
Abstract
Background
Youths are people aged between 15 and 24 years. Globally, there were 37.7 million people living with HIV/AIDS, and 90% occur among youths. Despite enormous efforts made in Ethiopia to improve the reproductive health of the youth the utilization is still low. There is no study conducted on YFRHS utilization and associated factors among youths in East Belesa. Therefore, this study is aimed to assess YFRHS utilization and its associated factors among secondary school youths in East Belesa district.
Objective
To assess the prevalence of youth friendly reproductive health service utilization and associated factors among secondary school students in East Belesa district, Ethiopia, 2022.
Method
Institution based cross-sectional study design was used with a total sample size of 347 youths in East Belesa schools from May 23 to June 12, 2022. Stratified simple random sampling was employed. Data were entered using EpiData and analyzed using Stata version 14. Descriptive statistics and Logistic regression were done to describe and identify factors associated with reproductive health services utilization. A P-value of less than 0.05 was considered to declare a level of significance.
Results
A total of 346 students participated in the study with a response rate of 99.8%.the magnitude of youth friendly reproductive health service utilization was 28.9% (24.3, 33.9). Being married (AOR = 0.27, 95%CI: 0.14, 0.52), mothers attended higher education (AOR = 1.40, 95%CI: 1.87, 4.95), availability (AOR = 2.58. 95%CI: 1.29, 5.16) and students who had never discussed about reproductive issues with their families (AOR = 0.18, 95%CI: 0.07, 0.49) were significantly associated with youth friendly service utilization. Therefore, behavior change communication interventions targeted at advancing mothers’ knowledge, encouraging open discussion between parents and children, and enhancing the availability of youth friendly services are important to enhance youth friendly service utilization.
Similar content being viewed by others

Introduction
Youths are people aged between the age groups of 15 and 24 years [1,2,3]. In 2019, the youth population accounted 1.2 billion (16%) of the global population, 211 million (18.3%) of the youths were living in sub-Saharan Africa. In Ethiopia the youth account for one third of the Ethiopian population [1, 4].
Youth Friendly Reproductive Health Services (YFRHS) are those services that are accessible, acceptable and appropriate for the youth including general counseling services about sexuality, voluntary counseling and testing (VCT), treatment and diagnosis of sexually transmitted infections, contraception, condom, perinatal care services, abortion and post abortion care services [2, 4]. Globally, there were 37.7 million people living with Human Immune Virus Acquired Immune Deficiency Syndrome ( HIV/AIDS), and 90% occur among youths [5]. Youth in Sub-Saharan Africa countries are at greater risk of Sexual and Reproductive Health (SRH) problems than those youth from the other parts of the world [6]. The overall utilization of YFRHS in Ethiopia was 42.87% [3].
In Ethiopia, SRH of youth has become a major public health concern [7]. To address the sexual and reproductive health problem of the youth, the Federal Ministry of Health (FMOH) established Youth Friendly Reproductive Health Services (YFRHS) strategy in 2015 [8].
Numerous studies found that sex, maternal education, discussion with families/friends and, educational level, knowledge and attitude were factors associated with intention to use YFRHS [2,3,4, 6, 9,10,11,12,13,14]. Despite enormous policies, programs, and efforts that have been made in Ethiopia to improve reproductive health outcomes of the youth, the level of utilization is still very low [3, 15]. To the best of our knowledge there is no study conducted on YFRHS utilization and associated factors among secondary school students in East Belesa. Therefore, this study is aimed to assess YFRHS utilization and its associated factors among secondary school youths in East Belesa district.
