
Abstract
Background
Data remain scarce on the costs of HIV services for key populations (KPs). The objective of this study was to bridge this gap in the literature by estimating the unit costs of HIV services delivered to KPs in the LINKAGES program in Kenya and Malawi. We estimated the mean total unit costs of seven clinical services: post-exposure prophylaxis (PEP), pre-exposure prophylaxis (PrEP), HIV testing services (HTS), antiretroviral therapy (ART), sexually transmitted infection (STI) services, sexual and reproductive health (SRH) services, and management of sexual violence (MSV). These costs take into account the costs of non-clinical services delivered alongside clinical services and the pre-service and above-service program management integral to the LINKAGES program.
Methods
Data were collected at all implementation levels of the LINKAGES program including 30 drop-in-centers (DICs) in Kenya and 15 in Malawi. This study was conducted from the provider’s perspective. We estimated economic costs for FY 2019 and cost estimates include start-up costs. Start-up and capital costs were annualized using a discount rate of 3%. We used a combination of top-down and bottom-up costing approaches. Top-down methods were used to estimate the costs of headquarters, country offices, and implementing partners. Bottom-up micro-costing methods were used to measure the quantities and prices of inputs used to produce services in DICs. Volume-weighted mean unit costs were calculated for each clinical service. Costs are presented in 2019 United States dollars (US$).
Results
The mean total unit costs per service ranged from US$18 (95% CI: 16, 21) for STI services to US$635 (95% CI: 484, 785) for PrEP in Kenya and from US$41 (95% CI: 37, 44) for STI services to US$1,240 (95% CI 1156, 1324) for MSV in Malawi. Clinical costs accounted for between 21 and 59% of total mean unit costs in Kenya, and between 25 and 38% in Malawi. Indirect costs—including start-up activities, the costs of KP interventions implemented alongside clinical services, and program management and data monitoring—made up the remaining costs incurred.
Conclusions
A better understanding of the cost of HIV services is highly relevant for budgeting and planning purposes and for optimizing HIV services. When considering all service delivery costs of a comprehensive HIV service package for KPs, costs of services can be significantly higher than when considering direct clinical service costs alone. These estimates can inform investment cases, strategic plans and other budgeting exercises.
Similar content being viewed by others


Background
Together with their partners, key populations (KPs) at higher risk of HIV infection—including men who have sex with men (MSM), sex workers (SW), people who inject drugs (PWID), and transgender women (TGW)—are estimated to comprise 65% of new HIV infections globally [1]. In sub-Saharan Africa, new infections among KPs and their partners make up 72% of new HIV infections in West and Central Africa and 32% in Southern and Eastern Africa and there is growing concern that as HIV epidemics in the general population are better controlled, the relative importance of KPs will increase [1,2,3]. Forty years since the first cases of AIDS were reported, KPs continue to be marginalized and criminalized in many countries, HIV prevention services for KPs continue to be inaccessible to many, and providing HIV testing and treatment services to KPs living with HIV remains a challenge even in countries with high performing HIV programs [1]. To achieve HIV epidemic control, countries around the world, including in sub-Saharan Africa, will need to significantly scale up effective HIV services for KPs [2,3,4].
Global guidance on HIV services for KPs describes a package of clinical services—many of which are the same services as for the general population [5]. However, effective HIV services for KPs differ in important ways from HIV services for general populations. To address the challenges and barriers often faced by KPs, clinical services for KPs need to be implemented interdependently with structural interventions that address stigma, discrimination, and violence [6,7,8]. In addition, besides service-level activities, effective KP HIV services also comprise important efforts below- and above-service level [9,10,11]. KPs often require substantial outreach conducted by peers in the community to facilitate service utilization and retention in care [12,13,14]. Effective KP programs include differentiated service delivery models and community-based and community-led approaches to service delivery [5, 15]. Likewise, community organization staff and volunteers often need substantial support, including program management support, technical assistance, training, and oversight. Moreover, pre-service delivery activities, including population mapping and size estimation, are integral to the effective delivery of KP HIV services [16,17,18]. Critically, these non-clinical features are viewed as core elements of comprehensive HIV services for KPs and not as optional extras [4].
To scale up HIV services for KPs, additional resources will need to be allocated to these services. To date, KP HIV services globally have been significantly under-funded with expenditures on KP HIV services much lower than would be expected given the burden of HIV among KPs [19, 20] and representing only a fraction of estimated resource needs [21]. Developing investment cases for additional resources and allocating available resources efficiently across HIV services requires accurate and timely information on the costs of HIV services. Though there is a growing literature on the costs of HIV services for general populations in low- and middle-income countries, data remain scarce on the costs of HIV services for KPs and these mostly focus on the delivery of clinical services alone [22]. We are aware of only one costing study of a KP HIV program that considered the costs of clinical and non-clinical service elements, including interventions required to reach and engage KPs and project management [10].
