
Abstract
Background
The COVID-19 pandemic wreaked havoc on long-term care facilities (LTCFs). Some LTCFs performed better than others at slowing COVID-19 transmission. Emerging literature has mostly described infection prevention and control strategies implemented by LTCFs during the pandemic. However, there is a need for a comprehensive review of factors that influenced the performance of LTCFs in containing COVID-19 spread to inform public health policy.
Objective
To build on the existing literature, we conducted a scoping review of factors that influenced LTCF performance during the COVID-19 pandemic using a multidimensional conceptual framework of performance.
Methods
We followed the Joanna Briggs Institute’s methodology for scoping reviews. We queried CINAHL, MEDLINE (Ovid), CAIRN, Science Direct, Scopus, and Web of Science for peer-reviewed literature in English or French published between January 1st, 2020 and December 31st, 2021. Retrieved records were screened for context (COVID-19 pandemic), population (LTCFs), interest (internal and external factors that influenced LTCF performance), and outcomes (dimensions of performance: equity, accessibility, reactivity, safety, continuity, efficacy, viability, efficiency). Descriptive characteristics of included articles were summarized. Dimensions of performance as well as internal (e.g., facility characteristics) and external (e.g., visitors) factors identified to have influenced LTCF performance were presented.
Results
We retained 140 articles of which 68% were classified as research articles, 47% originated in North America, and most covered a period between March and July 2020. The most frequent dimensions of performance were “efficacy” (75.7%) and “safety” (75.7%). The most common internal factors were “organizational context” (72.9%) and “human resources” (62.1%), and the most common external factors were “visitors” (27.1%) and “public health guidelines” (25.7%).
Conclusions
Our review contributes to a global interest in understanding the impact of the COVID-19 pandemic on vulnerable populations residing and working in LTCFs. Though a myriad of factors were reported, a lack of randomized controlled trials makes it impossible to establish causality between the identified factors and LTCF performance. The use of a multidimensional framework can be recommended to evaluate healthcare system performance not merely in terms of efficacy and safety, but alongside other critical dimensions such as efficiency and equity.
Trial registration
Research Registry ID: researchregistry7026
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
On March 11th 2020 the World Health Organization declared COVID-19 a pandemic in response to the alarming propagation of the highly transmissible and virulent virus [1, 2]. Residents of long-term care facilities (LTCFs) around the world bore the brunt of the pandemic, experiencing high morbidity and mortality [3]. As of July 2020, LTCF residents represented 47% of COVID-19-related deaths across 12 countries within the Organization for Economic Co-operation and Development (OECD), while in Canada this number approached 80% [4]. In the Canadian province of Québec, between March and July of 2020, more than 90% of all deaths due to COVID-19 occurred among adults over the age of 70, of whom 64% resided in LTCFs [5]. As of February 2021, an average of 41% of COVID-19-related deaths across 25 OECD countries occurred among LTCF residents, with the highest percentage of 75% recorded in Australia, compared to 39% in the United States of America (USA) and 59% in Canada [6]. As of July 2022, 43% of Canada’s overall deaths due to COVID-19 were among LTCF residents and staff [7].
Amidst the crisis, some LTCFs performed better than others, slowing COVID-19 transmission more effectively and, as a consequence, experiencing fewer cases and lower mortality [8]. It is critical to understand the reasons behind this differential LTCF performance to inform the prevention of and response to outbreaks in the future. Literature describing COVID-19 in LTCFs has primarily focused on reporting disease outcomes [3], identifying effective infection prevention and control (IPC) strategies [8, 9], and formulating IPC guidance [10]. A growing number of publications have described factors that influenced the effectiveness or failure of implemented IPC strategies to prevent or mitigate COVID-19 outbreaks. Factors associated with more successful control of COVID-19 spread in LTCFs include: strong partnerships between LTCFs, laboratory services, hospitals, and public health officials; greater funding with more care hours per resident; proactive leadership that enforced IPC measures; access to a multidisciplinary IPC team; monitoring of human and material resources; universal testing of residents and staff; and visitor restrictions [11,12,13,14,15,16,17,18,19,20,21,22,23,24]. Less effective responses have been linked to: inadequate national long-term care policies; a lack of integration between LTCFs, hospitals, and the public health sector; chronic underfunding; shortages of material resources and IPC trained staff; and the failure to detect and manage asymptomatic COVID-19 cases [19, 24,25,26,27,28,29,30,31,32,33]. In addition, the magnitude of COVID-19 outbreaks in LTCFs has been positively correlated with larger sized facilities, urban location, lower quality ratings, higher occupancy rooms, a greater proportion of racial/ethnic minority residents, and fewer care hours per resident [34,35,36,37,38,39,40,41,42].
Given the breadth and heterogeneity of the existing literature, there is a need for a comprehensive review of factors that influenced LTCF performance during the COVID-19 pandemic. Several reviews have been conducted to elucidate these factors. Gmehlin and Munoz-Price [43] offered an overview of the epidemiology, clinical manifestations, and interventions implemented to combat COVID-19 by LTCFs, underscoring the effectiveness of testing and subsequent cohorting of both residents and staff. Similarly, Dykgraaf et al.’s [8] rapid narrative review of strategies that helped limit COVID-19 spread in LTCFs stressed the importance of serial universal screening of residents and staff. A narrative review by Calcaterra et al. [44] synthesized IPC measures used by LTCFs to manage COVID-19 in several Asian countries, noting similarity of measures used elsewhere in the world, such as visitor restrictions. The authors speculated that the effective response demonstrated by LTCFs in these Asian countries may have been due to better integration into the healthcare system and greater preparedness informed by previous experience. In their scoping review, Palacios-Ceña et al. [45] synthesized the qualitative evidence relating to the experiences of LTCF staff, residents, and residents’ families during the COVID-19 pandemic. Themes that emerged from the data underscored LTCFs’ challenges with managing material and human resources, the emotional toll exerted by the pandemic on residents and staff, as well as the innovative solutions and adaptive strategies implemented by LTCF staff in response to the hardship. Furthermore, Frazer et al.’s [46] rapid systematic review linked the likelihood of experiencing a COVID-19 outbreak in a LTCF to a facility’s bigger size, for-profit status, higher crowding index, greater number of employees, and staff working at multiple facilities. In Konetzka et al.’s [47] systematic review of facility characteristics associated with COVID-19-related outcomes, a larger facility size and higher disease prevalence in the community emerged as the strongest predictors of COVID-19 cases and deaths. A more comprehensive review of factors that drove COVID-19 transmission in LTCFs was performed by Giri et al. [48]. Here, identified factors included: asymptomatic COVID-19 transmission, factors linked to the facilities (e.g., for-profit status), residents (e.g., malnutrition), or staff (e.g., high staff turnover), as well as external factors (e.g., underfunding).
The aforementioned studies offered insight into a range of factors that influenced the performance of LTCFs during the COVID-19 pandemic. However, no studies have applied a multidimensional approach to assessing LTCF performance during this challenging period. Accordingly, to examine LTCF performance during the first 2 years of the COVID-19 pandemic and more broadly, we performed a scoping review using a multidimensional conceptual framework of performance within healthcare systems. For the purposes of this scoping review, the performance of a healthcare system was defined as the system’s ability to achieve its objectives in relation to the population’s health as a function of the following dimensions of performance: equity, accessibility, reactivity, safety, continuity, efficacy, viability, and efficiency [49]. This framework helped to determine factors that could be viewed as either facilitators or barriers to the management of COVID-19 within LTCFs.
Methods
Conceptual framework
Despite being commonly expressed in terms of case numbers and death rates [50, 51], the performance of a healthcare system in the context of the COVID-19 pandemic can be conceptualized in multiple ways. For example, the OECD defines a healthcare system’s performance as the attainment of goals at the lowest possible cost [52], whereas the framework used by the Canadian Institute for Health Information evaluates healthcare system performance by answering the questions “How healthy are Canadians?” and “How healthy is the health system?” [53]. In Québec, the Ministère de la Santé et des Services Sociaux (MSSS) adopted a conceptual framework entitled the Cadre de référence ministériel d’évaluation de la performance du système public de santé et de services sociaux à des fins de gestion, where a healthcare system’s performance is conceptualized as the system’s ability to reach its objectives in relation to the population’s health, taking into consideration the optimization of resources and the quality and accessibility of services [54].
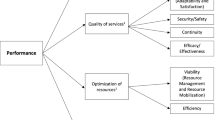
We chose the MSSS framework as the foundation of our scoping review’s conceptual framework because of its multifaceted approach to assessing healthcare system performance. Thus, the conceptual framework that guided our review encompassed eight dimensions of performance that fell under three fundamental elements of performance: 1) equity and accessibility within the accessibility of services; 2) reactivity, safety, continuity, and efficacy within the quality of services; and 3) viability and efficiency within the optimization of resources (see Fig. 1).

The conceptual framework of healthcare system performance adapted from the Cadre de référence ministériel d’évaluation de la performance du système public de santé et de services sociaux à des fins de gestion developed by the Québec’s Ministère de la Santé et des Services Sociaux (19)
The definitions of the dimensions of performance included in the original MSSS framework are presented in Table 1. To optimize database queries, we slightly modified the original MSSS framework’s dimensions in our search strategies. Specifically, we substituted the dimension of reactivity with the terms adaptability and satisfaction, whose definitions within the databases better aligned with the original MSSS definition of reactivity. By the same token, the terms resource management and resource mobilization were used in our searches in lieu of the dimension of viability. In addition, the CINAHL database terms effectiveness and security were identified as synonyms of the original MSSS dimensions of efficacy and safety, respectively, and thus were added to the search strategies to ensure all relevant literature was captured. Throughout the rest of the manuscript, only the original MSSS definitions are used (Table 1).
In addition to the dimensions of performance, the conceptual framework incorporated factors that could influence LTCF performance, as informed by the previous literature [48, 55]. Factors were categorized into eight internal and four external factors, as presented in Table 1.
Methodological framework
We followed the methodology for scoping reviews developed by the Joanna Briggs Institute, which expands on the work done by Arksey and O’Malley as well as Levac et al. [56, 57]. Accordingly, we followed these nine steps: 1) formulating and aligning the review’s objective(s) and question(s); 2) developing eligibility criteria in keeping with the established objective(s) and question(s); 3) describing the approach to database queries, article selection, data extraction, and presentation of findings; 4) searching for the evidence; 5) selecting the evidence; 6) extracting the evidence; 7) analyzing the evidence; 8) presenting the evidence; and 9) summarizing the evidence with respect to the review’s objective(s) and question(s), drawing conclusions, and noting potential implications.
To ensure our review included all necessary elements, we completed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Checklist (see Supplementary File 1) [58]. We also consulted the updated guideline for reporting scoping reviews that was outlined in the PRISMA 2020 Statement [59, 60].
