
Abstract
Objective
To understand developers’ perception of patient (versions of) guidelines (PVGs), and identify challenges during the PVG development, with the aim to inform methodological guidance for future PVG development.
Methods
We used a descriptive qualitative design. Semi-structured interviews were conducted virtually from December 2021 to April 2022, with a purposive sampling of 12 PVG developers from nine teams in China. Conventional and directed content analysis was used for data analysis.
Results
The interviews identified PVG developers’ understanding of PVGs, their current practice experience, and the challenges of developing PVGs. Participants believed PVGs were a type of health education material for patients; therefore, it should be based on patient needs and be understandable and accessible. Participants suggested that PVGs could be translated/adapted from one or several clinical practice guidelines (CPG), or developed de novo (i.e., the creation of an entirely new PVG with its own set of research questions that are independent of existing CPGs). Participants perceived those existing methodological guidelines for PVG development might not provide clear instructions for PVGs developed from multiple CPGs and from de novo development. Challenges to PVG development include (1) a lack of standardized and native guidance on developing PVGs; (2) a lack of standardized guidance on patient engagement; (3) other challenges: no publicly known and trusted platform that could disseminate PVGs; concerns about the conflicting interests with health professionals.
Conclusions and practice implications
Our study suggests clarifying the concept of PVG is the primary task to develop PVGs and carry out related research. There is a need to make PVG developers realize the roles of PVGs, especially in helping decision-making, to maximize the effect of PVG. It is necessary to develop native consensus-based guidance considering developers’ perspectives regarding PVGs.
What is new
To our knowledge, this is the first study to understand Chinese developers’ perceptions of patient versions of guidelines (PVGs). We found that no participant noticed the role of PVG in aiding decision-making due to their low awareness of the necessity for patients to make their clinical decisions.
Our study found that PVG developers have a misunderstanding of PVGs, which might be a reason why the interviewees stated that they used one of three models for the development of PVGs instead of following the GIN recommendation. Thus, a sound Chinese translation of the GIN material is urgently needed so that this misunderstanding can be avoided.
This is the first study to explore challenges encountered by PVG developers during the PVG development, including:1) a lack of standardized and native guidance on developing PVGs; 2) a lack of standardized guidance on patient engagement; 3) other challenges: no publicly known and trusted platform that could disseminate PVGs; concerns about the conflicting interests with health professionals.
A comprehensive and pragmatic PVG development method to standardize PVG development and a publicly known and trusted platform that could disseminate PVGs in China is warranted.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Patient versions of guidelines (PVGs) are tools that “translate” clinical practice guidelines (CPG) recommendations and their rationales produced initially for health professionals into a form that is more easily understood and used by patients and the public [1]. PVGs could support patient decision-making by providing multiple patient-related recommendations and informing patients of relevant information regarding option(s) (harms, benefits, and risks), eliciting values, preferences, and contemplation so that patients can choose the treatment or service most appropriate for them. In situations where the patients are not offered treatment or service options recommended in a PVG, patients may communicate with doctors to express their preferences. Then, doctors may choose the recommended intervention in the PVG after weighing the pros and cons; thus, supporting the source CPG implementation (from now on, we will refer to the CPGs and the recommendations selected for translation to PVG as “source CPGs” and “source recommendations”). PVGs are also one of the strategies to facilitate the decision-making between the patient and their provider. By making the recommendations accessible to patients and easy to understand, PVGs can increase shared decision-making with their providers [2]. To January 2023, the Scottish Intercollegiate Guidelines Network [3] has produced over 30 PVGs based on its CPGs, and US Preventive Services Task Force has over 100 CPG patient versions available [4]. A variety of medical topics were covered in those PVGs, including cancer (breast, lung, prostate, oesophagal, pancreatic, and melanoma), women’s health and reproduction, gastrointestinal conditions, diabetes, and mental health.
Many factors may influence the interpretation and utilization of CPGs, including the clarity and performability of the recommendation, the rigour of systematic review methods, and the factors the guideline panel has considered in making recommendations [5]. It is possible for developers to incorrectly translate a recommendation from a CPG into a PVG when they are unclear about the rationale for the recommendations. Therefore, producing a helpful PVG is more than tailoring the language to patients and the public, though the word “translate” suggests using a different language. Developers need to consider: who needs to be involved in PVG development, how to select the recommendations to be included in the PVG, how to make sure the recommendations are translated into PVG correctly, what should be in a PVG, how to communicate the strength of a recommendation, and what makes a good PVG for patients. To facilitate the development of PVGs, the Guidelines International Network (GIN) published a manual in 2015 to guide in developing useful guideline-derived materials for the public and patients (hereafter called “GIN public guidance”) [1].
