while the existing literature has not extensively explored the indirect effect of technology anxiety on intention through the mediator variable of attitude, a few studies highlighted its direct effect [46].
The moderation analysis showed that being male strengthened the association of social influence and behavioral intention than being female. This finding is consistent with previous research conducted in Canada [7]. The difference in the strength of this association might be attributed to variations in social factors and pressures experienced by males and females. Additionally, the likelihood of individuals imitating actions and behavior due to social influence may differ between the two genders. This finding is further supported by scholars who emphasized that responses to social influence learning strategies differ between males and females [90, 91].
Conversely, being female strengthened the association between personal innovativeness and behavioral intention than being male. This finding is supported by a study conducted in Taiwan [92]. The variation in the desire to explore and adopt emerging digital technologies between males and females may explain this difference.
Limitations and future research directions
The findings of this study should be applied cautiously by digital health implementers, considering the study's limitations. Future researchers are encouraged to address these limitations in their work. The first limitation of this study pertains to its generalizability. As our research was conducted among health professionals in public hospitals within resource-limited countries, the findings may not directly apply to technologically advanced nations. Thus, caution should be exercised when extrapolating the results to different contexts.
Another limitation is that this study focused on assessing behavioral intention during the pre-implementation phase, which may not fully represent actual acceptance and utilization after real implementation. Future research should aim to investigate acceptance and usage patterns during the post-implementation phase to gain a comprehensive understanding of the technology's impact. Given that the soundness of variables related to behavioral intention is influenced by the specific technology and discipline being studied, it is recommended that future researchers extend this model by incorporating different concepts and theories. Furthermore, it is important to verify the proposed model in diverse settings and disciplines to ensure its applicability across various contexts.
Despite these limitations, this study provides a baseline for the development of a novel model to examine behavioral intention toward digital health technologies. By addressing these limitations and building upon the proposed model, digital health implementers and researchers can further advance our understanding of behavioral intention and facilitate the successful implementation and adoption of digital health technologies.
Conclusion
Our study has provided valuable insights regarding the factors influencing behavioral intention in the adoption of EHR systems, with a specific focus on low-income countries. Notably, we introduced a new proposed model known as the extended UTAUT3 model, and its superior explanatory power was successfully demonstrated in comparison to previous models. Consequently, we have firmly established the extended UTAUT3 model as a robust framework for a comprehensive understanding of technology acceptance in healthcare, particularly about EHR systems.
Our findings revealed that personal innovativeness, performance expectancy, and attitude directly influenced the behavioral intention to use EHR systems. Interestingly, performance expectancy played a dual role, exerting both direct and indirect effects. Conversely, the impact of hedonic motivation and technology anxiety on behavioral intention operated solely through their indirect influence on attitude. This highlights the importance of personal innovativeness, hedonic motivation, technology anxiety, and performance expectancy in shaping individuals' attitudes towards EHR systems.
While social influence did not exhibit direct or indirect effects on behavioral intention, our moderation analysis unveiled significant gender differences, indicating the need for gender-specific interventions. Specifically, being male strengthened the association between social influence and behavioral intention more than being female. Consequently, social influence emerges as a crucial variable that should be targeted in interventions aimed at enhancing behavioral intention, particularly among males. Additionally, we found that the importance of personal innovativeness varied between males and females. Notably, being female amplified the association between personal innovativeness and behavioral intention, highlighting the necessity of addressing female individuals' personal innovativeness in interventions targeting behavioral intention.
Based on these findings, we recommend that, digital health implementers, policymakers, and concerned bodies consider the comprehensive range of direct, indirect, and moderating effects identified in our study. By addressing personal innovativeness, performance expectancy, attitude, hedonic motivation, technology anxiety, and the gender-specific impact of social influence, interventions can effectively enhance behavioral intention towards EHR systems.
This research makes a significant contribution to the existing literature by shedding light on the determinants of behavioral intention in the adoption of EHR systems, particularly in low-income countries. The insights gained can inform digital health implementers, policymakers, and concerned bodies in designing targeted interventions that promote the successful adoption and utilization of EHR systems in healthcare settings.
Availability of data and materials
The data used to support this study are not publicly available, as there are legal or ethical restrictions on sharing the data publically. However, the data can be made available upon a reasonable request directed to the corresponding author.