Eligibility criteria
Table 1 presents the eligibility criteria using the Population, Interest, Comparison, Outcome, and Time (PICOT) model.
Data sources and search strategy
The protocol for this review was registered with the Research Registry [researchregistry7026] and published [61]. We queried the databases CINAHL, MEDLINE (Ovid), CAIRN, Science Direct, Scopus, and Web of Science for records that met the eligibility criteria, including the context (COVID-19 pandemic), population (LTCFs), interest (factors that influenced LTCF performance), and outcomes (dimensions of performance: equity, accessibility, reactivity, safety, continuity, efficacy, viability, efficiency). We restricted our searches to peer-reviewed literature written in English or French and published during the first 2 years of the COVID-19 pandemic, between January 1st 2020 and December 31st 2021. We excluded records that focused on infections other than COVID-19 and healthcare settings other than LTCFs. We also excluded records that focused on pharmaceutical treatments or COVID-19 vaccination rates.
Two co-authors (JL, EB) performed database searches independently using strategies developed by our team (see Supplementary Files 2–7). All searches were performed using descriptors with the Boolean operators “AND” and “OR”. Retrieved records were imported to the EndNote software, and duplicates were removed.
Article selection
From Endnote, retrieved records were exported to the Rayyan web platform [62], duplicates were removed, and records were screened in accordance with an algorithm developed by our research team [63]. Two co-authors (JL, EB) pilot tested the algorithm for reliability by independently screening the titles and abstracts of the first 10% of articles and then comparing results. The screening algorithm was then elaborated upon, for example, by adding the definitions of the dimensions of performance.
Once the algorithm had been tested and refined, the first complete screening round took place, where the titles and abstracts of all records were screened by two co-authors (JL, EB) as well as divided between the other co-authors, such that each record was screened by three co-authors. All three co-authors had to deem a record eligible for it to pass to the second screening round, where each record was read in its entirety by one co-author who decided whether to include or exclude it (see Fig. 2). The decision of whether to retain a record was based on three questions, answered in order: 1) Does the record focus on management activities during the COVID-19 pandemic?; 2) Does the population include residents and/or staff of a single or multiple LTCF(s) during the pandemic?, and 3) Does the record discuss at least one factor (e.g., resident characteristics, financial resources, etc.) that influenced LTCF performance during the pandemic? At this stage, it was not required to identify all factors discussed in each record; once any one factor was identified in a record, the record was retained for data extraction.

Screening algorithm. Adapted from previous work by Tchouaket et al. [63]. Legend: Q1 MANAGEMENT OF COVID-19: Is the primary focus of the record on management activities (e.g., organisation, planning, IPC) within a healthcare facility during the COVID-19 pandemic? Q2 POPULATION: Does the record specify its population as LTCFs housing elderly residents or hospice/palliative care services occurring within the context of a single or multiple LTCF(s)? (Synonyms: nursing homes, assisted-living facilities, homes for the aged, aged care homes, retirement homes, long term care). Q3 INTERESTS: Does the record discuss at least one factor related to the management of COVID-19 and outcomes of the pandemic within a single or multiple LTCF(s)? Internal factors: 1) resident characteristics; 2) facility characteristics; 3) staff characteristics; 4) human resources; 5) material resources; 6) technological resources; 7) financial resources; and 8) organizational context. External factors: 1) admissions; 2) visitors; 3) virus circulation in the community; and 4) public health policies/guidelines. Note: All keywords were translated into French for the CAIRN database
Data extraction
Relevant data from retained articles were extracted in three stages. First, descriptive characteristics were extracted using a data charting form developed by two co-authors (JL, EB) and reviewed by the entire research team. These same two co-authors (JL, EB) pilot tested the form, after which data extraction by five co-authors (KK, FEM, SR, JL, EB) occurred using Google Forms. The following data were extracted from each article: citation, year of publication, country of origin, study objectives, design, setting, participants, and framework (if one was used).
Following the first stage, dimensions of performance were extracted using a coding frame, where each dimension was defined as per the adopted conceptual framework. To ensure reliability, two co-authors (KK, SR) were first assigned an identical set of 20% (28/140) of included articles. The co-authors read the articles independently to extract identified dimensions of performance along with verbatim or paraphrased examples (1–3 sentences). For each record, dimensions were coded as “1”, if extracted, or “0”, if not extracted. Inter-coder reliability was calculated by summing the number of dimensions upon which both co-authors had agreed (e.g., viability coded as “1” or “0” for both coders), dividing it by eight (total number of dimensions), and multiplying the result by 100% [64, 65]. Mean inter-coder reliability across the 28 records was 81.3%. The two co-authors (KK, SR) met to share feedback about the coding process, and, in the case of conflicts, a third co-author (ENT) arbitrated. The coding frame was then fine-tuned by specifying what did and did not qualify as supporting evidence for each dimension (see Supplementary File 8). Lastly, the remaining records were randomly allocated to the same co-authors (KK, SR), who completed the extraction of dimensions.
All relevant factors reported to have influenced LTCF performance were extracted from each retained article. To ensure reliability, two co-authors (KK, SR) were first assigned an identical set of 10% (14/140) of records. The co-authors read the articles independently to extract identified factors into an Excel spreadsheet along with verbatim or paraphrased examples (1–3 sentences). In the case of identifying a factor that was not specified in the screening algorithm, the factor was extracted under the category “Other”. The co-authors then met to discuss the coding process and resolve any conflicts. Following this discussion, the remaining articles were randomly allocated to the same co-authors (KK, SR), who completed the extraction of factors.
Data synthesis and presentation
Three co-authors (KK, SR, ENT) analyzed extracted data. Countries of origin were collapsed into geographic regions. Descriptive characteristics were summarized, and the data collection period was extracted to situate the evidence within the temporal progression of the COVID-19 pandemic. Dimensions were extracted and their frequencies displayed in tabular form as were the factors identified to have influenced at least one dimension of LTCF performance. The completed data charting form is provided in Supplementary File 9.
Research team
The principal investigator (ENT) was supported by a registered nurse (JL), who is an expert in the assessment of factors that contribute to outbreaks, IPC, and performance evaluation in nursing. The research team also included two professors (DS, IB) with extensive experience with scoping review methodology in the field of nursing sciences, as well as research professionals (KK, SR, EB, FEM, SS) and a doctoral student in nursing (MJ), who are all proficient in database searches, article selection, and manuscript preparation.
Results
Article selection
Results of the selection process are summarized in a PRISMA flow chart (see Fig. 3). After removing duplicates and screening titles and/or abstracts, 448 of the 9,895 retrieved records underwent full-text assessment. After eliminating 15 records for which full text was not accessible, 433 records were read in their entirety, of which 139 were retained. Reasons for exclusion included: addressing a wrong subject (n = 159), having a wrong interest (n = 108), focusing on a wrong population (n = 16), being in a language other than English or French (n = 9), and being a duplicate (n = 2). In addition, one record was added using a snowballing approach for the total of 140 articles.

PRISMA flow chart, outlining the identification and selection stages of this review. Adapted from The PRISMA 2020 statement: An updated guideline for reporting systematic reviews [59]. The term “report” signifies “a document (paper or electronic) supplying information about a particular study”, such as a journal article or government report, while the term “record” signifies “The title or abstract (or both) of a report indexed in a databased or website” [59]
Characteristics of retained articles
Table 2 summarizes descriptive characteristics of the 140 retained articles, including publication type, study design, setting, participants, data collection/analysis period, month/year of publication, country and region of origin, and framework (if one was used).
Countries and regions of origin
North America was the most represented region with 66 out of 140 (66/140, 47.1%) articles, of which 53 (80.3%) originated in the USA [11,12,13,14,15, 18, 19, 25, 29, 30, 34,35,36,37,38,39,40,41, 47, 50, 70, 73, 74, 76, 81, 89, 90, 92, 100,101,102,103,104, 108, 110, 111, 114, 117, 121,122,123, 126, 127, 129, 131, 137, 138, 141, 147, 148, 150, 159, 162], 12 (18.2%) came from Canada [16, 22, 24, 27, 107, 109, 113, 118, 124, 132, 139, 164], and one (1.5%) article covered both the USA and Canada [125]. North America was followed by Europe with 34 out of 140 (24.3%) articles, of which nine (26.5%) originated in France [21, 23, 28, 75, 78, 80, 87, 96, 136], six (17.6%) in England [72, 88, 119, 120, 143, 151], five (14.7%) in Italy [26, 67, 69, 77, 82], three (8.8%) in Germany [17, 94, 105], two (5.9%) in Spain [97, 140], and three (8.8%) covered several European countries [79, 95, 128], while the rest represented one country each, including Austria [33], Belgium [31], Cyprus [158], Norway [116], the Netherlands [91], and Turkey [71]. Nineteen of the 140 articles (13.6%) came from Asia, of which six (31.6%) originated in China [112, 115, 145, 160, 161, 163], five (26.3%) in Japan [66, 98, 133,134,135], two (10.5%) in Hong Kong [85, 144], two (10.5%) in Singapore [154, 155], two (10.5%) in South Korea [20, 149], and two (10.5%) in Taiwan [84, 146]. Australia was represented by six (4.3%) articles [99, 106, 152, 156, 157, 165], South America by two (1.4%) articles both coming from Brazil [93, 130], and the Middle East by one (0.7%) article originating in Saudi Arabia [68]. In addition, one (0.7%) article covered both Europe and Australia [83], and 11 (7.9%) articles—including seven reviews—adopted a global perspective [8, 32, 42, 43, 45, 46, 48, 55, 86, 142, 153].
Publication types
Of the 140 retained articles, 95 (67.9%) were classified as research articles and included, for example original articles, reviews, and brief reports [8, 11,12,13,14,15,16,17,18,19,20,21,22,23, 28, 33,34,35,36,37,38,39,40,41, 43, 45,46,47,48, 50, 55, 66,67,68,69,70,71,72, 74,75,76,77, 80, 82, 87, 89, 91,92,93, 96, 97, 100,101,102,103, 105,106,107,108,109,110,111,112,113,114, 116,117,118,119,120, 122,123,124, 126,127,128,129, 132, 135,136,137, 139, 142, 143, 145, 147,148,149, 151, 152, 158, 161,162,163,164]. In addition to research articles, our sample included 18 (12.9%) discussion papers [29,30,31,32, 78, 81, 85, 94, 125, 130, 131, 138, 140, 150, 153, 159, 160, 165]; 11 (7.9%) policy analysis papers [24, 26, 27, 83, 86, 88, 90, 95, 98, 115, 134]; seven (5.0%) letters to the editor [73, 84, 133, 144, 146, 154, 155]; three (2.1%) medical news articles [25, 104, 141]; two (1.4%) professional journal articles [99, 157]; one (0.7%) communication [156]; one (0.7%) guideline [79]; one (0.7%) conference proceedings paper [42]; and one (0.7%) morbidity and mortality weekly report [121].