Materials and methods
Study design and setting
An institution based cross-sectional study was conducted from May 23 to June 12, 2022. The study was conducted in East Belesa district. East Belesa is one of the districts in central Gondar zone, North West Ethiopia, Amhara regional state. It is bordered in the south by South Gondar zone, on the North by Jan Amora, on the West by West Belesa, on the North West by Wegera, and on the East by Wag-Hemra Zone. The district has 22 kebeles. The district is located 720 km far from Addis Ababa (the capital city of Ethiopia). In East Belesa there are four secondary schools including Gohala secondary school (9-12th = 4001), Zuy-Hamusit secondary school (9-12th = 2846), Timen secondary school (9-10th = 693) and Mukatera secondary school (9-10th = 298). There were a total of 7,838 secondary school students attending their education in East Belesa district in those four secondary schools. There is only one youth friendly service clinic in the district.
Source and study population
All secondary school students in East Belesa district were the source population and all secondary school students who were attending their education in East Belesa district and who were available during data collection were the study population for this study.
Inclusion and exclusion criteria
All secondary school students who were attending their education in East Belesa district and available during data collection were included in the study. However, Secondary school students who were seriously ill (to the extent of unable to read and write) during data collection period were excluded from the study.
Sample size determination and sampling procedure
The sample size was determined by using single population proportion formula: \(n=(z\alpha /2)2*pq/d\) 2. Assumptions: based on following Assumption; Estimated proportion (p) taken from previous study done at Debre Tabor on the utilization of youth friendly reproductive health services among youth (28.8%) [16], Margin of error d = 5%, Confidence level of 95%. The total sample size was: n = (1.96)2 (0.288)(0.712) /0.052 = 315. By considering non response rate 10% which is 32, the final sample size was 347. Stratified random sampling technique was used. The total sample was allocated to each grade [9,10,11,12] in proportion to their student size. The study participants were selected randomly by using computer-generated random numbers based on a sampling frame prepared by using their identification number (ID) obtained from their respective schools.
Study variables
Dependent variable
Utilization of youth friendly reproductive health services.
Independent variables
Socio-demographic variables (age, sex, marital status, residence, religion, education level, living arrangement, monthly pocket money, parental occupation and parental education), sexual experience (yes/no), availability, privacy, convenient time of service delivery (yes/no), communication /discussion with parents (yes/no), distance to health facility (≤ 30 min/>30 min),visited health facility with in the last 12 months (yes/no), media exposure (yes/no), participation in school clubs (yes/no), faced reproductive health problems (yes/no), knowledge (good/poor), and attitude (positive/negative).
Operational definition
Youth Friendly Reproductive Health Service
incorporates general counseling services, Family planning service, VCT, using condom, Treatment of sexually transmitted Infections, and perinatal care (Antenatal Care (ANC), delivery and postnatal care), abortion and post abortion care services.
YFRHS utilization
utilization of at least one component of youth friendly reproductive health services.
Sexual experience
was assessed by asking the participants “whether they ever had sexual intercourse or not” (yes/no).
Knowledge of YFRHS
Four composite score of knowledge items were used to measure the level of knowledge of the respondents regarding youth friendly reproductive health services. For each knowledge, item scores were summed up to get over all knowledge scores, individuals correctly answered the item given a value of “1” and for those answered incorrectly valued ”0”, and then mean and standard deviation were calculated. The mean knowledge score was 7.11 ± 2.21 (α = 0.75).
Youth reproductive health service utilization
Those respondents who utilize at least one of the following main RH services in the past one year [17].
Reproductive health problems
Those respondents who faced at least one of RH problems (unwanted pregnancy, abortion, sexual violence, teenage pregnancy, and Sexually Transmitted Infections (STIs) [17].
Attitude towards YFRHS utilization
Attitude (overall evaluation of YFRHS utilization as favorable or unfavorable) was assessed using four items with five point Likert scales. The sum score ranged from 4 to 20 and the higher score indicates favorable attitude towards using YFRHS (α = 0.91).
