
Abstract
Background
A significant and growing portion of the global burden of diseases is caused by neurological disorders. Tele-neurology has the potential to improve access to health care services and the quality of care, particularly in rural and underserved areas. The economic evaluation of the stepped wedge randomised controlled trial NeTKoH aims to ascertain the cost-effectiveness and cost-utility regarding the effects of a tele-neurologic intervention in primary care in a rural area in Germany.
Methods
This protocol outlines the methods used when conducting the trial-based economic evaluation of NeTKoH. The outcomes used in our economic analysis are all prespecified endpoints of the NeTKoH trial. Outcomes considered for the cost-utility and cost-effectiveness analyses will be quality-adjusted life years (QALYs) derived from the EQ-5D-5L, proportion of neurologic problems being solved at the GP’s office (primary outcome), hospital length-of-stay and number of hospital stays. Costs will be prospectively collected during the trial by the participating statutory health insurances, and will be analysed from a statutory health insurance perspective within the German health care system. This economic evaluation will be reported complying with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist.
Discussion
This within-trial economic evaluation relaying the costs and outcomes of an interdisciplinary tele-consulting intervention will provide high-quality evidence for cost-effectiveness and policy implications of a tele-neurological programme, including the potential for application in other rural areas in Germany or other jurisdictions with a comparable health system.
Trial registration
German Clinical Trials Register (DRKS00024492), date registered: September 28, 2021.
Similar content being viewed by others


Background
Although age-standardised incidence, mortality, and prevalence rates of many neurological disorders have been declining, the burden of neurological disorders, as measured by the absolute number of disability-adjusted life years (DALYs), keeps increasing [1]. In 2017, neurological disorders were the third main contributor of DALYs in the European Union (13.3%), right after cardiovascular diseases, and cancer. This can be explained by the long life expectancy in these countries, as well as by the increasing incidence, and the increasingly long duration of ageing-related diseases [2]. In 2010, the costs associated with brain disorders (mental and neurological disorders) in Europe amounted to €798 billion. The high costs of brain disorders were associated with €295 billion in direct health costs, €186 billion in non-medical costs (nursing homes, etc.), and €315 billion in indirect costs (absenteeism from work, pensions, etc.) [3].
Nonetheless, patients suffering from neurological disorders often face multiple hurdles to visit a specialist. While patients in Germany can easily visit a general practitioner (GP), visiting specialists is normally associated with considerable waiting times and logistical difficulties [4, 5]. This problem is more pronounced in rural areas. In the past, the number of neurologists per 100,000 inhabitants in the state of Mecklenburg-West Pomerania was below the national average [6]. Furthermore, there is a wave of outpatient specialists soon reaching retirement age, thus jeopardising the care of the local population [7].
Telemedicine has the potential to deliver health care services to both remote and underserved communities [7, 8]. It can be defined as “the use of telecommunications technology for medical diagnosis and patient care” [9]. Moreover, it has revolutionised inter- and multidisciplinary meetings, where physicians in different medical fields and supporting medical staff can interact. These meetings through telemedicine can foster access to expert opinion, and reduce time for diagnostics and treatment [10]. Telemedicine used in the context of neurological disorders (henceforth “tele-neurology”) can prove to be a powerful tool to strengthen the availability, affordability, and convenience of care for patients in these communities [11].
Multiple studies have analysed the (clinical) effectiveness of delivering telemedicine [12]. However, it is also important to take into account whether telemedicine services represent a good use of funds, and whether healthcare systems should reimburse them. Limitations on billing and reimbursement for time spent in teleconsultations, large investment costs in equipment, bandwidth requirements, and lack of trained employees to use the equipment are mentioned as barriers to the implementation of telemedicine [8, 13]. Thus, it is important to weigh the outcomes of telemedicine interventions and their associated costs against each other by conducting economic evaluations. A recent umbrella review of clinical and cost-effectiveness telemedicine trials assessed eighteen reviews and found evidence that telemedicine can be cost-effective [14]. However, none of the included systematic reviews focused on neurological disorders, and the methodological quality of the majority of the systematic reviews included was deemed as low or critically low, thus hindering the generalisability of their findings.
