
Abstract
Background
Compelling evidence supports the association between red and processed meat consumption and increased risk of colorectal cancer. Herein, we estimated the current (2018) and future (2030) federal direct healthcare costs of colorectal cancer in the Brazilian Unified Health System attributable to red and processed meat consumption. Considering reduced red and processed meat consumption, we also projected attributable costs of colorectal cancer in 2040.
Methods
We retrieved information on red and processed meat consumption from two nationally representative dietary surveys, the Household Budget Survey 2008–2009 and 2017–2018; relative risks for colorectal cancer from a meta-analysis; direct healthcare costs of inpatient and outpatient procedures in adults ≥ 30 years with colorectal cancer (C18-C20) from 2008–2019 by sex.
Results
Attributable costs of colorectal cancer were calculated via comparative risk assessment, assuming a 10-year lag. In 2018, US$ 20.6 million (8.4%) of direct healthcare costs of colorectal cancer were attributable to red and processed meat consumption. In 2030, attributable costs will increase to US$ 86.6 million (19.3%). Counterfactual scenarios of reducing red and processed meat consumption in 2030 suggested that US$ 2.2 to 11.9 million and US$ 13 to 74 million could be saved in 2040, respectively.
Conclusion
Red and processed meat consumption has an escalating economic impact on the Brazilian Unified Health System. Our findings support interventions and policies focused on primary prevention and cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Colorectal cancer is the third most common cancer for both men and women in Brazil, with an estimated 40,990 newly diagnosed cases in 2021, approximately 10% of all cancers (excluding non-melanoma skin cancer) [1]. By 2040, colorectal cancer is expected to increase by over 74% due to demographic changes (population growth and aging) [2]. The projected burden of colorectal cancer suggests an escalating economic impact on the treatment and care costs the Brazilian Health System will have to cope with.
The Brazilian Health System has a coexistence of public, private, and army systems. The Brazilian Unified Health System (Sistema Único de Saúde Brasileiro – SUS) is the most extensive public health system in the world benefiting approximately 200 million inhabitants. Over 70% of Brazilians rely exclusively on SUS [3]. The SUS Outpatient Information System (SIA/SUS) and the Inpatient Information System (SIH/SUS) are nationwide sources of direct healthcare costs and provide publicly available and deidentified inpatient and outpatient care data. In 2018, the federal government spent approximately US$1.7 billion on direct healthcare costs of cancer in Brazil, of which 15% (US$269 million out of US$1.7 billion) were due to colorectal cancer [4].
Primary cancer prevention is pivotal in cancer control, particularly considering the limited access to affordable and effective preventive screening and cancer treatment in low- and middle-income countries. In principle, colorectal cancer is one of the most preventable common cancers. In Brazil, approximately half of colorectal cancer cases and deaths could be prevented or postponed through primary prevention strategies focused on lifestyle risk factors, including diet and nutrition [5].
The International Agency for Research on Cancer (IARC) [6] and the World Cancer Research Fund, and the American Institute for Cancer Research (WCRF/AICR) [7] consider the evidence that processed meat consumption increases the risk of colorectal cancer as sufficient/convincing. This classification is based on consistent evidence showing that consumption of processed meat increases the risk of colorectal (increased risk per 50 g increase in consumption per day) and robust evidence for mechanisms operating in human [7]. Red meat consumption has been classified as probably carcinogenic to humans [6, 7]. WCRF/AICR [7] and the Brazilian National Cancer Institute (INCA) [8] recommend limiting red meat consumption to no more than three portions per week (< 500 g/week). For processed meat, the recommendation is to eat very little, if any. Despite these recommendations, per capita meat consumption has increased [9,10,11]. The average global consumption of all meats in 2010 was 122 g/day, with high-income and Latin American countries, including Brazil, eating the most [12]. Quantifying the current and future economic burden of colorectal cancer attributable to red and processed meat consumption in Brazil may help inform potential policy and prevention initiatives.
In this study, we estimated the current (2018) and future (2030) federal direct healthcare costs of colorectal cancer in the SUS attributable to red and processed meat consumption. In addition, we estimated potential savings in federal direct healthcare costs of colorectal cancer in 2040 by considering different counterfactual scenarios of reduction in red and processed meat consumption to be achieved in 2030.
Methods
Data and study design
This study applied a top-down costing approach and performed a macrosimulation model to estimate the future costs of colorectal cancer attributable to red and processed meat consumption, using the Brazilian population as a case study. We used the following data: 1. Relative risks (RR) from WCRF/AICR meta-analyses [13]; 2. Prevalence data (%) of red and processed meat consumption in adults aged 20 years or older who relied exclusively on the public health system from representative national surveys; 3. Nationwide registries of federal direct healthcare costs of inpatient and outpatient procedures in the SUS in adults aged 30 years or older with cancer. The parameters used in the model are available in Supplementary Material A.
