
Abstract
Background
Sickle cell disease (SCD) is a major public health concern in sub-Saharan Africa, accounting for nearly 75% of the global disease burden. The current analysis evaluated patient characteristics, treatment patterns, healthcare resource utilization (HCRU) and associated costs in patients with SCD based on a Private Medical Insurance Database in Ghana.
Methods
This retrospective longitudinal cohort study was conducted using an e-claims database from Ghana (01 January 2015 to 31 March 2021). Patients were stratified by age (0 month to < 2 years, ≥ 2 years to ˂6 years, ≥ 6 years to < 12 years, ≥ 12 years to < 16 years; ≥16 years), vaso-occlusive crisis (VOC) (< 1, ≥ 1 to < 3, and ≥ 3 per year), and continuous enrolment. Study outcomes related to patient characteristics, comorbidities, treatment pattern, HCRU were evaluated for pre- and post-index period (index period was between July 2015 to March 2020). Descriptive analysis was used to analyse different study variables.
Results
The study included 2,863 patients (mean age: 20.1 years; Min age: 0; Max age: 83; females 56.1%). Overall, 52.2% (n = 1,495) of SCD patients were ≥ 16 years and 17.0% (n = 486) were in the ≥ 2 to ˂6-years age group. The majority of patients aged ≥ 16 years (62.5%) in the database did not have reported VOC episodes, 35.9% of patients had 1 to 3 VOCs per year and 1.5% had ≥ 3 VOCs per year during the follow-up period. Consultation-based prevalence of SCD was 0.5% [95% confidence interval (CI): 0-1.3%] − 1.4% [CI: 0.6-2.2%]. Malaria, upper respiratory tract infection (URTI) and sepsis were the common complications of SCD. Analgesics were the most frequently prescribed medications followed by anti-infectives, hematinics, and antimalarials. Hydroxyurea, a routine standard of care for SCD was under-utilized. SCD patients had median cost incurred for consultation/hospital services of $11.3 (Interquartile range [IQR] $6.2 - $27.2). For patients with VOC, maximum median cost was incurred for medications ($10.9 [IQR $5.0-$32.6]). Overall median healthcare cost was highest for individuals with ≥ 3 VOCs per year during the follow-up period ($166.8 [IQR $70.3-$223.5]).
Conclusion
In this retrospective private insurance claims database analysis, SCD imposes a significant healthcare burden, especially in patients with VOC. There is a need for reimbursed treatment options that could reduce the long-term burden associated with SCD and VOC.
Similar content being viewed by others


Background
Sickle cell disease (SCD) is a group of monogenetic autosomal recessive disorders attributable to point mutations in the beta-globin gene [1, 2]. SCD leads to progressive organ dysfunction and failure due to vaso-occlusion, a chronic inflammatory state and endothelial dysfunction [1, 3]. There are many SCD genotypes, with the most common in sub-Saharan Africa being homozygous SCD and compound heterozygous β-globin S and β-globin C [4]. SCD is the most frequent genetically inherited life-threatening disorder, primarily affecting the African, Indian, Caribbean, and Arab populations [5]. According to the systematic analysis of the Global Burden of Disease Study, 3.2 million people are affected by SCD globally and 176,000 people die per year due to SCD-associated complications [3]. The highest prevalence of the disease is in sub-Saharan Africa where 240,000 people are born with SCD annually [6] and mortality rate is high, with an estimated 50–90% of children dying before the age of 5 [4]. In Ghana, SCD accounts for about 6.3% of the total disease burden in sub-Saharan Africa, with nearly 2% of neonates (~ 15,000) being diagnosed with SCD annually [7].
The clinical manifestations of SCD are broad, and include vaso-occlusive crisis (VOC), hemolytic anemia, acute aplastic crisis, infections including bacterial sepsis, respiratory complications, acute splenic sequestration, and psychosocial morbidity [5, 8]. The burden of malaria is high in sub-Saharan Africa [9]. VOCs are the primary cause of health care encounters in patients with SCD and increased VOC burden is associated with increased risk of mortality [10].
In the management of SCD, hydroxyurea, approved by the United States Food and Drug Administration (USFDA) and European Medicine Agency (EMA), remains a key therapeutic option. In 2018, the Ghana Food and Drug Authority approved the use of hydroxyurea in treatment of both adults and children with SCD [11]. Hydroxyurea exhibits multimodal action – it induces fetal hemoglobin production and reduces inflammation and cell adhesion. Long-term use of hydroxyurea is safe and effective in both pediatric and adult SCD patients [12]. However, laboratory monitoring (complete blood count with white blood cell differential and reticulocyte count) is warranted with the use of hydroxyurea to balance the efficacy and safety risk profile, as hydroxyurea therapy is associated with risk of developing infection, causing myelosuppression and hepatotoxicity [13,14,15]. In recent years, the treatment landscape of SCD has slowly expanded with the advent of novel therapeutic approaches. These therapeutic options target different categories of pathobiology – (i) inhibition of sickle hemoglobin polymerization (voxelotor), (ii) targeting sickle red blood cells (RBCs) - and white blood cells (WBCs) endothelial adhesive events (crizanlizumab), and (iii) antioxidant agents (L-glutamine) [12]. Other therapeutic agents used in SCD include antibiotics, antimalarial agents or antimalarial prophylactics and blood transfusions [12, 16]. Besides the diagnostic and therapeutic challenges, another major hurdle in the management of patients with SCD is the lack of established practices for transition from pediatric to adult care which adds to the healthcare resource utilization (HCRU) in terms of emergency room visits, higher inpatient stays and acute care visits [2].
Although significant progress has been made in the treatment of SCD, it still imposes a substantial economic burden in terms of cost, HCRU and out-of-pocket expenditure. VOC episodes further add to the economic burden of SCD as they are the most common cause of hospitalization and emergency department visits [17].
In the United States (US), the annual mean cost for SCD treatment was United States dollars [US$] 20,206, the highest in patients with more than 3 VOC episodes [18]. In addition, apart from the direct economic burden, SCD also levies an indirect economic burden in terms of loss in work productivity that amounts to US$ 3,145,862 in adult SCD patients with VOC episodes for a period of one year [19].