The NeTKoH trial will assess the use of tele-neurology in a primary care setting in an underserved area in Germany. To investigate the economic impact of NeTKoH on the German health care system, cost-effectiveness analyses, and a cost-utility analysis will be conducted alongside the NeTKoH trial to ascertain the relationship between health outcomes and costs of this new intervention in comparison to standard care. Findings from this economic evaluation can be used as a basis for health policy-makers to facilitate decisions.
Methods and design
Design and study population
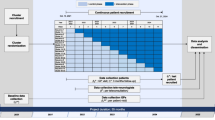
We will conduct the economic evaluation alongside the NeTKoH study, a cluster-randomised controlled trial with a stepped wedge design carried out in a rural area in Germany, from October 2021 to October 2024.
Briefly, NeTKoH offers patients who present themselves to their outpatient GPs with neurological symptoms and diseases in a rural area of northeast Germany to receive neurologic speciality care via a face-to-face video conferencing system between the local outpatient GP and a neurologist from a neurology department of a university clinic in the region. The patients in the control group receive standard care, which only involves in-person face-to-face visits with the local GP.
The main objective of NeTKoH is to strengthen the provision of neurologic care in outpatient GP offices in a rural area by increasing the proportion of neurologic problems being solved at the GP’s office (primary outcome). Secondary outcomes are the number of hospital stays, length-of-stay at the hospital, time until neurologic specialist appointments and diagnostics, patients’ health status and quality of life, and out- and inpatient referrals. Patients are eligible to participate in NeTKoH if they (1) are at least 18 years old, (2) present themselves with neurological symptoms (any symptoms that can warrant a referral to a specialist in neurology) to the participating GP, (3) members of any German statutory health insurance, and (4) able to give informed consent. Complete information on the study design and primary study population are detailed elsewhere [15].
Sample size
The sample size calculation for NeTKoH was based on the primary endpoint, the proportion of neurologic problems being solved in the GPs’ offices, measured by the number of outpatient referrals (neurologist/other specialist), and inpatient referrals (hospital/other). The target sample of 1,089 will provide 78% power at a 5% significance level (two-sided) to detect a 50% improvement in the intervention group, assuming a baseline proportion of 0.2 of neurologic problems solved in the GP’s offices in the control group, and a variation coefficient of 0.30. Assuming a coefficient of variation of 0.20 a power of 81% can be achieved. In the context of cluster randomised trials in the real world context, a coefficient of variation of ≤ 0.25 is considered appropriate [16]. Full details on the sample size calculation for the primary endpoint are reported elsewhere [link to main study protocol].
Patients’ claims data can only be obtained if they belong to the two statutory health insurances that are participating in this study (AOK Nordost and Techniker Krankenkasse). In Germany, claims data from the statutory health insurances are subject to a waiting period of up to 9 months (with waiting periods for inpatient claims data being shorter than those are for outpatient claims data). Hence, it will not be possible to analyse claims data from all recruited patients belonging to these statutory health insurances. According to the current information we obtained from the consortium, we expect to recruit and be able to analyse data from 841 patients belonging to these health insurances.
Besides the participants for whom no claims data will be available and for whom the primary endpoint is missing, this economic evaluation will include all randomised patients, according to the intention-to-treat principle.
Effects/Outcomes
For the cost-utility analysis, the outcome will be measured with the EQ-5D-5L, using German utility weights [17]. This questionnaire comprises five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression, and is collected during baseline and at the 3-month follow-up. Quality-adjusted life years (QALYs) will be calculated by taking the 'area under the curve' between the baseline and 3-month follow-up assessment scores. We will control for baseline EQ-5D-5L scores [18].
The outcome measures for the cost-effectiveness analyses will include the proportion of neurologic problems being solved in the GPs’ offices (primary endpoint), the number of hospital stays, and the length of stay at the hospital. The number of hospital stays and the hospital length-of-stay can be seen as a proxy for a health condition (in general, if an individual needs to stay in the hospital, their health condition is worse than for those who do not need it). Furthermore, hospital stays and days spent in the hospital can be interpreted as a general health outcome impacting a patient's quality of life negatively (patients may feel restricted and uncomfortable during their hospital stay). These outcomes will be assessed using patient-specific claims data during the first three months after study inclusion.