We estimated the potential impact of red and processed meat on federal direct healthcare costs of cancer, assuming a 10-year time lag between exposure and outcome via comparative risk assessment. We used the potential impact fraction (PIF) equation and the Monte Carlo simulation method to estimate the attributable costs and their 95% uncertainty intervals, considering the theoretical-minimum-risk exposure and other counterfactual (alternative) red and processed meat consumption scenarios. We assessed cancer costs attributable to red and processed meat, multiplying PIF by the direct healthcare costs of cancer.
Relative risk estimates and cancer sites
We considered in our study only colorectal cancer as there is strong evidence of association (convincing or probable) with red and processed meat according to the WCRF/AICR [7]. The WCRF/AICR method of grading evidence has been designed to operationalize the criteria identified by Bradford Hill as contributing to an inference of causation from observational data. Strong evidence of association sustains a judgment of a convincing causal (or protective) relationship that justifies making recommendations designed to reduce cancer risk. This evidence is robust enough to be unlikely to be altered in the foreseeable future as new evidence accumulates [7]. We detailed the list of the 10th Revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes in Supplementary Material B.
We obtained the \({RR}_{x}\) for colorectal cancer incidence by sex from the WCRF/AICR dose–response meta-analysis [13], considering the increment of \(x\) g/day of red and processed meat (\(x\)=100 and 50, respectively). It is important to enphazise that this meta-analysis [13] represents the last update from WCRF concerning the evidence from observational studies (cohort, nested case–control and case-cohort designs) on the association between foods, nutrients, physical activity, body adiposity and the risk of colorectal cancer in men and women. The WCRF/AICR dose–response meta-analysis is part of the CUP (Continuous Update Project), a global network of researchers that evaluates cancer prevention research.
We converted these measures per increment of 1 g /day of the exposure (\({RR}_{1}\)) using the following equation [14]:
To obtain the RR for each exposition category (RRc) (Supplementary Material C), we used the following equation [15]:
where Mc represents the median value in each category, and ref represents the reference category value (< 70 g/day for red meat and 0 g for processed meat). The reference category reflected the theoretical minimum risk exposure level [7] and the Brazilian INCA recommendations [8].
Assessment of red and processed meat consumption prevalence
We obtained an estimated prevalence of red and processed meat consumption in the adult population aged ≥ 20 years from the National Household Budget Survey (Pesquisa de Orçamentos Familiares – POF), a cross-sectional nationally representative survey conducted in Brazil in 2008–2009 [16] and 2017–2018 [17]. We considered only adults aged 20 years or older who reported not having health insurance to obtain the prevalence and 95% confidence interval for each red and processed meat consumption by sex.
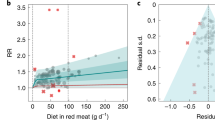
POF collected two 24-h real-time food records from 34,003 participants in 2008–2009 [16] and 37,690 participants in 2017–2018 [17]. Using a food portion table, we converted reported food amounts into grams [18]. We estimated red meat consumption (g/day) based on the consumption of all types of meat from mammals, such as beef, horse, goat, lamb, mutton, and pork, whereas processed meat (g/day) on the consumption of meat preserved by smoking, curing, salting, the addition of chemical preservatives (e.g., bacon, chorizo, corned beef, ham, pastrami, salami, and sausages). We displayed categories of red and processed meat consumption in grams/day in Figs. 1 and 2, respectively. The reference category (< 70 g/day of red meat and 0 g/day of processed meat) aimed to reflect the theoretical minimum risk exposure level [7] as well as the recommendations of the Brazilian INCA [8].

Red meat consumption distribution in 2008–2009 and 2017–2018 and levels fixed in counterfactual (alternative) scenarios to be achieved in 2030

Processed meat consumption distribution in 2008–2009 and 2017–2018 and levels fixed in counterfactual (alternative) scenarios to be achieved in 2030
The POF microdata is available in the public domain via the Brazilian Institute of Geography and Statistics (IBGE) at http://www.ibge.gov.br (Supplementary Material D). We incorporated the complex sample design into all estimates using RStudio version 1.4.1103.