Sickle cell disease management requires an integrated and holistic approach. However, there are many challenges with the provision of SCD care in sub-Saharan Africa, such as lack of newborn screening, and diagnostic tools, inequities in access to healthcare, including novel therapeutic options, absence of standard treatment guidelines, significant stigmatization, the need for well-resourced and equipped laboratories, few dedicated SCD treatment centers, lack of appropriate preventive and curative services, lack of disease awareness, weak public health systems, financial and emotional cost burden [20, 21].
According to World Bank classification, Ghana is categorized as a lower middle-income country, with incidence of poverty being 45.6% [22]. In the year 2016 (the most recent year for which World Bank estimates are currently available), the poverty headcount ratio at $2.1 a day was 25.3% in the Ghanaian population [23]. As per recent reports, the gross living wage per month in Ghana is $257, while the minimum wage has remained $2 past 2 decades [24]. In a study conducted by the Consortium for the Advancement of Sickle Cell Research, SCD patients in Ghana visited emergency or outpatient departments more frequently for their pain episodes (annualized mean 2.0) compared to SCD patients in the US, United Kingdom (UK), and Italy [25]. In a country like Ghana with high poverty levels, frequent hospitalization and other healthcare expenditures associated with SCD, can impose a substantial economic burden on the affected families and healthcare facilities. In this context, the current study was conducted to determine the treatment pattern and financial burden of SCD in Ghana. The aim of the current analysis was to evaluate the patient characteristics, treatment patterns, hospitalizations, HCRU, total cost incurred in patients with SCD and its subsets, based on the analysis of a private medical insurance (Nationwide Medical Insurance) database in Ghana.
Methods
Study design
This was a longitudinal, secondary database, retrospective, single-cohort study performed using insurance claims data from January 1, 2015 to March 31, 2021. The index date for each patient was defined as the date of first record of diagnosis of SCD, identified during the index period (from 01 July 2015 to 31 March 2020) in the database. Patients with at least 1 SCD-related diagnosis claim in the index period and a minimum follow-up period of 12 month were included in the study. The pre-index period (refers to specified period prior to index date i.e., 6-month baseline before the index period) and post-index period (refers to specified period after index date i.e., 12-month follow-up after the index period) were required to assess the study outcomes.
Data source
The Nationwide Medical Insurance Claims Database is an anonymized patient-level database of all insurance claims generated from their subscribers across Ghana. The database includes manually processed claims from the hospital. Each patient has a unique identifier (ID) in the database and using this ID, patients are linked to multiple visits and other services.
In the current study’s context, the database provided comprehensive data on patient demographics (age and sex), date of attendance, encounter type (inpatient or outpatient), activity type (drugs, consumables [medical/surgical supplies], procedures [medical/surgical procedures or diagnostic investigations], services [consultation or hospital services] and others [administrative services]), claimed amount, reimbursed amount, and diagnostic information.
Study population
The study population was identified based on International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes (ICD-10 codes for diagnosis of SCD [D57: Sickle cell disorders; D57.0: Sickle cell crisis/VOC with acute chest syndrome; D57.1: Sickle cell anemia without crisis; D57.2: Double heterozygous sickling disorders; and D57.8: Other sickle cell disorders]). The study population was stratified by age group (0 month to < 2 years, ≥ 2 years to ˂6 years, ≥ 6 years to < 12 years, ≥ 12 years to < 16 years; ≥16 years). Sub-group analysis was also conducted based on the number of episodes of VOC per year and VOC claims among SCD patients aged ≥ 16 years (< 1 VOC episode per year, ≥ 1 to < 3 VOC episodes per year, ≥ 3 VOC episodes per year). In the study, discrete VOC-related claims within a 3-day gap were combined and recorded as a single VOC episode. VOC episodes were identified based on ICD-10 codes (D57.0, D57.1, D57.2) or prescription of medications (non-steroidal anti-inflammatory drugs [NSAIDs]/Opioids).
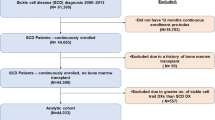
The study included patients with follow-up data of at least 12 months, for ≥ 1 diagnosis claims with SCD during the index period. Continuous medical enrolment data for at least 1 claim (any service) during the 6-month baseline period and 12-month follow-up period were assessed. There were no explicit exclusion criteria for patient selection in the study; however, the patients with no follow-up data or continuous medical enrolment data were excluded. Out of 3,980 potentially eligible patients identified from the database, 2,863 (71.9%) patients met the inclusion criteria and were included in the analysis.
Ethical considerations
Ethics committee approval or obtaining informed consent from patients was not required for this study as it did not involve the collection, use or transmittal of individual identifiable data. Patient identity or medical records were not disclosed in this study. The database uses anonymized data. Anonymization refers to the process of protecting private or sensitive information of patient by complete removal of identifiers such as name of the patient, date of birth, email address etc., that can connect the individual to the data. The study conformed to the ethical principles outlined in the Good Pharmacoepidemiology Practices Guidelines, Declaration of Helsinki 1964 and its later amendments, Good Epidemiological Practice guidelines issued by the International Epidemiological Association, Good Practices for Outcomes Research issued by the International Society for Pharmacoeconomics and Outcomes Research and other applicable guidelines/laws. The dataset and the security of the office where the data set were kept met the requirements of the Health Insurance Portability and Accountability Act of 1996.
The data used for the current study was not publicly available. This data was obtained from Nationwide Medical Insurance following all necessary legal procedures to acquire and use this anonymized patient claims data.
Study outcome measures
-
Demographics and patient characteristics comprising of age, gender and VOC episodes per year were extracted from the claim records.
-
The consultation-based prevalence was calculated for the patients with SCD and those with VOC during the study period (01 January 2015 to 31 March 2021) considering the overall population registered in Nationwide’s Database.
-
Number of patients with each SCD genotype were analyzed based on the ICD-10-CM codes, by year and overall time periods.
-
The comorbidities/complications were assessed during the study period for patients based on age groups and having ≥ 1 SCD claim in the index period.
-
Prescription patterns of SCD treatment (including VOC crisis) in terms of number of patients and claims were evaluated based on different drug categories.
-
The time to first hospitalization (refers to the period from index date to first hospitalization date) during the study period and annual rate of hospitalization during the 12-month follow-up period were also assessed. The assessment was done for both SCD and VOC episodes based on the ICD-10-CM codes for VOC episodes (D57.0, D57.1 and D57.2).