Designs of research articles
The 95 research articles included 39 (41.1%) studies that analyzed secondary quantitative data [13, 18, 20, 34,35,36,37,38,39, 41, 50, 66, 69, 71, 72, 76, 77, 80, 89, 92, 100,101,102,103, 105,106,107,108, 110, 111, 118, 122, 123, 129, 132, 137, 139, 148, 162], 38 (40.0%) studies that used primary quantitative data [11, 12, 14, 15, 17, 19, 21,22,23, 28, 33, 40, 67, 68, 70, 74, 75, 87, 91, 93, 96, 97, 109, 112,113,114, 117, 119, 126, 127, 135, 136, 143, 145, 147, 149, 158, 161], eight (8.4%) qualitative studies [16, 112, 120, 124, 151, 152, 163, 164], one (1.1%) study that used both primary and secondary quantitative data [82], as well as nine (9.5%) reviews, including three rapid reviews [8, 55, 142], two scoping reviews [45, 48], one systematic review [47], one rapid systematic review [46], one literature review [43], and one narrative review [128].
The 39 studies that analyzed secondary quantitative data encompassed 24 (61.5%) cross-sectional studies [34,35,36,37,38,39, 50, 69, 71, 72, 92, 100,101,102, 105, 106, 108, 110, 111, 122, 123, 137, 139, 148], seven (17.9%) retrospective cohort studies [80, 89, 103, 107, 118, 132, 162], three (7.7%) case-control studies [41, 76, 129], three (7.7%) descriptive epidemiological studies [13, 20, 66], one (2.6%) repeated cross-sectional study [77], and one (2.6%) prospective cohort study [18].
The 38 studies that collected primary quantitative data included 10 (26.3%) cross-sectional studies [11, 15, 23, 87, 91, 112, 119, 136, 143, 145], eight (21.1%) prospective cohort studies [14, 19, 28, 40, 67, 68, 117, 147], four (10.5%) implementation research studies [70, 74, 97, 127], two (5.3%) implementation research/cross-sectional studies [21, 109], two (5.3%) descriptive epidemiological studies [114, 149], two (5.3%) mixed-methods studies [93, 161], two (5.3%) retrospective cohort studies [17, 75], one (2.6%) cross-sectional study based on computational modeling [126], one (2.6%) mixed-methods pre-post evaluation study [113], one (2.6%) quasi-experimental before-and-after study [22], one (2.6%) repeated cross-sectional study [12], one (2.6%) retrospective cohort/cross-sectional study [33], one (2.6%) retrospective pre-post study [96], one (2.6%) complex intervention with a prospective cohort/pre-post study [158], and one (2.6%) interventional pre-post study [135].
Settings and participants of research articles
Of the 38 studies that used primary quantitative data, 27 (71.1%) were based on evidence from multiple LTCFs with the number of facilities ranging from 2 to 5,126 [11, 15, 19, 22, 23, 33, 40, 70, 74, 75, 87, 93, 96, 97, 109, 112,113,114, 117, 119, 127, 136, 143, 145, 149, 158, 161], whereas 11 (28.9%) focused on a single facility [12, 14, 17, 21, 28, 67, 68, 91, 126, 135, 147]. Of the 39 studies that were based on secondary quantitative data, 32 (82.1%) pooled evidence from multiple LTCFs with the number of facilities ranging from 3 to 15,390 [18, 20, 34,35,36,37,38,39, 41, 50, 69, 72, 76, 77, 89, 92, 100,101,102,103, 105, 106, 110, 111, 118, 122, 123, 129, 137, 139, 108, 148], whereas seven (7.7%) centered on a single facility [13, 66, 71, 80, 107, 132, 162]. Of the eight qualitative studies, seven (87.5%) presented evidence from multiple facilities [116, 120, 124, 151, 152, 163, 164] and one (12.5%) described the experiences of a single facility [16]. The one study based on both primary and secondary quantitative data used evidence from multiple facilities [82].
Of the 38 studies that relied on primary quantitative data, 20 (52.6%) included both residents and staff as participants [12, 17, 21, 28, 33, 67, 68, 75, 91, 97, 114, 117, 119, 126, 135, 136, 143, 147, 149, 158], 10 (26.3%) focused on staff [23, 70, 74, 87, 93, 109, 112, 113, 145, 161], six (15.8%) focused on residents [11, 14, 15, 19, 96, 127], and two (5.3%) collected facility-level data [22, 40]. Of the 39 studies that analyzed secondary quantitative data, 27 (69.2%) used facility-level data [18, 34,35,36,37,38,39, 41, 50, 76, 89, 92, 100,101,102,103, 106, 108, 110, 111, 118, 122, 123, 129, 137, 139, 148], nine (23.1%) included both residents and staff as participants [13, 20, 66, 71, 80, 105, 107, 132, 162], one (2.6%) focused on residents [77], one (2.6%) employed municipal- and facility-level data [69], and one (2.6%) used facility- and resident-level data [72]. The one study that combined primary and secondary quantitative data performed a facility-level analysis [82]. All participants in the eight qualitative studies were staff members [16, 116, 120, 124, 151, 152, 163, 164].
COVID-19 pandemic timeframe
To situate the evidence within the temporal progression of the COVID-19 pandemic, we plotted the period of data collection or analysis for the 95 research articles (see Fig. 4). Most research articles (81/95, 85.3%) used one or more consecutive weeks/months during 2020 as their period of data collection or analysis [8, 11,12,13,14,15,16,17,18,19,20,21,22,23, 28, 33,34,35,36,37,38,39,40,41, 43, 46, 50, 66,67,68,69,70,71,72, 75, 82, 91,92,93, 96, 97, 100, 102, 103, 105,106,107,108,109,110,111,112,113,114, 116,117,118,119,120, 122,123,124, 126,127,128, 132, 136, 137, 142, 143, 145, 147,148,149, 151, 152, 158, 161,162,163,164]. In addition, of the 95 research articles, eleven (11.6%) articles used a period beginning in 2020 and extending into 2021 [45, 47, 48, 55, 74, 76, 87, 89, 101, 129, 139], one (1.1%) article focused on a 2-month period in 2021 [80], one (1.1%) article reported results of an interventional study conducted between April 2019 and March 2021 [135], and one (1.1%) article covered two non-consecutive periods, one corresponding to the first wave of the pandemic in 2020 and the other to the second wave in 2021 [77].

Plot of the period of data collection/analysis for research articles (n = 95); numbers represent the number of articles covering each period. *Data collection began in 2019
Frameworks
Of the 140 articles, 12 (8.6%) applied a conceptual or theoretical framework, including: a checklist of measurable IPC practices adapted from guidelines for managing COVID-19 in LTCFs [16]; an adapted organizational framework analysis focusing on social ties and the interdependency between individuals and organizations [120]; Barker’s behavior setting theory [161]; Ernst and Chrobot-Mason’s framework of boundary spanning leadership [81]; a “fuzzy comprehensive evaluation method” that integrates internal and external factors to evaluate performance in terms of IPC [112]; the organizational crisis management theory [112]; the health and social care framework [45]; the Infection Prevention and Control Assessment and Response Tool [40]; the Plan-Do-Study-Act Cycle [14]; Macrae and Wiig’s resilience framework [116]; the vulnerable population conceptual framework [162]; Behrens and Naylor’s operational framework for a coordinated response to the COVID-19 pandemic [153]; and the framework of the determinants of the risk of severe infection in conjunction with the concept of deep defense within infection management [134].
Dimensions of LTCF performance
Table 3 displays dimension(s) of LTCF performance extracted from all retained articles. Efficacy and safety were the most frequently discussed dimensions; these were extracted from 106 (75.7%) of the 140 articles each, followed by viability (81/140, 57.9%), continuity (43/140, 30.7%), accessibility (38/140, 27.1%), and reactivity (37/140, 26.4%). Equity and efficiency were the least frequently addressed dimensions; these were extracted from 19 (13.6%) and 18 (12.9%) articles, respectively.
Factors that influenced COVID-19 management in LTCFs
Factors that were discussed in relation to the management of COVID-19 within LTCFs were extracted from all 140 articles (see Table 4). Among internal factors, “organizational context” and “human resources” were the most frequently reported factors; these were extracted from 102 (72.9%) and 87 (62.1%) of the 140 articles, respectively, followed by “material resources” (63/140, 45.0%), “facility characteristics” (53/140, 37.9%), “staff characteristics” (52/140, 37.1%), “resident characteristics” (37/140, 26.4%), “technological resources” (26/140, 18.6%), and “financial resources” (18/140, 12.9%) (see Table 4). Among external factors, “visitors” and “public health policies/guidelines” were the most frequently reported factors; these were extracted from 38 (27.1%) and 36 (25.7%) of the 140 articles, respectively, followed by “virus circulation in the community” (22/140, 15.7%), and “admissions” (17/140, 12.1%). Sixteen (11.4%) articles reported factors that were extracted under the category “Other”. These included asymptomatic or atypical presentation of COVID-19, the lack of knowledge about COVID-19 symptoms, and vaccination.
Discussion
This scoping review identified and synthesized factors that could influence LTCF performance by analyzing a vast body of international literature from early in the COVID-19 pandemic until the end of 2021. By applying a multidimensional conceptual framework of healthcare system performance, this study brings to light various factors that were reported to have influenced the accessibility and quality of healthcare services during the pandemic, how the available resources were optimized, and how these parameters contributed to overall LTCF performance.
LTCF performance during the COVID-19 pandemic
The majority of included articles considered the performance of a single or multiple LTCF(s) along the dimensions of efficacy (75.7%) and safety (75.7%). As per this review’s conceptual framework, these two dimensions gauge healthcare system performance in terms of the quality of the services provided. This finding reflects the urgency of the pandemic response demanded from LTCF management around the world, which led to the prioritization of the delivery of safe care amidst a public health crisis. Efficacy was predominantly discussed in terms of the degree to which IPC interventions implemented by LTCFs were successful at decreasing the transmission of COVID-19 or managing COVID-19 outbreaks once they occurred. Effective reduction of COVID-19 incidence, morbidity, and mortality was linked to early implementation of and adherence to IPC measures, including: the use of personal protective equipment (PPE), hand hygiene, sanitation, isolation, universal serial testing of residents and staff, cohorting, vaccination, visitor restrictions, and the availability of IPC trained staff (e.g., [11, 12, 15,16,17,18, 43, 71, 73, 76, 79, 80, 85, 105, 115, 121, 129]). Furthermore, close integration between acute and long-term care, communication between LTCFs and public health authorities, and access to a multidisciplinary clinical team emerged as strategies that contributed to a more successful COVID-19 response (e.g., [8, 21, 31, 81, 109, 124]). In terms of safety, IPC measures put in place by LTCFs to limit viral spread were most commonly reported. Multiple publications provided evidence of how LTCF staff acted as vectors of COVID-19 introduction and transmission, for example when working at multiple facilities or when not using PPE properly, if at all, due to severe resource shortages (e.g., [24, 79, 141]). Safety risks associated with LTCF staff working at multiple facilities can be addressed by asking staff to reside with residents under isolation, which was reported to be effective at reducing COVID-19 incidence and mortality [48, 75]. However, the implementation of any IPC protocol must be weighed against its potential impact on the mental health of residents and staff and on overall quality of life. One proposed antidote to negative mental health outcomes as a consequence of strict IPC measures was a person-centered approach to long-term care, where the delivery of care is negotiated between the LTCF resident and the healthcare professional and delivered in a personalized and respectful manner [94].