Counterfactual (alternative) scenarios for red and processed meat consumption
We proposed four counterfactual (alternative) scenarios of population-wide reduction in red and processed meat consumption (observed in 2017–2018) to be achieved in Brazil in 2030 to save direct healthcare costs with cancer in 2040 (Figs. 1 and 2). The counterfactual scenarios considered reduction in one serving per week (Scenario 1: -120 g/week of red meat and -50 g/week of processed meat) and shifting red and processed meat categories, which considered a scenario where everyone consumes: for red meat: Scenario 2) < 140 g/day; Scenario 3) < 210 g/day; Scenario 4) < 280 g/day; for processed meat: Scenario 2) < 50 g/day; Scenario 3) < 100 g/day; Scenario 4) < 150 g/day.
Federal direct healthcare costs of cancer in the Brazilian SUS in 2030 and 2040
We retrieved registries of federal direct healthcare costs of inpatient and outpatient cancer-related procedures between 2008 and 2019 from the SIH/SUS and SIA/SUS (Supplementary Material D). We used the 10th Revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes for recovering cancer procedures from information systems (Supplementary Material B). We stratified the direct healthcare costs by sex. Assuming a 10-year time lag between exposure and outcome, we considered the procedures approved for payment in adults with cancer aged 30 years or older in 2030 and 2040.
We performed a simple linear regression to predict the future costs of cancer (dependent variable) as a function of time (independent variable) up to 2030 and 2040 based on the values practiced over time between 2008 and 2019. Controlling for potential confounders while examining the possible determinants of cost is crucial. Once our outcome was the direct healthcare costs over time, it was unnecessary to control for confounders because we observed their effect in the observed costs used to fit the regression model [19]. We transformed the monetary values in Brazilian Real (R$) to United States Dollar (US$), considering the purchasing power parity (PPP) of 2018 (conversion factor 2.226) to current costs and of 2019 (conversion factor 2.281) to future costs [20].
Cancer costs attributable to red and processed meat consumption
Based on the abovementioned intermediate inputs of the models, we calculated the (PIF) for colorectal cancer by sex and counterfactual (alternative) scenario using the following equation [21]:
where \({P}_{i}\) is the proportion of the population at the level \(i\) of red and processed meat consumption in a given year, \({P{\prime}}_{i}\) is the proportion of the population at the level \(i\) of red and processed meat consumption in a given counterfactual (alternative) scenario, and \({RR}_{i}\) is the RR of colorectal cancer at the level \(i\) of red and processed meat consumption. We displayed the levels \(i\) for red and processed meat consumption in Figs. 1 and 2. Of note, the PIF equals the Population Attributable Fraction (PAF) when the counterfactual (alternative) scenario represents the theoretical minimum risk exposure level [21, 22].
To estimate the fraction of colorectal cancer costs attributable to combined red and processed meat consumption, we used the joint PIF/PAF equation [23], which assumes the absence of interaction between risk factors:
To assess the cancer costs attributable to red and processed meat, we multiplied PIF by the total colorectal cancer costs. We considered the prevalence in 2008–2009 and 2017–2018 and the costs of cancer in 2018 and 2030, respectively, assuming at least a 10-year time lag between exposure and outcome (i.e., based on the average follow-up time of prospective cohort studies [13]). Finally, we calculated the potential savings in cancer costs in 2040 if reduced red and processed meat consumption occurred in Brazil to levels fixed in the counterfactual (alternative) scenarios in 2030.
We quantified the uncertainty in all modeled estimates using the Monte Carlo simulation approach [24, 25] with 10,000 iterations. The simulation works thoroughly, producing a draw from the distributions of a) baseline prevalence per red and processed meat consumption category considering a binomial distribution; b) the log of the RR per exposure category for the association of red and processed meat consumption with colorectal cancer risk assuming a normal distribution. We calculated PIF by sex for the 50th, 2.5th, and 97.5th percentiles as the central estimate and 95% uncertainty intervals across all simulations. Negative values of PIF derived from the Monte Carlo simulation were rounded to 0, assuming that reducing red and processed meat consumption values may not increase the risk of cancer and, consequently, the attributable costs. We used R Studio version 1.3.1093 for analysis.
Results
Consumption of red and processed meat in Brazil in 2008–2009 and 2017–2018
Comparing 2008–2009 and 2017–2018, the prevalence of ≥ 70 g/day of red meat consumption (i.e., above the Brazilian INCA recommendations) decreased from 47.2% to 32.5% in men and 34.4% to 22.6% in women. We observed changes in other categories of higher consumption of red meat. For instance, the prevalence of ≥ 280 g/day of red meat consumption changed from 4.3% to 3.8% in men and 1.3% to 1.7% in women (Fig. 1). On the other hand, between 2008–2009 and 2017–2018, processed meat consumption in Brazil increased from 33.7% to 64.4% in men and 30.6% to 60.4% in women. The prevalence of ≥ 150 g/day of processed meat increased from 2.8% to 15.4% in men and 1.6% to 8.1% in women in the same period (Fig. 2).