Data collection and analysis
Data was collected through a pretested and structured questionnaire after reviewing different relevant literatures [1, 3, 13, 14, 17,18,19,20,21,22,23]. Four diploma nurses as data collectors and two B.sc health officers as supervisors were trained for two days. The data was collected by using self-administered structured questionnaire which was prepared by using the local language (Amharic) and translated back to English. Data was entered to EpiData version 4.6 and exported to STATA version 14 for its analysis. The results of the descriptive statistics were summarized by using mean, standard deviation, percentage, frequency tables and graphs. Both binary and multivariable logistic regression analyses were conducted. Those variables which have a p-value of < 0.2 in binary logistic regression analysis were candidate variables for multivariable logistic regression analysis. Moreover, Adjusted Odds ratio (AOR) with 95% confidence interval was used to determine the strength of association between predictor and outcome variables In multivariable logistic regression analysis variables having a p-value < 0.05 with 95% confidence interval were considered as statistically significant.
Results
Socio-demographic characteristics of participants
Among 347 students included in the study, 346 participated in the study. with a response rate of 99.8%. The mean age of the participants was 18.7 ± 2.25 years old, and 63.3% of the respondents were within the age group of 15–19 years. Majority of respondents 90.5% were orthodox religion followers. More than half (59.0%) of childhood residents were from a rural area. Majority of respondents were living with their families 83.8% (Table 1 ).
Knowledge about Youth friendly Reproductive Health Services
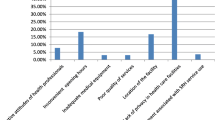
Two-thirds 250 (72.3%) of youths have ever heard about YFRHS. The common source of information was health professionals (36.4%) and teachers (23.2%). The most common components of YFRHS by respondents were general counseling service (40.8%) and family planning (31.6%). About (67.2 %) of the respondents had good knowledge on YRHS (Table 2).
Magnitude of YFRHS utilization
Overall reproductive health utilization was (28.9%) (95% CI: 24.3–33.9). Among the YFRHS components, general counseling services 35 (10.1%), voluntary counseling and testing for HIV 23 (6.7%), STI diagnosis and treatment 17 (4.9%), Family planning 13 (3.8%), Antenatal care services 9 (2.6%) and condom 3 (0.9%) were utilized by school youths in East Belesa district in the last 12 months.
Factors Associated with utilization of YFRHS
In multiple logistic regression, marital status, mother’s education, availability and discussion with parents were significantly associated with YFRHS utilization.
The odds of YFRHS utilization was 73% lower among married students as compared to single students (AOR = 0.27, 95%CI: 0.14, 0.52). The odds of YFRHS utilization was 1.40 times higher among students having mothers who attended higher education as compared with students having mothers who have no formal education (AOR = 1.40, 95%CI: 1.87, 4.95). The likelihood of YFRHS utilization was 2.58 times higher among students who reported YFRHS are available in their area unlike those students who indicated that YFRHS are not available in the area. (AOR = 2.58. 95%CI:1.29, 5.16). The odds of YFRHS utilization were lowered by 82% among students who had never discussed with reproductive and sexual health issues with their parents/friends as compared as compared with their counterparts (AOR = 0.18, 95%CI: 0.07, 0.49) (Table 3).
Discussions
This study is aimed to asses YFRHS utilization and associated factors among secondary school students in East Belesa district 2022. The magnitude of YFRHS utilization was 28.9% (24.3, 33.9). This is in line with studies done in Debre Tabor town, Northwest Ethiopia and Woreta town, South Gondar, North West Ethiopia [1, 16].
This finding is lower than the studies conducted in Amhara region, Harar town, east Ethiopia, Bossat District, Oromia Region, Ethiopia and Bale Zone of Ethiopia [2, 4, 14, 17]. However this finding is higher than the study findings reported in Western Ethiopia, Ambo Town, Oromia Regional State, Ethiopia and Mecha District, Northwest Ethiopia [9, 19, 24]. The possible justification for the discrepancy might be the variation in socio-demographic characteristics, study design and period. Some areas might have better availability and accessibility of YFRHS than others which may affect the utilization of YFRHS among youths and may have a significant role in the observed variation in the magnitude of YFRHS utilization [21, 25].