-
Claims data for patients were analyzed for baseline all-cause, SCD-related and VOC–related HCRU, and associated costs (all-cause costs refers to the healthcare costs incurred for all the claims that the patient encountered during the follow-up period; SCD-related and VOC-related costs refers to the healthcare costs incurred for claims that were specific to SCD and VOC, respectively, during the follow-up period) in a 12-month follow-up period from the index diagnosis date (IDD), based on visit type (inpatient and outpatient) and activity type (drugs, consumables, procedures, services, and others). The patients were not mutually exclusive. All-cause HCRU and associated costs were also analyzed for the 6-month baseline period prior to the IDD, only by visit type. The overall HCRU and associated costs were calculated for the VOC-related claims by the adolescent and adult SCD patients (≥ 16 years). This was for the 12-month follow-up period from the IDD and by the VOC episodes.
-
Number and percentage of SCD patients visiting different specialties were evaluated based on claims during the study period after the IDD.
-
Different diagnostic methods, procedures and techniques used in the management of SCD during the study period were assessed based on the number and percentage of patients who underwent the diagnostic tests.
Statistical analysis
Descriptive analysis was used to analyze the different study variables throughout the pre-index and post-index periods. Continuous variables were summarized as number of observations, mean, standard deviation, median, interquartile range (IQR), minimum and maximum, as appropriate. Categorical variables were summarized as frequency and percentages (n, %), and by subgroups of VOC episodes, where appropriate. Demographics, prevalence estimates and SCD types were reported with 95% confidence interval (CI).
Results
Demographics and baseline characteristics of patients with SCD
The mean age of eligible patients was 20.1 ± 16.0 years with the majority being females (n = 1,607, 56.1%). About 52.2% (n = 1,495) of the patients belonged to the age group of ≥ 16 years (Table 1). With respect to VOC episodes in adolescent and adult patients (n = 1,495), 935 patients (62.5%) had zero VOC episodes per year, 537 patients (35.9%) had ≥ 1 to < 3 VOC episodes per year, while 23 patients (1.5%) had ≥ 3 VOCs episodes per year. At least 1 episode of VOC was reported by a total of 1,211 SCD patients and around half (46.2%) of these patients were aged ≥ 16 Years (Table 2).
Consultation-based prevalence of patients with SCD and VOC
During the study period (January 2015-March 2021), year-on-year prevalence of patients with SCD and VOC were analyzed using the claims database. A steady increase in prevalence of patients with SCD and patients with SCD and VOC episodes was observed from year 2015 (0.6%; [95% CI: 0-1.6%] and 0.2%; [95% CI: 0-1.1%], respectively) till the year 2019 (1.4% [95% CI: 0.6-2.2%] and 0.7% [95% CI: 0-1.5%], respectively). However, a dip in the prevalence to 0.5% [95% CI: 0-1.3%] for SCD and 0.3% [95% CI: 0-1.1%] for SCD patients with VOC episodes was noted for the year 2020 (Fig. 1).

Comparison of consultation-based prevalence in patients with SCD and VOC. Abbreviations: SCD: Sickle cell disease; VOC: Vaso-occlusive crisis
Types of SCD
The study patients (n = 2,863) were categorized based on the clinical type of SCD reported, using the ICD-10-CM diagnosis codes. During the study period (January 2015-March 2021), of the 2,863 study patients, 89% (n = 2,562; [95% CI: 88−91%]) of patients reported with diagnosis code for sickle cell disorders (D57), 9% (n = 251; [95% CI: 5−12%]) for other sickle cell disorders (D 57.8) and 7% (n = 211; [95% CI: 4−11%]) of patients for sickle cell crisis/VOC with acute chest syndrome (D57.0) (Table S1)). It should be noted that patient counts were not mutually exclusive.
Comorbidities/Complications in patients with SCD
The most common complications in ≥ 16 years age group included malaria (n = 1,440; 96.3%), upper respiratory tract infection (URTI) (n = 1,071; 71.6%), sepsis/septicemia (n = 445; 29.8%), acute chest syndrome (n = 214; 14.3%) and cellulitis (n = 108; 7.2%), and this trend was similar in patients of ≤ 16 years age group (Table 3). Other complications more commonly observed in the ≥ 16 years age group and not in the younger age groups were end-stage kidney disease requiring dialysis (n = 847; 56.7%) and liver disease (n = 336; 22.5%). The most common complications in patients with VOC episodes were malaria (< 1 VOC per year: n = 894, 95.6%; ≥ 1 to < 3 VOCs per year: n = 523, 97.4%; ≥ 3 VOCs per year: n = 23, 100%), URTI (< 1 VOC per year: n = 671, 71.8%; ≥ 1 to < 3 VOCs per year: n = 383, 71.3%; ≥ 3 VOCs per year: n = 17, 73.9%) and end-stage kidney disease requiring dialysis (< 1 VOC per year: n = 552, 59.0%; ≥ 1 to < 3 VOCs per year: n = 287, 53.4%; ≥ 3 VOCs per year: n = 8, 34.8%). Other complications observed in patients having ≥ 3 VOCs per year were gallstones (n = 4, 17.4%) and osteomyelitis (n = 4, 17.4%).
Treatment patterns
Of the total study patients (n = 2,863), 1,500 patients (52.4%) were treated with different drug classes. The most common drug classes prescribed to patients were NSAIDs (n = 1,134, 75.6%), anti-infectives (n = 783, 52.2%), hematinics (n = 419, 27.9%), antimalarial (n = 398, 26.5%), opioids (n = 146, 9.7%), non-opioids (n = 19, 1.3%) and hydroxyurea (n = 4, 0.3%). Out of 1,497 patients ≥ 16 years of age, 738 patients (49.4%) were treated with different drug classes. The most common drug classes prescribed for patients more than ≥ 16 years were NSAIDs (n = 501, 67.9%), anti-infectives (n = 308, 41.7%), hematinics (n = 271, 36.7%), antimalarial (n = 158, 21.4%), opioids (n = 117, 15.9%) and non-opioids (n = 16, 2.2%) (Table 4).