Federal direct healthcare costs of colorectal cancer in Brazil in 2018 attributable to the consumption of red and processed meat in 2008–2009
In 2018, federal direct healthcare costs of colorectal cancer were approximately US$ 245 million. Colorectal cancer costs were higher in men (US$ 124 million) than in women (US$ 121 million). We estimated that 3.5% or US$ 8.5 million direct healthcare costs of colorectal cancer were attributable to red meat consumption and 5.1% or US$ 12.6 million to processed meat consumption. The combined fraction of direct healthcare costs of colorectal cancers attributable to combined red and processed meat consumption was 8.4%, corresponding to US$ 20.6 million in 2018 (Table 1).
Projected federal direct healthcare costs of colorectal cancer in Brazil in 2030 attributable to red and processed meat consumption in 2017–2018
In 2030, we projected approximately US$ 450 million in direct healthcare costs for colorectal cancer in Brazil. We estimated that 2.5% or US$ 11.4 million in direct healthcare costs of colorectal cancer would be attributable to red meat consumption and 17.2% or US$ 77.3 million to processed meat consumption. The combined fraction of direct healthcare costs of colorectal cancers attributable to red and processed meat consumption will be 19.3%, corresponding to US$ 86.6 million in 2030 (Table 1).
The potential impact of the reduction in the consumption of red and processed meat on projected direct healthcare costs of colorectal cancer in Brazil in 2040
We displayed in Figs. 1 and 2 the potential reductions (counterfactual scenarios) in Brazil’s red and processed meat consumption to be achieved in 2030. We estimated that approximately US$ 2.2 to 11.9 million in 2040 could be saved by reducing red meat consumption in 2030. Reducing processed meat consumption to levels fixed in the counterfactual scenarios in 2030 could save US$ 13.7 to 74.4 million in 2040 (Table 2).
Discussion
Our study quantified that red and processed meat consumption in 2008–2009 was responsible for US$ 20.6 million in direct healthcare costs of colorectal cancer in the SUS in 2018. Considering the changes in meat consumption from 2008–2009 to 2017–2018, and the projected growing economic burden of colorectal cancer in Brazil, we estimated that red and processed meat consumption will be responsible for US$ 86.6 million in 2030. Reduced processed meat consumption to levels fixed in the counterfactual scenarios in 2030 could save US$13.7 to 74.4 million in direct healthcare costs of colorectal cancer in 2040.
Meat consumption has some adverse effects on human health [9]. Epidemiological studies have consistently reported that meat consumption increases the risk of noncommunicable diseases, such as cardiovascular diseases, diabetes, and cancer [6, 7, 26, 27]. The most robust evidence is for the harmful effect of processed meat consumption on colorectal cancer risk [6, 7]. IARC and WCRF have classified processed meat as carcinogenic to humans, whereas red meat is probably carcinogenic to humans [6, 7]. Globally, diets high in processed meats are responsible for 34 thousand cancer deaths per year, whereas diets high in red meat are responsible for 50 thousand cancer deaths per year [28]. In Brazil, red meat was responsible for 1,900 cancer cases and 1,000 cancer deaths, and processed meat for 1,700 cancer cases and 1,000 cancer deaths in 2012 [5].
Few comparative risk assessment studies have modeled the potential impact of constraining red and processed meat on health and economic outcomes, particularly on the financial burden of cancer [5, 29,30,31]. Our study showed that meat consumption also had escalated economic impact on the SUS over the years. In Canada, $CAN 168 million in direct ($CAN 29 million) and indirect ($CAN 139 million) costs with colorectal cancers were attributable to red meat consumption in 2014. For processed meat, these values were $CAN 202 million in direct ($CAN 34 million) and indirect ($CAN 167 million) costs of colorectal cancer in the same year [29]. In the US, the cost-effectiveness of implementing nutritional policies on processed meat consumption on the burden of cancer has been recently evaluated. The model showed that excise tax and warning labels would avert 77,000 to 85,400 cases of colorectal cancer, with net savings of $2.7 billion to $4.5 billion from a societal perspective, including $1.3 billion in healthcare costs saved [30]. These studies suggest that nutritional policies may be a cost-saving strategy that substantially benefits health and the economy. Our results showed that policies aimed at reducing processed meat consumption may significantly impact colorectal cancer costs. For instance, our projected costs saved in 2040 were 5–sevenfold higher for reducing processed meat than red meat consumption.
