
Abstract
Background
Stage III and IV pressure injuries (PIs) in patients with spinal cord injury (SCI) require complex interdisciplinary and interprofessional treatment approaches that are difficult to implement. Practical aspects, such as information exchange and coordination, remain challenging. We investigated whether a computerized decision support system (CDSS) could increase treatment adherence and improve clinical outcomes and interprofessional collaboration.
Method
In this feasibility study, a core team developed the initial treatment process and adapted it based on several discussions with clinical experts and information technologists. The CDSS followed the Basel Decubitus Approach and was used in a clinic specializing in SCI. Thirty patients with SCI admitted for stage III/IV PI between July 2016 and May 2017 were randomly allocated to standard or CDSS-supported care. Between-group differences in treatment adherence, complication rates, length of stay, and costs were analyzed using descriptive statistics. The use of the CDSS and potential barriers and facilitators were evaluated through interprofessional focus groups, transcribed verbatim, and thematically analyzed (30 participants).
Results
No differences in SCI characteristics, comorbidities, or PI characteristics (localization: ischium [number (n) = 19 PI, 63%], sacrum [n = 10 PI, 33%], recurrent PI [n = 21, 70%]) were found between the two groups. Furthermore, no statistically significant differences were observed in treatment adherence, frequency of major (20% vs. 13% between CDSS and control group) and minor (33% vs 27%) complications, and length of stay (98 [±28] vs 81 [±23] days). Healthcare professionals found the CDSS to be helpful for visualizing the treatment process. However, the high workload and difficulties in the information technology processes, such as missing reminders, slow computer performance and data processing, and poor accessibility, hindered the effective implementation of the CDSS.
Conclusion
The implementation of the CDSS to support the treatment of stage III/IV PI in patients with SCI was feasible and included definitions of milestones, interventions, and outcomes. However, to assess the impact of the CDSS, a longer observation period is required. Further, the technical difficulties must be addressed, and solid integration of the CDSS into the clinical information system is necessary.
Trial Registration
This quality improvement project received a declaration of no objection from the Ethics Committee of Northwest and Central Switzerland (EKNZ UBE-16/003), and ethical approval was received for the focus groups (EKNZ Req-2017-00860).
Similar content being viewed by others


Introduction
Process management is an innovative methodological step in healthcare [1,2,3,4,5,6]. It includes a series of defined diagnostic and therapeutic interventions for treating a problem, achieving a goal, shaping and structuring different clinical settings, and improving guideline adherence. However, the implementation of process management in many clinical settings is challenging due to a lack of awareness of all process elements, a lack of knowledge translation, and the complexity of treatment [2]. Hence, computerized decision support systems (CDSSs) were developed to improve guideline adherence by leading health-care professionals (HCPs) through these processes, reminding them of relevant steps, and managing them in their specific duties [3]. CDSSs optimize adherence to treatment processes, reduce teams’ workloads, and consequently reduce total treatment costs [1, 3]. Most importantly, standard treatment processes may be reevaluated and continuously improved by using data from daily clinical management. To date, CDSSs have mainly been evaluated for the management of acute clinical situations. They have been shown to lead to reduced complication rates [7], increased employee satisfaction [8, 9], better communication during visits, and a better overview of information for all involved HCPs [10, 11]. While CDSSs are tools for quality improvement and influence quality indicators [11, 12], contradictory results have been obtained from process management and CDSS implementation in clinical contexts, regardless of whether the CDSS led to improved guideline adherence or to a reduction in complication rates [5, 7].
According to the European Pressure Ulcer Advisory Panel (EPUAP), the treatment of stage III and IV pressure injuries (PIs) in patients with spinal cord injury (SCI) consists of acute care and rehabilitation provided by various HCPs. The interdisciplinary team includes different physicians, such as plastic surgeons, paraplegiologists, internal medicine physicians, and infectiologists as well as HCPs from other professions, such as nurses, physio- and occupational therapists, psychologists, and social workers [13]. Due to the complex coordination needs in interdisciplinary treatment, this treatment could benefit from process management and CDSS-supported therapy to achieve clearly structured procedures. PIs are among the most frequent and cost-intensive complications in people with SCI [14, 15]. Often aggravated by early and late postsurgical complications [16,17,18,19,20], PIs can lead to long hospital stays and reduced quality of life [21, 22]. Internationally, it is accepted that stage III/IV PIs require flap reconstruction [17, 19, 22], postsurgical immobilization, and antibiotic therapy [23]. Because complications during early postsurgical treatment occur more often in patients with a high-risk profile, individual risk analyses are recommended, such as malnutrition screening, as well as the diagnosis and treatment of comorbidities [19, 24,25,26].