The concept of PVG was first introduced to China in approximately 2015, following GIN’s definition of PVG and GIN public guidance offered through an academic forum. The earliest known PVGs in China date back to 2016 as documented by Jiang et al. [6] and Li et al. [7]. As of February 20, 2022, a total of 26 PVGs (both ongoing and completed) have been identified in China [8]. Even though the number of PVGs is increasing, it remains relatively small compared with the number of CPGs developed in mainland China (over 100 CPGs every year) [9]. Because there is currently no commissioning organization for their development, but only a registration platform (http://www.guidelines-registry.cn/) available for both PVGs and CPGs. Therefore, developers typically take the lead in developing a PVG for a particular disease, with input from a multidisciplinary team of clinical experts and patient representatives to ensure accurate translation of recommendations from other CPGs [8].
The majority of PVG developers in China claim to have followed GIN’s public guidance when developing their PVGs [8]. However, despite citing GIN’s definition of PVG, most PVGs were not simply translations of existing CPGs into patient versions. Instead, they were adapted patient versions based on existing CPGs [6] or from de novo development (i.e., the creation of an entirely new PVG with its own set of research questions that are independent of existing CPGs) [10]. Moreover, the development processes described by different PVG teams vary greatly. For example, regarding the source recommendations, some PVG development teams adopted (without modifications) the source recommendations [11], and some adapted source recommendations with modifications. However, some PVG teams formulated new recommendations through consensus or voting, and the source recommendations are just for reference during this process [12]. Additionally, some teams integrated recommendations when there were two or more relevant recommendations based on their principles [6]. As to the content of PVGs, we found that some PVGs only educated patients on what to do [11], without any information to assist patients in making decisions, such as potential benefits and harms of the diagnoses, which looks like a general health education material.
Although the number of PVGs is increasing, research on the methodology of PVG development is also continuing [13,14,15,16], we are not aware of studies that consider the perspectives of developers regarding PVGs. So, we did the interviews to explore Chinese developers’ perceptions of PVG and experiences of developing PVGs, to inform further methodological guidance for PVG development. This qualitative study is one in a series of three that evaluate the state, perceived challenges, and solutions related to PVG development.
Methods
We applied a qualitative descriptive study design using semi-structured interviews. This manuscript follows the recommendations provided by the Standards for Reporting Qualitative Research [17]. We used the term “Patient versions of guidelines” to refer to guidelines produced for patients and the public.
Researchers’ characteristics
Two female PhD-level researchers (LJ and ZY) with experience in qualitative methods conducted the interviews and performed the primary analysis. The researchers are PhD students with experience in developing standard guidelines, and one researcher has participated in developing two PVGs [6, 11].
Participants
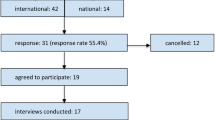
According to our scoping review of PVG in China [8], 26 PVGs developed by 16 teams could be identified. We tried to acquire the contact information of all PVG teams in China; however, many PVGs only have registration information (PVG title, organization, name of the person who submitted the registration) available, and we could only obtain the contact information of 11 teams who were responsible for 15 PVGs. We contacted all members by email or WeChat with an invitation letter. Next, we invited team members in different roles, including the lead persons of the PVG, methodologists, and external review experts. We conducted all interviews virtually between December 2021 and April 2022.
Data collection tool and process
We explored participants’ perceptions of PVG, experiences with current practice in PVG development and experiences with challenges in the PVG development process. Topics related to challenges encountered during the PVG development process were based on the development process identified in the scoping review of PVGs in China [8] and MC-PCG. Two investigators developed an initial draft of interview guide (LJ, JL) and discussed it with other research team members to obtain consensus and make amendments. Interview guide was pretested and subsequently adapted if necessary. We used the first two interviews as a pretest. The research team approved a final set of 16 questions (supplementary appendix 1). Characteristics of participants were collected before the interview. We audio-recorded each interview with participants’ permission.