Marital status was significantly associated with YFRHS utilization. Married students were less likely to use YFRHS than unmarried students. This is in line with the studies done in Gondar city, Ethiopia [26]. This might be due to married students’ decision to use YFRHS may also affected by their spouse/partner. This implies that married students might not be autonomous and make reproductive health decisions alone.
Educational level of mothers was also significantly associated with YFRHS utilization.
Students with mothers who attended higher education were more likely to utilize YFRHS than that of students having mothers who have no formal education [3, 6]. This can be explained that women at higher level of education might have a better access to SRH information and would be more flexible to deal with their children or investigate for any problems their children encounter regarding SRH services use. Maternal education about RH issues influences their children’s ability to freely discuss sexual and reproductive issues, allows them to use RH services and enables children to protect and promote their health and well-being [6].
Availability of youth friendly services was significantly associated with YFRHS utilization. Students who reported YFRHS are available in their area were more likely to use YFRHS unlike those students who declared that YFRHS are not available in the area. This in line with the study done in Kenya and Nigeria [27, 28]. This could be attributed to easy availability of YFRHS may facilitate their motive to use those services.
Discussion with parents about sexual and reproductive issues was significantly associated with YFRHS utilization. Students who had never discussed reproductive and sexual health issues with their parents/friends were less likely to use YFRHS as compared to their counterparts. This is in line with the studies done in Southern Ethiopia, a systematic review and meta-analysis done in Ethiopia [3, 6]. This might be due to the fact that open discussion about SRH issue between family and their children increases awareness and avoids feeling shy and fear of being seen while getting SRH services. Moreover, the discussion creates more opportunities to share SRH information and experience of health-related problems, then the youths would have better knowledge and awareness about SRH services and develop positive attitudes towards YFRHS Which in turn might motivate them to use those services [16, 17].
Limitations
It is difficult to establish temporal association between YFRHS utilization and its predictors. The study used a self-reporting instrument that has a potential of introducing social desirability bias. This study might be subjected to recall bias since respondents were requested to answer their past experiences.
Conclusion
The magnitude of youth friendly reproductive health service utilization in East Belesa was low. Marital status, maternal education, availability of services and discussion with families were significantly associated with YFRHS utilization. Therefore, behavior change communication interventions primarily targeted at promoting open discussion between youth and families, enhancing mothers’ knowledge, enhancing the availability of youth friendly services, and school reproductive health clubs especially for those married youths are important to enhance youth friendly service utilization rate. Hence, East Belesa district health offices, East Belesa education offices and other organizations working in the area of youths reproductive health services are recommended to give awareness on youth friendly service utilization for youth’s mothers through provision of training in collaboration with East Belesa town administration.
Abbreviations
- AIDS:
-
Acquired Immune Deficiency Virus
- AOR:
-
Adjusted Odds Ratio
- CI:
-
Confidence Interval
- HIV:
-
Human Immunodeficiency Virus
- VCT:
-
Voluntary Counseling and Testing
- WHO:
-
World Health Organization
- YFRHS:
-
Youth Friendly Reproductive Health Services
References
Abate AT, Ayisa AA, Wmariam TG. Reproductive health services utilization and its associated factors among secondary school youths in Woreta town, South Gondar, North West Ethiopia: A cross sectional study. BMC Res Notes . 2019;12(1):1–7. Available from: https://doi.org/10.1186/s13104-019-4129-z
Motuma A, Syre T, Egata G, Kenay A. Utilization of youth friendly services and associated factors among youth in Harar town, east Ethiopia : a mixed method study. BMC Health Serv Res. 2016;1–10. Available from: https://doi.org/10.1186/s12913-016-1513-4
Belay HG, Arage G, Degu A, Getnet B, Necho W, Dagnew E et al. Youth-friendly sexual and reproductive health services utilization and its determinants in Ethiopia: A systematic review and meta-analysis. Heliyon. 2021;7(12):e08526. Available from: https://doi.org/10.1016/j.heliyon.2021.e08526
Bogale N, Agero G. Youth Friendly Health Care Services utilization and Associated factors among High School students in Bossat District. Oromia Region Ethiopia. 2020;6(6):42–53.