The Basel Decubitus Approach is a set of principles for the treatment of PIs that has been developed over the past few decades. It includes different therapeutic elements, such as pressure relief; debridement; treatment of risk factors, such as anemia, renal failure, uncontrolled diabetes, and spasticity; flap surgery; prevention of early postsurgical complications and PI recurrence; transfer training; and re-evaluation of assistive devices [21, 25,26,27,28,29]. Due to the complexity of this treatment approach, its implementation and adherence in the clinical setting have been difficult [18, 21, 26, 28, 30]. We hypothesized that a CDSS would support process management, thus increasing adherence to the Basel Decubitus Approach and improving the quality of treatment for patients with SCI and stage III and IV PIs by reducing complications, shortening the length of stay, and improving secondary prevention strategies [31].
This feasibility study aimed to describe the effect of a CDSS on adherence to the Basel Decubitus Approach by comparing complication rates, length of stay, total-, intervention-, and occupation-specific costs, and the performance of examinations and interventions between standard and CDSS-supported care. Additionally, this study explored HCPs’ perspectives on the use of this CDSS.
Methods
Design
We conducted a feasibility study with routinely collected data for our quality improvement project and a qualitative focus group study. For reporting, we used the CONsolidated Standards of Reporting Trials (CONSORT) 2010 extension pilot or feasibility trial checklist [32, 33] (Appendix 1).
Setting
This study was conducted at a Swiss acute and rehabilitation clinic that specializes in SCI. This clinic integrates a plastic surgery team from a nearby university hospital and is specialized in the treatment of PI in patients with SCI using the Basel Decubitus Approach. The Basel Decubitus Approach [26,27,28, 34] is based on six main principles: pressure relief (1); debridement (2); treatment of risk factors and comorbidities, (3) such as anemia, renal failure, uncontrolled diabetes, and spasticity; wound conditioning (4), flap surgery (5); and prevention of early postsurgical complications and PI recurrence (6). Some interventions, such as nutritional and psychological counseling, have redefined and integrated into the Basel Decubitus Approach [25, 29, 30].
The treatment approach for PI includes paraplegiology, plastic surgery, infectious disease management, specialized acute and rehabilitation care, physical therapy, occupational therapy, nutritionist support, and psychotherapy [21, 24, 27,28,29,30].
Participants
We included adult patients with SCI or similar syndromes (e.g., multiple sclerosis) presenting with a stage III/IV PI according to the EPUAP classification over the ischium, sacrum, or trochanter who were admitted for inpatient treatment, including plastic surgery. Patients with a malignant disease, a local skin disease (e.g., fungal infection), or who denied use of their data were excluded.
All patients meeting the inclusion criteria between July 2016 and May 2017 were randomly assigned by the admission case management team to standard care or to treatment by specially trained teams using the CDSS. Three out of six teams in the clinic in different wards were trained to use the CDSS. The admission case management team, whose members were not informed about the CDSS use, simply assigned patients to “free” beds and distributed the workload equally among the nursing wards. The admission case management team was blinded to the assignment of patients to wards, and the research team was not involved in the ward assignment process.
Intervention
Development of the CDSS
The objective of the CDSS was to illustrate interprofessional management according to the Basel Decubitus Approach and to guide the HCPs through the complex treatment intervention. The development of the CDSS involved four steps.
First, during the preparation phase from 2015 to 2016, the core team (a specialized physician [AS-S], a wound care nurse [KGL], a quality management expert [KS], and an information technology (IT) specialist [SS]) defined the use case. A “use case” is the starting point in the IT logic for creating a business process modeling notation (BPMN). It includes a list of actions or event steps in this specific process. The core team defined the milestones during the treatment process. For example, after the flap surgery the patient was immobilized on an airflow mattress. If there were no complications, the suture material was removed 21 days after the surgery. In case of delayed wound healing, wound dehiscence, or other complications, such as hematoma or infection, the timing of the suture removal was determined individually by the plastic surgeon. Influential dependencies between each step were described and visualized according to the Basel Decubitus Approach. The core team determined that the CDSS should guide the HCPs through the treatment process and make the process visible. The CDSS informed the physicians of the list of required steps during the treatment process (prescription of various assessments, examinations, and other therapies). The CDSS guided the interprofessional team through the complex treatment process with relevant milestones, which were integrated into their clinical management. The IT process and milestones were adapted if required based on clinically indicated individual changes in treatment.