Approximately 13% of the included articles considered LTCF performance along the dimensions of efficiency and equity, which evaluate performance in terms of the optimization of resources and the accessibility of services, respectively. Staff producing their own PPE, allocation of unused areas for staff self-confinement, storage of material supplies by pharmacies for distribution to multiple LTCFs, and technological innovations, such as portable infection equipment trolleys, were highlighted as strategies employed by some LTCFs to ensure an efficient use of available resources (e.g., [75, 81, 116, 120]). In relation to equity, several articles, most of which originated in the USA, noted how the COVID-19 pandemic put a spotlight on the existing health inequities and, in some cases, exacerbated them among already vulnerable populations, notably low-income individuals and communities of color (e.g., [72, 90, 162]). An association was commonly reported between a LTCF housing a greater proportion of racial/ethnic minority residents and a higher probability of COVID-19 cases (e.g., [35, 39, 43, 48]).
The two most frequently extracted dimensions of performance, efficacy and safety, are strongly linked to the two factors most commonly reported by the included articles—organizational context (72.9%) and human resources (62.1%). This finding underscores the pressing need for increased investment in long-term care infrastructure and workforce globally to ensure satisfactory working conditions, job security, decent pay, and adequate levels of staff who are competent in IPC, geriatrics, and palliative care [166]. Enforcement of safety standards and continuous human resource development are necessary steps towards reductions in staff absenteeism and turnover rates, better continuity of care, and improved care delivery [166].
About one in nine (11.4%) articles included in the review noted unexpected factors, including: the initial lack of knowledge about the virus and the symptoms it causes [42, 78, 132]; the difficulty detecting and managing asymptomatic and atypical COVID-19 cases [13, 43, 48, 68, 94, 114, 134] which was subsequently addressed by universal serial testing of residents and staff [23, 73, 130]; and the ability to curb COVID-19 transmission with early administration of vaccines [32, 129].
Our findings are in line with a scoping review by Giri et al. [48], which showed that the ability of LTCFs to contain COVID-19 outbreaks was influenced by an interplay of various internal (related to residents, staff, and facilities) and external (material resources and public health policies) factors, as well as asymptomatic transmission of COVID-19. Building on Giri et al.’s classification of factors, our review provides a more fine-grained understanding of why some LTCFs performed better than others by extracting a greater number of factors and linking these factors to multiple dimensions of performance using a conceptual framework. Furthermore, our findings emphasized the contribution of the LTCF’s organizational structure and the quality of its leadership to the facility’s capacity to effectively respond to the COVID-19 pandemic. Organizational challenges leading to shortages of staff and material resources during the first wave of the pandemic were also highlighted by Palacios-Ceña et al.’ [45] scoping review of qualitative evidence. Consistent with our findings, this narrative synthesis found evidence of LTCF staff taking initiative in procuring supplies by cultivating connections within the community.
Directions for future research
The descriptive characteristics of the articles included in our scoping review revealed a gap in the existing knowledge pertaining to the performance of LTCFs during the COVID-19 pandemic. First, except for one quasi-experimental pre-post study [22], all research articles included in our review were non-experimental studies, which precludes the establishment of causality between the identified factors and LTCF performance. Therefore, experimental studies should be prioritized in the future to help understand which factors could predict LTCF performance during the ongoing COVID-19 pandemic or future outbreaks. When experimental designs are not feasible, qualitative studies can help gain a deeper, more nuanced understanding of the various factors that facilitated or hindered the management of COVID-19 in LTCFs by gleaning perspectives of diverse stakeholders, such as facility leadership and staff, residents and their families, and public health officials [167]. Second, the majority of research articles in our review were cross-sectional, thus providing only a snapshot of LTCF response to COVID-19, with the bulk of evidence coming from the first wave of the pandemic (between March and July 2020). The skewness towards the early phases of the pandemic might have been behind efficacy and safety being the most commonly reported dimensions of performance, reflecting the urgency to provide care to LTCF residents in a safe and effective manner amidst a public health crisis. Additional population-based longitudinal studies are warranted to explore long-term impacts of the reported factors on LTCF performance [168]. Third, only 9% of the included articles used a framework to guide their inquiry. We recommend future studies adopt a framework to help understand complex healthcare systems, as it would allow for inter-study comparability and a fine-grained analysis of structures and processes that influence the delivery and outcomes of care [169]. Fourth, a few articles included in our review discussed LTCF performance as a function of the dimensions of efficiency and equity. Thus, more research is needed to examine LTCF performance in terms of the optimization of available resources and fair access to services both in the context of the COVID-19 pandemic and more broadly. Fifth, the reviewed qualitative literature mostly examined the practices and perspectives of LTCF staff. Studies exploring LTCF residents’ experiences in the pandemic context, for example with respect to their feelings of loneliness, may provide valuable information that could help maintain and improve residents’ quality of life (e.g., [170, 171]). Lastly, of the 11 Canadian-based studies included in our review, 10 originated in the provinces of Ontario and British Columbia, and only one came from Québec. This represents a substantial knowledge gap given that Québec experienced the highest COVID-19 mortality rate in Canada between March 2020 and October 2021 [172]. Future work should examine the failures of IPC in hard-hit regions of the world to obtain insight into the causes and mechanisms of inadequate healthcare, as well as provide opportunities to innovate and apply higher quality care in the future [173, 174].
Limitations and strengths
Due to the evolving nature of the COVID-19 pandemic, the results of this review may not reflect the current public health profile. Furthermore, because our review focused on the management of COVID-19, the findings may not fully capture indirect effects of the IPC measures implemented by LTCFs that have, nonetheless, had an influence on residents’ mental health. For example, the restriction or prohibition of family visits and group activities in LTCFs resulted in residents experiencing social isolation and loneliness [175,176,177]. Though six databases were used for queries we could have included more. We did not search for articles written in languages other than English or French, and French articles that were retrieved were screened and excluded.
Despite these limitations, our study offers a comprehensive review of various factors reported to have influenced the management of COVID-19 within LTCFs by applying a multidimensional conceptual framework of performance. The adopted framework guided us throughout the entire review process by providing a clear focus on our review’s aim and objectives. In addition to the conceptual framework, adherence to the JBI methodology for scoping reviews helped us maintain the overall rigor of the study. This work may inform the development of more effective IPC interventions to help prevent or mitigate future outbreaks in LTCFs, while being sensitive to the needs, preferences, and values of residents and staff. The lessons learned thus far should be considered on an evolving basis when developing IPC programs specific to long-term care.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
Abbreviations
- DS:
-
Drissa Sia
- EB:
-
Emilie Bélanger
- ENT:
-
Eric Nguemeleu Tchouaket
- IPC:
-
Infection prevention and control
- IS:
-
Idrissa Beogo
- JBI:
-
Joanna Briggs Institute
- JL:
-
Josiane Létourneau
- KK:
-
Katya Kruglova
- LTCFs:
-
Long-term care facilities
- MJ:
-
Maripier Jubinville
- MSSS:
-
Ministère de la Santé et des Services Sociaux
- OECD:
-
Organisation for Economic Co-operation and Development
- PRISMA-P:
-
Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols
- PRISMA-ScR:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews
- SR:
-
Stephanie Robins
- SS:
-
Shiyang Shen
References
World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19 - 11 March 2020. 2020. https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-11-march-2020. Accessed 20 July 2021.
Leung NH. Transmissibility and transmission of respiratory viruses. Nat Rev Microbiol. 2021;19(8):528–45.
Comas-Herrera A, Zalakaín J, Lemmon E, Henderson D, Litwin C, Hsu A, et al. Mortality associated with COVID-19 in care homes: international evidence. International Long Term Care Policy Network; 2020.
Sepulveda ER, Stall NM, Sinha SK. A comparison of COVID-19 mortality rates among long-term care residents in 12 OECD countries. JAMDA. 2020;21(11):1572-4.e3. https://doi.org/10.1016/j.jamda.2020.08.039.
TchouaketNguemeleu E, Robins S, Sia D, Létourneau J, Borgès Da Silva R, Kilpatrick K, et al. Validation and pilot testing of a guide to measure the costs associated with the management of COVID-19 and of healthcare associated infections in residential and long-term care facilities in Quebec. Sci Nurs Health Pract. 2021;4(1):1–31. https://doi.org/10.7202/1077991ar.
Rocard E, Sillitti P, Llena-Nozal A. COVID-19 in long-term care: Impact, policy responses and challenges. OECD Health Working Papers No 131. 2021. https://doi.org/10.1787/b966f837-en.
National Institute on Ageing. Counting COVID-19 in Canada’s long-term care homes: NIA long-term care COVID-19 Tracker project summary report. Toronto: National Institute on Ageing, Toronto Metropolitan University; 2022.
Dykgraaf SH, Matenge S, Desborough J, Sturgiss E, Dut G, Roberts L, et al. Protecting nursing homes and long-term care facilities from COVID-19: a rapid review of international evidence. JAMDA. 2021;22(10):1969–88. https://doi.org/10.1016/j.jamda.2021.07.027.
Usher K, Durkin J, Gyamfi N, Warsini S, Jackson D. Preparedness for viral respiratory infection pandemic in residential aged care facilities: a review of the literature to inform post-COVID-19 response. J Clin Nurs. 2021. https://doi.org/10.1111/jocn.15863.
Ayukekbong J. Infection prevention and control in long-term care: lessons learned from COVID-19 outbreaks and future perspectives. Can J Infect Control. 2021;36(1):16–9.
Bigelow BF, Tang O, Barshick B, Peters M, Sisson SD, Peairs KS, et al. Outcomes of universal COVID-19 testing following detection of incident cases in 11 long-term care facilities. JAMA Inter Med. 2021;181(1):127–9. https://doi.org/10.1001/jamainternmed.2020.3738.
Eckardt P, Guran R, Hennemyre J, Arikupurathu R, Poveda J, Miller N, et al. Hospital affiliated long term care facility COVID-19 containment strategy by using prevalence testing and infection control best practices. Am J Infect Control. 2020;48(12):1552–5. https://doi.org/10.1016/j.ajic.2020.06.215.