Data analysis
The raw data were first recorded and then transcribed verbatim using the IFLYREC app (iFLYTEK CO.LTD, Version: 6.0.3171). The resulting transcripts were further reviewed and examinated by LJ. Two authors (LJ and ZY, ZY did not participate in the interviews) used conventional and directed content analysis approaches [18] to analyze the data. We began by reading each transcript from beginning to end, as one would read a novel. Then, we read each transcript carefully, highlighting text and writing a keyword or phrase that seemed to capture the perceptions and experiences of developing PVGs, using the participants’ words. As we worked through the transcript, we attempted to limit these developing codes as much as possible. After open coding of three to four transcripts, we decided on preliminary codes. Then, we coded the remaining transcripts (and recoded the original ones) using these codes and adding new codes when we encountered data that did not fit into an existing code. Once all transcripts had been coded, these codes were then grouped into subcategories and generic categories. Categories used for challenges arising from specific PVG development processes were informed by the scoping review of PVGs in China [8] and minimum criteria for the development process, content, and governance of PVGs (MC-PCG) [15]. We used NVivo (V.12 for Microsoft) for qualitative analysis. The final findings were further discussed by the research team (JP, JL, ZY, LJ) to achieve investigator triangulation and reach a consensus.
Ethics
Ethical approval was obtained from the Beijing University of Chinese Medicine for conducting this interview (Approval Number: 2022BZYLL0706). All participants received an introduction to this study in advance, written and verbal informed consent was obtained from all participants. All methods were carried out in accordance with the Declaration of Helsinki. The participants were made aware that they could withdraw from the study at any time, that their information would be kept confidential, and that they would remain anonymous in any publications. All participants were provided with a compensation of 600 RMB for their participation.
Results
Twelve developers from nine PVG teams participated in the individual interviews. Their demographics have been listed in Table 1. The interviews identified PVG developers’ understanding of PVGs, their current practice experience, and the challenges of developing PVGs. See Table 2.
Understanding of PVGs
The participants thought PVGs are the versions developed for patients, so PVGs should be based on patient’s needs, accessible, and understandable to patients. During the interview, participants expressed their views on the differences and connections between PVGs, general health education materials, clinical practice guidelines, and decision aids. The fundamental difference between PVG and CPG is the difference in audience. PVG should be developed based on the needs of patients, while CPG should be developed based on the needs of clinical medical staff. The difference between PVG and general health education material is that PVG is designed with a more rigorous method and provides recommendations. The difference with patient decision aids (PDAs) is that PDAs help patients make decisions. PVG developers thought it is not feasible to help patients make decisions by themselves; they developed PVG based on patient needs instead of PDA. See Table 3.
Current practice
Three models of PVG development
According to PVG developers, there are three models for PVG development. Model 1: PVG development based on one CPG, is a translation of a CPG that is in development, saves more time, and can facilitate doctor-patient communication and shared decision making. However, it does not perfectly address the concerns of patients and the public. Thus, this model is not adopted by many PVG developers. Most developers adopted Model 2, PVG development based on multiple CPGs, and Model 3, de novo development of PVGs.
The PVG developers explained that they had to refer to multiple existing CPGs or developing new PVGs from scratch because they discovered that the identified needs of patients, as revealed through clinical surveys and interviews, were not addressed in any single existing CPG. In short, the two models are derived from patients’ needs. In addition, developers who used the third model felt that although they can translate PVGs from existing CPGs, the quality and feasibility of the PVGs and whether the recommendations apply to the target population need to be considered. Developers think it is often difficult to find CPGs that meet these requirements, so they prefer the third model.
Participant A: I think the first scenario is that maybe this clinical practice guideline is almost completed, and then they did surveys and found that the patients also need some recommendations in this guideline, and I think this is the first model of PVG development which is based on a clinical practice guideline…And then, there is another situation where no single clinical practice guideline could address all patients’ questions. This is precisely what happened to us; there are no single clinical practice guidelines for stroke and physical dysfunction (but patients need them). And then, we need to do a synthesise of many guidelines. Those are the two models of PVG development.
Participant D: I think, for example, to translate the guideline I developed into the patient version. I feel that it doesn’t work; why not? Because the questions that patients raised are not necessarily included in the guideline. It’s not necessarily the questions that the clinical practice guidelines will address. For example, our clinical practice guidelines mentioned glycosylated haemoglobin-related questions and recommendations, but none of our patients asked these questions in the interviews.