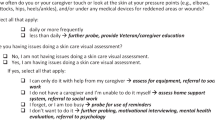
Second, we defined the measurement of baseline assessments, milestones, timelines, and outcomes according to the Basel Decubitus Approach (Table 1). The process combined the following milestones: admission, debridement and bone biopsy, flap surgery, suture removal, mobilization, and discharge (Fig. 1). Nine general therapeutic interventions, seven assessments, five consultations, and all professional-orientated responsibilities were defined (Appendix Table 1). In the presence of osteomyelitis, an infectious disease specialist was also involved. The core team met monthly for coordination.

Treatment principles and milestones in the “ Basel Decubitus Approach”. Authors own work, copyright @anke.scheel-sailer
Third, consensus conferences were held with experts from all disciplines involved (physician specialists for paraplegiology; a plastic surgeon; an infectiologist; nurses; physio-, occupational and nutritional therapists; and a psychologist) to review the first draft and describe the use case based on key principles of the Basel Decubitus Approach. Several adaptations were necessary, including feedback systems, dependencies between different sub-processes, the need and controlling for assessments, consultations, and visibility.
Fourth, IT specialists were responsible for converting the use case into a BPMN. The CDSS was pilot tested in three cases with the responsible interprofessional team during the pre-test period. The core team participated in weekly meetings in which they demonstrated and documented the treatment procedures. After the pilot testing, dependencies between suture removal and changes in mattresses were no longer automatically connected due to frequent individual changes. In the CDSS, three key aspects of the process were visible: treatment elements, consultations, and milestones (Appendix Fig. 2). HCPs could see an overview of the entire process: they could click on the CDSS picture in a field showing the different treatment elements and were led to prescribe different specialist consultations and therapies. As soon as these consultations were prescribed, the color of the field in the process picture turned green. Once all consultations and therapies were prescribed, the color in the overview level also changed to green. The development of the CDSS required about 300 hours of interprofessional engagement and about 10,000 hours of IT work.
Implementation of the CDSS
When the development phase was completed, the involved interprofessional teams were informed, and a specific training program based on a structured manual was organized in June 2016. Specifically, the core team offered three interprofessional team information events, which lasted about 60 minutes each, with representatives of all professions (junior physicians, senior consultants, nurses, physio- and occupational therapists, social workers, and psychologists). In addition, individual support was offered on demand.
Patient-related data collection
The following data were gathered manually from the hospital records: patient, SCI, and PI characteristics; osteomyelitis; examinations; and interventions as they were defined as milestones and outcome parameters (minor and major complications, length of stay). The following information on examinations, interventions, and milestones was collected: SCI neurological impairment based on the International Standard for Neurological Classification in SCI (ISNCSCI), electrocardiogram, pulse oximetry, spirometry, nutrition laboratory, and range of motion. To monitor the treatment process and adherence to the Basel Decubitus Approach, we collected data on the prescription of plastic surgery consultation; physical, occupational, nutritional, psychological, music, and/or art therapy; the beginning of physical, occupational, nutritional, psychological, music, and/or art therapy; the performance of flap surgery; leg movement; and first mobilization in a wheelchair. The workload of physicians per patient was documented in five-minute steps for different tasks (direct patient contact, interprofessional exchange, documentation). Complications were divided into four categories: no complications, minor complications (prolonged bedrest), and major complications (re-surgery) directly related to the surgical intervention and other independent complications, such as pneumonia or urinary tract infection.
Cost analysis/calculation
The length of hospital stay was used to calculate the total costs, as the reimbursement included day taxes. Individual real hospital costs were collected as patient cost calculations performed by the finance department. Specific treatment costs were analyzed in terms of the costs of plastic surgical care, therapies, nursing, laboratory medical examinations, medication, and physicians’ time.