The objective of this study was to bridge this gap in the literature by estimating the unit costs of the HIV services delivered to KPs in the Linkages Across the Continuum of HIV Services for Key Populations Affected by HIV (LINKAGES) program in Kenya and Malawi. LINKAGES was led by FHI 360 and funded by the United States President’s Emergency Plan for AIDS Relief (PEPFAR) from 2014 to 2021. Implemented in over 30 countries in Africa, Asia, and the Caribbean, the program provided a comprehensive package of services to KPs with the goal of reducing HIV transmission among KPs and their sexual partners and improving KP enrollment and retention in HIV treatment services. We estimated the unit costs of the following clinical HIV services delivered to KPs as part of LINKAGES in Kenya and Malawi: post-exposure prophylaxis (PEP), pre-exposure prophylaxis (PrEP), HIV testing services (HTS), antiretroviral therapy (ART), sexually transmitted infection (STI) services, sexual and reproductive health (SRH) services, and management of sexual violence (MSV). Our unit cost estimates also reflect the cost of non-clinical services delivered alongside these clinical services (peer outreach, structural interventions that address stigma, discrimination, and violence, KP empowerment) and the pre-service (KP mapping and size estimation) and above-service program management and data monitoring that was an integral part of the LINKAGES program.
Methods
Study setting
Kenya and Malawi have generalized HIV epidemics with concentrated sub-epidemics among KPs [23]. In 2021, HIV prevalence in 15–49-year-old adults was estimated to be 4% in Kenya [24] and 7.7% in Malawi [25]. Recent HIV prevalence data for FSW and MSM in Kenya are not available [24]. In Malawi, the latest HIV prevalence for FSW and MSM was estimated to be 49.9% and 12.9% [25]. KPs face important structural barriers in both countries that impact their vulnerability to HIV infection and impede their access to health services [26]. A recent cross-country analysis of law, criminalization, and HIV describes sex work as criminalized in both countries and same-sex sexual acts as criminalized in Kenya and partially criminalized in Malawi [26].
Program description
In each country, operationalization of LINKAGES involved an initial start-up phase with pre-service delivery activities. Subsequently, a comprehensive package of KP HIV services was scaled up with activities executed at multiple implementation levels (Figure S1). LINKAGES program headquarters provided overall program guidance and technical assistance. LINKAGES country offices provided on-the-ground program management and technical support. Local community-based organizations, including KP-led organizations, referred to as implementing partners (IPs) delivered HIV services to KPs. Services were delivered in communities through outreach activities and at drop-in centers (DICs)—sites where KPs received HIV services, met with peers, and conducted social and community mobilization activities.
The LINKAGES program included the following core program areas based on global guidance [5, 27,28,29,30]: 1) engage KPs in population size estimation, mapping, and program planning; 2) KP empowerment and engagement; 3) structural interventions; 4) peer outreach; 5) clinical services including PEP, PrEP, HTS, ART, STI services, SRH services, MSV, and condom and lubricant promotion and distribution; 6) program management; and 7) monitoring and data use. These core program areas were subdivided into program elements, spelling out the interventions carried out (Figure S2). All programmatic work and technical assistance were organized along these program areas and elements.
Study sample
Our study sample corresponded to the multi-level LINKAGES program implementation structure and included 30 DICs in Kenya and 15 DICs in Malawi; 18 IPs in Kenya and two IPs in Malawi; two LINKAGES country offices (one per country); and LINKAGES program headquarters. Of the 30 DICs in Kenya, 11 DICs provided services to FSW only, three to MSW only, two to MSM only, and 14 DICs provided services to FSW, MSW, and MSM. Of the 15 DICs in Malawi, 11 DICs provided services to FSW and four to MSM and TGW. In Kenya, we included all IPs and DICs that were part of the LINKAGES program in FY 2019. In Malawi, one IP was excluded (along with its four DICs).
Data collection
This costing study was implemented following the Global Health Cost Consortium guidelines [31]. We developed costing frameworks for each country to capture the LINKAGES program activities at all implementation levels. Our frameworks mapped activities and associated inputs and outputs to the seven program areas mentioned above. Costing frameworks were developed for the start-up years (FY 2015 and FY 2016 for Malawi and FY 2016 for Kenya) and for FY 2019. Based on these costing frameworks, we developed standardized Excel-based tools to collect information comparable across implementation levels in the two countries. Data were collected retrospectively for the start-up years and prospectively for FY 2019. Cost data were obtained from financial reports, payroll records, program manager reports, facility consumption data reports, program expense files, and asset registers. Additional data from headquarters and country offices were extracted from expenditure records provided by LINKAGES program headquarters. We collected monthly data on quantities and prices for seven input categories: staff, clinical supplies, utilities and operations, transportation, equipment, training, and external services (Table S1). Corresponding output data were obtained from databases in IPs and DICs including number of people treated with PEP, number of people on PrEP, number of people tested for HIV, number of people on ART, number of people screened for STIs, number of people provided a contraceptive method, and number of people provided post-gender-based violence care. For each staff member in country offices, IPs, and DICs, we collected estimates of the proportion of time spent on each of the seven program areas and on each of the clinical services through questionnaires.
Costing approach
This costing study was conducted from the provider’s perspective (i.e., the LINKAGES program). We estimated economic costs, which include the value of all resources used in the program, including those for which there was no financial transaction, such as donated goods. Annual costs were estimated with service delivery costs calculated for U.S. Government (USG) fiscal year (FY) 2019 (October 1, 2018 to September 30, 2019). Our cost estimates also include start-up costs incurred prior to service delivery. Start-up and capital costs were annualized using a discount rate of 3% and capital goods were assumed to have a useful life of 10 years [31]. We used a combination of top-down and bottom-up costing approaches to estimate unit costs of clinical HIV services delivered to KPs [10, 32]. Top-down methods were used to estimate headquarters, country office, and IP costs and allocate them to DICs. Bottom-up methods were used to measure the quantities and prices of all inputs used to produce services in DICs. We allocated all DIC-level costs to estimate site-level costs of clinical services (PEP, PrEP, HTS, ART, STI services, SRH services, MSV, and condom and lubricant promotion and distribution). All costs are presented in 2019 US dollars (US$). Country costs for FY 2019 were converted from local currencies to US$ using mid-year exchange rates for 2019 (Kenya: 102.01 Kenyan shillings and Malawi: 739.46 Malawian kwacha).