Hospitalization during 12-Month follow-up period
Overall, 80 patients were hospitalized with 109.5 (IQR 39.0-198.0) median days of time to first hospitalization and a median annual rate of hospitalization of 1.0 (IQR 1.0–2.0). For the patients who experienced VOC episodes (n = 37), the median time to first hospitalization was 162.0 (IQR 48.0253.0) days and median annual rate of hospitalization was 1.0 (IQR 1.0–2.0) (Table S2).
Healthcare resource utilization and associated costs
Healthcare resource utilization and cost during the 6-month baseline period by visit type
During the baseline period of 6 months, for patients with SCD, the total number of claims was higher for outpatient visits (3.0 [IQR 2.0–6.0]) compared to inpatient visits (1.0 [IQR 1.0–1.0]), however, the median inpatient cost was higher compared to outpatient cost ($576.4 [IQR $291.9-$1,129.2] and $49.9 ([IQR $25.5-$91.4], respectively). Similarly, for SCD patients experiencing VOC episodes, the median number of claims for outpatient visit was higher than inpatient visits (3.0 [IQR2.0-5.0]) and 1.0 [IQR 1.0–1.0], respectively), while the inpatient cost was higher than outpatient cost ($70.4 ([IQR $36.8-$141.6] and $43.4 [IQR $23.2-$81.2], respectively). Higher overall healthcare costs were incurred by SCD patients compared to SCD patients experiencing VOC episodes ($55.4 (IQR $27.7-$107.9) and $48.8 (IQR $25.0-$100.9), respectively) (Table S3). This could be attributed to the fact that SCD patients group included the overall population while SCD patients experiencing VOC episodes included only the patients above 16 years of age. Additionally, the HCRU cost assessed during the baseline period also included the costs incurred for all comorbidities-related claims for patients with SCD and SCD with VOC; while the HCRU cost evaluated during the follow-up period included only costs specific to SCD and SCD with VOC claims.
Healthcare resource utilization and cost during 12-month follow-up period by visit type
Assessment of disease-specific HCRU and associated costs for 12-month follow-up period among all SCD patients showed that despite median HCRU outpatient claims and inpatient claims (1.0 claims) being same, the median healthcare cost incurred due to inpatient claims ($92.6) was higher than the cost of outpatient claims ($25.8). A similar observation was noted in SCD patients with VOC episodes. The median HCRU cost was higher due to the inpatient visits ($95.2) than the outpatient visits ($24.6). A higher median overall cost was noted to be incurred by SCD patients with VOC episode ($32.9) than all SCD patients ($30.8) despite the number of all SCD patients (n = 406) being twice as more than the SCD patients with VOC (n = 206) (Table 5).
Healthcare resource utilization and cost during 12-month follow-up period by activity type
The median number of claims was same for different activity types for SCD patients and SCD patients with VOC episodes. In patients with SCD, the highest cost incurred was for consultation or hospital services ($11.3 [IQR $6.2-$27.2]) and lowest cost was for administrative services ($5.1 [IQR $2.4-$13.8]). However, for patients with VOC episodes, cost incurred was highest for medications ($10.9 [IQR $5.0-$32.6]) and lowest for administrative services ($6.8 [IQR $2.8-$13.8]) (Table S4). Availability of free health care in the USA or Europe compared to sub-Saharan Africa could explain overall reported relative higher rates of hospital admission versus VOC managed in an outpatient setting [26].
By VOC episodes and age groups: for 12-month follow-up
In terms of VOC episodes, maximum number of visits was reported for patients with ≥ 1 to < 3 VOC episodes per year (n = 216); however, median was higher in case of ≥ 3 VOCs per year (4.0 [IQR 2.0–7.0]). The median healthcare cost was highest for patients with ≥ 3 VOCs per year ($166.8 [IQR $70.3-$223.5]) (Table 6).
The healthcare costs pertaining to visit type and activity type in SCD patients were higher compared to those costs in SCD patients with VOC episodes, during the 12-month follow-up period.
Specialties visited by patients with SCD
Of the total 2,863 patients in the study, 2,408 patients visited physicians of different specialties for treatment advice. General physician (GP) visits were the highest with patient visits of 1,810 (75.2%) and claims of 2,867 (69.7%). This was followed by pediatric and gynecology consultations (Table S5). Around 5.7% (n = 137) patients had specialist consultation with a total of 252 claims (6.1%).
Diagnostic investigations
Of the overall study population (n = 2,863), 96% of patients (n = 2,759) underwent diagnostic investigations with total 4,185 claims. The most frequently used diagnostic investigations with the highest number of claims were full blood count, hemoglobin electrophoresis, blood smear for malaria parasites, sickling test, and routine urine examination (Table S6).
Discussion
SCD is a global public health concern due to substantial morbidity, mortality, and socioeconomic burden. The sub-Saharan Africa region accounts for more than 75% of global SCD burden [20, 21, 27,28,29]. Despite this considerable disease burden, there is a dearth of real-world data published on the disease burden, treatment patterns and economic burden of SCD from the sub-Saharan Africa region and could be attributed to the lack of a national database on patients with SCD care in regions of sub-Saharan Africa [30]. Hence, this cost of illness study was conducted to evaluate the HCRU for patients with SCD and VOC episodes in Ghana using Nationwide Medical Insurance Database. The study also assessed diagnostic investigations, treatment patterns and specialties visited for treatment advice among patients with SCD and VOC, in a real-world setting.
The yearly prevalence of patients with SCD as well as the SCD patients with VOC episodes during the study period exhibited an increasing trend, suggestive of the growing disease burden in Ghana. However, a dip in prevalence was observed in the year 2020 which could be attributed to the under-reporting of the claims due to coronavirus disease (COVID-19) pandemic. Majority of the patients were ≥ 16 years of age (52.2%) with a predominantly female population and having VOC episodes. These findings are consistent with the real-world study by Foundation for Sickle Cell Disease Research [31]. In the current study, 33% in of the patients belonged to 0 months to < 6 years age group. A systematic review and meta-analysis reports highest prevalence and mortality of SCD in children under 5 years of age, in Africa [32].