Statistical analyses
Categorical variables were presented with absolute and relative frequencies separately for the CDSS group, the control group, and all patients. Continuous variables were presented with mean or median lower and upper quartiles for each group. The continuous variables were divided into respective categories, ranging from normal to slightly deviant to strongly deviant values: body mass index (BMI) (< 17, 17–24, > 24 m/kg2) [35], hemoglobin (< 80, 80–120, < 120 g/l), vitamin D (< 30, 30–75, > 75), and glomerular filtration rates (GFR) (< 30, 30–90, > 90 mm/l). A time-to-event analysis was carried out to assess the mean time between admission and milestones or interventions of the Basel Decubitus Approach between the CDSS and control groups. P-values for the group comparisons were computed using chi-square tests and Fisher’s exact test for categorical variables. We used the unpaired two-sample t-test for continuous variables. The alpha level for statistical significance was set at 0.05. Data preparation and statistical analysis were conducted using Stata SE 15 (Stata for Windows, College Station, TX, USA).
Evaluation of the user perspective
In November and December 2017, we conducted four profession-specific focus groups (junior physicians, nurses, physio- and occupational therapists, and senior consultants) with five to eight participants, which lasted approximately 60 minutes each (Appendix Table 3). All participants had experience with the CDSS during the pilot testing. The semi-structured interview guide covered questions concerning experiences (“What experience have you had using the process management system?”), possibilities (“What tasks should such a system perform?”), and challenges (“What negative impact could such a system have on your activities?”) related to the newly implemented CDSS. These focus groups were audio recorded, transcribed verbatim, anonymized, and thematically analyzed [35]. We encoded the data using ATLAS.ti software (ATLAS.ti Scientific Software Development GmbH, Berlin, Germany). KK, PL, and AS-S grouped the obtained codes into subthemes and identified recurring themes through an iterative process.
Results
Patient and disease characteristics
Each group had 15 patients, and no dropouts occurred during the observation period. The patient characteristics are presented in Table 2. Twenty-two participants were male (73%), and the mean age was 56 years (interquartile range: 42–70 years). The two groups were equally distributed in terms of demographic factors. Nineteen patients had a complete SCI (63%), and 11 had a cervical SCI (37%). Comorbidities, such as diabetes, hypertonia, and renal failure, were equally frequent between the groups. Time since injury (means of 18 and 23 years in the CDSS and control groups, respectively) and BMI (means of 20.8 kg/m2 and 24.6 kg/m2 in the CDSS and control groups, respectively) were similar between the groups (Table 2).
Clinical outcome: Complication rates
PI characteristics, including the localization (n = 19 PI over the ischium [63%]), recurrence (21 patients, 70%), treatment with a rotation flap (12 patients, 40%), and treatment with a posterior thigh flap (15 patients, 50%), did not statistically differ between the groups (Table 3). The five major (16%) and nine minor (39%) complications were distributed similarly between the groups. Likewise, the length of stay (90 days on average) as well as the overall and detailed intervention costs did not differ significantly between the groups (Appendix Table 4).
Treatment approach adherence
A trend toward more prescriptions of therapies and examinations was observed under the CDSS (Table 4). For example, physical and occupational therapy was prescribed to 15 patients (100%) in the CDSS group and 13 patients (87%) in the usual care group; however, therapy took place in both groups equally (Table 3). Psychology was prescribed in 12 patients (80%) in the CDSS group compared to nine patients (60%) in the usual care group. The beginning of psychological treatment differed less between the CDSS group (mean 13.4 days; confidence interval (CI) 8.3–18.4) and the usual care group (mean 27.6 days; CI 6.1–49.0). Pulse oximetry, as an example of an examination, was conducted in seven patients (47%) in the CDSS group compared to five (33%) in the usual care group. All examinations were performed in accordance with the Basel Decubitus Approach. There was no statistically significant difference in the proportion of patients in the CDSS group vs. the control group regarding the prescription of additional therapies, such as psychological or nutritional therapy (Table 4).
Feedback from healthcare professionals and evaluation of user perspectives
The focus groups included 30 HCPs (26 female, 87%), consisting of eight nurses, six physiotherapists, three occupational therapists, seven junior physicians, and six senior consultants with 405 collective years of work experience and, more specifically, 231 collective years of work experience in this clinic (Appendix Table 3). Participants in all groups mentioned topics concerning IT process requirements and workload, clinical relevance, and the meaningfulness of the CDSS (Table 5). A benevolent willingness to use the CDSS became apparent (Questions [Qs] 1, 2, and 3). Participants acknowledged that the CDSS supported the use of guideline recommendations (Q4). Moreover, the HCPs expressed their awareness of directing the system, that is, that they could use it and adapt it individually if needed (Q5). While different HCPs underlined the opportunity to obtain a good interprofessional overview using the CDSS (Q6), others criticized what they regarded as a poor overview (Q7). HCPs often felt that the level of detail was too high (Qs 8 and 9).