Further details on the methods and allocation weights used to distribute above-service level (headquarters, country office, IP) and start-up costs to DICs can be found in Table S2. In summary, headquarters and country office costs for FY2019 were distributed equally across DICs. Start-up costs were annualized over ten years using a 3% discount rate and the FY 2019 allocation of start-up costs was distributed equally across DICs. For the 13 IPs with only one DIC, IP costs were allocated to the corresponding DIC. For the seven IPs with multiple DICs, the allocation approach used was a function of the input: IP costs of staff, recurrent inputs, and equipment were allocated proportionally across DICs; transportation and training costs, which were available only at the IP level, were distributed across DICs based on DIC staff time weights. We used bottom-up methods to estimate the DIC costs of clinical supplies, staff, peer workers, other recurrent inputs, and equipment, multiplying the number of inputs used with input prices. Total LINKAGES program costs per DIC were obtained by aggregating above-service level allocations to DICs with DIC-level costs.
We used the following approach to estimate the unit cost of PEP, PrEP, HTS, ART, STI, SRH, and MSV services from these DIC-specific total LINKAGES program costs (Table S3). We separated costs into direct and indirect input costs. Direct input costs included the costs of clinical staff and peer workers and the costs of clinical supplies. Costs of clinical staff and peer workers were allocated to each clinical service based on the time allocation they reported. Similarly, clinical supplies were allocated to each clinical service based on resource use. For all indirect inputs shared across services (non-clinical staff, utilities, external services, equipment, training, transportation, headquarters, country office, and start-up), we weighted input costs using allocation weights derived by combining the annual number of clients per service over the total annual number of clients in the DIC and the proportion of staff and peer worker time dedicated to each service (Table S3). The proportion of clinical services provided in each DIC was used to distribute the costs of condom and lubricant promotion and distribution to the other clinical services provided, as no output data were available for this clinical service. We present volume-weighted mean unit costs for each service, which were calculated as the sum of total service costs across all DICs in a country divided by the sum of service outputs across all DICs in the country [33].
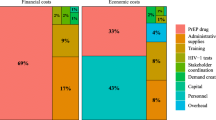
Given the centrality of the program areas to the LINKAGES program, we also assessed the breakdown of the overall unit costs of PEP, PrEP, HTS, ART, STI, SRH, and MSV services across the LINKAGES program areas: 1) engage KPs in population size estimation, mapping, and program planning; 2) KP empowerment and engagement; 3) structural interventions; 4) peer outreach; 5) clinical services; 6) program management; and 7) monitoring and data use. As described in more detail in Table S4, we separated inputs into two categories: those for which the program area was identified in the data collection tool (clinical and non-clinical staff, peer workers, clinical supplies, transportation, and training) and those for which the program area was unspecified (utilities, external services, equipment, headquarters, country office, and start-up). Unspecified inputs were allocated according to program area staff time weights (Table S4). Average country-level program area staff time weights were then used to distribute the unit costs per service across LINKAGES program areas.
We bootstrapped all unit costs reported 100 times to estimate standard errors and calculate 95% confidence intervals.
Results
Table 1 shows the number of clinical services provided in DICs in Kenya and Malawi during FY 2019. All clinical services were delivered in both countries except for PEP, which was only provided in Kenya. Though most DICs in Kenya provided PrEP, only three DICs in Malawi did so. In both countries, only DICs serving FSW delivered SRH services. Almost all DICs in both countries provided HTS, ART, STI, and MSV services. The vast majority of services delivered in both countries were STI services and HTS. In Kenya, STI screenings and HIV tests each comprised 46% of all services DICs delivered by DICs. In Malawi, STI screenings and HIV tests made up 73% and 17% of all services provided. The number of services and visits for each clinical service varied substantially by DIC in both countries. Facilities in Kenya tended to have significantly more clients than those in Malawi for all services except SRH services.
The volume-weighted mean unit costs for the clinical services implemented in Kenya and Malawi are shown in Table 2. For each service, Table 2 also shows the breakdown of the mean total unit cost into the following components: direct clinical service costs, condom and lubricant promotion and distribution costs, and indirect costs. Given the small number of outputs, we did not calculate the unit cost for PrEP in Malawi. When looking at the overall unit cost, the mean unit cost per clinical service ranged from US$18 (95% CI: 16, 21) for STI services to US$635 (95% CI: 484, 785) for PrEP in Kenya and from US$41 (95% CI: 37, 44) for STI services to US$1,240 (95% CI 1156, 1324) for MSV in Malawi. Considering the direct clinical service unit cost, the mean unit cost per clinical service ranged from US$2 (95% CI: 2, 3) for STI to US$162 (95% CI: 125, 198) for ART in Kenya and from US$9 (95% CI: 7, 10) for STI services to US$362 (95% CI: 242, 367) for MSV in Malawi. Clinical costs, including both direct clinical service costs and the costs of condom and lubricant promotion and distribution, accounted for between 21% (MSV) and 59% (ART) of unit costs in Kenya, and between 25% (MSV) and 38% (ART) in Malawi. Total unit costs were lower in Kenya than they were in Malawi and the difference was especially large for MSV services.