In the current study, number of VOC episodes were evaluated only in patients with SCD aged ≥ 16 years and not in patients with SCD < 16 years. The probable reasons could be difficulty in characterizing VOC episodes in children. Diagnosis of VOC in children is complicated by the fact that VOC affecting the bone is the most common acute clinical manifestation of SCD in this population. Furthermore, VOCs are often confused with the much less frequently occurring osteomyelitis [33, 34]. A recent Phase 3 study reported that a shorter duration of VOC episode was observed in patients < 16 years of age [35]. Additionally, the grouping was done in line with the previous trials conducted on patients with SCD (SOLACE trial and SUSTAIN trial [36, 37]. Moreover, the demographic data obtained during the analysis also represented the high disease burden in patients < 16 years of age (47.8%). Hence, the patients were stratified into subpopulation < 16 years and ≥ 16 years.
In the current study, majority of SCD patients had common sequelae of SCD – VOC episodes, infections, malaria, sepsis, and acute chest syndrome among others in accord with other studies [5, 8]. Furthermore, regions of sub-Saharan Africa with high incidence of SCD are also associated with highest density of malaria. Although the sickle cell mutation at one allele of beta-globin gene confers a survival advantage in malaria endemic areas, inheritance of the mutation at both alleles, predisposes individuals to severe malaria and increased mortality from other complications of SCD [38]. Studies have reported that VOC in SCD patients accounts for 95% of emergency department visits and inpatient admissions [34, 39, 40]. This analysis also evaluated the annual rate of hospitalization admissions which was found to be 1.6 ± 1.1. A study conducted in Ghana on patients (with SCD), aged > 13 years reported the annual hospitalization rate to be 2.6%, attributed mostly to the acute complications [27].
Our analysis identified a greater number of prescriptions for analgesics, anti-infectives, and hematinics as compared to hydroxyurea, the standard of care treatment for SCD. Despite hydroxyurea being included in the World Health Organization model list of essential medications for children and the large body of evidence for its established efficacy in terms of reduced frequency of VOC episodes, transfusions, and hospitalizations [41,42,43,44], its use is sub-optimal in the sub-Saharan African region. Minimal use of hydroxyurea in the region could be attributed to lack of data on magnitude and impact of SCD in the region, lack of evidence-based guidelines on feasibility, safety, and benefits of hydroxyurea in the region. Other barriers to use of hydroxyurea in the region include drug availability, cost of treatment and laboratory monitoring. Another study in the region emphasized on wider access to hydroxyurea which provides a cost-effective therapeutic approach to deter the progression of disease in SCD patients [45, 46]. Through public-private partnerships, Novartis is working with Ministry of Health of Ghana, Ghana Health Service, Sickle Cell Foundation and Patient Association Groups to increase access to hydroxyurea including a pediatric-friendly formulation.
Comprehensive management of SCD requires effective healthcare systems and necessitates healthcare professionals to have appropriate knowledge of the disease. The current study noted that the treatment of SCD was largely by GP practice compared to specialized care [47]. Considering the limited number of specialist physicians such as hematologists and pediatricians in the region, upskilling community practice physicians such as GPs and internal medicine doctors could help strengthen the care delivery for SCD patients.
In the current study, cost due to inpatient claims for SCD patients was significantly higher compared to cost due to outpatient claims; the cost incurred on consultation/hospital services was highest compared to other HCRU costs (drugs, consumables, procedure, and administrative services). The SCD patients who experienced ≥ 3 VOC episodes per year incurred nearly 3 times more healthcare costs than those with lesser VOC episodes per year [48]. A retrospective cohort analysis of patient-level data from Medicaid database reported that patients with > 3 VOC episodes had the highest annual SCD cost across all settings (mean: US$ 58,950); suggesting that HCRU costs increased with the increase in number of VOC episodes [18]. Few studies which have assessed the economic burden of SCD in countries within sub-Saharan Africa show that households spend a considerable proportion of their income on direct costs (hospitalization, medications, outpatient visits) associated with SCD [49]. The Economic Intelligence Unit 2020 reported that Nigeria had the highest annual costs (direct and indirect costs) of SCD (US$ 6.5 billion per year), followed by Angola (US$ 719.6 million per year) and Ghana (US$ 472.8 million per year) among other sub-Saharan countries [50]. The report highlighted that in Ghana, medication was the major cost driver for patients aged 5–14 and ≥ 15 years (US$ 346 per year and US$ 526 per year, respectively) [51].
Our study noted higher healthcare costs incurred by SCD patients with VOC episodes than SCD patients without VOC episodes, despite the number of SCD patients without VOC being twice as many as SCD patients with VOC.
Our major limitation for this analysis is based on its retrospective design and analysis from a claims database. The study sample size includes only a subset of the privately insured population of Ghana with continuous enrolment during the study period whose demographic data mapping was available; thus, the results might not be applicable for the entire population with SCD in Ghana. Analysis of Ghana Demographic health survey dataset suggested that economic and educational status, marital status (single/widowed), and geographical disparity are the major determinants for not enrolling in the private insurance in Ghana. The financial status determined the insurance status, with poorest, poorer, and middle-income groups being less likely to pay themselves for insurance. Women (single/widowed) were less likely to be covered relative to married women although this group was more likely to pay the insurance premiums themselves. Geographic disparities and educational status also accounted for inequity in the insurance enrolment [52]. Clinical and disease-specific parameters (e.g., duration or severity of the disease) could not be obtained from the claims data. Emergency department visits have not been included or may have been combined with the inpatient visit, leading to information bias. There could be a possibility of missing data due to patients not following up at the same hospital or group of hospitals or not being able to follow-up at all. The medications filled over the counter, provided by the physicians or obtained out-of-pocket could not be ascertained in the claims data. Only direct healthcare costs were evaluated; indirect costs such as work productivity and quality of life were not analyzed for SCD. The database also does not allow one-to-one mapping between diagnosis and medications/procedures/consumables. Hence, some of the reported SCD specific medications, services and costs may not be related directly to SCD. VOC admission within a gap of 3 days was taken as a single episode to validate the accurate capture of VOC episode and to overcome under- or over-representation of VOC episodes. Additionally, VOC episodes managed at home were not captured. Moreover, VOC data for children under 16 years of age were not captured during the analysis. Our study was designed to capture only VOC data above 16 years of age. The high prevalence and mortality rate associated with children has been noted in previous studies [53, 54]. Hence the VOC sub-group in our study cohort could have been under-represented which has implications on the cost distribution and our findings around this major complication of SCD.