Escobar DJ, Lanzi M, Saberi P, Love R, Linkin DR, Kelly JJ, et al. Mitigation of a coronavirus disease 2019 outbreak in a nursing home through serial testing of residents and staff. Clin Infect Dis. 2021;72(9):e394–6. https://doi.org/10.1093/cid/ciaa1021.
Finger HJ, Rao RN, Sansone GR, Hazel EJ, Silvestri-Tan CT. Newly developed COVID-19 bundle greatly reduces the infection fatality rate for a highly vulnerable nursing home population. Am J Med Qual. 2021;37(1):46–54. https://doi.org/10.1097/01.JMQ.0000741984.07868.d4.
Goto M, Ueckert N, Meiches RK, Perencevich EN. Successful multimodal measures preventing coronavirus disease 2019 (COVID-19) outbreaks without universal frequent testing within long-term care units in the Midwestern Veterans’ Health Care Network. Infect Control Hosp Epidemiol. 2021;42(12):1503–5. https://doi.org/10.1017/ice.2020.1419.
Havaei F, MacPhee M, Keselman D, Staempfli S. Leading a long-term care facility through the COVID-19 crisis: successes, barriers and lessons learned. Healthc Q. 2021;23(4):28–34. https://doi.org/10.12927/hcq.2020.26396.
Krone M, Noffz A, Richter E, Vogel U, Schwab M. Control of a COVID-19 outbreak in a nursing home by general screening and cohort isolation in Germany. Euro Surveill. 2021;26(1):2001365. https://doi.org/10.2807/1560-7917.ES.2021.26.1.2001365.
Lipsitz LA, Lujan AM, Dufour A, Abrahams G, Magliozzi H, Herndon L, et al. Stemming the tide of COVID-19 infections in Massachusetts nursing homes. J Am Geriatr Soc. 2020;68(11):2447–53. https://doi.org/10.1111/jgs.16832.
Montoya A, Jenq G, Mills JP, Beal J, Chun ED, Newton D, et al. Partnering with local hospitals and public health to manage COVID-19 outbreaks in nursing homes. J Am Geriatr Soc. 2021;69(1):30–6. https://doi.org/10.1111/jgs.16869.
Park SY, Choi G, Lee H, Kim NY, Lee SY, Kim K, et al. Early intervention reduces the spread of covid-19 in long-term care facilities in the Republic of Korea. Osong Public Health Res Perspect. 2020;11(4):259–64. https://doi.org/10.24171/j.phrp.2020.11.4.16.
Poupin P, N’Diaye D, Chaumier F, Lemaignen A, Bernard L, Fougere B. Management of COVID-19 in a French nursing home: experiences from a multidisciplinary mobile team. J Frailty Aging. 2021;10(4):363–6. https://doi.org/10.14283/jfa.2021.16.
Vijh R, Prairie J, Otterstatter MC, Hu Y, Hayden AS, Yau B, et al. Evaluation of a multisectoral intervention to mitigate the risk of severe acute respiratory coronavirus virus 2 (SARS-CoV-2) transmission in long-term care facilities. Infect Control Hosp Epidemiol. 2021;42(10):1181–8. https://doi.org/10.1017/ice.2020.1407.
Bayle C, Cantin D, Vidal J-S, Sourdeau E, Slama L, Dumesges N, et al. Asymptomatic SARS COV-2 carriers among nursing home staff: a source of contamination for residents? Infect Dis Now. 2021;51(2):197–200. https://doi.org/10.1016/j.idnow.2020.11.008.
Liu M, Maxwell CJ, Armstrong P, Schwandt M, Moser A, McGregor MJ, et al. COVID-19 in long-term care homes in Ontario and British Columbia. Can Med Assoc J. 2020;192(47):E1540–6. https://doi.org/10.1503/cmaj.201860.
Abbasi J. “Abandoned” nursing homes continue to face critical supply and staff shortages as COVID-19 toll has mounted. JAMA. 2020;324(2):123–5. https://doi.org/10.1001/jama.2020.10419.
Arlotti M, Ranci C. The impact of COVID-19 on nursing homes in Italy: the case of Lombardy. J Aging Soc Policy. 2021;33(4–5):431–43. https://doi.org/10.1080/08959420.2021.1924344.
Beaulieu M, Cadieux Genesse J, St-Martin K. High death rate of older persons from COVID-19 in Quebec (Canada) long-term care facilities: chronology and analysis. J Adult Prot. 2021;23(2):110–5. https://doi.org/10.1108/JAP-08-2020-0033.
Bernadou A, Bouges S, Catroux M, Rigaux JC, Laland C, Levêque N, et al. High impact of COVID-19 outbreak in a nursing home in the Nouvelle-Aquitaine region, France, March to April 2020. BMC Infect Dis. 2021;21(1):198. https://doi.org/10.1186/s12879-021-05890-6.
Chapman S, Harrington C. Policies matter! Factors contributing to nursing home outbreaks during the COVID-19 pandemic. Policy Polit Nurs Pract. 2020;21(4):191–2. https://doi.org/10.1177/1527154420959021.
Cigler BA. Nursing homes and COVID-19: one state’s experience. Int J Public Adm. 2021;44(11–12):963–73. https://doi.org/10.1080/01900692.2021.1937216.
Deschacht M, Malfait S, Eeckloo K. Integrated care for older adults during the COVID-19 pandemic in Belgium: lessons learned the hard way. Int J Older People Nurs. 2021;16(3):e12366. https://doi.org/10.1111/opn.12366.
Power GA, Carson J. The promise of transformed long-term care homes: evidence from the pandemic. Healthc Manage Forum. 2021;35(1):25–8. https://doi.org/10.1177/08404704211037794.
Zollner-Schwetz I, König E, Krause R, Pux C, Laubreiter L, Schippinger W. Analysis of COVID-19 outbreaks in 3 long-term care facilities in Graz, Austria. Am J Infect Control. 2021;49(11):1350–3. https://doi.org/10.1016/j.ajic.2021.08.006.
Gopal R, Han X, Yaraghi N. Compress the curve: a cross-sectional study of variations in COVID-19 infections across California nursing homes. BMJ Open. 2021;11(1):e042804. https://doi.org/10.1136/bmjopen-2020-042804.
Gorges RJ, Konetzka RT. Staffing levels and COVID-19 cases and outbreaks in U.S. nursing homes. J Am Geriatr Soc. 2020;68(11):2462–6. https://doi.org/10.1111/jgs.16787.
Gorges RJ, Konetzka RT. Factors associated with racial differences in deaths among nursing home residents with COVID-19 infection in the US. JAMA Netw Open. 2021;4(2):e2037431. https://doi.org/10.1001/jamanetworkopen.2020.37431.
Harrington C, Ross L, Chapman S, Halifax E, Spurlock B, Bakerjian D. Nurse staffing and coronavirus infections in California nursing homes. Policy Polit Nurs Pract. 2020;21(3):174–86. https://doi.org/10.1177/1527154420938707.
Khairat S, Zalla LC, Adler-Milstein J, Kistler CE. US nursing home quality ratings associated with COVID-19 cases and deaths. JAMDA. 2021;22(10):2021–5. https://doi.org/10.1016/j.jamda.2021.07.034.
Li Y, Cen X, Cai X, Temkin-Greener H. Racial and ethnic disparities in COVID-19 infections and deaths across US nursing homes. J Am Geriatr Soc. 2020;68(11):2454–61. https://doi.org/10.1111/jgs.16847.
Telford CT, Bystrom C, Fox T, Holland DP, Wiggins-Benn S, Mandani A, et al. COVID-19 infection prevention and control adherence in long-term care facilities, Atlanta, Georgia. J Am Geriatr Soc. 2021;69(3):581–6. https://doi.org/10.1111/jgs.17001.
Abrams HR, Loomer L, Gandhi A, Grabowski DC. Characteristics of U.S. nursing homes with COVID-19 cases. JAGS. 2020;68(8):1653–6. https://doi.org/10.1111/jgs.16661.
Heckman GA, Kay K, Morrison A, Grabowski DC, Hirdes JP, Mor V, et al. Proceedings from an International Virtual Townhall: reflecting on the COVID-19 pandemic: themes from long-term care. JAMDA. 2021;22(6):1128–32. https://doi.org/10.1016/j.jamda.2021.03.029.
Gmehlin C, Munoz-Price LS. Coronavirus disease 2019 (COVID-19) in long-term care facilities: a review of epidemiology, clinical presentations, and containment interventions. Infect Control Hosp Epidemiol. 2020;43(4):504–9. https://doi.org/10.1017/ice.2020.1292.
Calcaterra L, Cesari M, Lim WS. Long-term care facilities (LTCFs) during the COVID-19 pandemic—lessons from the Asian approach: a narrative review. JAMDA. 2022;23(3):399–404.
Palacios-Ceña D, Fernández-Peña R, Ortega-López A, Fernández-Feito A, Bautista-Villaécija O, Rodrigo-Pedrosa O, et al. Long-term care facilities and nursing homes during the first wave of the COVID-19 pandemic: a scoping review of the perspectives of professionals, families and residents. Int J Environ Res Public Health. 2021;18(19):10099. https://doi.org/10.3390/ijerph181910099.
Frazer K, Mitchell L, Stokes D, Lacey E, Crowley E, Kelleher CC. A rapid systematic review of measures to protect older people in long-term care facilities from COVID-19. BMJ Open. 2021;11(10):e047012.
Konetzka RT, White EM, Pralea A, Grabowski DC, Mor V. A systematic review of long-term care facility characteristics associated with COVID-19 outcomes. J Am Geriatr Soc. 2021;69(10):2766–77. https://doi.org/10.1111/jgs.17434.
Giri S, Chenn LM, Romero-Ortuno R. Nursing homes during the COVID-19 pandemic: a scoping review of challenges and responses. Eur Geriatr Med. 2021;12(6):1127–36. https://doi.org/10.1007/s41999-021-00531-2.
Ministère de la Santé et des Services Sociaux. Cadre de référence ministériel d’évaluation de la performance du système public de santé et de services sociaux à des fins de gestion. 2012.
Braun RT, Yun H, Casalino LP, Myslinski Z, Kuwonza FM, Jung H-Y, et al. Comparative performance of private equity–owned US nursing homes during the COVID-19 pandemic. JAMA Netw Open. 2020;3(10):e2026702. https://doi.org/10.1001/jamanetworkopen.2020.26702.
Wilmink G, Summer I, Marsyla D, Sukhu S, Grote J, Zobel G, et al. Real-time digital contact tracing: development of a system to control COVID-19 outbreaks in nursing homes and long-term care facilities. JMIR Public Health Surveill. 2020;6(3):e20828. https://doi.org/10.2196/20828.