Table 3 displays the breakdown of the total volume-weighted mean unit costs shown in Table 2 by LINKAGES program area. These program areas do not line up perfectly with the unit cost components shown in Table 2. However, they provide additional insight into the relative importance of start-up costs, other KP interventions implemented with clinical services, and above-service level support. The clinical service program area accounted for the largest proportion of total mean unit cost for most services. However, this represented between 20% (MSV) and 54% (ART) of total mean unit costs in Kenya and between 24% (MSV) and 34% (ART) of the costs in Malawi. Program management and monitoring and data use accounted for between 27% (ART) and 42% (SRH and MSV services) of mean unit costs in Kenya and between 31% (PrEP) and 40% (STI services) in Malawi. The KP interventions implemented alongside clinical services (peer outreach, structural interventions, and KP empowerment) accounted for between 15% (ART) and 34% (PEP) of total mean unit costs in Kenya and between 25% (ART) and 31% (MSV) in Malawi. KP mapping and size estimation accounted for between 3% (ART) and 5% (SRH and MSV services) of costs in Kenya and between 6% (PrEP, HTS, ART) and 7% (STI, SRH, and MSV services) in Malawi.
Figure 1 shows scatterplots of the relationship between total unit cost and number of services provided for each clinical intervention across DICs (see data in Table S5). The figure shows that for all services, there was a great deal of variation in unit costs in DICs within and between countries. Overall, unit costs tended to be lower at sites providing larger numbers of services consistent with the existence of economies of scale, though the association between unit cost and number of services provided varied across services and was weaker for STI services. DICs in Malawi tended to have fewer clients than those in Kenya for most services and the highest unit costs for ART, HTS, and MSV services were in the DICs in Malawi that provided the fewest services––mostly DICs serving MSM/TGW. Even at comparable volumes of services delivered, unit costs tended to be higher in DICs in Malawi, especially for ART, STI, and SRH services.

Unit costs per clinical service and numbers of services provided by LINKAGES program drop-in centers in Kenya and Malawi, FY 2019, US$ 2019. Notes: FY 2019 refers to U.S. Government fiscal year from October 1, 2018 to September 30, 2019; FSW female sex workers, MSW male sex workers, MSM men who have sex with men, TGW transgender women, PEP post-exposure prophylaxis, PrEP pre-exposure prophylaxis, HTS HIV testing services, ART antiretroviral therapy, STI sexually transmitted infections, SRH sexual and reproductive health, MSV management of sexual violence. For PrEP and ART, unit costs represent the annual cost per person on PrEP and ART
Discussion
This study describes the costs of PEP, PrEP, HTS, ART, STI, SRH, and MSV services delivered to KPs as part of the LINKAGES program in Kenya and Malawi. We found that mean total unit costs for PEP and PrEP were US$356 and US$456 in Kenya. Across the two countries, total unit costs for HTS, ART, STI, SRH, and MSV services ranged between US$24-US$84, US$368-US$757, US$18-US$41, US$95-US$108, and US$90-US$1240 respectively. Direct clinical service costs accounted for between 21 and 59% of total mean unit costs in Kenya, and between 25 and 38% of unit costs in Malawi. Our results show that in comprehensive HIV programs for KPs, considering direct clinical service costs alone grossly underestimates the cost of service delivery to KPs.
Our assessment of clinical service unit costs by LINKAGES program area shows that above-service program management and data monitoring and non-clinical services delivered to KPs alongside clinical services––deemed to be essential by experts––made up large components of service costs [4]. Program management and data monitoring accounted for between 27–42% (Kenya) and 31–32% (Malawi) of mean unit costs for the seven clinical services. KP interventions implemented alongside clinical services (peer outreach, structural interventions that address stigma, discrimination, and violence, and KP empowerment) accounted for between 18–34% (Kenya) and 25–31% (Malawi) of total service unit costs.
We found differences in mean unit costs between the two countries with the mean unit cost for everything except condoms lower in Kenya than in Malawi. Comparing the two countries is difficult, even though the costing methods applied in both countries were the same. We know that in both Kenya and Malawi, KPs face important structural barriers that impact their vulnerability to HIV infection and impede their access to health services [26]. However, from the information available, it is difficult to ascertain the heterogeneity in the levels of stigma, discrimination, and violence against KPs between the two countries. In general, organizations in Kenya delivered significantly more services than those in Malawi. This was true for almost all service categories, and it was especially true for MSV which had the largest difference in unit cost. The differences in service volumes across DICs likely plays an important role in cost differences in the two countries and these could be due to overall differences in site maturity [34]. Another factor contributing to the differences in cost between the two countries is that headquarter and country office costs were proportionally higher in Malawi. Summaries of LINKAGES program achievements in Kenya and Malawi suggest that the program in Malawi may have had a larger portfolio of above-service level activities playing key roles in national HIV policy and guideline development [35, 36].