Abbreviations
- AGFI:
-
Adjusted goodness-of-fit-index
- AMOS:
-
Analysis of moment structures
- AVE:
-
Average variance extracted
- CET:
-
Cognitive Evaluation Theory
- CFI:
-
Comparative fit index
- CI:
-
Confidence interval
- CMB:
-
Common method bias
- CR:
-
Composite reliability
- Cα:
-
Cronbach's alpha
- DHIS2:
-
District health information system two
- eCHIS:
-
Electronic Community Health Information System
- EHR:
-
Electronic health record
- FMOH:
-
Federal ministry of health
- GFI:
-
Goodness-of-fit-index
- HAP:
-
Habit/automaticity perspective
- HIT:
-
Health information technology
- HTMT:
-
Heterotrait-monotrait ratio
- IAP:
-
Instant activation perspective
- ICT:
-
Information communication technology
- IT:
-
Information technology
- NFI:
-
Normed fit index
- RMSEA:
-
Root mean square error of approximation
- RMSR:
-
Root mean square residual
- SEM:
-
Structural equation modeling
- SPSS:
-
Statistical package for the social sciences
- TAM:
-
Technology Acceptance Model
- UTAUT:
-
Unified theory of acceptance and use of technology
- VIF:
-
Variance inflation factor
References
Walsham G. Health information systems in developing countries: some reflections on information for action. Inf Technol Dev. 2020;26(1):194–200.
Venot A, Burgun A, Quantin C. Medical Informatics, e-Health: Fundamentals and Applications. Cham: Springer International Publishing. 2014;12(3):191–220. https://doi.org/10.1007/978-2-8178-0478-1.
LaForge K, Gold R, Cottrell E, Bunce AE, Proser M, Hollombe C, et al. How 6 organizations developed tools and processes for social determinants of health screening in primary care: an overview. J Ambula Care Manag. 2018;41(1):2.
Riazi H, Jafarpour M, Bitaraf E. Towards national ehealth implementation–a comparative study on WHO/ITU national eHealth strategy toolkit in Iran. Studies in Health Technology and Informatics. IOS Press. 2014;205(1):246–50. https://doi.org/10.3233/978-1-61499-432-9-246.
Poon EG, Wright A, Simon SR, Jenter CA, Kaushal R, Volk LA, et al. Relationship between use of electronic health record features and health care quality: results of a statewide survey. Med Care. 2010;48(3):203–9. https://doi.org/10.1097/MLR.0b013e3181c16203.
Noblin A, Cortelyou-Ward K, Cantiello J, Breyer T, Oliveira L, Dangiolo M, et al. EHR implementation in a new clinic: a case study of clinician perceptions. J Med Syst. 2013;37:1–6.
Gagnon M-P, Talla PK, Simonyan D, Godin G, Labrecque M, Ouimet M, et al. Electronic health record acceptance by physicians: testing an integrated theoretical model. J Biomed Inform. 2014;48:17–27.
Kukafka R, Ancker JS, Chan C, Chelico J, Khan S, Mortoti S, et al. Redesigning electronic health record systems to support public health. J Biomed Inform. 2007;40(4):398–409.
Ngusie HS, Kassie SY, Chereka AA, Enyew EB. Healthcare providers’ readiness for electronic health record adoption: a cross-sectional study during pre-implementation phase. BMC Health Serv Res. 2022;22(1):1–12.
Organization WH. Electronic health record system implementation in healthcare system Geneva: WHO; 2020. https://www.who.int/gho/goe/electronic_health_records/en/.
Odekunle FF, Odekunle RO, Shankar S. Why sub-Saharan Africa lags in electronic health record adoption and possible strategies to increase its adoption in this region. Int J Health Sci. 2017;11(4):59.
Akanbi MO, Ocheke AN, Agaba PA, Daniyam CA, Agaba EI, Okeke EN, et al. Use of electronic health records in sub-Saharan Africa: progress and challenges. Journal of Medicine in the Tropics. 2012;14(1):1.
Taye G, Ayele W, Biruk E, Tassew B, Beshah T. The Ethiopian Health Information System: where are we? And where are we going? Ethiop J Health Dev. 2021;35(1):52–7.
Ethiopian Ministry of Health. Annual Performance Report 2012 (2019 2020). Scribd. 2020. [cited 2023 Aug 12]. Available from: https://www.scribd.com/document/518384802.