Changing population diets, especially foods considered “natural, normal, necessary or nice” [9, 32], is challenging. For instance, a systematic review of health-related values and preferences regarding meat consumption found that omnivores consume meat because they consider it an essential component of a healthy diet, like food, feel that meat is part of their traditions, and believe they have not the culinary knowledge and skills to prepare a proper meatless meal [33]. In addition, there is insufficient evidence of the effectiveness of interventions to reduce meat consumption [9]. The diversity of factors that influence the price and availability of meat and how it is processed and marketed determines a socioeconomic scenario that profoundly affects and is affected by norms and behavior. Changing dietary behaviors in response to interventions takes a lot of work. Still, social norms can and must change, and the coordinated efforts of civil society, health organizations, and government can aid this process. Governmental interventions could transform food systems through economic, political, and legal actions. Decreasing the production and consumption of meat and, consequently, its adverse environmental, health, social, and economic effects, as shown in our study, would be aligned with the 2030 United Nations Agenda for Sustainable Development Goals and the World Health Organization targets to reduce premature mortality from noncommunicable diseases [34]. However, the World Trade Organization rules may limit state-sponsored interventions in food systems. Recently, there has been a discussion about other interventions targeting unconscious/automatic behavioral choices for meat (e.g., choice architecture, environmental restructuring, and marketing and advertising) [9], but the effectiveness and ethics of these actions aimed at manipulating population behaviors are concerned [35]. Among the interventions proposed to reduce the consumption of red and processed meat is taxation, which has been used, e.g., as an effective tool to reduce the consumption of sugar-sweetened beverages. Efforts to raise consumer awareness of meat’s adverse health and environmental impacts, like warning labels, can also change behavior, redirecting meat subsidies to more sustainable and nutritious crops such as fruits and vegetables. Finally, national dietary guidelines can also play an essential role in decreasing red and processed meat consumption [36].
To our knowledge, this is the first study to quantify the direct costs of colorectal cancer treatment attributable to combined red and processed meat consumption. We used two nationally representative dietary survey data from over 60 thousand Brazilian adults, RR from meta-analysis, and 5.7 million nationwide registries of the SUS direct-healthcare costs of colorectal cancers. However, our study has some limitations. To estimate the PIF/PAF for Brazil, we used information on red and processed meat consumption from two 24-h real-time food records. However, we did not consider food preparations in 2008–2009 and 2017–2018, which could lead to an underestimation of meat consumption. We assumed the portability of the pooled RR from meta-analysis, which did not include Brazilian cohort studies. However, we incorporated the uncertainty of these estimates in the models via the Monte Carlo simulation approach. We also assumed at least a 10-year time lag between exposure and outcome based on the average follow-up time of prospective cohort studies [13]. We further recognize that non-linear changes concerning the cost of colorectal cancer treatment may occur. During data analysis, we tested multiple regression models by including predictor variables: time, aging, cancer incidence, cancer mortality, technological incorporation, and judicialization of health care. However, the multiple regression did not fit better than simple linear regression, and we opted for parsimony. Future modeling approaches using proportional multistate lifetable modeling of preventive interventions may be helpful to incorporate a time dimension more appropriately [37]. Our model did not account for recurring events or include the interaction between exposures and substitutions of meats from other food options.
Conclusions
Red and processed meat consumption has an escalating economic impact on the SUS. We found that 8.4% or US$ 20.6 million in direct healthcare costs of colorectal cancer in 2018 were attributable to red and processed meat consumption. In 2030, the direct healthcare costs of colorectal cancer will increase to 19.3% or US$ 86.6 million. We estimated that reducing red meat consumption could save approximately US$ 2.2 to 11.9 million in 2040. Decreasing processed meat to levels fixed in the counterfactual scenarios in 2030 could save US$ 13.7 to 74.4 million in 2040. Our findings may help support policies to reduce meat consumption and cancer prevention strategies in Brazil. Considering the limited and finite resources available to health systems, it is urgent to prioritize primary prevention actions, especially in the context of exponential cancer treatment costs.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Abbreviations
- AICR:
-
American Institute for Cancer Research
- CUP:
-
Continuous Update Project
- CLUA:
-
Climate and Land Use Alliance
- IBGE:
-
Instituto Brasileiro de Geografia e Estatística - Brazilian Institute of Geography and Statistics
- IARC:
-
International Agency for Research on Cancer
- ICD-10:
-
10th Revision of the International Statistical Classification of Diseases and Related Health Problems
- INCA:
-
Brazilian National Cancer Institute
- POF:
-
Pesquisa de Orçamentos Familiares - National Household Budget Survey
- PAF:
-
Population Attributable Fraction
- PIF:
-
Potential impact fraction
- PPP:
-
Purchasing power parity
- RR:
-
Relative risks
- SUS:
-
Sistema Único de Saúde Brasileiro - Brazilian Unified Health System
- SIH:
-
Sistema de Informações Hospitalares do Sistema Único de Saúde Brasileiro - Inpatient Information System of the Brazilian Unified Health System
- SIA:
-
Sistema de Informações Ambulatoriais do Sistema Único de Saúde Brasileiro - Outpatient Information System of the Brazilian Unified Health System
- WCRF:
-
World Cancer Research Fund
References
Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F. Global Cancer Observatory: Cancer Today. International Agency for Research on Cancer. 2020. https://gco.iarc.fr/today. Accessed 22 Sept 2021.
Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2020: incidência de câncer no Brasil. Instituto Nacional de Câncer José Alencar Gomes da Silva. 2019. https://www.inca.gov.br/estimativa. Accessed 15 Sept 2021.
Souza Júnior PRB, Szwarcwald CL, Damacena GN, Stopa SR, Vieira MLFP, Almeida WDS, Oliveira MM, Sardinha LMV, Macário EM. Health insurance coverage in Brazil: analyzing data from the National Health Survey, 2013 and 2019. Cien Saude Colet. 2021;26:2529–41. https://doi.org/10.1590/1413-81232021266.1.43532020.
Ferreira Corrêa, da Silva R, Bahia LR, Machado da Rosa MQ, Malhão TA, Mendonça EP, Rosa RDS, Araújo DV, Maya Moreira LG, Schilithz AOC, Diogenes Melo MEL. Costs of cancer attributable to excess body weight in the Brazilian public health system in 2018. PLoS One. 2021;16:e0247983. https://doi.org/10.1371/journal.pone.0247983.
Rezende LFM, Lee DH, Louzada MLDC, Song M, Giovannucci E, Eluf-Neto J. Proportion of cancer cases and deaths attributable to lifestyle risk factors in Brazil. Cancer Epidemiol. 2019;59:148–57. https://doi.org/10.1016/j.canep.2019.01.021.
Bouvard V, Loomis D, Guyton KZ, Grosse Y, Ghissassi FE, Benbrahim-Tallaa L, Guha N, Mattock H, Straif K, International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015;16:1599–600. https://doi.org/10.1016/S1470-2045(15)00444-1.
World Cancer Research Fund/ American Institute for Cancer Research. Meat, fish, dairy products, and the risk of cancer. Continuous Update Project Expert Report 2018. 2018. https://www.wcrf.org/wp-content/uploads/2021/02/Meat-fish-and-dairy-products.pdf. Accessed 15 Jan 2021.
Instituto Nacional de Câncer José Alencar Gomes da Silva. Dieta, nutrição, atividade física e câncer: uma perspectiva global: um resumo do terceiro relatório de especialistas com uma perspectiva brasileira. Instituto Nacional de Câncer José Alencar Gomes da Silva. 2020. https://www.inca.gov.br/sites/ufu.sti.inca.local/files//media/document//dieta_nutricao_atividade_fisica_e_cancer_resumo_do_terceiro_relatorio_de_especialistas_com_uma_perspectiva_brasileira.pdf. Accessed 15 Jan 2021.
Godfray HCJ, Aveyard P, Garnett T, Hall JW, Key TJ, Lorimer J, Pierrehumbert RT, Scarborough P, Springmann M, Jebb SA. Meat consumption, health, and the environment. Science. 2018;361:eaam5324. https://doi.org/10.1126/science.aam5324.
Ritchie H, Roser M. Meat and Dairy Production. Our World in Data. 2017. https://ourworldindata.org/meat-production#note-1. Accessed 29 Sept 2021.
Organization for Economic Cooperation and Development/ Food and Agriculture Organization of the United Nations. OECD‑FAO Agricultural Outlook 2018‑2027. Organization for Economic Cooperation and Development. 2018. https://www.agri-outlook.org/commodities/Agricultural-Outlook-2018-Meat.pdf. Accessed 28 Sept 2021.
Micha R, Khatibzadeh S, Shi P, Andrews KG, Engell RE, Mozaffarian D, Global Burden of Diseases Nutrition and Chronic Diseases Expert Group. Global, regional and national consumption of major food groups in 1990 and 2010: a systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open. 2015;5:e008705. https://doi.org/10.1136/bmjopen-2015-008705.