We also found important differences in unit costs across facilities within countries. This variation suggests that efficiency of service provision might be improved in certain DICs. Our mapping of DIC service unit costs against numbers of services provided suggests the potential for economies of scale as DICs expand the volume of services delivered, although we recognize that there may be a tension between large volume increases and the provision of services to marginalized and hard to reach populations. It is also possible that there are economies of scope and that DICs that provide more categories of services are more efficient than DICs providing fewer categories of services [37, 38]. Finally, there could be differences in the management of DICs that account for some of the variation in unit costs [39]. Though these issues are beyond the scope of this paper, we will explore the relationships between unit cost and service scale, scope, and facility management in future analyses.
We are not aware of previous studies that have captured the unit costs of a combination of clinical services delivered to KPs in Kenya or Malawi. However, we can compare the mean clinical-service unit costs of HTS, ART, and PrEP to those of previous studies conducted in Kenya and Malawi. Our direct clinical service unit costs of US$5 for HTS in Kenya is similar to previous estimates [40, 41] though our unit costs of US$162 and US$127 for ART and PrEP are slightly lower than earlier studies [42,43,44,45,46,47]. Our direct clinical service unit costs of US$25 for HTS and US$260 for ART in Malawi are somewhat higher than those of previous studies [48,49,50,51,52,53]. Of course, comparisons across cost studies should be done with caution as input utilization and costs vary over time and methods differ across studies.
The only other costing study of a comprehensive HIV program for KPs that we are aware of is the costing study of the Avahan program in India [4, 10]. Cost analysis of the Avahan program also considered non-clinical service elements including interventions to reach and engage FSW, MSM, and TGW. Like our study, the Avahan costing study also captured the full costs of program implementation including service-level and above-service level costs. The Avahan program components differ and are difficult to compare with those of the LINKAGES program and the scope of the clinical services provided in the Avahan program was more limited focusing mostly on the provision of STI services. It is however possible to compare the proportion of program management and monitoring across the two studies. The proportion of program management and monitoring we found in this study was consistent with the 37% program management component in the costing study of the Avahan program [10].
Given the decline in HIV resources in recent years, there is a growing urgency to understand the cost of HIV services to make sure that HIV resources can be allocated effectively and efficiently [21, 54]. This study provides detailed information on the costs of seven HIV services provided to KPs in Kenya and Malawi. These data together with information on the costs of other HIV services including those for the general population, data on the effectiveness of interventions, as well as epidemiological and demographic data, can be used to inform investment cases, strategic plans, and other budgeting exercises. One of the strengths of this study is that the data analyzed are the result of a unique collaboration with the LINKAGES program in which all levels of the LINKAGES program made data available. The study also benefited from the underlying costing frameworks we developed for each country which mapped out activities and associated inputs and outputs and captured all the activities undertaken at all levels of program implementation.
The following limitations should be kept in mind when considering our findings. We used allocation weights based on staff time allocation to allocate above-service level costs to DICs, to allocate indirect input costs to clinical services, and to allocate unspecified costs to LINKAGES program areas. Staff time allocation in our study was based on self-reported time which can be less reliable when staff activities are irregular [31]. We were unable to use time motion direct observation which is generally viewed as the gold standard though this method is not without limitations (i.e., bias from the observer effect) [31, 55]. Confidentiality concerns in settings with significant stigma, discrimination, and violence against KPs as well as resource constraints made it impossible for us to directly observe staff providing services to KPs. One possibility for future studies on the cost of KP services might be to use text messaging to collect information on current activity for a representative sample of providers, days, and hours. Another limitation was that no information was available on the outputs for peer outreach, structural interventions, KP empowerment, for example, and the overlap between these outputs and the outputs of each of the clinical services. An additional challenge was that we used routine monitoring data to capture information on outputs. Though the LINKAGES program had a reasonably robust system for data reporting and verification, the level of detail, quality, and completeness of routine data varied across IPs and DICs. The documentation of donated goods also varied across IPs and DICs and some misreporting of in-kind contributions is possible. Finally, we acknowledge that this study focuses on the costs of services provided to KPs as part of the LINKAGES program in Kenya and Malawi and we do not capture the costs of any referrals from DICs to public health facilities. Similarly, we do not capture information on the costs of HIV services provided to KPs who access services directly from public health facilities.
Conclusions
A better understanding of the cost of HIV services is highly relevant for budgeting and planning purposes and for optimizing HIV services. This descriptive analysis of the costs of HIV services for KPs in Kenya and Malawi shows that when considering all service delivery costs of a comprehensive HIV service package for KPs, costs of services can be significantly higher than when considering direct clinical service costs alone. These estimates can be used to inform investment cases, strategic plans and other budgeting exercises in Kenya and Malawi. They can also be used to pressure test the cost of KP services used in planning and budgeting exercises in other countries where no similar data are available. Additional studies on the cost of comprehensive KP services are urgently needed.
Availability of data and materials
The data generated and/or analyzed during this study are available upon reasonable request.
Abbreviations
- ART:
-
Antiretroviral therapy
- DIC:
-
Drop-in-center
- FSW:
-
Female sex workers
- FY:
-
Fiscal year
- HTS:
-
HIV testing services
- IP:
-
Implementing partners
- KP:
-
Key population
- LINKAGES:
-
Linkages Across the Continuum of HIV Services for Key Populations Affected by HIV
- MSM:
-
Men who have sex with men
- MSV:
-
Management of sexual violence
- MSW:
-
Male sex workers
- PEP:
-
Post-exposure prophylaxis
- PEPFAR:
-
United States President’s Emergency Plan for AIDS Relief
- PREP:
-
Pre-exposure prophylaxis
- PWID:
-
People who inject drugs
- SDG:
-
Sustainable Development Goal
- SRH:
-
Sexual and reproductive health
- STI:
-
Sexually transmitted infection
- SW:
-
Sex workers
- TGW:
-
Transgender women
- US$:
-
United States dollars
- USG:
-
United States Government
References
Joint United Nations Programme on HIV/AIDS. Confronting inequalities: lessons for pandemic responses from 40 years of AIDS. Geneva: UNAIDS; 2021.