Application of existing methods for PVG Development
Participants reported that they developed PVG following GIN Public guidance and MC-PCGs. However, they found that the existing methodological guidance for PVG development did not guide model 2, PVG development based on multiple PVGs, and Model 3, de novo development of PVGs. So they integrated other related guidance such as evidence synthesis methodology to deal with a recommendation from different CPGs, guideline adaptations guideline to deal with recommendations from another context, and the WHO handbook [19] to guide the de novo development. However, none followed exclusively one methodology because each methodology has limitations. Therefore, they compensate for their shortcomings by integrating or adopting multiple methodologies. Following is the inapplicability of GIN Public guidance, MC-PCGs, and the WHO handbook described by participants (Table 4).
Challenges for developing PVGs
We identified three challenges for developing PVGs: (1) the lack of standardized and native methodology to develop PVGs; (2) challenges in patient engagement; (3) other challenges: the lack of publicly known platform to disseminate PVGs, conflicts of interest and resources required for developing PVGs.
The lack of standardized and native methodology to develop PVGs
The most commonly perceived obstacle to developing PVGs was the lack of a standardized and native method. Participants indicated that although there are some methodological guidelines for PVG development, the existing methodological guidelines do not provide comprehensive guidance and are not entirely applicable, as detailed in Table 2. The lack of standardized and native methodology has made them unsure if they are doing PVG development correctly or under which situations it would be best suited. Some of them have even omitted some crucial steps for PVG development, such as “understanding patient needs”, due to the lack of standardized and native methodological guidelines.
Participant G: Sometimes, if you are given the rules and requirements and straightforward advice, you do it with less effort. When you do it according to the standards and requirements, you will have more confidence in it (the PVG you produced).
Participant H: There is no standard, and then I am not sure if this is the right way or not, so I am just feeling my way.
Given the limitation of existing guidance and lack of standardized and native methods to develop PVGs, there were many challenges arising from a specific development process, including (1) team; (2) identifying patient needs; (3) evidence retrieval, evidence synthesis and forming recommendations; (4) the content and format of PVG; (5) test of PVG; and (6) dissemination. See supplementary appendix 2 for detail.
Team (Contributors and their role in PVG development): Challenges encountered by participants during the process of the team, is the lack of standards for team composition (what roles are needed, the number of people for each role, qualifications for each role) and limited capabilities for PVG development.
Participants commented that GIN Public guidance and MC-PCGs only mention the need to include patients, editors and source CPG developers, but do not specify whether other roles, such as methodologists, should be included in PVG development, especially when the source CPG developers cannot be included. Thus, PVG developers feel unsure if they had a good team composition for developing a qualified PVG. According to participants’ views and experiences, the team requirements for PVG development are almost the same as CPG development, including the methodologists, clinical professionals, and patient representatives. However, PVG needs more patients and editors with experience in writing to individuals who are not in healthcare.
In addition, some perceived their limited capabilities for PVG development as a big challenge for them. Participant G indicated:
“Due to our professional scope is limited, we also have limited ability (to develop PVGs), we actually believe if there are more excellent teams or individuals joining us here, more authoritative, and more experienced experts to join in, it will be better.”
Identifying patients’ needs: Firstly, there is no guidance for identifying what types of patients’ needs. Participants were confused about whether they should identify the topics that patients want to address before CPG selection, or just identify information that patients need to help them understand and implement the recommendations after CPG selection. On the one hand, some participants think that it is necessary for PVG developers to identify the topics that patients want to address before CPG selection, because “we are not sure if patients will be interested in those questions addressed in the CPGs, or if there are some questions that patients care about but are not included in our CPGs (Participant C).” On the other hand, doing this will likely result in some topics that are not included in the existing CPGs and require a de novo development of PVG; while de novo development needs more resources and a higher requirement for the team.
Secondly, the conflict between limited resources and identifying patients’ needs from different backgrounds is also a challenge encountered. Participants indicated the patients to be surveyed should be from different backgrounds (clinical, community, or family) because heterogeneity in patients will probably capture the whole picture of patients’ needs. However, this requires more resources and is time intensive.
Evidence retrieval, evidence synthesis, and forming recommendations: Firstly, framing the right questions is challenging, because they found patient’s concerned questions were too broad (for example from participant H, Can I use Traditional Chinese medicine to treat my stroke) or too specific (for example from participant D, diabetic patients should drink skim milk or low-fat milk?), which left them confused about how to frame the question, to facilitate the evidence retrieval.
Secondly, lack of evidence was perceived as an important obstacle, many questions that patients raise are likely to be of lesser concern to researchers, resulting in a lack of evidence in this area. Regardless, patients might not value evidence; they just want answers which could help them to know what they could do for themselves. There is a lack of guidance to support developers to balance the challenges of patients’ needs and a lack of evidence when producing PVGs.