Costs
The economic evaluation will be undertaken from a German statutory health insurance perspective.
We will use claims data from two statutory health insurances (AOK Nordost and Techniker Krankenkasse) to obtain patient-specific costs. Direct medical, and direct non-medical costs, as well as indirect costs, will be considered. Direct medical costs include hospital stays, outpatient visits, drugs, therapeutic appliances, and assistive devices. Direct non-medical costs include reimbursed travel costs to medical examinations and for the indirect costs, sickness leave benefits are considered. In Germany, sick leave payments are only covered by statutory health insurances starting on the 43rd day of sickness. Up until day 42, these costs are covered by employers and are thus not considered in our analysis. We will also include costs associated with the intervention (‘intervention costs’). These include costs for training, investment costs for setting up the infrastructure, and operating costs related to the equipment. Costs associated with tele-consulting systems will be annualised over their lifetime, as provided by the firm making them available for the study. Furthermore, we will take into account staff costs related to conducting and preparing a teleconsultation, as well as the time spent with training on how to use the tele-neurology video-conferencing system. Table 1 lists the cost categories that will be considered.
All costs will be reported in euros, using 2024 as the reference year.
This economic evaluation will compare the costs and effects of each arm over the first 3 months after randomisation. Neither outcomes nor costs will be discounted, since we are only considering outcomes and costs related to the same year when they occur. The relationships between the outcomes and the costs of NeTKoH will be analysed in terms of the incremental cost-effectiveness ratios (ICER). ICERs are calculated as the difference in the mean costs between the intervention and control group divided by the difference in the mean outcomes between the intervention and control group.
Statistical analysis
The parametric G-formula will be used to estimate incremental costs and incremental effects [19, 20].
For the costs, a generalised linear regression with a gamma distribution and log-link function will be carried out to account for the skewness of the costing data. Moreover, it will include random effects for the clusters, with the groups to be compared (intervention or control), and a priori selected covariates (age, sex, and step) as independent variables. Using this model, the expected value of the costs for each individual will be predicted for two hypothetical scenarios, in which the patient receives or does not receive the intervention. The predicted costs under each hypothetical scenario will be calculated for all patients to obtain the mean cost in each scenario (all patients in the study would have received the intervention or all patients in the study would have received the control). The difference between the mean costs in these two scenarios is then calculated to determine the incremental cost of the intervention.
A similar procedure will be used for the remaining outcomes. To calculate the incremental QALYs and incremental hospital length-of-stay caused by the intervention, both continuous variables, a linear regression will be fitted that will include the same random and fixed effects. In the regression in which QALYs is the dependent variable, we will also control for the EQ-5D-5L baseline value, as recommended in the literature [18]. For the primary endpoint (proportion of neurologic problems being solved at the GP’s office), we will run a logistic mixed regression model to predict each individual’s probability of having their case solved at the GP’s office per scenario. We will consider the same random and fixed effects as for other endpoints. Then, the probability of a case being solved will be summed across all patients for each hypothetical scenario to obtain the average number of cases resolved per scenario. Finally, the incremental average number of cases solved by the intervention will be calculated as the difference between the average number of cases solved in the intervention group and the average number of cases solved in the control group. For the endpoint number of inpatient stays, a generalised linear mixed regression with a Poisson distribution will be carried out, with the group and a priori selected covariates as independent variables. Furthermore, random effects for the clusters will be considered.
Incremental mean costs and incremental mean effects (QALYs in the cost-utility analysis and proportion of neurologic problems being solved at the GP’s office, number of inpatient stays, and hospital length-of-stay in the cost-effectiveness analysis) will be used to estimate ICERs.
Assuming a missing at random mechanism and taking into account the clustered data structure, we will conduct multilevel multiple imputation by chained equations with five datasets to impute missing values. Point estimates for incremental effects and incremental costs will be obtained as the averages across the imputed datasets. The imputation models will include as covariates the same variables included in the regression models of the primary effectiveness study, following the guidelines for handling missing data in economic evaluations [21].
Handling uncertainty
Multiple methods will be used to deal with uncertainty: Bootstrapping, sensitivity analyses and extreme value analyses (worst-case scenario).