Barr D, Garnett GP, Mayer KH, Morrison M. Key populations are the future of the African HIV/AIDS pandemic. J Int AIDS Soc. 2021;24 Suppl 3:e25750.
Garnett GP. Reductions in HIV incidence are likely to increase the importance of key population programmes for HIV control in sub-Saharan Africa. J Int AIDS Soc. 2021;24(Suppl 3):e25727.
DiCarlo MC, Dallabetta GA, Akolo C, Bautista-Arredondo S, Digolo HV, Fonner VA, et al. Adequate funding of comprehensive community-based programs for key populations needed now more than ever to reach and sustain HIV targets. J Int AIDS Soc. 2022;25(7):e25967.
World Health Organization. Consolidated Guidelines on HIV Prevention, Diagnosis, Treatment and Care for Key Populations. Geneva: World Health Organization; 2016.
Beattie TS, Bhattacharjee P, Suresh M, Isac S, Ramesh BM, Moses S. Personal, interpersonal and structural challenges to accessing HIV testing, treatment and care services among female sex workers, men who have sex with men and transgenders in Karnataka state, South India. J Epidemiol Community Health. 2012;66(Suppl 2):ii42-8.
Laga M, Vuylsteke B. Evaluating AVAHAN’s design, implementation and impact: lessons learned for the HIV Prevention Community. BMC Public Health. 2011;11(Suppl 6):S16.
Vassall A, Chandrashekar S, Pickles M, Beattie TS, Shetty G, Bhattacharjee P, et al. Community mobilisation and empowerment interventions as part of HIV prevention for female sex workers in Southern India: a cost-effectiveness analysis. PLoS One. 2014;9(10):e110562.
Chandrashekar S, Guinness L, Kumaranayake L, Reddy B, Govindraj Y, Vickerman P, et al. The effects of scale on the costs of targeted HIV prevention interventions among female and male sex workers, men who have sex with men and transgenders in India. Sex Transm Infect. 2010;86(Suppl 1):i89-94.
Chandrashekar S, Guinness L, Pickles M, Shetty GY, Alary M, Vickerman P, et al. The costs of scaling up HIV prevention for high risk groups: lessons learned from the Avahan Programme in India. PLoS One. 2014;9(9):e106582.
Vassall A, Pickles M, Chandrashekar S, Boily MC, Shetty G, Guinness L, et al. Cost-effectiveness of HIV prevention for high-risk groups at scale: an economic evaluation of the Avahan programme in south India. Lancet Glob Health. 2014;2(9):e531–40.
Herce ME, Miller WM, Bula A, Edwards JK, Sapalalo P, Lancaster KE, et al. Achieving the first 90 for key populations in sub-Saharan Africa through venue-based outreach: challenges and opportunities for HIV prevention based on PLACE study findings from Malawi and Angola. J Int AIDS Soc. 2018;21(Suppl 5):e25132.
Joint United Nations Programme on HIV/AIDS. UNAIDS guidance for partnerships with civil society, including people living with HIV and key populations. Geneva: UNAIDS; 2011.
Weir SS, Figueroa JP, Scott M, Byfield L, Jones Cooper C, Hobbs MC. Reaching key populations through key venues: Insights from the Jamaica HIV Prevention Program. PLoS One. 2018;13(11):e0206962.
Society IA. Differentiated service delivery for HIV: A decision framework for differentiated antiretorivral therapy delivery for key populations. Amsterdam: IAS; 2018.
Edwards JK, Hileman S, Donastorg Y, Zadrozny S, Baral S, Hargreaves JR, et al. Estimating Sizes of Key Populations at the National Level: Considerations for Study Design and Analysis. Epidemiology. 2018;29(6):795–803.
Safarnejad A, Groot W, Pavlova M. Study design and the estimation of the size of key populations at risk of HIV: lessons from Viet Nam. BMC Int Health Hum Rights. 2018;18(1):7.
Wolf RC, Bingham T, Millett G, Wilcher R. Building the evidence base to optimize the impact of key population programming across the HIV cascade. J Int AIDS Soc. 2018;21(Suppl 5):e25146.
Aidsfonds. Fast-track or off track: how insufficient funding for key populations jeopardises ending AIDS by 2030. Amsterdam: Aidsfonds; 2020.
Jones A, Honermann B, Lankiewicz E, Sherwood J, Millett G. Current allocations and target apportionment for HIV testing and treatment services for marginalized populations: characterizing PEPFAR investment and strategy. J Int AIDS Soc. 2021;24 Suppl 3(Suppl 3):e25753.
Joint United Nations Programme on HIV/AIDS. In Danger: UNAIDS Global AIDS Update 2022. Geneva: UNAIDS; 2022.
Global Health Cost Consortium (GHCC). Unit cost study repository 2022. Available from: https://ghcosting.org/pages/data/ucsr/app/.