UNAIDS data 2021 . 2021. Available from: https://www.unaids.org/sites/default/files/media_asset/JC3032_AIDS_Data_book_2021_En.pdf
Haile B, Shegaze M, Feleke T, Glagn M, Andarge E. Disparities in utilization of sexual and reproductive health services among high school adolescents from youth friendly service implemented and non-implemented areas of Southern Ethiopia. Arch Public Heal. 2020;78(1):1–11.
Abebe M. Awoke W. Utilization of Youth Reproductive Health Services and Associated Factors among High School Students in Bahir Dar, Amhara Regional State, Ethiopia. Open J Epidemiol. 2014;4:69-75. https://doi.org/10.4236/ojepi.2014.42012.
Kereta W, Belayihun B, Hagos K, Molla Y, Pirzadeh M, Asnake M. Youth-Friendly Health Services in Ethiopia: What Has Been Achieved in 15 Years and What Remains to be Done. 2021.
Tilahun T, Bekuma TT, Getachew M, Seme A. Assessment of access and utilization of adolescent and youth sexual and reproductive health services in western Ethiopia. Reprod Health [Internet]. 2021;18(1):1–9. Available from: https://doi.org/10.1186/s12978-021-01136-5
Geary RS, Gómez-Olivé FX, Kahn K, Tollman S, Norris SA. Barriers to and facilitators of the provision of a youth-friendly health services programme in rural South Africa. BMC Health Serv Res. 2014;14(1):1–8.
Ninsiima LR, Chiumia IK, Ndejjo R. Factors influencing access to and utilisation of youth-friendly sexual and reproductive health services in sub-Saharan Africa: a systematic review. Reprod Health [Internet]. 2021;18(1):135. Available from: https://doi.org/10.1186/s12978-021-01183-y
Khanal SP. Multi-level barriers for utilization of Youth Friendly Reproductive Health Services (YFRHS) among youths. J Heal Promot. 2020;8(June):95–108.
Thongmixay S, Essink DR, De Greeuw T, Vongxay V, Sychareun V, Broerse JEW. Perceived barriers in accessing sexual and reproductive health services for youth in Lao People’s Democratic Republic. PLoS ONE. 2019;14(10):1–16.
Aa, Kerbo. Youth Friendly Sexual and Reproductive Health Services Utilization and Associated Factors, Bale Zone, Ethiopia: Community Based Cross-Sectional Study. 2018.
DeMaria LM, Smith KV, Berhane Y. Sexual and reproductive health in Ethiopia: gains and reflections over the past two decades. Reprod Health [Internet]. 2022;19(1):1–6. Available from: https://doi.org/10.1186/s12978-022-01464-0
Simegn A, Azale T, Addis A, Dile M, Ayalew Y, Id BM. Youth friendly sexual and reproductive health service utilization among high and preparatory school students in Debre Tabor town, Northwest Ethiopia : A cross sectional study. 2020;1–13. Available from: https://doi.org/10.1371/journal.pone.0240033
Liyeh TM, Goshu YA, Belay HG, et al. Youth Reproductive Health Service Utilization and Associated Factors among Amhara Region Female Night Students, Ethiopia. Biomed Res Int. 2021;2021:6640219. https://doi.org/10.1155/2021/6640219.
1. Ma J, Hainsworth G, Solter C, Cnm. A Rapid Assessment of Youth Friendly Reproductive Health Services. Pathfind Int. 2010.
Tsega MT. Sexual and Reproductive Health Services utilization and Associated factors among Preparatory School students in Mecha District, Northwest Ethiopia: Cross Sectional Study. J Gynecol Womens Heal. 2018;11(5):1–8.