All HCPs complained about the high time effort required for the active maintenance of the CDSS (Q10), the slowness of the IT system (Q11), and the instability of the IT system (Q12). The whole process was not automatically initiated or self-explanatory (Q13). Automatic reminders were not yet technically feasible (Q14). An immense problem appeared concerning the duplicity in the documentation. Since different IT systems were used in parallel, information had to be documented in different places (Qs 15, 16, 17, and 18). However, collected data could not be automatically displayed in different places and used in different processes (Q19).
HCPs could not develop a clinical management routine due to the rare use of CDSS with only a small number of patients per ward (Q20). Therefore, the CDSS did not noticeably support information exchange in staff shift changes (Q21). For some users, the purpose of the CDSS was perceived as limited to collecting data for research, leading to less motivation and more resistance to its use (Qs 19 and 22). Finally, HCPs were accustomed to paper-based process management (Q23) and did not experience improved quality when using the CDSS (Q24), only a compulsory task (Q25).
The feasibility study stopped in June 2017 because the management board finished the use of this specific IT system due to high costs, an inability to manage the interfaces, a lack of applicability to all IT users in the clinic, and the inability of the IT company that developed the system to fulfill all requirements. The management board finally decided to use another IT system in the whole clinic and to stop the use of this specific IT system that had explicitly developed the CDSS. Therefore, the developed CDSS could no longer be used for clinical management.
Discussion
To the best of our knowledge, this is the first feasibility study on the use of a CDSS in the treatment of PI in patients with SCI. The prescriptions and therapies were carried out almost equally in both groups. Nevertheless, in the CDSS group, the prescriptions and therapies generally started earlier than in the control group. The use of the CDSS did not significantly improve clinical and economic outcomes during this observation period. All HCPs showed interest in the CDSS and a willingness to integrate it into their clinical routine. HCPs endorsed the CDSS as a way to improve the quality of patient care by integrating guideline recommendations, allowing individual adaptations, and supporting interdisciplinary and interprofessional treatment. However, technical difficulties and time-consuming tasks characterized the use of the CDSS, which hindered its use as an extra IT system.
Different attitudes and principles between the clinical and the IT management group became apparent [3] in the monthly discussions of the core team. The importance of mutual understandings of the perspectives of the interprofessional clinical team and the IT team during the development process was evident during the consensus conferences [3]. As reported in the literature, clinical decision-making is characterized by its complexity and flexibility in adapting to individual patients’ situations. This appeared to contradict the IT logic of clear and linear causalities and predictable dependencies [3]. To overcome the challenge of these different professional perspectives and work methods, it was necessary to elaborate the benefits of a consensus based clinical management and to clarify the most relevant aspects of the treatment approach and interprofessional coordination. The interprofessional dependencies between activities of different professions had to be clearly defined to transform the collaborative processes into a clear IT logic. This study demonstrated that use case development was feasible in this interdisciplinary and interprofessional treatment process [3] when detailed information about the interprofessional and interdisciplinary interventions, milestones, and treatment elements could be elaborated [17, 19]. The relevant milestones and treatment elements in the Basel Decubitus Approach include debridement, surgical procedures, diagnosis and treatment of osteomyelitis, time of immobilization, and the respective start of mobilization, risk analyses, and additional interventions based on the biopsychosocial model.
The overall goal of this feasibility study, as part of a quality improvement project using a CDSS, was to optimize clinical processes and, consequently, clinical outcomes [10]. Our study hypothesis was that the use of the CDSS would increase the quality of treatment, including optimal coordination, intervention, and risk prevention, and thus reduce complication rates and lengths of stay. However, the use of the CDSS did not result in a reduction in complication rates, time expenses of physicians, total cost per patient, or hospitalization time. Regarding the latter, there are many possible explanations. We had to stop the use of the CDSS at the end of the pilot phase due to the transition to another IT system that did not include the specially developed Decubitus process. This led to a relevant loss of knowledge and induced high costs. Furthermore, due to the complex health conditions of the patients and the high rate of complications, the effect of CDSS-supported care might take longer to show effects on complication rates by changing the whole culture of process management [1]. The implementation took place in a team with an established culture that had worked with paper-based structures for many years. The paper-based management was faster and more established than IT-based interprofessional solutions [10]. The slightly earlier prescription of therapies (e.g., psychology or nutritional therapy) in the CDSS group vs. the control group might be explained by the fact that during the initial acute phase of stage III/IV PI treatment, the main focus is on plastic surgery and wound care. In contrast, the Basel Decubitus Approach integrates long-term secondary prevention, such as complex risk analyses, from the beginning. These therapies are often forgotten when usual care is applied, whereas a CDSS can lead the HCPs to perform treatment in a complex way right from the beginning. In the treatment course, the members of the interprofessional team remember the necessary missing therapies, so they are then registered in the course in line with recommendations [25]. A CDSS may be more useful for inexperienced teams with restricted collaboration time when HCP turnover increases [3]. In the future, as the shortage of experienced HCPs becomes a problem for health systems, CDSS-based treatment may become more important.