Tanser F, de Oliveira T, Maheu-Giroux M, Barnighausen T. Concentrated HIV subepidemics in generalized epidemic settings. Curr Opin HIV AIDS. 2014;9(2):115–25.
Joint United Nations Programme on HIV/AIDS. Country factsheets: Kenya: UNAIDS; 2021. Available from: https://www.unaids.org/en/regionscountries/countries/kenya.
Joint United Nations Programme on HIV/AIDS. Country factsheets: Malawi: UNAIDS; 2021. Available from: https://www.unaids.org/en/regionscountries/countries/malawi.
Kavanagh MM, Agbla SC, Joy M, Aneja K, Pillinger M, Case A, et al. Law, criminalisation and HIV in the world: have countries that criminalise achieved more or less successful pandemic response? BMJ Glob Health. 2021;6(8):e006315.
United Nations Development Programme, IRGT: A Global Network of Transgender Women and HIV, United Nations Population Fund, UCSF Center of Excellence for Transgender Health, Johns Hopkins Bloomberg School of Public Health, World Health Organization, et al. Implementing comprehensive HIV and STI programmes with transgender people: practical guidance for collaborative interventions. New York (NY): United Nations Development Programme; 2016.
United Nations Office on Drugs and Crime, International Network of People Who Use Drugs, Joint United Nations Programme on HIV/AIDS, United Nations Development Programme, United Nations Population Fund, World Health Organization, et al. Implementing comprehensive HIV and HCV programmes with people who inject drugs: practical guidance for collaborative interventions. Vienna: United Nations Office on Drugs and Crime; 2017.
United Nations Population Fund, Global Forum on MSM & HIV, United Nations Development Programme, World Health Organization, United States Agency for International Development, World Bank. Implementing comprehensive HIV and STI programmes with men who have sex with men: practical guidance for collaborative interventions. New York (NY): United Nations Population Fund; 2015.
World Health Organization, United Nations Population Fund, Joint United Nations Programme on HIV/AIDS, Global Network of Sex Work Projects, Bank TW. Implementing comprehensive HIV/STI programmes with sex workers: practical approaches from collaborative interventions. Geneva: World Health Organization; 2013.
Vassall A, Sweeney S, Kahn J, Gomez GB, Bollinger L, Marseille E, et al. Reference Case for Estimating the Costs of Global Health Services and Interventions. London, UK: London School of Hygiene & Tropical Medicine; 2017.
Zeng W, Halasa YA, Cros M, Akhter H, Nandakumar AK, Shepard DS. Costing essential services package provided by a non-governmental organization network in Bangladesh. Health Policy Plan. 2017;32(10):1375–85.
Clarke-Deelder E, Vassall A, Menzies NA. Estimators used in multisite healthcare costing studies in low- and middle-income countries: a systematic review and simulation study. Value Health. 2019;22(10):1146–53.
Menzies NA, Berruti AA, Blandford JM. The determinants of HIV treatment costs in resource limited settings. PLoS One. 2012;7(11):e48726.
LINKAGES. LINKAGES Malawi: Summary of Achievements February 2015-September 2019. FHI 360: Durham (NC); 2019.
LINKAGES. LINKAGES Kenya: Summary of Achievements, March 2016–October 2019. Durham (NC): FHI 360; 2019.
Obure CD, Guinness L, Sweeney S, Initiative I, Vassall A. Does integration of HIV and SRH services achieve economies of scale and scope in practice? A cost function analysis of the Integra Initiative. Sex Transm Infect. 2016;92(2):130–4.
Sweeney S, Obure CD, Maier CB, Greener R, Dehne K, Vassall A. Costs and efficiency of integrating HIV/AIDS services with other health services: a systematic review of evidence and experience. Sex Transm Infect. 2012;88(2):85–99.
Sosa-Rubi SG, Bautista-Arredondo S, Chivardi-Moreno C, Contreras-Loya D, La Hera-Fuentes G, Opuni M. Efficiency, quality, and management practices in health facilities providing outpatient HIV services in Kenya, Nigeria, Rwanda, South Africa and Zambia. Health Care Manag Sci. 2021;24(1):41–54.
Bautista-Arredondo S, Sosa-Rubi SG, Opuni M, Contreras-Loya D, Kwan A, Chaumont C, et al. Costs along the service cascades for HIV testing and counselling and prevention of mother-to-child transmission. AIDS. 2016;30(16):2495–504.
Obure CD, Sweeney S, Darsamo V, Michaels-Igbokwe C, Guinness L, Terris-Prestholt F, et al. The Costs of Delivering Integrated HIV and Sexual Reproductive Health Services in Limited Resource Settings. PLoS One. 2015;10(5):e0124476.
Larson BA, Bii M, Halim N, Rohr JK, Sugut W, Sawe F. Incremental treatment costs for HIV-infected women initiating antiretroviral therapy during pregnancy: a 24-month micro-costing cohort study for a maternal and child health clinic in Kenya. PLoS One. 2018;13(8):e0200199.
Larson BA, Bii M, Henly-Thomas S, McCoy K, Sawe F, Shaffer D, et al. ART treatment costs and retention in care in Kenya: a cohort study in three rural outpatient clinics. J Int AIDS Soc. 2013;16:18026.
Peebles K, Mugwanya KK, Irungu E, Odoyo J, Wamoni E, Morton JF, et al. Low costs and opportunities for efficiency: a cost analysis of the first year of programmatic PrEP delivery in Kenya’s public sector. BMC Health Serv Res. 2021;21(1):823.