Lorenzi NM, Riley RT. Managing change: an overview. J Am Med Inform Assoc. 2000;7(2):116–24.
Kuo K-M, Liu C-F, Ma C-C. An investigation of the effect of nurses’ technology readiness on the acceptance of mobile electronic medical record systems. BMC Med Inform Decis Mak. 2013;13:1–14.
AL-ASWAD AM, Brownsell S, Palmer R, Nichol JP. A review paper of the current status of electronic health records adoption worldwide: the gap between developed and developing countries. J Health Inform Develop Count. 2013:7(2);206–17.
Shiells K, Holmerova I, Steffl M, Stepankova O. Electronic patient records as a tool to facilitate care provision in nursing homes: an integrative review. Inform Health Soc Care. 2019;44(3):262–77.
Ahmed MH, Bogale AD, Tilahun B, Kalayou MH, Klein J, Mengiste SA, et al. Intention to use electronic medical record and its predictors among health care providers at referral hospitals, north-West Ethiopia, 2019: using unified theory of acceptance and use technology 2 (UTAUT2) model. BMC Med Inform Decis Mak. 2020;20(1):1–11.
Bramo SS, Desta A, Syedda M. Acceptance of information communication technology-based health information services: Exploring the culture in primary-level health care of South Ethiopia, using Utaut Model. Ethnographic Study Digital Health. 2022;8:20552076221131144.
Shiferaw KB, Mehari EA. Modeling predictors of acceptance and use of electronic medical record system in a resource limited setting: Using modified UTAUT model. Informatics in Medicine Unlocked. 2019;17:100182.
Kim S, Lee K-H, Hwang H, Yoo S. Analysis of the factors influencing healthcare professionals’ adoption of mobile electronic medical record (EMR) using the unified theory of acceptance and use of technology (UTAUT) in a tertiary hospital. BMC Med Inform Decis Mak. 2015;16(1):1–12.
Dwivedi YK, Rana NP, Jeyaraj A, Clement M, Williams MD. Re-examining the unified theory of acceptance and use of technology (UTAUT): Towards a revised theoretical model. Inf Syst Front. 2019;21(3):719–34.
Tamilmani K, Rana NP, Dwivedi YK. Consumer acceptance and use of information technology: A meta-analytic evaluation of UTAUT2. Inf Syst Front. 2021;23:987–1005.
Farooq MS, Salam M, Jaafar N, Fayolle A, Ayupp K, Radovic-Markovic M, et al. Acceptance and use of lecture capture system (LCS) in executive business studies: Extending UTAUT2. Interactive Technology and Smart Education. 2017;14(4):329–48.
Tamilmani K, Rana NP, Wamba SF, Dwivedi R. The extended Unified Theory of Acceptance and Use of Technology (UTAUT2): a systematic literature review and theory evaluation. Int J Inf Manage. 2021;57:102269.
Cimperman M, Brenčič MM, Trkman P. Analyzing older users’ home telehealth services acceptance behavior—applying an Extended UTAUT model. Int J Med Informatics. 2016;90:22–31.
Gunasinghe A, Hamid JA, Khatibi A, Azam SF. The viability of UTAUT-3 in understanding the lecturer’s acceptance and use of virtual learning environments. Int J Technol Enhanced Learn. 2020;12(4):458–81.
Blut M, Chong A, Tsiga Z, Venkatesh V. Meta-Analysis of the Unified Theory of Acceptance and Use of Technology (UTAUT): Challenging its Validity and Charting a Research Agenda in the Red Ocean. J Assoc Inf Syst. 2021;6(1):124–32. https://ssrn.com/abstract=3834872.
Shiferaw KB, Mengiste SA, Gullslett MK, Zeleke AA, Tilahun B, Tebeje T, et al. Healthcare providers’ acceptance of telemedicine and preference of modalities during COVID-19 pandemics in a low-resource setting: an extended UTAUT model. PLoS ONE. 2021;16(4):e0250220.
Afthanorhan W. A comparison of partial least square structural equation modeling (PLS-SEM) and covariance based structural equation modeling (CB-SEM) for confirmatory factor analysis. Int J Eng Sci Innov Technol. 2013;2(5):198–205.
Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of information technology: Toward a unified view. MIS quarterly. 2003;27(3):425–78. https://doi.org/10.2307/30036540.