Kelley E, Hurst J. Health care quality indicators project: conceptual framework paper. OECD Health Working Papers. 2006. https://doi.org/10.1787/440134737301.
Canadian Institute for Health Information. Health indicators 2011. Ottawa: CIHI; 2011.
Ministère de la Santé et des Services Sociaux. Cadre de référence ministériel d’évaluation de la performance du système public de santé et de services sociaux à des fins de gestion. Québec: Government of Québec; 2012.
Stratil JM, Biallas RL, Burns J, Arnold L, Geffert K, Kunzler AM, et al. Non-pharmacological measures implemented in the setting of long-term care facilities to prevent SARS-CoV-2 infections and their consequences: a rapid review. Cochrane Database Syst Rev. 2021;9(9):CD015085.
Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H. Chapter 11: scoping reviews (2020 version) In: Aromarits E, Munn Z, editors. JBI manual for evidence synthesis. 2020.
Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. JBI Evid Implement. 2015;13(3):141–6. https://doi.org/10.1097/XEB.0000000000000050.
Tricco A, Lillie E, Zarin W, O’Brien K, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73. https://doi.org/10.7326/M18-0850.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. 2021;134:103–12.
Joanna Briggs Institute. Appendix 11.2 PRISMA ScR extension fillable checklist. 2021.
Létourneau J, Bélanger E, Sia D, Beogo I, Robins S, Kruglova K, et al. Identifying performance factors of long-term care facilities in the context of the COVID-19 pandemic: a scoping review protocol. Syst Rev. 2022;11(1):203.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):1–10. https://doi.org/10.1186/s13643-016-0384-4.
Tchouaket EN, Beogo I, Sia D, Kilpatrick K, Séguin C, Baillot A, et al. Protocol for a systematic review of economic analyses of nosocomial infection prevention and control interventions in OECD hospitals. BMJ Open. 2020;10(7):e037765. https://doi.org/10.1136/bmjopen-2020-037765.
Gwet KL. Handbook of inter-rater reliability: the definitive guide to measuring the extent of agreement among raters. Gaithersburg: Advanced Analytics, LLC; 2014.
O’Connor C, Joffe H. Intercoder reliability in qualitative research: debates and practical guidelines. Int J Qual Methods. 2020;19:1609406919899220.
Abe T, Tokuda Y, Iriyama H, Iwagami M, Komori A, Sugiyama T, et al. Surgical mask use by healthcare personnel to prevent COVID-19 spread in a long-term care facility. J Gen Fam Med. 2020;22(2):100–3. https://doi.org/10.1002/jgf2.394.
Agostinis P, Vianello V, Dereani E, Caruso G, Montessoro B, Taurian M, et al. Response to a massive SARS-CoV-2 infection in a nursing home transformed into a caring center. Aging Clin Exp Res. 2021;33(2):443–50. https://doi.org/10.1007/s40520-020-01784-w.
Alawi MMS. Successful management of COVID-19 outbreak in a long-term care facility in Jeddah, Saudi Arabia: epidemiology, challenges for prevention and adaptive management strategies. Am J Public Health. 2021;14(4):521–6. https://doi.org/10.1016/j.jiph.2020.12.036.
Amore S, Puppo E, Melara J, Terracciano E, Gentili S, Liotta G. Impact of COVID-19 on older adults and role of long-term care facilities during early stages of epidemic in Italy. Sci Rep. 2021;11(1):12530. https://doi.org/10.1038/s41598-021-91992-9.
Archbald-Pannone LR, Harris DA, Albero K, Steele RL, Pannone AF, Mutter JB. COVID-19 collaborative model for an academic hospital and long-term care facilities. JAMDA. 2020;21(7):939–42. https://doi.org/10.1016/j.jamda.2020.05.044.
Aykaç N, Yüksel Eryiğit Ö, Elbek O. Evaluation of the measures taken in nursing homes of the Istanbul metropolitan municipality during the COVID-19 pandemic. Turk J Geriatr. 2021;24(1):13–22. https://doi.org/10.31086/tjgeri.2021.195.
Bach-Mortensen AM, Degli EM. Is area deprivation associated with greater impacts of COVID-19 in care homes across England? A preliminary analysis of COVID-19 outbreaks and deaths. J Epidemiol Community Health. 2021;75:624–7. https://doi.org/10.1136/jech-2020-215039.
Bakaev I, Retalic T, Chen H. Universal testing-based response to COVID-19 outbreak by a long-term care and post-acute care facility. J Am Geriatr Soc. 2020;68(7):E38–9. https://doi.org/10.1111/jgs.16653.
Baughman AW, Renton M, Wehbi NK, Sheehan EJ, Gregorio TM, Yurkofsky M, et al. Building community and resilience in Massachusetts nursing homes during the COVID-19 pandemic. J Am Geriatr Soc. 2021;69(10):2716–21. https://doi.org/10.1111/jgs.17389.
Belmin J, Um-Din N, Donadio C, Magri M, Nghiem QD, Oquendo B, et al. Coronavirus disease 2019 outcomes in French nursing homes that implemented staff confinement with residents. JAMA Netw Open. 2020;3(8):e2017533. https://doi.org/10.1001/jamanetworkopen.2020.17533.
Benin AL, Soe MM, Edwards JR, Bagchi S, Link-Gelles R, Schrag SJ, et al. Ecological analysis of the decline in incidence rates of COVID-19 among nursing home residents associated with vaccination, United States, December 2020-January 2021. JAMDA. 2021;22(10):2009–15. https://doi.org/10.1016/j.jamda.2021.08.004.
Benvenuti E, Rivasi G, Bulgaresi M, Barucci R, Lorini C, Balzi D, et al. Caring for nursing home residents with COVID-19: a “hospital-at-nursing home” intermediate care intervention. Aging Clin Exp Res. 2021;33(10):2917–24. https://doi.org/10.1007/s40520-021-01959-z.
Bertrand C, Laurent M, Lecarpentier E. SAMU and residential care homes (EHPAD) COVID cell crisis. Méd Catastrophe Urgences Collect. 2020;4(3):209–11. https://doi.org/10.1016/j.pxur.2020.07.004.
Blain H, Rolland Y, Schols JMGA, Cherubini A, Miot S, O’Neill D, et al. August 2020 Interim EuGMS guidance to prepare European long-term care facilities for COVID-19. Eur Geriatr Med. 2020;11(6):899–913. https://doi.org/10.1007/s41999-020-00405-z.
Burugorri-Pierre C, Lafuente-Lafuente C, Oasi C, Lecorche E, Pariel S, Donadio C, et al. Investigation of an outbreak of COVID-19 in a French nursing home with most residents vaccinated. JAMA Netw Open. 2021;4(9):e2125294. https://doi.org/10.1001/jamanetworkopen.2021.25294.
Caramanica L, O’Rourke P. Boundary spanning leadership in response to the COVID-19 pandemic: experience of nurse leaders in a large integrated long-term health care system. Nurs Adm Q. 2021;45(4):277–84. https://doi.org/10.1097/NAQ.0000000000000488.
Cazzoletti L, Zanolin ME, Tocco Tussardi I, Alemayohu MA, Zanetel E, Visentin D, et al. Risk factors associated with nursing home COVID-19 outbreaks: a retrospective cohort study. Int J Environ Res Public Health. 2021;18(16):8434. https://doi.org/10.3390/ijerph18168434.
Chan DKY, McLaws M-L, Forsyth DR. COVID-19 in aged care homes: a comparison of effects initial government policies had in the UK (primarily focussing on England) and Australia during the first wave. Int J Qual Health Care. 2021;33(1):1–6. https://doi.org/10.1093/intqhc/mzab033.
Chen C-R, Huang H-C, Wei C. Preparing for COVID-19: the experiences of a long-term care facility in Taiwan. Geriatr Gerontol Int. 2020;20(7):734–5. https://doi.org/10.1111/ggi.13943.
Cheng HWB. Combating coronavirus disease-2019 outbreak in long-term care facilities for frail older adults: preventive measures and palliative care go hand-in-hand. J Palliat Care. 2021;37:8–12. https://doi.org/10.1177/08258597211039364.
Chu CH, Wang J, Fukui C, Staudacher S, Wachholz PA, Wu B. The impact of COVID-19 on social isolation in long-term care homes: perspectives of policies and strategies from six countries. J Aging Soc Policy. 2021;33(4–5):459–73. https://doi.org/10.1080/08959420.2021.1924346.
Coulongeat M, Aïdoud A, Poupin P, Dubnitskiy-Robin S, Fougère B. A local COVID-19 support platform for nursing homes: feedback and perspectives. JAMDA. 2021;22(8):1599–601. https://doi.org/10.1016/j.jamda.2021.06.001.
Daly M. COVID-19 and care homes in England: what happened and why? Soc Policy Adm. 2020;54(7):985–98. https://doi.org/10.1111/spol.12645.
Das Gupta D, Kelekar U, Turner SC, Sule AA, Jerman TG. Interpreting COVID-19 deaths among nursing home residents in the US: the changing role of facility quality over time. PLoS One. 2021;16(9):e0256767. https://doi.org/10.1371/journal.pone.0256767.
Dawson WD, Boucher NA, Stone R, Van Houtven CH. COVID-19: the time for collaboration between long-term services and supports, health care systems, and public health is now. Milbank Q. 2021;99(2):565–94. https://doi.org/10.1111/1468-0009.12500.
de Man P, Paltansing S, Ong DSY, Vaessen N, van Nielen G, Koeleman JGM. Outbreak of coronavirus disease 2019 (COVID-19) in a nursing home associated with aerosol transmission as a result of inadequate ventilation. Clin Infect Dis. 2021;73(1):170–1. https://doi.org/10.1093/cid/ciaa1270.
Dean A, Venkataramani A, Kimmel S. Mortality rates from COVID-19 are lower in unionized nursing homes. Health Aff. 2020;39(11):1993–2001. https://doi.org/10.1377/hlthaff.2020.01011.
Dias A, Scavarda A, Reis A, Silveira H, Ebecken NFF. Managerial strategies for long-term care organization professionals: COVID-19 pandemic impacts. Sustainability. 2020;12(22):9682. https://doi.org/10.3390/su12229682.
Dichter MN, Sander M, Seismann-Petersen S, Köpke S. COVID-19: it is time to balance infection management and person-centered care to maintain mental health of people living in German nursing homes. Int Psychogeriatr. 2020;32(10):1157–60. https://doi.org/10.1017/S1041610220000897.
Doetter LF, Preuss B, Rothgang H. Taking stock of COVID-19 policy measures to protect Europe’s elderly living in long-term care facilities. Glob Soc Policy. 2021;21(3):529–49. https://doi.org/10.1177/14680181211013717.