World Cancer Research Fund International. Systematic Literature Review. The Associations between Food, Nutrition and Physical Activity and the Risk of Colorectal Cancer. 2017. https://www.wcrf.org/wp-content/uploads/2021/02/colorectal-cancer-slr.pdf. Accessed 15 Jan 2021.
Islami F, Goding Sauer A, Miller KD, Siegel RL, Fedewa SA, Jacobs EJ, McCullough ML, Patel AV, Ma J, Soerjomataram I, Flanders WD, Brawley OW, Gapstur SM, Jemal A. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018;68:31–54. https://doi.org/10.3322/caac.21440.
Brenner DR, Poirier AE, Ruan Y, Hebert LA, Grevers X, Walter SD, Villeneuve PJ, Friedenreich CM, ComPARe Study Team. Estimates of the current and future burden of cancer attributable to excess body weight and abdominal adiposity in Canada. Prev Med. 2019;122:49–64. https://doi.org/10.1016/j.ypmed.2019.03.014.
Instituto Brasileiro de Geografia e Estatística. Pesquisa de orçamentos familiares 2008–2009: Análise do consumo alimentar pessoal no Brasil. Instituto Brasileiro de Geografia e Estatística. 2011. https://biblioteca.ibge.gov.br/visualizacao/livros/liv50063.pdf. Accessed 15 Jan 2021.
Instituto Brasileiro de Geografia e Estatística. Pesquisa de orçamentos familiares 2017–2018: primeiros resultados. Instituto Brasileiro de Geografia e Estatística. 2019. https://biblioteca.ibge.gov.br/visualizacao/livros/liv101670.pdf. Accessed 15 Jan 2021.
Universidade de São Paulo. Tabela de Composição de Alimentos. Food Research Center. 2020. http://www.fcf.usp.br/tbca. Accessed 15 Mar 2021.
Ward ZJ, Bleich SN, Cradock AL, Barrett JL, Giles CM, Flax C, Long MW, Gortmaker SL. Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity. N Engl J Med. 2019;381:2440–50. https://doi.org/10.1056/NEJMsa1909301.
Organization for Economic Cooperation and Development. Purchasing power parities (PPP) (indicator). Total, National currency units/US dollar, 2000–2019. 2021. https://data.oecd.org/conversion/purchasing-power-parities-ppp.htm. Accessed 15 Out 2021.
Murray CJL, Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S. Comparative quantification of health risks: conceptual framework and methodological issues. World Health Organization. 2004. https://apps.who.int/iris/bitstream/handle/10665/42792/9241580348_eng_Volume1.pdf;jsessionid=0F625E412E1125E1D804A57F6894CFA1?sequence=1. Accessed 15 Jan 2021.
Rezende LF, Eluf-Neto J. Population attributable fraction: planning of disease prevention actions in Brazil. Rev Saude Publica. 2016;50:30. https://doi.org/10.1590/S1518-8787.2016050006269.
Ezzati M, Hoorn SV, Rodgers A, Lopez AD, Mathers CD, Murray CJ, Comparative Risk Assessment Collaborating Group. Estimates of global and regional potential health gains from reducing multiple major risk factors. Lancet (London, England). 2003;362:271–80. https://doi.org/10.1016/s0140-6736(03)13968-2.
Steenland K, Greenland S. Monte Carlo sensitivity analysis and Bayesian analysis of smoking as an unmeasured confounder in a study of silica and lung cancer. Am J Epidemiol. 2004;160:384–92. https://doi.org/10.1093/aje/kwh211.
Greenland S. Interval estimation by simulation as an alternative to and extension of confidence intervals. Int J Epidemiol. 2004;33:1389–97. https://doi.org/10.1093/ije/dyh276.
Micha R, Wallace SK, Mozaffarian D. Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: a systematic review and meta-analysis. Circulation. 2010;121:2271–83. https://doi.org/10.1161/CIRCULATIONAHA.109.924977.
Abete I, Romaguera D, Vieira AR, Lopez de Munain A, Norat T. Association between total, processed, red and white meat consumption and all-cause, CVD and IHD mortality: a meta-analysis of cohort studies. Br J Nutr. 2014;112:762–75. https://doi.org/10.1017/S000711451400124X.
International Agency for Research on Cancer. Q&A on the carcinogenicity of the consumption of red meat and processed meat. World Health Organization. 2015. https://www.iarc.who.int/wp-content/uploads/2018/11/Monographs-QA_Vol114.pdf. Accessed 15 Jan 2021.