As a sensitivity analysis, we will conduct a logarithmic transformation of the cost variable to decrease the skewness of the data, and approximate it with a normal distribution to fit a linear mixed regression model.
Bootstrapping allows the analysis of the joint uncertainty due to sampling variation without making parametric assumptions about the distribution. We will conduct multilevel nonparametric bootstrapping according to the Boot MI method to obtain 95% confidence intervals [22]. After multiple imputation on each bootstrapped dataset, we will consider the 2.5% and 97.5% percentiles of the resulting distribution of average metric (across the 5 imputed datasets) as the confidence interval. We will also illustrate the joint uncertainty surrounding both costs and outcomes by plotting cost-effectiveness and cost-utility planes with the bootstrapped cost-effectiveness and cost-utility pairs resulting from the bootstrapping replication runs [23].
The health economic analyses will take the perspective of the German statutory health insurance. However, it is currently uncertain whether the statutory health insurance scheme would provide coverage for the tele-neurology devices used in the outpatient sector. Therefore, the effects of including this cost category will be evaluated in scenario analyses (worst-case scenario).
The reporting of this economic evaluation will follow the Consolidated Health Economic Evaluation Reporting Standards guidelines [24].
The statistical analyses will be carried out using R v4.2.1 (or higher) [25].
Discussion
Patients residing in rural areas of Germany often encounter two major challenges when seeking care from neurologists: lengthy waiting periods and considerable travel distances. Given the current demographic trends, it is imperative to identify measures that can mitigate these issues. Tele-neurology has emerged as a viable solution, and the NeTKoH trial will conduct an economic evaluation to determine the relationship between the outcomes of a tele-neurological intervention and its associated costs. This evaluation aims to quantify the benefits of tele-neurology and provide insights into its cost-effectiveness.
Typically, an intervention is deemed cost-effective if the ICER falls below a certain threshold established by decision-makers in a specific setting. In Germany, there is currently no official threshold in place. The WHO threshold recommendations are based on the country’s gross domestic product (GDP) per capita [26]. According to these recommendations, an intervention can be considered highly cost-effective if the ICER is lower than the GDP per capita. If the ICER falls between one and three times the GDP per capita, the intervention is deemed cost-effective. However, if the ICER is higher than three times the GDP per capita, the intervention is generally considered not cost-effective. The Netherlands has a similar healthcare system (characterised by a mixed compulsory social insurance and private voluntary insurance) with an official threshold range of up to €80,000/QALY [27]. Independently of the threshold considered, we aim to present the cost-utility and cost-effectiveness results in a way that allows decision-makers to weigh up the costs and benefits and decide which interventions to adopt. We will also provide evidence-based results that can be used in the telemedicine field and, more specifically, tele-neurology.
A strength of this study is that patients’ direct medical costs, direct non-medical costs, as well as indirect costs will be obtained directly from the statutory health insurances, thus we are not dependent on patients’ self-reported data that may suffer from memory bias. Furthermore, we will use both a logarithmic transformation of the cost variable to fit a linear mixed regression model, and a generalised linear mixed model with a gamma distribution. These analyses will allow taking into account the methodological uncertainty in the modelling of costs, employing commonly used methods [28]. Moreover, our economic evaluation will include analyses with different endpoints, thus providing a more nuanced understanding of the impact of the intervention. A further strength of our study is the use of the EQ-5D-5L questionnaire to calculate utility scores. Given its widespread use, its use will allow the comparison of the NeTKoH results with other analogous (international) studies.
This planned economic evaluation has some limitations. The first involves the follow-up of the study. While we have planned the follow-up that adequately captures all relevant costs and benefits of the intervention, the follow-up may run too short. In such cases, extrapolation or modelling may be necessary to estimate long-term outcomes. However, such an approach is not feasible in this study due to the significant heterogeneity of the population under investigation. Specifically, the inclusion criteria encompass patients with diverse non-life-threatening neurological symptoms, and the small sample size precludes modelling across subgroups. Second, we will not be able to analyse claims data from all recruited patients because in Germany claims data from statutory health insurances are subject to a waiting period of up to 9 months. Hence, it will not be possible to analyse claims data from all recruited patients. Furthermore, we can only analyse claims data from recruited patients if they belong to two specific statutory health insurances (AOK Nordost and Techniker Krankenkasse). Although in total there are 97 statutory health insurances in Germany, the two insurances participating in this trial belong to different categories of statutory health insurances (Allgemeine Ortskrankenkasse—Local General Sickness Fund and Verband der Ersatzkassen—Association of Substitute Funds) [29]. Thus, we believe that the patients for which claims data will be available will be representative of the entire NeTKoH study population.