Thirdly, no framework to guide PVG development groups to make judgments on recommendations from different source CPGs which are developed by other organizations. PVG developers are not clear how to address context differences between source CPGs and PVGs; or how to address inconsistency and integrate recommendations from different source CPGs.
Finally, due to the lack of standards for making the decision between a comprehensive search and a targeted search for CPGs, participants are unclear about whether they should conduct a comprehensive search for all relevant CPG to answer patients’ questions when they already have found one relevant and high-quality CPG.
Contents and format: The challenges arise from the process of drafting the PVG including the disparity in patients’ educational levels, the conflict between the function of PVG in aiding patients’ decision making and the understandability of PVG, as well as big differences between different patients’ need and their reading preferences.
PVG developers found that preferences for the content and format for people at different educational levels varied greatly, with some preferring only text and others preferring graphics, leaving them confused about which educational level they should present the PVG for.
In addition, participants were often faced with challenges in translating evidence into clear messaging that can be understood by patients. On the one hand, PVGs must include sufficient information regarding the evidence to aid patients in their decision-making; and, on the other hand, they must ensure that the recommendations can be easily interpreted by patients.
No framework to guide the presentation of recommendations was also mentioned by the participants. Participants were unsure whether and in what situation they should present the following information in a recommendation, including the quality of the evidence, recommendation level, the rationale for the recommendation, and other supported background information.
In order to help patients’ self-management after reading PVG, participants believed they should include more self-management information beyond recommendations. Consequently, the content of a PVG may be very lengthy, while lengthy information will make patients lose interest in reading. Thus, PVG developers are unclear about how much information should be presented.
Test and evaluation: To ensure the quality of PVGs, participants test and evaluate them before they are finalized, which are called external reviews by participants. Due to the lack of a standard PVG evaluation tool, to define a good PVG, participants don’t know what aspects they should ask external reviewers to give advice and suggestions, and who should be involved in the external review. According to participants’ views and experiences, PVGs should be tested and evaluated from multiple perspectives; for example, they used AGREE 2 to evaluate the recommendations, and some presented the source recommendations, with the translated recommendations to experts for assessing the accuracy of the translation, some assessed the understandability using a health education evaluation tool by DECERN, some evaluated its feasibility, appropriateness, meaningfulness, and effectiveness based on FAME framework.
Challenges in patient engagement
Lack of standard methodological guidance on how patients should be involved in the development of PVG: participants stated there is a lack of methodological guidance on patient engagement in PVG development. They were confused about when to involve patients; how many patients should be included; and how to include representative patients. They called for methodological guidance which can provide methods and skills to facilitate patients’ engagement. See Appendix Table 1 for detail.
When to involve patients: They were confused about whether patients should be involved in the whole development process or only some particular stages of the process.
Participate A: Which development process would be better for patients and editors to be involved in PVG development? Should they be involved in the whole development process, but can this really make a difference? Because they (patients) may not have as much time as we do, so we can’t invite them every time.
How to include representative patients.
Participate C: because we look for some patients in the hospital, of course, we need to find some patients, and parents who are more cooperative, because parents of low cooperation will not participate. Then, we did find some of the parents with a high degree of cooperation, however, they are less likely to say, less likely to raise different voices, they are less likely to tell us there are problems existing in our PVG.
Patients’ lack of knowledge of PVGs: patients’ lack of knowledge of PVG was perceived as a barrier to their engagement in PVG development. They couldn’t express their needs and different opinions regarding PVG, as they don’t know what the PVG is for, or what it should be.
Other challenges
In addition to the above challenges, a number of other challenges were expressed by participants. There is no publicly known and trusted platform that could disseminate PVGs; or resources required for developing PVGs. Some participants also expressed their concerns about the conflicting interests related issues; for example, some health providers think the PVG may hinder patients’ compliance with the treatment regimen they provided after reading the PVG, if the PVG recommended different treatment, or if patients interpret the recommendations in the PVG differently (Participate G).
Discussion and conclusion
Discussion
PVGs are essential for supporting patient decision-making and facilitating SDM. In this study, twelve PVG developers from nine teams in China were interviewed. Our study summarizes the perceptions and experience of PVG developers, which includes their understanding of PVG, their experience of PVG development, and the challenges that arose during development.