However, the strength of the study lies in the fact that it is the first-of-its-kind being conducted in Ghana using the National Private Insurance Claims database. It captures information for the population covered by Nationwide Medical Insurance Claims Database representing 10–15% of the Ghanaian population.
Conclusion
To the best of our knowledge, the current study is the first-of-its-kind analysis conducted using e-claims database to evaluate the disease and economic burden on patients with SCD in Ghana. The study findings indicate an increased disease burden on patients with SCD and a substantial impact on the healthcare costs, especially in the sub-group of patients with VOC episodes. In our study VOC episodes were seen in less than half of the SCD patients. The most common complications were malaria, URTI and sepsis. Hydroxyurea use was sub-optimal in this cohort of patients. We hypothesized that barriers relating to drug availability, cost of treatment, and laboratory monitoring could have contributed although this is a cohort of patients with private health insurance. Understanding these barriers and efforts to increase access both in private and public sectors of Ghana is paramount for reducing the disease and economic burden associated with SCD. The study also reported a significantly higher HCRU in the treatment of VOC. The VOC cost burden equals the cost burden of SCD treatment, which warrants the need for better management of VOC. However, the limitations of the current study, as listed above, make it likely that the costs of SCD in Ghana are higher than the cost estimates stated here. Additionally, the direct medical expenses and societal costs have disproportionately larger impact on low-income families.
In 2021, the Ghana Food and Drug Authority approved registration of crizanlizumab for prevention of VOC in SCD patients >16 years and over. Additionally, Ghana is participating in the ongoing Phase 3 clinical trial (STAND) with crizanlizumab, the first time a clinical study has been conducted with a biologic agent for managing SCD. Innovative treatments with disease modifying modalities such as crizanlizumab, targeting VOC episodes could be considered in SCD patients who are intolerable to hydroxyurea or with recurring VOCs despite maximum tolerable doses of hydroxyurea.
Availability of data and materials
All data generated or analyzed during this study are included in this published article/as supplementary information files.
Abbreviations
- SCD:
-
Sickle cell disease
- VOC:
-
Vaso-occlusive crisis
- USFDA:
-
United States Food and Drug Administration
- EMA:
-
European Medicine Agency
- RBC:
-
Red blood cell
- WBC:
-
White blood cell
- HCRU:
-
Healthcare resource utilization
- US:
-
United States
- US$:
-
United States dollar
- UK:
-
United Kingdom
- ID:
-
Identifier
- ICD-10-CM:
-
International Classification of Diseases, Tenth Revision, Clinical Modification
- NSAID:
-
Non-steroidal anti-inflammatory drugs
- IDD:
-
Index diagnosis date
- IQR:
-
Interquartile range
- CI:
-
Confidence interval
- N:
-
Number of patients
- URTI:
-
Upper respiratory tract infection
- GP:
-
General physician
- COVID-19:
-
Coronavirus disease
References
Ogu UO, Billett HH. Comorbidities in sickle cell disease: adult providers needed! Indian J Med Res. 2018;147(6):527–9.
Ogu UO, Badamosi NU, Camacho PE, Freire AX, Adams-Graves P. Management of Sickle Cell Disease Complications Beyond Acute chest syndrome. J Blood Med. 2021;12:101–14.
Sundd P, Gladwin MT, Novelli EM. Pathophysiology of Sickle Cell Disease. Annu Rev Pathol. 2019;14:263–92.
Grosse SD, Odame I, Atrash HK, Amendah DD, Piel FB, Williams TN. Sickle cell disease in Africa: a neglected cause of early childhood mortality. Am J Prev Med. 2011;41(6 Suppl 4):398–405.
Inusa BPD, Hsu LL, Kohli N, Patel A, Ominu-Evbota K, Anie KA, et al. Sickle Cell Disease-Genetics, Pathophysiology, clinical presentation and treatment. Int J Neonatal Screen. 2019;5(2):20.
Paintsil V, Amuzu EX, Nyanor I, Asafo-Adjei E, Mohammed AR, Yawnumah SA, et al. Establishing a Sickle Cell Disease Registry in Africa: experience from the Sickle Pan-African Research Consortium, Kumasi-Ghana. Front Genet. 2022;13:802355.
Ohene-Frempong K, Oduro J, Tetteh H, Nkrumah F. SCREENING NEWBORNS FOR SICKLE CELL DISEASE IN GHANA. Pediatrics. 2008;121(Supplement2):120–S1.
Pecker LH, Darbari DS. Psychosocial and affective comorbidities in sickle cell disease. Neurosci Lett. 2019;705:1–6.
Organization WH, World Malaria. Day 2022 2022 [Available from: https://www.who.int/campaigns/world-malaria-day/2022.].
Desai RJ, Mahesri M, Levin R, Globe D, McKerracher K, Mutebi A, et al. Clinical outcomes and Healthcare utilization in patients with Sickle Cell Disease: a Nationwide Cohort Study of Medicaid beneficiaries. Blood. 2019;134(Supplement1):3459.
Allotey-Babington GLSO, Williams AA, Asiedu EA, Amuakwa MK, Nettey H. Hydroxyurea granules for the management of sickle cell disease in children. Sci Afr. 2022;16:1–8.
Matte A, Zorzi F, Mazzi F, Federti E, Olivieri O, De Franceschi L. New Therapeutic Options for the treatment of Sickle Cell Disease. Mediterr J Hematol Infect Dis. 2019;11(1):e2019002.
Okocha EC, Gyamfi J, Ryan N, Babalola O, Etuk E-A, Chianumba R, et al. Barriers to therapeutic use of Hydroxyurea for Sickle Cell Disease in Nigeria: a cross-sectional survey. Front Genet. 2022;12:765958.
LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Phenotypes Of Drug Induced Liver Injury. [Updated 2019 May 4]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548473/.
McGann PT, Ware RE. Hydroxyurea therapy for sickle cell anemia. Expert Opin Drug Saf. 2015;14(11):1749–58.
Adepoju P. Ghana takes on sickle-cell disease. The Lancet. 2020;395(10222):402.