Dolveck F, Strazzulla A, Noel C, Aufaure S, Tarteret P, de Pontfarcy A, et al. COVID-19 among nursing home residents: results of an urgent pre-hospital intervention by a multidisciplinary task force. Braz J Infect Dis. 2021;25(1):101039. https://doi.org/10.1016/j.bjid.2020.11.004.
Echeverría P, Mas Bergas MA, Puig J, Isnard M, Massot M, Vedia C, et al. COVIDApp as an innovative strategy for the management and follow-up of COVID-19 cases in long-term care facilities in Catalonia: implementation study. JMIR Public Health Surveill. 2020;6(3):e21163. https://doi.org/10.2196/21163.
Estévez-Abe M, Ide H. COVID-19 and long-term care policy for older people in Japan. J Aging Soc Policy. 2021;33(4–5):444–58. https://doi.org/10.1080/08959420.2021.1924342.
Eye of the storm. The Lamp: The Magazine of the NSW Nurses and Midwives’ Association. 2020;77(3):14–7.
Figueroa JF, Wadhera RK, Papanicolas I, Riley K, Zheng J, Orav EJ, et al. Association of nursing home ratings on health inspections, quality of care, and nurse staffing with COVID-19 cases. JAMA. 2020;324(11):1103–5. https://doi.org/10.1001/jama.2020.14709.
Gibson DM, Greene J. Admissions of COVID-positive patients to US nursing homes with personal protective equipment or staffing shortages. J Am Geriatr Soc. 2021;69(9):2393–403. https://doi.org/10.1111/jgs.17302.
Gilman M, Bassett MT. Characteristics and quality of nursing homes reporting COVID-19 admissions from hospitals. J Am Geriatr Soc. 2021;69(9):2440–2. https://doi.org/10.1111/jgs.17287.
Gmehlin CG, Rivera F, Ramos-Castaneda JA, Pezzin LE, Ehn D, Duthie EH, et al. SARS-CoV-2 and Wisconsin nursing homes: temporal dynamics during the COVID-19 pandemic. JAMDA. 2021;22(11):2233–9. https://doi.org/10.1016/j.jamda.2021.08.021.
Hard-hit nursing homes face catch-22 to reopen. Am J Nurs. 2020;120(9):15. https://doi.org/10.1097/01.NAJ.0000697568.96803.48.
Heudorf U, Müller M, Schmehl C, Gasteyer S, Steul K. COVID-19 in long-term care facilities in Frankfurt am Main, Germany: incidence, case reports, and lessons learned. GMS Hyg Infect Control. 2020;15:Doc26. https://doi.org/10.3205/dgkh000361.
Ibrahim JE, Li Y, McKee G, Eren H, Brown C, Aitken G, et al. Characteristics of nursing homes associated with COVID-19 outbreaks and mortality among residents in Victoria, Australia. Australas J Ageing. 2021;40(3):283–92. https://doi.org/10.1111/ajag.12982.
Kain D, Stall N, Brown K, McCreight L, Rea E, Kamal M, et al. A longitudinal, clinical, and spatial epidemiologic analysis of a large COVID-19 long-term care home outbreak. JAMDA. 2021;22(10):2003–8. https://doi.org/10.1016/j.jamda.2021.07.021.
Konetzka RT, Gorges RJ. Nothing much has changed: COVID-19 nursing home cases and deaths follow fall surges. J Am Geriatr Soc. 2021;69(1):46–7. https://doi.org/10.1111/jgs.16951.
Lamb MJ, La Delfa A, Sawhney M, Adams D, Abdel-Shahied K, Belfer T, et al. Implementation and evaluation of an IPAC SWAT team mobilized to long-term care and retirement homes during the COVID-19 pandemic: a pragmatic health system innovation. JAMDA. 2021;22(2):253–5. https://doi.org/10.1016/j.jamda.2020.11.033.
Li Y, Temkin-Greener H, Shan G, Cai X. COVID-19 infections and deaths among Connecticut nursing home residents: facility correlates. J Am Geriatr Soc. 2020;68(9):1899–906. https://doi.org/10.1111/jgs.16689.
Li Y, Fang F, He M. Exploring the N95 and surgical mask supply in US nursing homes during COVID-19. J Appl Gerontol. 2021;40(3):257–62. https://doi.org/10.1177/0733464820969015.
Liang Y, Xu J. Crisis response of nursing homes during COVID-19: evidence from China. Int Rev Econ Finance. 2021;72:700–10. https://doi.org/10.1016/j.iref.2020.12.024.
Lingum NR, Sokoloff LG, Meyer RM, Gingrich S, Sodums DJ, Santiago AT, et al. Building long-term care staff capacity during COVID-19 through just-in-time learning: evaluation of a modified ECHO model. JAMDA. 2021;22(2):238–44. https://doi.org/10.1016/j.jamda.2020.10.039.
Louie JK, Scott HM, DuBois A, Sturtz N, Lu W, Stoltey J, et al. Lessons from mass-testing for Coronavirus Disease 2019 in long-term care facilities for the elderly in San Francisco. Clin Infect Dis. 2021;72(11):2018–20. https://doi.org/10.1093/cid/ciaa1020.
Lum T, Shi C, Wong G, Wong K. COVID-19 and long-term care policy for older people in Hong Kong. J Aging Soc Policy. 2020;32(4–5):373–9. https://doi.org/10.1080/08959420.2020.1773192.
Lyng HB, Ree E, Wibe T, Wiig S. Healthcare leaders’ use of innovative solutions to ensure resilience in healthcare during the Covid-19 pandemic: a qualitative study in Norwegian nursing homes and home care services. BMC Health Serv Res. 2021;21:878. https://doi.org/10.1186/s12913-021-06923-1.
MacCannell T, Batson J, Bonin B, Kc A, Quenelle R, Strong B, et al. Genomic epidemiology and transmission dynamics of SARS-CoV-2 in congregate healthcare facilities in Santa Clara County, California. Clin Infect Dis. 2021;74(5):829–35. https://doi.org/10.1093/cid/ciab553.
Malikov K, Huang Q, Shi S, Stall NM, Tuite AR, Hillmer MP. Temporal associations between community incidence of COVID-19 and nursing home outbreaks in Ontario, Canada. JAMDA. 2021;22(2):260–2. https://doi.org/10.1016/j.jamda.2020.12.011.
Marossy A, Rakowicz S, Bhan A, Noon S, Rees A, Virk M, et al. A study of universal severe acute respiratory syndrome coronavirus 2 RNA testing among residents and staff in a large group of care homes in South London. J Infect Dis. 2021;223(3):381–8. https://doi.org/10.1093/infdis/jiaa565.
Marshall F, Gordon A, Gladman JRF, Bishop S. Care homes, their communities, and resilience in the face of the COVID-19 pandemic: interim findings from a qualitative study. BMC Geriatr. 2021;21:102. https://doi.org/10.1186/s12877-021-02053-9.
McBee SM, Thomasson ED, Scott MA, Reed CL, Epstein L, Atkins A, et al. Notes from the field: universal statewide laboratory testing for SARS-CoV-2 in nursing homes—West Virginia, April 21–May 8, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(34):1177–9. https://doi.org/10.15585/mmwr.mm6934a4.
McGarry BE, Grabowski DC, Barnett ML. Severe staffing and personal protective equipment shortages faced by nursing homes during the COVID-19 pandemic: study examines staffing and personal protective equipment shortages faced by nursing homes during the COVID-19 pandemic. Health Aff. 2020;39(10):1812–21.
McGarry BE, SteelFisher GK, Grabowski DC, Barnett ML. COVID-19 test result turnaround time for residents and staff in US nursing homes. JAMA Inter Med. 2021;181(4):556–9.
McGilton KS, Krassikova A, Boscart V, Sidani S, Iaboni A, Vellani S, et al. Nurse practitioners rising to the challenge during the coronavirus disease 2019 pandemic in long-term care homes. Gerontologist. 2021;61(4):615–23.
McGregor MJ, Harrington C. COVID-19 and long-term care facilities: does ownership matter? Can Med Assoc J. 2020;192(33):E961–2.
Miller SL, Mukherjee D, Wilson J, Clements N, Steiner C. Implementing a negative pressure isolation space within a skilled nursing facility to control SARS-CoV-2 transmission. Am J Infect Control. 2021;49(4):438–46. https://doi.org/10.1016/j.ajic.2020.09.014.
Mills WR, Buccola JM, Sender S, Lichtefeld J, Romano N, Reynolds K, et al. Home-based primary care led-outbreak mitigation in assisted living facilities in the first 100 days of coronavirus disease 2019. JAMDA. 2020;21(7):951–3.
Miralles O, Sanchez-Rodriguez D, Marco E, Annweiler C, Baztan A, Betancor É, et al. Unmet needs, health policies, and actions during the COVID-19 pandemic: a report from six European countries. Eur Geriatr Med. 2021;12:193–204.
Mor V, Gutman R, Yang X, White EM, McConeghy KW, Feifer RA, et al. Short-term impact of nursing home SARS-CoV-2 vaccinations on new infections, hospitalizations, and deaths. J Am Geriatr Soc. 2021;69(8):2063–9. https://doi.org/10.1111/jgs.17176.
Moraes ENd, Viana LdG, Resende LMH, Vasconcellos LdS, Moura AS, Menezes A, et al. COVID-19 in long-term care facilities for the elderly: laboratory screening and disease dissemination prevention strategies. Cien Saude Colet. 2020;25:3445–58.
Morris SC, Resnick AT, England SA, Stern SA, Mitchell SH. Lessons learned from COVID-19 outbreak in a skilled nursing facility, Washington State. J Am Coll Emerg Physicians Open. 2020;1(4):563–8.
Murti M, Goetz M, Saunders A, Sunil V, Guthrie JL, Eshaghi A, et al. Investigation of a severe SARS-CoV-2 outbreak in a long-term care home early in the pandemic. Can Med Assoc J. 2021;193(19):E681–8. https://doi.org/10.1503/cmaj.202485.
Obayashi K, Kodate N, Kondo H, Okamoto Y, Ishii Y, Nonoda T, et al. The COVID-19 pandemic and organizational resilience as unanticipated outcome of introducing socially assistive robots in nursing homes. Geriatr Gerontol Int. 2021;21(8):752–4. https://doi.org/10.1111/ggi.14222.
Ochi S, Murakami M, Hasegawa T, Komagata Y. Prevention and control of COVID-19 in imperfect condition: practical guidelines for nursing homes by Japan Environment and Health Safety Organization (JEHSO). Int J Environ Res Public Health. 2021;18(19):10188. https://doi.org/10.3390/ijerph181910188.
Ohta R, Ryu Y, Sano C. Effects of implementation of infection control measures against COVID-19 on the condition of Japanese rural nursing homes. Int J Environ Res Public Health. 2021;18(11):5805.