Lieffers JRL, Ekwaru JP, Ohinmaa A, Veugelers PJ. The economic burden of not meeting food recommendations in Canada: The cost of doing nothing. PLoS One. 2018;13:e0196333. https://doi.org/10.1371/journal.pone.0196333.
Kim DD, Wilde PE, Michaud DS, Liu J, Lizewski L, Onopa J, Mozaffarian D, Zhang FF, Wong JB. Cost Effectiveness of Nutrition Policies on Processed Meat: Implications for Cancer Burden in the U.S. Am J Prev Med. 2019;57:e143–52. https://doi.org/10.1016/j.amepre.2019.02.023.
Ruan Y, Poirier AE, Hebert LA, Grevers X, Walter SD, Villeneuve PJ, Brenner DR, Friedenreich CM, ComPARe Study Team. Estimates of the current and future burden of cancer attributable to red and processed meat consumption in Canada. Preventive medicine. 2019;122:31–9. https://doi.org/10.1016/j.ypmed.2019.03.011.
Piazza J, Ruby MB, Loughnan S, Luong M, Kulik J, Watkins HM, Seigerman M. Rationalizing meat consumption. The 4Ns. Appetite. 2015;91:114–28. https://doi.org/10.1016/j.appet.2015.04.011.
Valli C, Rabassa M, Johnston BC, Kuijpers R, Prokop-Dorner A, Zajac J, Storman D, Storman M, Bala MM, Solà I, Zeraatkar D, Han MA, Vernooij RWM, Guyatt GH, Alonso-Coello P, NutriRECS Working Group. Health-Related Values and Preferences Regarding Meat Consumption: A Mixed-Methods Systematic Review. Ann Intern Med. 2019;171:742–55. https://doi.org/10.7326/M19-1326.
Pan American Health Organization. Monitoring the premature mortality from the four major noncommunicable diseases (cardiovascular diseases, cancer, diabetes mellitus, and chronic respiratory diseases) in the Region of the Americas, 2000–2019. 2021. https://www.paho.org/en/noncommunicable-diseases-and-mental-health/enlace-data-portal-noncommunicable-diseases-mental/risk. Accessed 15 Jan 2021.
Hausman DM, Welch B. Debate: To Nudge or Not to Nudge. J Polit Philos. 2010;18:123–36. https://doi.org/10.1111/j.1467-9760.2009.00351.x.
Frank SM, Jaacks LM, Batis C, Vanderlee L, Taillie LS. Patterns of Red and Processed Meat Consumption across North America: A Nationally Representative Cross-Sectional Comparison of Dietary Recalls from Canada, Mexico, and the United States. Int J Environ Res Public Health. 2021;18:357. https://doi.org/10.3390/ijerph18010357.
Blakely T, Moss R, Collins J, Mizdrak A, Singh A, Carvalho N, Wilson N, Geard N, Flaxman A. Proportional multistate lifetable modelling of preventive interventions: concepts, code and worked examples. Int J Epidemiol. 2020;49:1624–36. https://doi.org/10.1093/ije/dyaa1.
Acknowledgements
Not applicable.
Funding
This research received financial support from Climate and Land Use Alliance (CLUA) (Grant Number G-2007–56990). The funder had no role in study design, data collection, analysis, decision to publish, or manuscript preparation and does not necessarily share the positions expressed in the Grantee's publication.
Author information
Authors and Affiliations
Contributions
LFMR, TAM, and RSB conducted the data acquisition and analysis. LFMR prepared the first draft of the manuscript and TAM prepared tables and figures. LFMR, TAM, RSB, AOCS, RCFS, LGMM, and MELD substantially contributed to the work’s conception and design. All authors substantively participated in the interpretation of data and revised the work, approved the submitted version and agreed both to be personally accountable for the author's contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out following relevant guidelines and regulations. Although datasets were publicly available and contained deidentified participants’ data, ethics approval was obtained from the Institutional Review Board of the Brazilian INCA at the Brazilian Ministry of Health (CAAE 12008119.8.0000.5274).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no financial or non-financial competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Material A.
Parameters considered in the macrosimulation model. Supplementary Material B. 10th revision of the International Statistical Classification of Diseases and Related Health Problems codes. Supplementary Material C. Relative risk of colorectal cancer per exposition category of red and processed meat consumption and sex. Supplementary Material D. Hyperlinks to publicly archived datasets.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rezende, L.F.M., Malhão, T.A., da Silva Barbosa, R. et al. The current and future costs of colorectal cancer attributable to red and processed meat consumption in Brazil. BMC Health Serv Res 23, 1182 (2023). https://doi.org/10.1186/s12913-023-10169-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-10169-4