A key finding emerging from the interviews is developers’ misunderstanding of PVG, which are supposed to be translated versions of CPGs. However, interviewees believe that PVGs are guidelines for patients, with the emphasis on guidelines “for patients”, which can be a translated version of CPGs, or an adapted, or de novo developed patient version of guidelines based on patient needs. This finding is also evidenced by the existing introduction literature to the PVG [20], which references GIN’s definition of the PVG, but translates it into “PVG refers to the guidelines for patients, which are developed under the guidance of evidence-based medicine philosophy, centered on the health issues of patient concern and based on the best available evidence”. Almost all of these interviewees share the same understanding of PVG, and therefore, they pointed out that there could be three models for the development of PVG: Model 1, PVG development based on one CPG (with translation) as GIN pointed out; Model 2, PVG development based on multiple CPGs (with adaptation); and Model 3, de novo development of PVGs. It was due to a misunderstanding of the concept of PVGs that developers found many inadequacies and confusion associated with the development of PVGs when they followed the GIN public guidance. Therefore, clarifying the concept of PVG on the basis of a correct translation is the primary task for us to develop PVGs and carry out related research.
PVG developers indicated the role of PVG in educating patients, and in providing recommendations. Still, none indicated the role of PVG in aiding decision-making due to PVG developers’ low awareness of the necessity for patients to make their clinical decisions. This explains why some PVGs only educated patients on what to do, without any information to assist patients in making decisions. However, recommendations in the CPGs only involve the CPG development group’s value judgments, which may be not appropriate for individual patients. PVGs must convey this idea to both healthcare professionals and patients and provide information to facilitate the decision-making process [21]. In addition, according to the conceptual framework for patient-directed knowledge tools developed by Dreesens et al. 2019 [14], the purpose of PVG is not only to inform or educate and provide recommendation(s) but also to support decision-making. Thus, it is important to raise PVG developers’ awareness of PVG’s role in aiding decision-making.
To this day, few studies explored the challenges that arose during PVG development. Only SIGN has identified the challenges for PVG development from the perspective of PVG users, including the challenge to provide sufficient information while avoiding information overload, a lack of consensus on the usefulness of rating the strength of evidence and recommendations [22, 23]. But no studies looked at the challenges from the perspective of PVG developers. Our study identified the following challenges:
First, participants reported there is a lack of standard methods to develop PVGs, resulting in challenges arising from the specific development process, such as no framework to define a good PVG; no framework to guide the presentation of recommendations for patients; no explicit methodology on PVG development initiated by PVG developers who are not involved in the CPG development. Moreover, the existing PVG development guidance is developed in a different context (MC-PCGs are developed in the Netherlands), and published in English, which may cause difficulty in understanding, such as “Personalization of PVG recommended in GIN Public guidance” is difficult to understand for non-native English PVG developers, as stated by interviewer G. Therefore, native consensus-based guidance considers the perspectives of developers is needed.
Second, the challenges in patient engagement: participants stated they were unclear about whom to include as the representative patients, how many to have, at what stage in the development process to include them, or how best to include them, and it is difficult for patients to voice different opinions and express their needs as they expected. Those challenges are also encountered by CPG developers. However, CPG developers worldwide, including GIN, Canadian Task Force on Preventive Health Care (CTFPHC) [24], Scottish Intercollegiate Guidelines Network [25], and National Institute for Health and Care Excellence [26], have provided strategies to involve patients and the public in the guideline (or PVG) development. For example, GIN recommends that it is desirable to collaborate with the patient during the whole development process of the PVG. Still, it is more feasible to include patients in the planning and consultation stages. In addition, Ainsley Moore et al. 2021 developed a 12-item Patient Engagement Evaluation Tool (PEET) to inform guideline developers about the quality of patient and public involvement activities [27]. Therefore, PVG developers could refer to existed guidance or tools on patient engagement.
Third, a number of other challenges were expressed by the participants during the development. There is no publicly known and trusted platform like National Health Care Institute in the Netherlands that could disseminate PVGs. Therefore, we identified many PVGs were published in the professional database and patients had no access to them. Concern of conflicting interests with health professionals is also a challenge for PVG developers. Actually, this concern is also raised by patients [24]. However, this issue has not been addressed in the literature. Therefore, we suggest PVG providers should pay attention to this issue and could have feedback from health providers regarding this when they finalized the PVG.