The CDSS was judged as relevant and feasible by the HCPs [9], but different challenges hindered the successful integration of this project into the clinical routine. As reported in previous studies [9], IT problems, the rare use of the CDSS in the treatment of stage III/IV PI, and the increased time required for additional documentation overshadowed the positive aspects of this project [6]. Further, HCPs’ engagement with and acceptance of the CDSS decreased because the main advantage of automatic data use for different purposes was not yet possible, and analysis of big data using the CDSS data was not achieved [36].
Although some participants showed a willingness to use the CDSS, we found that misunderstandings about the purpose of the CDSS contributed to resistance by others. HCPs were disappointed with the CDSS because they interpreted its use as part of a scientific study and not as a means to improve clinical management. This underlines the importance of effective communication with users to reduce misunderstandings and resistance in a pilot study as part of a quality improvement project [37].
Although the CDSS demonstrated some advantages that could lead to future improvements in process-based clinical care, the decision regarding its implementation should be made carefully given the high investment in terms of costs and workload [3]. The commitment from different professions, the support from the executive board of the clinic, and the cultural change in the clinic to a process-based organization were helpful [3]. However, it appeared that several learning cycles were necessary to change clinical management to process management and to develop the adequate IT capacity. The knowledge gained in the development of the Basel Decubitus Approach could be transferred to other CDSS implementation in the clinical setting. Furthermore, the findings can be applied to other complex care settings.
Study limitations
There are some limitations that should be mentioned. First, this CDSS development and implementation was the only project in the clinic that used a CDSS in an extra IT system [10, 36]. Consequently, the implementation was hindered by the infrequent use of the application [10, 36]. Integration in a broader context and different quality initiatives could have increased its impact. Second, the small sample size of the study is one of the main limitations of the analysis of this CDSS. Because a new IT system for the whole clinic was introduced soon after, the CDSS was not further developed. Third, the experiences of this CDSS project were influenced by the disappointing perception of spending money on an IT system that was subsequently abandoned. This included the complete development of this new clinic information software system. Nevertheless, the analyses of the HCPs’ perspectives and clinical parameters led to a comprehensive description of the project and can be used for further development projects.
Conclusion
We demonstrated that the implementation of a CDSS was feasible for complex treatment procedures, such as the treatment of stage III and IV PI in people with SCI. Milestone adherence, time to prescribe, and cost capture can be used as quality indicators of the implementation. HCPs’ perspectives should always be integrated into the implementation processes, especially in clinical processes with low evidence and a need for consensus-based management. The IT processes should include reminder systems, allow multiple data use for different purposes, and provide high-speed performance to increase the acceptance by HCPs. We learned that other factors, such as the time required for training and integration with existing information systems, were also important for successful implementation and that implementation is akin to cultural development.
Availability of data and materials
Datasets used and analyzed during the current study are available from the corresponding author on reasonable request. All personal identifiers were removed from the dataset.
Abbreviations
- BPMN:
-
Business Process Modeling Notation
- CDSS:
-
Clinical Decision Support System
- PUAP:
-
European Pressure Ulcer Advisory Panel
- HCPs:
-
Healthcare Professionals
- ICF:
-
International Classification of Functioning Disability and Health
- PI:
-
Pressure Injury
- SCI:
-
Spinal Cord Injury
References
Rotter T, Kinsman L, James E, Machotta A, Gothe H, Willis J, et al. Clinical pathways: effects on professional practice, patient outcomes, length of stay and hospital costs. Cochrane Database Syst Rev. 2010;(3):CD006632. https://doi.org/10.1002/14651858.CD006632.pub2. PMID: 20238347.