Roberts DA, Barnabas RV, Abuna F, Lagat H, Kinuthia J, Pintye J, et al. The role of costing in the introduction and scale-up of HIV pre-exposure prophylaxis: evidence from integrating PrEP into routine maternal and child health and family planning clinics in western Kenya. J Int AIDS Soc. 2019;22(Suppl 4):e25296.
Shade SB, Osmand T, Luo A, Aine R, Assurah E, Mwebaza B, et al. Costs of streamlined HIV care delivery in rural Ugandan and Kenyan clinics in the SEARCH Studys. AIDS. 2018;32(15):2179–88.
Wanga V, Peebles K, Obiero A, Mogaka F, Omollo V, Odoyo JB, et al. Cost of pre-exposure prophylaxis delivery in family planning clinics to prevent HIV acquisition among adolescent girls and young women in Kisumu, Kenya. PLoS One. 2021;16(4):e0249625.
Maheswaran H, Petrou S, MacPherson P, Choko AT, Kumwenda F, Lalloo DG, et al. Cost and quality of life analysis of HIV self-testing and facility-based HIV testing and counselling in Blantyre. Malawi BMC Med. 2016;14:34.
McBain RK, Petersen E, Tophof N, Dunbar EL, Kalanga N, Nazimera L, et al. Impact and economic evaluation of a novel HIV service delivery model in rural Malawi. AIDS. 2017;31(14):1999–2006.
Mwenge L, Sande L, Mangenah C, Ahmed N, Kanema S, d’Elbee M, et al. Costs of facility-based HIV testing in Malawi, Zambia and Zimbabwe. PLoS One. 2017;12(10):e0185740.
Orlando S, Diamond S, Palombi L, Sundaram M, Shear Zimmer L, Marazzi MC, et al. Cost-Effectiveness and Quality of Care of a Comprehensive ART Program in Malawi. Medicine (Baltimore). 2016;95(21):e3610.
Tagar E, Sundaram M, Condliffe K, Matatiyo B, Chimbwandira F, Chilima B, et al. Multi-country analysis of treatment costs for HIV/AIDS (MATCH): facility-level ART unit cost analysis in Ethiopia, Malawi, Rwanda, South Africa and Zambia. PLoS One. 2014;9(11):e108304.
Vyas S, Songo J, Guinness L, Dube A, Geis S, Kalua T, et al. Assessing the costs and efficiency of HIV testing and treatment services in rural Malawi: implications for future “test and start” strategies. BMC Health Serv Res. 2020;20(1):740.
De Lay PR, Benzaken A, Karim QA, Aliyu S, Amole C, Ayala G, et al. Ending AIDS as a public health threat by 2030: Time to reset targets for 2025. PLoS Med. 2021;18(6):e1003649.
Bratt JH, Foreit J, Chen PL, West C, Janowitz B, de Vargas T. A comparison of four approaches for measuring clinician time use. Health Policy Plan. 1999;14(4):374–81.
Acknowledgements
We are grateful for the support and helpful comments on this analysis received from Hally Mahler of FIH360, Gina Dallabetta and Kate Harris from the Bill and Melinda Gates Foundation, staff of the Global Fund, and managers and staff of the LINKAGES program in Kenya and Malawi. We thank Obed Ocampo, Rouseline Gómez, and Gina La Hera for their assistance with data analysis. We also thank the United States Agency for International Development (USAID) for support to the LINKAGES program (Cooperative Agreement AID-OAA-A-14-00045).
Funding
This study was funded by the Bill and Melinda Gates Foundation (grant: OPP1175038). The funding agency had no role in the study design, collection/analysis of data, data interpretation, or manuscript writing.
Author information
Authors and Affiliations
Contributions
Conceptualization: SBA. Formal analysis: JESM, ASO. Funding acquisition: SBA. Investigation: MO, JESM, JLFO, ASO, SBA. Methodology: MO, SBA. Supervision: SBA. Writing – original draft: MO, JESM. Writing – review & editing: MO, JESM, JLFO, ASO LMB, AO, SM, JK, MD, SBA. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethical review board of the National Institute of Public Health, Mexico, approved the study (CI: 1554). Informed consent was not required for this study, which did not involve human subjects research.
Consent for publication
Not applicable.
Competing interests
MO received consulting fees for the conduct of this study. The other authors declare there are no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary information 1: Figure S1.
LINKAGES program implementation levels and sample size by level. Figure S2. LINKAGES program areas and elements. Table S1. Cost categories and sub-categories included in the LINKAGES costing study. Table S2. Methods used to estimate total LINKAGES program cost per DIC. Table S3. Approach used to estimate costs per clinical service (PEP, PREP, HTS, ART, STI, SRH, MSV). Table S4. Approach used to estimate costs per LINKAGES program area (KP mapping & size estimation, KP empowerment, structural interventions, peer outreach, clinical services, management, monitoring & data use). Table S5. Unit costs per clinical service and numbers of services provided by LINKAGES program drop-in centers in Kenya and Malawi, FY 2019, US$ 2019.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Opuni, M., Sanchez-Morales, J.E., Figueroa, J.L. et al. Estimating the cost of HIV services for key populations provided by the LINKAGES program in Kenya and Malawi. BMC Health Serv Res 23, 337 (2023). https://doi.org/10.1186/s12913-023-09279-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09279-w