Lastly, while at baseline patients fill in their questionnaires at the GP offices, during the 3-month follow-up, questionnaires are administered by phone. Consequently, this may affect the administration of the EQ-5D-5L.
Conclusion
NeTKoH is an interdisciplinary tele-neurological intervention that seeks to provide location-independent and cost-effective treatment to patients suffering from neurological symptoms in underserved areas of Germany. By leveraging modern telecommunication technologies, NeTKoH aims to enhance access to high-quality neurological care, which is currently limited by factors such as long travel distances and waiting times. The economic evaluation results conducted alongside this trial will yield high-quality evidence regarding the use of tele-neurology in primary care settings. The insights gained from this evaluation will be invaluable in informing the development of telemedicine strategies that can optimise the delivery of neurological care to patients in need, regardless of their geographical location.
Availability of data and materials
Not applicable.
Abbreviations
- G-BA:
-
Federal Joint Committee
- GP:
-
General Practitioner
- NeTKoH:
-
Neurologic Tele-Consultations in GP Practices
- SHI:
-
Statutory Health Insurance
- QALY:
-
Quality-Adjusted Life Year
References
Feigin VL, Nichols E, Alam T, Bannick MS, Beghi E, Blake N, et al. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18:459–80.
Deuschl G, Beghi E, Fazekas F, Varga T, Christoforidi KA, Sipido E, et al. The burden of neurological diseases in Europe: an analysis for the Global Burden of Disease Study 2017. The Lancet Public Health. 2020;5:e551–67.
Olesen J, Gustavsson A, Svensson M, Wittchen H-U, Jönsson B, CDBE2010 study group, et al. The economic cost of brain disorders in Europe. Eur J Neurol. 2012;19:155–62.
Kassenärztlichen Bundesvereinigung. Versichertenbefragung der Kassenärztlichen Bundesvereinigung 2020 n.d. https://www.kbv.de/media/sp/Berichtband_Ergebnisse_KBV_Versichertenbefragung_2020.pdf (accessed March 21, 2022).
Feldmeier G, Löffler C, Altiner A, Wollny A, von Podewils F, Ritzke M. Audiovisual teleconsultation for patients with epilepsy in primary care in rural Germany: a pilot study on feasibility and acceptance. Pilot Feasibility Stud. 2022;8:213.
Albrecht M, Fürstenberg T, Gottberg A. Strukturen und Finanzierung der neurologischen und psychiatrischen Versorgung. Berlin: IGES Institut Für Gesundheits-Und Sozialforschung GmbH; 2007.
Landtag Mecklenburg-Vorpommern 7. Wahlperiode. Abschlussbericht der Enquete-Kommission „Zukunft der medizinischen Versorgung in Mecklenburg-Vorpommern“ 2021. https://www.landtagmv.de/fileadmin/media/Dokumente/Druckerzeugnisse/Enquete_Kommission_7_WP_Abschlussbericht.pdf.
Wechsler LR, Tsao JW, Levine SR, Swain-Eng RJ, Adams RJ, Demaerschalk BM, et al. Teleneurology applications: Report of the Telemedicine Work Group of the American Academy of Neurology. Neurology. 2013;80:670–6.
Currell R, Urquhart C, Wainwright P, Lewis R. Telemedicine versus face to face patient care: effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2000:CD002098. https://pubmed.ncbi.nlm.nih.gov/10796678/.
Aghdam MRF, Vodovnik A, Hameed RA. Role of Telemedicine in Multidisciplinary Team Meetings. J Pathol Inform. 2019;10:35.
Cardinale AM. The Opportunity for Telehealth to Support Neurological Health Care. Telemedicine and E-Health. 2018;24:969–78.