Williams MD, Rana NP, Dwivedi YK. The unified theory of acceptance and use of technology (UTAUT): a literature review. J Enterp Inf Manag. 2015;28(3):443–88.
Venkatesh V, Thong JY, Xu X. Consumer acceptance and use of information technology: extending the unified theory of acceptance and use of technology. MIS Q. 2012;36(1):157–78.
Childers TL, Carr CL, Peck J, Carson S. Hedonic and utilitarian motivations for online retail shopping behavior. J Retail. 2001;77(4):511–35.
Simon HA. Theories of Decision-Making in Economics and Behavioural Science. In: Surveys of Economic Theory. London: Palgrave Macmillan; 1966. p. 1–28. https://doi.org/10.1007/978-1-349-00210-8_1.
Kim SS, Malhotra NK, Narasimhan S. Research note—two competing perspectives on automatic use: a theoretical and empirical comparison. Inf Syst Res. 2005;16(4):418–32.
Ajzen I, Fishbein M. Attitudes and the attitude-behavior relation: Reasoned and automatic processes. Eur Rev Soc Psychol. 2000;11(1):1–33.
Agarwal R, Prasad J. A conceptual and operational definition of personal innovativeness in the domain of information technology. Inf Syst Res. 1998;9(2):204–15.
Lala G. The emergence and development of the technology acceptance model (TAM). Marketing from Information to Decision. 2014;7:149–60.
Alshare KA, Lane PL. Predicting student-perceived learning outcomes and satisfaction in ERP courses: An empirical investigation. Commun Assoc Inf Syst. 2011;28(1):34.
Koh CE, Prybutok VR, Ryan SD. A model for mandatory use of software technologies: an integrative approach by applying multiple levels of abstraction of informing science. Informing Science. 2010;13:177–203.
Rana NP, Dwivedi YK, Lal B, Williams MD, Clement M. Citizens’ adoption of an electronic government system: towards a unified view. Inf Syst Front. 2017;19(3):549–68.
Šumak B, Polancic G, Hericko M. An Empirical Study of Virtual Learning Environment Adoption Using UTAUT. 2010 Second International Conference on Mobile, Hybrid, and On-Line Learning. Saint Maarten, Netherlands Antilles: IEEE; 2010. p. 17-22. https://doi.org/10.1109/eLmL.2010.11.
Deci EL, Ryan RM. Cognitive Evaluation Theory. In: Intrinsic Motivation and Self-Determination in Human Behavior. Perspectives in Social Psychology. Boston, MA: Springer; 1985. p. 43–85. https://doi.org/10.1007/978-1-4899-2271-7_3.
Hoque R, Sorwar G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int J Med Informatics. 2017;101:75–84.
Celik V, Yesilyurt E. Attitudes to technology, perceived computer self-efficacy and computer anxiety as predictors of computer supported education. Comput Educ. 2013;60(1):148–58.
Guo X, Sun Y, Wang N, Peng Z, Yan Z. The dark side of elderly acceptance of preventive mobile health services in China. Electron Mark. 2013;23:49–61.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191.
Bawack RE, Kamdjoug JRK. Adequacy of UTAUT in clinician adoption of health information systems in developing countries: The case of Cameroon. Int J Med Informatics. 2018;109:15–22.
Chang A. UTAUT and UTAUT 2: A review and agenda for future research. The Winners. 2012;13(2):10–114.
San Martín H, Herrero Á. Influence of the user’s psychological factors on the online purchase intention in rural tourism: Integrating innovativeness to the UTAUT framework. Tour Manage. 2012;33(2):341–50.
Nordén L-Å, Mannila L, Pears A. Development of a self-efficacy scale for digital competences in schools. IEEE Frontiers in Education Conference (FIE). Indianapolis, IN, USA; IEEE; 2017. p. 1–7. https://doi.org/10.1109/FIE.2017.8190673.
Becker D. Acceptance of mobile mental health treatment applications. Procedia Comp Sci. 2016;98:220–7.
Zha H, Liu K, Tang T, Yin Y-H, Dou B, Jiang L, et al. Acceptance of clinical decision support system to prevent venous thromboembolism among nurses: an extension of the UTAUT model. BMC Med Inform Decis Mak. 2022;22(1):221.