Rizio AA, Bhor M, Lin X, McCausland KL, White MK, Paulose J, et al. The relationship between frequency and severity of vaso-occlusive crises and health-related quality of life and work productivity in adults with sickle cell disease. Qual Life Res. 2020;29(6):1533–47.
Shah N, Bhor M, Xie L, Paulose J, Yuce H. Medical Resource Use and costs of treating Sickle Cell-related Vaso-occlusive Crisis Episodes: a retrospective claims study. J Health Econ Outcomes Res. 2020;7(1):52–60.
Holdford D, Vendetti N, Sop DM, Johnson S, Smith WR. Indirect Economic Burden of Sickle Cell Disease. Value Health. 2021;24(8):1095–101.
Williams TN. Sickle cell disease in Sub-Saharan Africa. Hematol Oncol Clin North Am. 2016;30(2):343–58.
Mburu J, Odame I. Sickle cell disease: reducing the global disease burden. Int J Lab Hematol. 2019;41(Suppl 1):82–8.
Initiative OPaHD. Multidimensional Poverty – Ghana [Available from: https://ophi.org.uk/multidimensional-poverty-ghana/].
Bank TW. Poverty headcount ratio at $2.15 a day(2017 PPP) (% of population)-Ghana [Available from: https://data.worldbank.org/indicator/SI.POV.DDAY?locations=GH .].
Andersen LEMA, Gonzales A. Living Wage Update Report: Peri-urban, Lower Volta Area, Ghana, 2022 2022 [Available from: https://www.globallivingwage.org/wp-content/uploads/2018/04/Updatereport_Ghana_2022_29032022final.pdf].
Strunk C, Tartaglione I, Piccone CM, Colombatti R, Andemariam B, Manwani D, et al. Global geographic differences in healthcare utilization for sickle cell disease pain crises in the CASiRe cohort. Blood Cells Molecules and Diseases. 2021;92:102612.
Inusa BPD, Colombatti R, Rees DC, Heeney MM, Hoppe CC, Ogutu B, et al. Geographic differences in phenotype and treatment of children with Sickle Cell Anemia from the multinational DOVE study. J Clin Med. 2019;8(11):2009.
Asare EV, Wilson I, Benneh-Akwasi Kuma AA, Dei-Adomakoh Y, Sey F, Olayemi E. Burden of Sickle Cell Disease in Ghana: the Korle-Bu experience. Adv Hematol. 2018;2018:6161270.
Mulumba LL, Wilson L. Sickle cell disease among children in Africa: an integrative literature review and global recommendations. Int J Afr Nurs Sci. 2015;3:56–64.
McGann PT, Hernandez AG, Ware RE. Sickle cell anemia in sub-saharan Africa: advancing the clinical paradigm through partnerships and research. Blood. 2017;129(2):155–61.
Narh CT, Der J, Ofosu A, Blettner M, Wollschlaeger D. Time trends, sociodemographic and health factors associated with discharge and length of stay of hospitalised patients with sickle cell disease in Ghana: a retrospective analysis of national routine health database. BMJ Open. 2021;11(10):e048407.
Bronté-Hall L, Parkin M, Green C, Tchouambou E, Huynh L, Puri-Sharma C, et al. Real-world clinical burden of Sickle Cell Disease in the US Community-Practice setting: a single-center experience from the Foundation for Sickle Cell Disease Research. Blood. 2019;134(Supplement1):5856.
Wastnedge E, Waters D, Patel S, Morrison K, Goh MY, Adeloye D, et al. The global burden of sickle cell disease in children under five years of age: a systematic review and meta-analysis. J Glob Health. 2018;8(2):021103.
Zolaly M, Al-Mohammadi G, Al-Saadi G, Qasim D. Vaso-occlusive crises in patients with sickle cell disease: parents’ perspectives and association with disease outcomes. J Taibah Univ Med Sci. 2019;14(6):515–22.
Darbari DS, Sheehan VA, Ballas SK. The vaso-occlusive pain crisis in sickle cell disease: definition, pathophysiology, and management. Eur J Haematol. 2020;105(3):237–46.
Casella JF, Barton BA, Kanter J, Black LV, Majumdar S, Inati A, et al. Effect of Poloxamer 188 vs placebo on painful vaso-occlusive episodes in children and adults with Sickle Cell Disease: a Randomized Clinical Trial. JAMA. 2021;325(15):1513–23.
Kutlar A, Kanter J, Liles DK, Alvarez OA, Cançado RD, Friedrisch JR, et al. Effect of crizanlizumab on pain crises in subgroups of patients with sickle cell disease: a SUSTAIN study analysis. Am J Hematol. 2019;94(1):55–61.
Heeney MM, Rees DC, De Montalembert M, Odame I, Brown RCC, Wali Y, et al. Initial safety and efficacy results from the phase II, Multicenter, open-label Solace-Kids Trial of Crizanlizumab in Adolescents with Sickle Cell Disease (SCD). Blood. 2021;138(Supplement 1):12.
McAuley CF, Webb C, Makani J, Macharia A, Uyoga S, Opi DH, et al. High mortality from Plasmodium falciparum malaria in children living with sickle cell anemia on the coast of Kenya. Blood. 2010;116(10):1663–8.
Lee S, Vania DK, Bhor M, Revicki D, Abogunrin S, Sarri G. Patient-reported outcomes and economic burden of adults with Sickle Cell Disease in the United States: a systematic review. Int J Gen Med. 2020;13:361–77.
Oladapo A, Swallow E, Briggs A, Zichlin ML, Mellgard BL. Prevalence of Vaso-Occlusive crises in patients with Sickle Cell Disease: a retrospective US claims database analysis. Blood. 2020;136(Supplement 1):8–9.
Le PQ, Gulbis B, Dedeken L, Dupont S, Vanderfaeillie A, Heijmans C, et al. Survival among children and adults with sickle cell disease in Belgium: benefit from hydroxyurea treatment. Pediatr Blood Cancer. 2015;62(11):1956–61.
Quarmyne MO, Dong W, Theodore R, Anand S, Barry V, Adisa O, et al. Hydroxyurea effectiveness in children and adolescents with sickle cell anemia: a large retrospective, population-based cohort. Am J Hematol. 2017;92(1):77–81.