Piet E, Maillard A, Mallaval FO, Dusseau JY, Galas-Haddad M, Ducki S, et al. Outbreaks of covid-19 in nursing homes: a cross-sectional survey of 74 nursing homes in a French area. J Clin Med. 2021;10(18):4280. https://doi.org/10.3390/jcm10184280.
Poltavskiy E, Tabriz AA, Romano PS, Bang H, Kshirsagar AV. Predicting COVID-19 at skilled nursing facilities in California: do the stars align? BMJ Open Qual. 2021;10(1):e001099. https://doi.org/10.1136/bmjoq-2020-001099.
Powell T, Bellin E, Ehrlich AR. Older adults and Covid-19: the most vulnerable, the hardest hit. Hastings Cent Rep. 2020;50(3):61–3. https://doi.org/10.1002/hast.1136.
Pue K, Westlake D, Jansen A. Does the profit motive matter? COVID-19 prevention and management in Ontario long-term care homes. Can Public Policy. 2021;47(1):421–38. https://doi.org/10.3138/cpp.2020-151.
Rada AG. Covid-19: the precarious position of Spain’s nursing homes. BMJ. 2020;369:m1554. https://doi.org/10.1136/bmj.m1554.
Relias Media. OSHA issues alert on safety of nursing home workers. 2020.
Rios P, Radhakrishnan A, Williams C, Ramkissoon N, Pham B, Cormack GV, et al. Preventing the transmission of COVID-19 and other coronaviruses in older adults aged 60 years and above living in long-term care: a rapid review. BMC Syst Rev. 2020;9(1):1–8.
Shallcross L, Burke D, Abbott O, Donaldson A, Hallatt G, Hayward A, et al. Factors associated with SARS-CoV-2 infection and outbreaks in long-term care facilities in England: a national cross-sectional survey. Lancet Healthy Longevity. 2021;2(3):e129–42.
Shea Y-F, Lam HY, Yuen JKY, Adrian Cheng KC, Chan TC, Mok WYW, et al. Maintaining zero Coronavirus Disease 2019 infection among long-term care facility residents in Hong Kong. JAMDA. 2020;21(7):981–2. https://doi.org/10.1016/j.jamda.2020.05.042.
Shi M, Zhang F, He X, Huang S, Zhang M, Hu X. Are preventive measures adequate? An evaluation of the implementation of COVID-19 prevention and control measures in nursing homes in China. BMC Health Serv Res. 2021;21:641. https://doi.org/10.1186/s12913-021-06690-z.
Shih T-P, Wang J-H, Chao C-M. Infection control for COVID-19 in a nursing home in Taiwan. Int J Gerontol. 2020;14(4):349. https://doi.org/10.6890/IJGE.202011_14(4).0018.
Shimotsu ST, Johnson ARL, Berke EM, Griffin DO. COVID-19 infection control measures in long-term care facility, Pennsylvania, USA. Emerg Infect Dis. 2021;27(2):644–5. https://doi.org/10.3201/eid2702.204265.
Simoni-Wastila L, Wallem A, Fleming S, Le T, Kepczynska P, Yang J, et al. Staffing and protective equipment access mitigated COVID-19 penetration and spread in US nursing homes during the third surge. JAMDA. 2021;22(12):2504–10. https://doi.org/10.1016/j.jamda.2021.09.030.
Song R, Kim HS, Yoo SJ, Lee K, Park JH, Jang JH, et al. COVID-19 in nursing facilities: experience in Republic of Korea. Osong Public Health Res Perspect. 2020;11(4):164–9. https://doi.org/10.24171/j.phrp.2020.11.4.04.
Steiner C. How one long-term care facility held off COVID-19. Infection Control Today. 2021;25(3):22–4.
Stocker R, Russell S, Liddle J, Barker RO, Remmer A, Gray J, et al. Experiences of a National Early Warning Score (NEWS) intervention in care homes during the COVID-19 pandemic: a qualitative interview study. BMJ Open. 2021;11:e045469. https://doi.org/10.1136/bmjopen-2020-045469.
Sunner C, Giles M, Parker V, Kable A, Foureur M. COVID-19 preparedness in aged care: a qualitative study exploring residential aged care facility managers experiences planning for a pandemic. J Clin Nurs. 2021. https://doi.org/10.1111/jocn.15941.
Szczerbińska K. Could we have done better with COVID-19 in nursing homes? Eur Geriatr Med. 2020;11:639–43. https://doi.org/10.1007/s41999-020-00362-7.
Tan LF, Seetharaman S. Preventing the spread of COVID-19 to nursing homes: experience from a Singapore geriatric centre. J Am Geriatr Soc. 2020;68(5):942. https://doi.org/10.1111/jgs.16447.
Tan LF, Seetharaman SK. COVID-19 outbreak in nursing homes in Singapore. J Microbiol Immunol Infect. 2021;54(1):123–4. https://doi.org/10.1016/j.jmii.2020.04.018.
Viray P, Low Z, Sinnappu R, Harvey PA, Brown S. Residential aged care facility COVID-19 outbreaks and magnitude of spread among residents: observations from a Victorian residential in-reach service. Intern Med J. 2021;51(1):99–101. https://doi.org/10.1111/imj.15143.
Vital COVID lessons ignored. The Lamp: The Magazine of the NSW Nurses and Midwives’ Association. 2020;77(5):12–4.
Vogazianos P, Argyropoulos CD, Haralambous C, Mikellidou CV, Boustras G, Andreou M, et al. Impact assessment of COVID-19 non-pharmaceutical interventions in long term care facilities in Cyprus: safety improvement strategy. Saf Sci. 2021;143:105415. https://doi.org/10.1016/j.ssci.2021.105415.
Wagner EH. The vulnerability of nursing home residents to the Covid-19 pandemic. Int J Care Coord. 2020;23(2–3):57–60. https://doi.org/10.1177/2053434520958860.
Wang L, Qi N, Zhou Y, Zhang H. Prevention and infection control of COVID-19 in nursing homes: experience from China. Age Ageing. 2020;49(6):894–5. https://doi.org/10.1093/ageing/afaa148.
Wang Z. Use the environment to prevent and control COVID-19 in senior-living facilities: an analysis of the guidelines used in China. HERD. 2021;14(1):130–40. https://doi.org/10.1177/1937586720953519.
Watts T, Tucker M, Gray C, Lee K, Modina K, Gray Z. Lessons learned in preventing COVID-19 within a skilled nursing facility during the early pandemic. Geriatr Nurs. 2021;42(6):1388–96. https://doi.org/10.1016/j.gerinurse.2021.09.005.
Yang X-F, Li M-Q, Liao L-L, Feng H, Zhao S, Wu S, et al. A qualitative study of the first batch of medical assistance team’s first-hand experience in supporting the nursing homes in Wuhan against COVID-19. PLoS One. 2021;16(4):e0249656. https://doi.org/10.1371/journal.pone.0249656.
Yau B, Vijh R, Prairie J, McKee G, Schwandt M. Lived experiences of frontline workers and leaders during COVID-19 outbreaks in long-term care: a qualitative study. Am J Infect Control. 2021;49(8):978–84. https://doi.org/10.1016/j.ajic.2021.03.006.
Zheng A, Govindasamy LS, Thomas J, Branley J, Craig AT, Douglas M. Lessons from a successful public health response to COVID-19 in a New South Wales residential aged care facility, 2020. Aust N Z J Public Health. 2021;45(1):13–6. https://doi.org/10.1111/1753-6405.13077.
OECD. Workforce and safety in long-term care during the COVID-19 pandemic. 2020.
Tremblay S, Castiglione S, Audet L-A, Desmarais M, Horace M, Peláez S. Conducting qualitative research to respond to COVID-19 challenges: reflections for the present and beyond. Int J Qual Methods. 2021;20:16094069211009680.
Demakakos P. Importance of population-based longitudinal studies to understanding the impact of COVID-19. J Epidemiol Community Health. 2021;75:815–6.
Bethel C, Reed PG, Brewer BB, Rainbow JG. Selecting a theoretical framework to guide research on the COVID-19 pandemic impacts on nursing care delivery and the critical care work system (using Reed’s Intermodern approach to theory critique). Appl Nurs Res. 2022;63:151513.
Ickert C, Stefaniuk R, Leask J. Experiences of long-term care and supportive living residents and families during the COVID-19 pandemic: “It’s a lot different for us than it is for the average Joe.” Geriatr Nurs. 2021;42(6):1547–55.
Smith CB, Wong KLY, To-Miles F, Dunn S, Gregorio M, Wong L, et al. Exploring experiences of loneliness among Canadian long-term care residents during the COVID-19 pandemic: a qualitative study. Int J Older People Nurs. 2023;18(1):e12509.
McGrail K. Excess mortality, COVID-19 and health care systems in Canada. Can Med Assoc J. 2022;194(21):E741–5.
Alami H, Lehoux P, Fleet R, Fortin J-P, Liu J, Attieh R, et al. How can health systems better prepare for the next pandemic? Lessons learned from the management of COVID-19 in Quebec (Canada). Front Public Health. 2021;9:671833.
Vernon N, Myers J. Acknowledging and learning from different types of failure. Environ Health Insights. 2021;15:11786302211018096.
McArthur C, Saari M, Heckman GA, Wellens N, Weir J, Hebert P, et al. Evaluating the effect of COVID-19 pandemic lockdown on long-term care residents’ mental health: a data-driven approach in New Brunswick. JAMDA. 2021;22(1):187–92. https://doi.org/10.1016/j.jamda.2020.10.028.
Simard J, Volicer L. Loneliness and isolation in long-term care and the COVID-19 pandemic. JAMDA. 2020;21(7):966–7. https://doi.org/10.1016/j.jamda.2020.05.006.
Van der Roest HG, Prins M, van der Velden C, Steinmetz S, Stolte E, van Tilburg TG, et al. The impact of COVID-19 measures on well-being of older long-term care facility residents in the Netherlands. JAMDA. 2020;21(11):1569–70. https://doi.org/10.1016/j.jamda.2020.09.007.
Acknowledgements
The authors would like to thank the Université du Québec en Outaouais for funding this research.
Patient and public involvement
This scoping review did not involve any patient or public involvement.
Funding
This study was funded by an internal post-doctoral fellow scholarship from the Université du Québec en Outaouais, Québec, Canada.
Author information
Authors and Affiliations
Contributions
ENT, KK, JL, EB, SR, MJ, FEM, SS, IB, and DS were all involved in the conception, drafting, and revision of this manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable, as ethical approval for this review was not required since it utilized data that had been previously published.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tchouaket, E.N., Kruglova, K., Létourneau, J. et al. Factors influencing long-term care facility performance during the COVID-19 pandemic: a scoping review. BMC Health Serv Res 24, 901 (2024). https://doi.org/10.1186/s12913-024-11331-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-024-11331-2