Goodwin-Wilson C, Watkins M, Gardner-Elahi C. Developing evidence-based process maps for spinal cord injury rehabilitation. Spinal Cord. 2010;48(2):122.
Haynes RB, Wilczynski NL. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: Methods of a decision-maker-researcher partnership systematic review. Implement Sci. 2010;5(1):12.
Hunt DL, et al. Effects of computer-based clinical decision support systems on physician performance and patient outcomes: a systematic review. JAMA. 1998;280(15):1339–46.
Garg AX, et al. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA. 2005;293(10):1223–38.
Kirschner S, et al. Klinische Pfade. Orthopade. 2007;36(6):516–22.
Litvin CB, Hyer JM, Ornstein SM. Use of clinical decision support to improve primary care identification and management of chronic kidney disease (CKD). J Am Board Fam Med. 2016;29(5):604–12.
Dexter PR, et al. Effectiveness of computer-generated reminders for increasing discussions about advance directives and completion of advance directive formsa randomized. Controlled Trial Ann Internal Med. 1998;128(2):102–10.
Davidson TM, et al. Pilot evaluation of a tablet-based application to improve quality of care in child mental health treatment. Behav Ther. 2019;50(2):367–79.
Lau F, et al. A review on systematic reviews of health information system studies. J Am Med Informatics Assoc. 2010;17(6):637–45.
Litvin CB, et al. Adoption of a clinical decision support system to promote judicious use of antibiotics for acute respiratory infections in primary care. Int J Med Inform. 2012;81(8):521–6.
Jesus TS, et al. Person-centred rehabilitation: what exactly does it mean? Protocol for a scoping review with thematic analysis towards framing the concept and practice of person-centred rehabilitation. BMJ Open. 2016;6(7):e011959.
Panel, E.P.U.A.P.a.N.P.U.A. Prevention and treatment of pressure ulcer; quick reference guide 2009; 2009:2012. Available from: http://www.epuap.org/guidelines/QRG_Prevention_in_German.pdf. Cited 2012 30.11.
DeVivo M, Farris V. Causes and costs of unplanned hospitalizations among persons with spinal cord injury. Top Spinal Cord Inj Rehabil. 2011;16(4):53–61.
Jensen M, et al. Frequency and age effects of secondary health conditions in individuals with spinal cord injury: a scoping review. Spinal Cord. 2013;51(12):882–92.
Guihan M, et al. Comparing multicomponent interventions to improve skin care behaviors and prevent recurrence in veterans hospitalized for severe pressure ulcers. Arch Phys Med Rehabil. 2014;95(7):1246–1253.e3.
Tran BNN, et al. National perioperative outcomes of flap coverage for pressure ulcers from 2005 to 2015 using American College of Surgeons National Surgical Quality Improvement Program. Arch Plast Surg. 2018;45(5):418–24.
Kreutzträger M, et al. Outcome analyses of a multimodal treatment approach for deep pressure ulcers in spinal cord injuries: a retrospective cohort study. Spinal Cord. 2018;56(6):582–90.
Bamba R, Madden JJ, Hoffman AN, Kim JS, Thayer WP, Nanney LB, Spear ME. Flap reconstruction for pressure ulcers: an outcomes analysis. Plast Reconstr Surg Glob Open. 2017;5(1):e1187. https://doi.org/10.1097/GOX.0000000000001187.
Krause JS, Broderick L. Patterns of recurrent pressure ulcers after spinal cord injury: identification of risk and protective factors 5 or more years after onset. Arch Phys Med Rehabil. 2004;85(8):1257–64.
Wettstein R, et al. Local flap therapy for the treatment of pressure sore wounds. Int Wound J. 2013.
Gelis A, et al. French guidelines from PERSE, SoFCPRE and SOFMER for the medical and surgical management of pressure ulcers in persons with spinal cord injury. Ann Phys Rehabil Med. 2018;61(5):352–4.
Wong D, Holtom P, Spellberg B. Osteomyelitis Complicating Sacral Pressure Ulcers: Whether or Not to Treat With Antibiotic Therapy. Clin Infect Dis. 2018;68(2):338–42.
Rigazzi J, et al. Osteomyelitis and antibiotic treatment in patients with grade IV pressure injury and spinal cord lesion-a retrospective cohort study. Spinal Cord. 2022;60(6):540–7.