Napit K, Shrestha KB, Magar SA, Paudel R, Thapa B, Dhakal BR, et al. Factors associated with utilization of adolescent-friendly services in Bhaktapur district, Nepal. J Health Popul Nutr. 2020;39(1):2.
Tlaye KG, Belete MA, Demelew TM, Getu MA, Astawesegn FH. Reproductive health services utilization and its associated factors among adolescents in Debre Berhan town, Central Ethiopia: a community-based cross-sectional study. Reprod Health. 2018;15(1):1–11.
Ansha MG, Bosho CJ, Jaleta FT. Reproductive Health Services Utilization and Associated Factors Among Adolescents in Anchar District, East Ethiopia. J Fam Reprod Heal [Internet]. 2017;11(2):110–8. Available from: https://www.ncbi.nlm.nih.gov/pubmed/29282419%0Ahttps://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC5742664
Binu W, Marama T, Gerbaba M, Sinaga M. Sexual and reproductive health services utilization and associated factors among secondary school students in Nekemte town, Ethiopia. Reprod Health. 2018;15(1):1–10.
Fikadu A, Teferi E, Mekuria M, Birhanu A, Benti T. Youth Friendly Reproductive Health Service utilization and Associated factors among School Youths in Ambo Town, Oromia Regional State, Ethiopia, 2018. Am J Heal Res. 2020;8(4):60.
Gunta M, Tantu T, Wolka S, Meskele M, Ayza A, Duko B. Sexual and Reproductive Health Services Utilization among Wolaita Sodo University Students, Ethiopia: A Mixed Method Approach. ScientificWorldJournal. 2021;2021:2415023. https://doi.org/10.1155/2021/2415023.
Alem AT, Sisay MM, Alemayehu AM. Factors affecting Voluntary HIV/AIDS counseling and testing service utilization among Youth in Gondar City, Northwest Ethiopia. HIV AIDS (Auckl). 2020;12:667–73.
1. Ajibade B, Oguguo C. Recommendations for removing access barriers to effective Sexual/Reproductive Health Services (SRHS) for young people in South East Nigeria: A systematic review. Int J Sex Reprod Heal Care. 2022;5:47–60.
AKINYI OP, DETERMINANTS OF UTILIZATION OF YOUTH FRIENDLY REPRODUCTIVE HEALTH SERVICES AMONG SCHOOL AND COLLEGE YOUTH IN THIKA WEST, DISTRICT, KIAMBU COUNTY, KENYA [Internet]. KENYATTA UNIVERSITY; 2009. Available from: http://publichealth.ku.ac.ke/images/stories/docs/students-research/Obonyo-Perez.pdf
Acknowledgements
We are also pleased to thank East Belesa health office for writing permission letter. We would like to thank East Belesa secondary school teachers, directors for their facilitation. Lastly but not the least, we are glad to thank study participants, data collectors and supervisors for their time and contribution to this work.
Data sharing statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding
The study was funded for academic purpose by Ambo University, College of Medicine and Health Sciences, department of public Health. The funder had no impact on design, collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from of University of Gondar, College of Medicine and Health Sciences, Institute of Public Health, Institutional Review committee. Permission letter was obtained from district health office and oral permission was taken from each school principals. After the purpose and objective of the study was informed, written informed consent was obtained from each study participants. For participants with the age of less than 18 years, informed consent has been taken from their parents. All participants were informed that participation was on a voluntary basis and they could withdraw from the study at any time if they were not comfortable with the questionnaire. To maintain confidentiality data were collected and analyzed anonymously. All methods were carried out in accordance with Helsinki declarations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they had no any conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tsegaw, M., Kassie, A. & Alemnew, W. Youth friendly reproductive health service utilization and its associated factors among secondary school students, East Belesa district, northwest, Ethiopia, 2022. BMC Health Serv Res 23, 184 (2023). https://doi.org/10.1186/s12913-023-09152-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09152-w