Kijsanayotin B, Pannarunothai S, Speedie SM. Factors influencing health information technology adoption in Thailand’s community health centers: applying the UTAUT model. Int J Med Informatics. 2009;78(6):404–16.
Woldeyohannes HO, Ngwenyama OK, editors. Factors influencing acceptance and continued use of mHealth apps. HCI in Business, Government and Organizations Interacting with Information Systems: 4th International Conference, HCIBGO 2017, Held as Part of HCI International 2017, Vancouver, BC, Canada, July 9–14, 2017, Proceedings, Part I 4; 2017: Springer.
Wang H, Tao D, Yu N, Qu X. Understanding consumer acceptance of healthcare wearable devices: an integrated model of UTAUT and TTF. Int J Med Informatics. 2020;139:104156.
Luyten J, Marneffe W. Examining the acceptance of an integrated Electronic Health Records system: Insights from a repeated cross-sectional design. Int J Med Informatics. 2021;150:104450.
Schillewaert N, Ahearne MJ, Frambach RT, Moenaert RK. The adoption of information technology in the sales force. Ind Mark Manage. 2005;34(4):323–36.
Ayub AFM, Zaini SH, Luan WS, Jaafar WMW. The influence of mobile self-efficacy, personal innovativeness and readiness towards students’ attitudes towards the use of mobile apps in learning and teaching. Int J Academ Res Business Soc Sci. 2017;7(14):364–74.
Venkatesh V, Davis FD. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manage Sci. 2000;46(2):186–204.
Tamilmani K, Rana NP, Prakasam N, Dwivedi YK. The battle of Brain vs. heart: a literature review and meta-analysis of “hedonic motivation” use in UTAUT2. Int J Inform Manag. 2019;46:222–35.
Novela S, Sihombing YO, Novita, Caroline E, Octavia R. The Effects of Hedonic and Utilitarian Motivation toward Online Purchase Intention with Attitude as Intervening Variable. Int Conf Inf Manag Technol (ICIMTech). Bandung, Indonesia: IEEE; 2020. p. 75–80. https://doi.org/10.1109/ICIMTech50083.2020.9211197.
Verplanken B, Aarts H. Habit, attitude, and planned behaviour: is habit an empty construct or an interesting case of goal-directed automaticity? Eur Rev Soc Psychol. 1999;10(1):101–34.
Walle AD, Jemere AT, Tilahun B, Endehabtu BF, Wubante SM, Melaku MS, et al. Intention to use wearable health devices and its predictors among diabetes mellitus patients in Amhara region referral hospitals, Ethiopia: using modified UTAUT-2 model. Informatics in Medicine Unlocked. 2023;36:101157.
Conner M, Wilding S, Norman P. Testing predictors of attitude strength as determinants of attitude stability and attitude–behaviour relationships: A multi-behaviour study. Eur J Soc Psychol. 2022;52(4):656–68. https://doi.org/10.1002/ejsp.2844.
Huang WM, Chen T, Hsieh CW. An empirical study on the physicians' behavioral intention with electronic medical record systems in Taiwan [Internet]. PACIS 2014 Proceedings. 2014; p. 160. [cited 2023 June 6]. Available from: http://aisel.aisnet.org/pacis2014/160.
Nikolopoulou K, Gialamas V, Lavidas K. Habit, hedonic motivation, performance expectancy and technological pedagogical knowledge affect teachers’ intention to use mobile internet. Computers and Education Open. 2021;2:100041.
Barbeite FG, Weiss EM. Computer self-efficacy and anxiety scales for an Internet sample: testing measurement equivalence of existing measures and development of new scales. Comput Hum Behav. 2004;20(1):1–15.
Moghavvemi S. Impact of perceived self-efficacy and capability to use IT innovation on individual use behaviour. Available at SSRN 2561739. 2015.
Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. 1981;18(1):39–50.
Barclay D, Higgins C, Thompson R. The Partial Least Squares (PLS) Approach to Causal Modelling: Personal Computer Adoption and Use as an Illustration. Technol Stud. 1995;2(2):285–309.
Hair JF Jr, Black WC, Babin BJ, Anderson RE. Multivariate data analysis. Upper Saddle River (NJ): Prentice Hall; 2009. 832-841.
Falk RF, Miller NB. A primer for soft modeling. University of Akron Press; 1992. [cited 2023 Aug 25]. Available from: https://psycnet.apa.org/record/1992-98610-000.