Strength and limitations
This is the first study to explore PVG developers’ perception of PVGs, and the challenges they have encountered during the PVG development process. While the data set is highly novel, the sample size was modest. Future investigation of the findings discussed herein with larger samples would be valuable. This study only included PVG developers from China, the conclusions drawn from the interviews do not necessarily compare to the viewpoint of PVG developers from other countries. In addition, we did not include role members such as patient representatives and editors in the PVG team. This makes the results of this study missing some of the experiences and perceptions from their perspective. However, this study primarily hopes to identify the methodological challenges of PVG developers during PVG development. Thus, this does not have a significant impact on the results of this study.
Conclusions
Our study identified that all PVG developers ignored the roles of PVGs in helping patients’ decision-making, and have a misunderstanding of PVG, which might be a reason why the interviewees stated that they used one of three models for the development of PVGs instead of following the GIN recommendation. Thus, a sound Chinese translation of the GIN material is urgently needed so that this misunderstanding can be avoided. Moreover, PVG developers encountered many challenges arising from the specific development process, as the existing PVG development guidance only focuses on providing guidance to source CPG developers. Therefore, a comprehensive and pragmatic PVG development method to standardize PVG development is warranted. Moreover, PVG developers also call for a publicly known and trusted platform that could disseminate PVGs in China.
Implications
There is a need to make PVG developers realize the roles of PVGs, especially in helping decision-making, to maximize the effect of PVG. Firstly, providing continuing education programs to assist PVG developers in understanding the essentials of PVG is key to promoting the development of high-quality PVGs. Secondly, the benefits of SDM must continually be emphasized, and a positive attitude towards SDM must be promoted. A sound Chinese translation of the GIN material is urgently needed to avoid the misunderstanding of PVG. It is necessary to develop native consensus-based guidance considering the perspectives of PVG developers regarding PVGs.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- GIN:
-
Guidelines International Network
- CPG:
-
Clinical practice guidelines
- PVG:
-
Patient versions of the guideline
- MC-PCG:
-
Minimum criteria for the development process, content, and governance of PVGs
- NICE:
-
National Institute for Health and Care Excellence
- SIGN:
-
Scottish Intercollegiate Guidelines Network
References
Karen G, Corinna S, Nancy S. How to develop information from guidelines for patients and the public. 2021. In: GIN PUBLIC toolkit [Internet]. Available from: https://g-i-n.net/wp-content/uploads/2022/01/Toolkit-combined.pdf. Accessed 20 Dec. 2022
van der Weijden T, Pieterse AH, Koelewijn-van Loon MS, Knaapen L, Légaré F, Boivin A, et al. How can clinical practice guidelines be adapted to facilitate shared decision making? A qualitative key-informant study. BMJ Qual Saf. 2013;22(10):855–63.
SIGN. Patient Publications. Available from: https://www.sign.ac.uk/patient-and-public-involvement/patient-publications/. Accessed 20 Dec. 2022
US Preventive Services Task Force. Information for consumers. Available from: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation-topics/information-for-consumers?SORT=T&PAGE=7. Accessed 17 Jan. 2022
Brignardello-Petersen R, Carrasco-Labra A, Guyatt GH. How to interpret and use a clinical Practice Guideline or recommendation: users’ Guides to the Medical Literature. JAMA. 2021;326(15):1516–23.
Jiang Y, Tian R, Duan S, Yan L, Han L, Wang J, et al. Thoughts on creating guidelines for high risk of Diabetic Foot Ulcer patients. Chin Nurs Manage. 2016;16(12):1628–32.
Li Y, Chen Y, Chen J, Shang H, Yang K, Guo G, et al. Guideline Protocol of Non-Pharmacological secondary Prevention for myocardial infarction. Chin J Evidence-Based Med. 2016;16(5):617–20.
Yan LJ, Li SA, Jin XJ, Yang D, Scott SE, Wang ZJ, et al. Development of patient versions of guidelines in chinese mainland: a systematic survey of current practices and methods. Patient Educ Couns. 2022;105(12):3410–21.
Chen Y, Wang C, Shang H, Yang K, Norris SL. Clinical practice guidelines in China. BMJ. 2018;360:j5158.
Liu H, Wang H, Liu Y, Yang N, Wu S, Liu X, et al. Protocol for the development of guideline for the management of foreign bodies in the digestive tract of children in China (patients and public version,2022). Chin J Practical Pediatr. 2022;37(2):81–7.
Wang R, Zhu S, Zhou L, Cai J, Yan L, Jiang Y. Construction of patient version of guidelines for secondary prevention of ischemic stroke. Chin Nurs Res. 2021;35(24):4351–7.