Voskaridou E, Christoulas D, Bilalis A, Plata E, Varvagiannis K, Stamatopoulos G, et al. The effect of prolonged administration of hydroxyurea on morbidity and mortality in adult patients with sickle cell syndromes: results of a 17-year, single-center trial (LaSHS). Blood. 2010;115(12):2354–63.
Peine BR, Callaghan MU, Callaghan JH, Glaros AK. Prophylactic Hydroxyurea treatment is Associated with Improved Cerebral Hemodynamics as a surrogate marker of stroke risk in Sickle Cell Disease: a retrospective comparative analysis. J Clin Med. 2022;11(12):3491.
Tshilolo L, Tomlinson G, Williams TN, Santos B, Olupot-Olupot P, Lane A, et al. Hydroxyurea for children with Sickle Cell Anemia in Sub-Saharan Africa. N Engl J Med. 2019;380(2):121–31.
McGann PT, Tshilolo L, Santos B, Tomlinson GA, Stuber S, Latham T, et al. Hydroxyurea Therapy for Children with Sickle Cell Anemia in Sub-Saharan Africa: Rationale and Design of the REACH Trial. Pediatr Blood Cancer. 2016;63(1):98–104.
Jonathan A, Tutuba H, Lloyd W, Ndunguru J, Makani J, Ruggajo P, et al. Healthcare Workers’ knowledge and resource availability for care of Sickle Cell Disease in Dar es Salaam, Tanzania. Front Genet. 2021;12:773207.
Shah N, Bhor M, Xie L, Halloway R, Arcona S, Paulose J, et al. Evaluation of Vaso-occlusive crises in United States Sickle Cell Disease Patients: a retrospective claims-based study. J Health Econ Outcomes Res. 2019;6(3):106–17.
Ngolet LO, Moyen Engoba M, Kocko I, Elira Dokekias A, Mombouli JV, Moyen GM. Sickle-cell Disease Healthcare cost in Africa: experience of the Congo. Anemia. 2016;2016:2046535.
Assessing the burden of sickle cell disease in Sub-Saharan Africa. : a cost-of-illness study: ECONOMIST INTELLIGENCE UNIT; [Available from: https://www.eiu.com/n/campaigns/assessing-the-burden-of-sickle-cell-disease-in-sub-saharan-africa-a-cost-of-illness-study/].
Adegoke SA, Abioye-Kuteyi EA, Orji EO. The rate and cost of hospitalisation in children with sickle cell anaemia and its implications in a developing economy. Afr Health Sci. 2014;14(2):475–80.
Ayanore MA, Pavlova M, Kugbey N, Fusheini A, Tetteh J, Ayanore AA, et al. Health insurance coverage, type of payment for health insurance, and reasons for not being insured under the National Health Insurance Scheme in Ghana. Health Econ Rev. 2019;9(1):39.
Makani J, Cox SE, Soka D, Komba AN, Oruo J, Mwamtemi H, et al. Mortality in Sickle Cell Anemia in Africa: a prospective cohort study in Tanzania. PLoS ONE. 2011;6(2):e14699.
Oppong M, Lamptey H, Kyei-Baafour E, Aculley B, Ofori EA, Tornyigah B, et al. Prevalence of sickle cell disorders and malaria infection in children aged 1–12 years in the Volta Region, Ghana: a community-based study. Malar J. 2020;19(1):426.
Acknowledgements
Medical writing and editorial support were provided by Dr Kavitha Ganesha (Senior Consultant, IQVIA, India), Sharda Kandwal (Senior Consultant, IQVIA, India) and Bushra Nabi (Associate Consultant, IQVIA, India) and assistance with data analysis was provided by Prashant Pandey from IQVIA, India. Support for this assistance was funded by Novartis.
Funding
This study was funded by Novartis.
Author information
Authors and Affiliations
Contributions
Conception or design of the work: KM, YD-A, CS, DD, AE, NA, KS, OE, KA; Conception or design of the work and analysis: BR, AN. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was based on secondary, de-identified data which comply with the Health Insurance Portability and Accountability Act (HIPAA). Ethics committee approval was not required for this study, as it did not involve the collection, use, or transmittal of individual identifiable data. Database contains anonymized structured insurance e-claims data of the patients. Patients’ identity or medical records were not disclosed for the purposes of this study, except where disclosure was allowed as per applicable law. The study conformed to the ethical principles of the Declaration of Helsinki of 1964 and its later amendments.
The data used for the current study was not publicly available. This data was obtained from Nationwide Medical Insurance following all necessary legal procedures to acquire and use this anonymized patient claims data. According to data sharing agreement between Nationwide Medical Insurance and IQVIA, IQVIA was granted a perpetual, non-exclusive license to use only the elements of the data described in the agreement. IQVIA was permitted to use the data after anonymizing and standardizing for health insurance claims data-based analysis and research studies and was allowed to share the anonymized and standardized data with its client for health insurance claims databased analysis and research studies. IQVIA agreed to adhere to measures to comply with applicable laws, including those related to data protection.
Consent for publication
Not applicable.
Novartis has no conflict of interest to declare related to patents, products in development and marketed products.
The authors have no conflict of interest to declare.
All Novartis Employees were full-time employee of Novartis during the conduct of the study. All IQVIA Employees were paid consultants to Novartis in connection with the development of this manuscript. These competing interests of the authors does not alter their adherence to (BMC Health Services Research) policies on sharing data and materials.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Type of Sickle Cell Disease (January 2015-March 2021). Table S2. Hospitalization in All the Patients Having SCD Diagnosis and Inpatient Visit (12-Month Follow-up period). Table S3. Healthcare Resource Utilization and Costs by Visit Type (6-Month Baseline Period). Table S4. Healthcare Resource Utilization and Costs by Activity Type (12-Month Follow-up). Table S5. Specialities Visited by Patients with SCD (January 2015-March 2021). Table S6. Diagnostic Investigations Conducted on Patients With SCD (January 2015-March 2021)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Marfo, K., Dei-Adomakoh, Y., Segbefia, C. et al. Evaluation of treatment patterns, healthcare resource utilization and cost of illness for sickle cell disease in Ghana: a private medical insurance claims database study. BMC Health Serv Res 23, 1018 (2023). https://doi.org/10.1186/s12913-023-09984-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09984-6