Sarstedt M, Hair JF, Pick M, Liengaard BD, Radomir L, Ringle CM. Progress in partial least squares structural equation modeling use in marketing research in the last decade. Psychol Mark. 2022;39(5):1035–64.
Hill CR, Hughes JN. An examination of the convergent and discriminant validity of the Strengths and Difficulties Questionnaire. Sch Psychol Q. 2007;22(3):380.
Henseler J, Ringle CM, Sarstedt M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J Acad Mark Sci. 2015;43:115–35.
Dijkstra TK, Henseler J. Consistent and asymptotically normal PLS estimators for linear structural equations. Comput Stat Data Anal. 2015;81:10–23.
Kock N. Harman’s single factor test in PLS-SEM: Checking for common method bias. Data Analysis Perspectives Journal. 2020;2(2):1–6.
Gatignon H, Gatignon H. Confirmatory Factor Analysis. In: Statistical Analysis of Management Data. Boston, MA: Springer; 2014. p. 77–154. https://doi.org/10.1007/978-1-4614-8594-0_4.
Baumgartner H, Homburg C. Applications of structural equation modeling in marketing and consumer research: A review. Int J Res Mark. 1996;13(2):139–61.
Hu Lt, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural equation modeling: a multidisciplinary journal. 1999;6(1):1–55.
Brown TA. Confirmatory factor analysis for applied research. New York, NY: Guilford Publications; 2015. p. 1–17.
Hoyle RH. Structural equation modeling: Concepts, issues, and applications. Thousand Oaks, CA: Sage; 1995. p. 36–42.
Leguina A. A primer on partial least squares structural equation modeling (PLS-SEM). Abingdon, UK: Taylor & Francis; 2015. p. 7–18.
Mukred M, Yusof ZM, Alotaibi FM, Asma’Mokhtar U, Fauzi F. The key factors in adopting an electronic records management system (ERMS) in the educational sector: a UTAUT-based framework. IEEE Access. 2019;7:35963–80.
Hew JJ, Lee VH, Ooi KB, Wei J. What catalyses mobile apps usage intention: an empirical analysis. Ind Manag Data Syst. 2015;115(7):1269–91. https://doi.org/10.1108/IMDS-01-2015-0028.
Oliver RL. Expectancy theory predictions of salesmen’s performance. J Mark Res. 1974;11(3):243–53.
Oyibo K, Orji R, Vassileva J, editors. The influence of culture in the effect of age and gender on social influence in persuasive technology. Adjunct publication of the 25th conference on user modeling, adaptation and personalization; 2017.
Rendell L, Fogarty L, Hoppitt WJ, Morgan TJ, Webster MM, Laland KN. Cognitive culture: theoretical and empirical insights into social learning strategies. Trends Cogn Sci. 2011;15(2):68–76.
Chiu YB, Lin CP, Tang LL. Gender differs: assessing a model of online purchase intentions in e-tail service. Int J Serv Ind Manag. 2005;16(5):416–35.
Acknowledgements
The authors would like to express their gratitude to the healthcare professionals, trainers, data collectors, and supervisors who actively participated in this study.
Funding
The author(s) received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
HSN, SYK, ADW, and SAM made substantial contributions to the conception, design, data collection, supervision, investigation, data analysis, interpretation, and manuscript writing. ABZ, EBE, MDK, and BTS contributed to the development of the proposal, validation, manuscript revision, figure preparation, data analysis, visualization, and interpretation. All authors (HSN, SYK, ABZ, ADW, SAM, EBE, MDK, and BTS) critically reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We obtained ethical clearance for this study from the ethical review board of Mettu University College of Health Science, under reference number RPG/90/13. We obtained verbal informed consent from all participants involved in the study. Due to practical reasons and the large number of participants, it was not feasible to obtain written consent from each individual. This approach was approved by the institutional review boards overseeing the study. To ensure documentation of consent, we assigned a unique identifier to each participant during data collection and recorded it alongside the questionnaire. The data collection process was anonymous and followed the guidelines outlined in the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing of interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ngusie, H.S., Kassie, S.Y., Zemariam, A.B. et al. Understanding the predictors of health professionals' intention to use electronic health record system: extend and apply UTAUT3 model. BMC Health Serv Res 24, 889 (2024). https://doi.org/10.1186/s12913-024-11378-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-024-11378-1