Snoswell CL, Chelberg G, De Guzman KR, Haydon HH, Thomas EE, Caffery LJ, et al. The clinical effectiveness of telehealth: A systematic review of meta-analyses from 2010 to 2019. J Telemed Telecare 2021:1357633X211022907.https://journals.sagepub.com/doi/10.1177/1357633X211022907?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed. https://pubmed.ncbi.nlm.nih.gov/34184580/.
Patel U, Malik P, DeMasi M, Lunagariya A, Jani V. Multidisciplinary Approach and Outcomes of Tele-neurology: A Review. 2019. https://doi.org/10.7759/cureus.4410.
Eze ND, Mateus C, Hashiguchi TCO. Telemedicine in the OECD: An umbrella review of clinical and cost-effectiveness, patient experience and implementation. PLoS One. 2020;15:e0237585.
Wainwright K, Mayer I, Oliveira Gonçalves AS, Schulz RS, Kiel S, Chenot J-F, et al. Effect evaluation of a tele-neurologic intervention in primary care in a rural area in Germany—the NeTKoH study protocol of a stepped-wedge cluster randomized trial. BMC Health Serv Res 2023;23. https://doi.org/10.1186/s12913-023-09724-w.
Hayes RJ, Moulton LH. Cluster Randomised Trials. Philadelphia, PA: Chapman & Hall/CRC; 2009. https://doi.org/10.1201/9781584888178.
Ludwig K, Graf von der Schulenburg J-M, Greiner W. German Value Set for the EQ-5D-5L. Pharmacoeconomics. 2018;36:663–74.
Manca A, Hawkins N, Sculpher MJ. Estimating mean QALYs in trial-based cost-effectiveness analysis: the importance of controlling for baseline utility. Health Econ. 2005;14:487–96.
Hernán MA, Robins JM. Causal inference: what if. Boca Raton: Chapman & Hall/CRC; 2020.
Oliveira Gonçalves AS, Rohmann JL, Piccininni M, Kurth T, Ebinger M, Endres M, et al. Economic evaluation of a mobile stroke unit service in Germany. Ann Neurol. 2023. https://doi.org/10.1002/ana.26602.
Faria R, Gomes M, Epstein D, White IR. A guide to handling missing data in cost-effectiveness analysis conducted within randomised controlled trials. Pharmacoeconomics. 2014;32:1157–70.
Schomaker M, Heumann C. Bootstrap inference when using multiple imputation. Stat Med. 2018;37:2252–66.
York Health Economics Consortium. Cost-Effectiveness Plane 2016. https://yhec.co.uk/glossary/cost-effectiveness-plane/ (accessed April 1, 2022).
Husereau D, Drummond M, Augustovski F, de Bekker-Grob E, Briggs AH, Carswell C, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 Explanation and Elaboration: A Report of the ISPOR CHEERS II Good Practices Task Force. Value Health. 2022;25:10–31.
R Core Team. R Core Team. R Core Team (2017). R: A language and environment for statistical computing. Austria: R Found Stat Comput Vienna; 2017.
Bertram MY, Lauer JA, De Joncheere K, Edejer T, Hutubessy R, Kieny M-P, et al. Cost-effectiveness thresholds: pros and cons. Bull World Health Organ. 2016;94:925–30.
Zwaap J, Knies S, van der Meijden C, Staal P, van der Heiden L. Cost-effectiveness in practice. Zorginstituut Nederland; 2015.
Malehi AS, Pourmotahari F, Angali KA. Statistical models for the analysis of skewed healthcare cost data: a simulation study. Health Econ Rev. 2015;5:11.
Bundesgesundheitsministerium. Gesetzliche Krankenversicherung Mitglieder, mitversicherte Angehörige und Krankenstand Monatswerte Januar-Februar 2022 n.d. https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/3_Downloads/Statistiken/GKV/Mitglieder_Versicherte/KM1_Januar_bis_Februar_2022_bf.pdf (accessed March 21, 2022).