Zhou Y, Huang N, Li L, Pan X, Zhao X, Zhao M. A protocol of guideline for patient involvement in non-pharmacological management for gestational diabetes mellitus. Chin Nurs Res. 2021;35(15):2749–52.
Santesso N, Morgano GP, Jack SM, Haynes RB, Hill S, Treweek S, et al. Dissemination of clinical practice guidelines: a content analysis of patient versions. Med Decis Making. 2016;36(6):692–702.
Dreesens D, Stiggelbout A, Agoritsas T, Elwyn G, Flottorp S, Grimshaw J, et al. A conceptual framework for patient-directed knowledge tools to support patient-centred care: results from an evidence-informed consensus meeting. Patient Educ Couns. 2019;102(10):1898–904.
van der Weijden T, Dreesens D, Faber MJ, Bos N, Drenthen T, Maas I, et al. Developing quality criteria for patient-directed knowledge tools related to clinical practice guidelines. A development and consensus study. Health Expect. 2019;22(2):201–8.
Loudon K, Santesso N, Callaghan M, Thornton J, Harbour J, Graham K, et al. Patient and public attitudes to and awareness of clinical practice guidelines: a systematic review with thematic and narrative syntheses. BMC Health Serv Res. 2014;14:321.
O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–51.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
WHO. WHO handbook for guideline development: World Health Organization. 2014. Available from: https://apps.who.int/iris/handle/10665/145714. Accessed 20 Dec. 2022
Xiao S-j, Gao Y-t, Wang X, Wang D-k, Zhou Q, Chen Y. Introduction of patient versions of guidelines and its development methods. Drug Evaluation. 2017;14(6):44–8.
Karen Graham S, Treweek NS, Schaefer C. Chapter 7: how to develop patient versions of guidelines (updated 2015). In: G-I-N public toolkit: patient and public involvement in guidelines [Internet]. Guidelines International Network (G-I-N), [cited 2021.10.12]. 2015. Available from: https://g-i-n.net/get-involved/resources/. Accessed 12 Oct. 2021
Fearns N, Walker L, Graham K, Gibb N, Service D. User testing of a scottish intercollegiate Guideline Network public guideline for the parents of children with autism. BMC Health Serv Res. 2022;22(1):77.
Fearns N, Graham K, Johnston G, Service D. Improving the user experience of patient versions of clinical guidelines: user testing of a scottish intercollegiate Guideline Network (SIGN) patient version. BMC Health Serv Res. 2016;16:37.
Julian S, Rashid A, Baker R, Szczepura A, Habiba M. Attitudes of women with menstrual disorders to the use of clinical guidelines in their care. Fam Pract. 2010;27(2):205–11.
SIGN. SIGN patient and public involvement. Available from: https://www.sign.ac.uk/patient-and-public-involvement. Accessed 1 Oct. 2022
NICE. NICE guidance. Available from: https://www.nice.org.uk/guidance. Accessed 10 Dec. 2022
Moore A, Wu Y, Kwakkenbos L, Silveira K, Straus S, Brouwers M, et al. The patient engagement evaluation tool was valid for clinical practice guideline development. J Clin Epidemiol. 2022;143:61–72.
Acknowledgements
The authors would like to thank Xiao-qin Wang from McMaster University for her assistance with recruitment for this study.
Funding
This study is supported by the National Natural Science Foundation project (No. 81830115).
Author information
Authors and Affiliations
Contributions
All authors have made substantive contributions to the development of this manuscript; LJY and JPL come up with the research question and conceptualized the research approach. LJY, JPL and JLH designed the protocol. LJY and ZYY did the interview. LJY, ZYY, and JLH were responsible for the coding. LJY, CS, JLH drafted the manuscript. SES, KG, SAL, XJJ and JPL were involved in critically revising the manuscript. JPL acquired the financial support for the project leading to this publication. The authors achieved investigator triangulation and reach consensus on the findings, and all have agreed on the final version.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All experimental protocols were approved by ethics committee of Beijing University of Chinese Medicine (Approval Number: 2022BZYLL0706). Written and verbal informed consent was obtained from all participants. All methods were carried out in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Karen Graham and Sarah E. Scott are authors of GIN Public Toolkit, which is cited in this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yan, L., Hu, J., Yu, Z. et al. The perceptions and experience of developing patient (version of) guidelines: a descriptive qualitative study with Chinese guideline developers. BMC Health Serv Res 23, 789 (2023). https://doi.org/10.1186/s12913-023-09591-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09591-5