Lussi C, et al. Nutritional blood parameters and nutritional risk screening in patients with spinal cord injury and deep pressure ulcer—a retrospective chart analysis. Spinal Cord. 2018;56(2):168.
Fähndrich C, et al. Treatment approaches of stage III and IV pressure injury in people with spinal cord injury: a scoping review. J Spinal Cord Med. 2022:1–11. https://doi.org/10.1080/10790268.2022.2108645 Epub ahead of print. PMID: 36129337.
Luscher NJ, et al. The sensory tensor fasciae latae flap: a 9-year follow-up. Ann Plasue Surg. 1991;26(4):306–10.
Rieger U, et al. Six treatment principles of the basle pressure sore concept. Handchir Mikrochir Plast Chir. 2007;39(3):206–14.
Meier C, et al. Treatment and cost of pressure injury stage III or IV in four patients with spinal cord injury: the Basel Decubitus Concept. Spinal Cord Series Cases. 2019;5:30.
Scheel-Sailer A, et al. Dekubitus – ein Update. Schweiz Med Forum. 2016;16(23):489–98.
Excellence, N.I.f.H.a.C. Pressure ulcers: prevention and management of pressure ulcers. 2014; Available from: http://www.nice.org.uk/guidance/cg179/resources/guidance-pressure-ulcers-prevention-and-management-of-pressure-ulcers-pdf. Cited 2014 29-09.
Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. PAFS consensus group. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239. https://doi.org/10.1136/bmj.i5239 PMID: 27777223; PMCID: PMC5076380.
Eldridge SM, Lancaster GA, Campbell MJ, Thabane L, Hopewell S, Coleman CL, et al. Defining feasibility and pilot studies in preparation for randomised controlled trials: development of a conceptual framework. PLoS One. 2016;11(3):e0150205. https://doi.org/10.1371/journal.pone.0150205 PMID: 26978655; PMCID: PMC4792418.
Wanner MB, et al. Chirurgische Therapie des Decubitus. SWISS MED. 1995;17(7–8):10–5.
Mayring P. Qualitative inhaltsanalyse. Weinheim: Beltz; 2011.
Koutkias, V., J. Bouaud, and S.E.f.t.I.Y.S.o.D. Support, contributions from the 2017 literature on clinical decision support. Yearb MedInform, 2018. 27(01): 122–128.
Wong S, et al. Morbid obesity after spinal cord injury: an ailment not to be treated? Eur J Clin Nutr. 2013;67(9):998–9.
Acknowledgements
We thank the health care professionals for their participation in the focus group discussion. We also thank Eva Jankovic planning, organizing, and transcribing the focus groups as part of her master thesis.
Funding
The authors received no funding.
Author information
Authors and Affiliations
Contributions
All authors conceptualized the study. AS-S, KK, PL, CF, and AG collected the data and performed the statistical and qualitative analyses. All authors discussed the results and the clinical relevance. All authors drafted the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study complies with the principles of good clinical practice. The study is in accordance with the Declaration of Helsinki and has been approved by the local ethics committee. The observation study received a declaration of no objection by the Ethics Committee northwest/central Switzerland (EKNZ UBE-16/003) and patients who denied retrospective use of their data were excluded. We received a waiver from ethics committee that the consent was not necessary in this quality improvement project (EKNZ UBE-16/003). The qualitative project holds a declaration of no objection by the Ethics Committee northwest/central Switzerland (EKNZ UBE-16/003) for the focus group interviews. Participants gave their informed consent before participating in the study in written form.
Consent for publication
Not applicable.
Competing interests
All authors declared no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix Table 1.
List of use case elements and different milestones in the “Basel Decubitus Appraoch”.
Additional file 2: Appendix Fig. 2.
CDSS overview of treatment elements (3a), of consultations (3b) and milestones in the six-week mobilisation scheme (3c). (Figures are presented in German).
Additional file 3: Appendix Table 3.
Participants in focus groups (profession, working years in the specific profession, working years in this clinic).
Additional file 4: Appendix Table 4.
Length of stay and profession related time invest and costs.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Scheel-Sailer, A., Koligi, K., Lampart, P. et al. Effect of a computerized decision support system on the treatment approach of stage III or IV pressure injury in patients with spinal cord injury: a feasibility study. BMC Health Serv Res 23, 103 (2023). https://doi.org/10.1186/s12913-023-09045-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09045-y