Acknowledgements
We would like to thank the NeTKoH Study Group. The NeTKoH Consortium: Paula J. Filser1, Tobias Kurth1, Imke Mayer1, Ana S. Oliveira Gonçalves1, Ricarda S. Schulz1, Kerstin Wainwright1, Aiham Alkhayer2, Anselm Angermaier2,♣, Agnes Flöel2, Verena Horn2, Wieland Köhn2, Malgorzata Kotarz-Boettcher2, Anne Krüger2, Felix von Podewils2, Cordula Weil2, Carl Witt2,, Jean-Francois Chenot3, Simone Kiel3, Elisa Michalowsky3, Michael Böttcher4, Diana Graja5, Katrin C. Reber5, Olga Resch5, Juliane Rothe6, Jacqueline Syring6, 1Institute of Public Health, Charité – Universitätsmedizin Berlin, Berlin, Germany. 2Department of Neurology, University Medicine Greifswald, Greifswald, Germany. 3Department of General Practice, Institute for Community Medicine, University Medicine Greifswald, Greifswald, Germany. 4MEYTEC, Werneuchen, Germany. 5AOK Nordost, Potsdam, Germany. 6Techniker Krankenkasse, Hamburg, Germany. ♣ Nominated consortium representative. Affiliations1 Institute of Public Health, Charité – Universitätsmedizin Berlin, Berlin, Germany2 Department of Neurology, University Medicine Greifswald, Greifswald, Germany³Department of General Practice, Institute for Community Medicine, University Medicine Greifswald, Greifswald, Germany4 MEYTEC, Werneuchen, Germany5AOK Nordost, Potsdam, Germany6Techniker Krankenkasse, Hamburg, Germany.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was supported by the German Innovation Committee for the promotion of new forms of care, which is part of the Federal Joint Committee (grant number 01NVF19007). The funding agency’s role is to review and monitor the project in order to account for public funding. The funding agency developed neither the innovative intervention nor the strategy for program evaluation. This protocol is based on the grant application for the project undergoing a competitive call and peer review process prior to receiving the funding. The study design and the methods described in this study protocol were peer reviewed together with the study presented in [15] during the same grant application process.
Author information
Authors and Affiliations
Consortia
Contributions
AA is the principal investigator of the study and TK is the principal investigator of the evaluation. ASOG and IM drafted the first version of the economic evaluation manuscript. ASOG and IM developed the statistical analysis plan for the economic evaluation. IM developed the statistical analysis plan for the main effectiveness study. All authors reviewed the drafted manuscript, provided feedback and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The project was reviewed and approved by the Ethics Committee of the University Medicine Greifswald, Germany (approval no. 88051/21). Any changes to the study protocol must be approved by the Ethics Committee. A data protection vote for the entire project was received from the data protection office at the University Medicine Greifswald, Germany. Written informed consent, including publication of results in peer-reviewed journals, will be obtained from all participating patients. No additional risks to patients are expected relative to standard care, as NeTKoH aims to improve the quality of care for patients by providing further access to medical care. All technical installations and data transfer protocols have been monitored by the local data protection officers of the participating institutions and are in compliance with the EU General Data Protection Regulation (GDPR), including the data for the evaluation, which will be anonymized. The analysis of NeTKoH is partially based on claims data. The release of the claims data for this purpose will have to be approved by the supervisory authority of the health insurance. The study will be conducted in accordance with the Declaration of Helsinki in its current version, the guidelines of the International Conference on Harmonization of Good Clinical Practice, and applicable national regulations. Important modifications to the protocol will be communicated to the funder, all relevant parties of the project, the trial registry and journals. The results of the evaluation will be reported to project stakeholders and the funding agency via a formal report. Furthermore, study findings will be published in peer-reviewed scientific journals and other publications. For manuscripts, press releases, and other formats of publication, authors, and collaborators will be involved. Dissemination of the results will also take place at conferences and on the project’s website.
Trial registration and status
This study was registered at the German Clinical Trials Register (DRKS00024492) on the 28th of September, 2021. Patient recruitment started in October 2021 and will end in October 2024. Results are expected in July 2025.
Consent for publication
Not applicable.
Competing interests
All authors report funding by the German Innovations Fund of the Federal Joint Committee (G-BA) for the duration of the project.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gonçalves, A.S.O., Mayer, I., Schulz, R.S. et al. Protocol for an economic evaluation of a tele-neurologic intervention alongside a stepped wedge randomised controlled trial (NeTKoH). BMC Health Serv Res 23, 1021 (2023). https://doi.org/10.1186/s12913-023-09985-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09985-5