
Abstract
Background
Healthcare workers (HCWs) is the high-risk group for COVID-19 infection due to increased workplace exposure. However, evidence of the disease burden and factors associated with severe COVID-19 infection among HCWs is limited. Therefore, this article aims to describe the prevalence of severe COVID-19 disease among HCWs in Sabah, Malaysia, and to determine the factors associated with severe COVID-19 infection.
Method
A retrospective cross-sectional study was carried out by assessing the data of COVID-19-infected HCWs in Sabah, Malaysia, from 1st March 2021 until 30th September 2021. Logistic regression analysis was used in this study.
Results
Three thousand and forty HCWs were diagnosed with COVID-19 from 1st March 2021 until 30th September 2021. Of the 3040 HCWs, 2948 (97.0%) HCWs were mild, whereas 92 (3.0%) were severe. The multivariate logistic regression model showed that severe COVID-19 among HCWs in Sabah was associated with those do not receive any COVID-19 vaccination (aOR 6.061, 95% CI 3.408 – 10.780), underlying co-morbidity (aOR 3.335, 95% CI 2.183 – 5.096), and female (aOR 1.833, 95% CI 1.090 – 3.081).
Conclusion
HCWs should strictly adhere to preventive measures, including vaccination, personal protective equipment, and early referral to a physician upon identifying severe COVID-19 infection. Early screening and aggressive co-morbidity treatment among HCWs are essential for public health practitioners to prevent severe COVID-19 disease. Regardless of co-morbidity status, HCWs should stay up to date with COVID-19 vaccination, including booster doses.
Similar content being viewed by others


Introduction
Since the pandemic of coronavirus disease 2019 (COVID-19) was declared by World Health Organization (WHO) on 11th March 2020, the healthcare system has been severely impacted [1, 2]. All healthcare workers (HCWs) must work to face the pandemic, even during the national lockdown. These phenomena affect all HCWs, both physically and mentally. Various literature stated that the COVID-19 pandemic had been associated with psychological consequences for HCWs, including stress, depression, anxiety, trauma, burnout, and even suicidal attempts [1, 3,4,5]. Another study showed that 36.5% of the HCWs working in UMMC experienced anxiety symptoms, while 29.5% reported depressive symptoms [4]. These harmful consequences of the pandemic on workers' mental health have prompted initiatives to prevent and control the problem through various mental health programs and religious coping [4, 5].
Besides being psychologically impacted, HCWs are also often considered a high-risk population for acquiring the infection as this population has frequent contact with COVID-19 patients and the risky working environment, such as treating patients in the indoor setting [6]. Despite becoming more resilient and improving occupational intervention to prevent infection among HCWs [7, 8], illness and death have profoundly affected the HCW. The previous report from the Italian health authority stated that 10.7% of overall COVID-19 cases were contributed by HCWs, with a rising number of deaths among medical doctors, nurses, nurse aides, and dentists [7]. In a large register-based cohort study among Scottish healthcare workers, HCWs and their households contributed to a sixth of COVID-19 cases [8]. A cohort study in the United Kingdom (UK) found that the essential workers, including HCWs, the risk of acquiring severe COVID-19 infection seven times greater compared to the non-essential workers (RR 7.43, 95% CI 5.52 to 10.00) [9]. Furthermore, the risk of disease among HCWs was more remarkable due to unprotected exposure to the infected individuals, involvement in aerosol-producing procedures, and contact with bodily secretions [10].
Severe COVID-19 infection can lead to long-term complications, including multisystem inflammatory syndrome, pulmonary fibrosis, and neurological manifestations [11,12,13,14,15,16]. Even though there is greater awareness and strict adherence to infection control measures, HCWs had a higher risk of severe COVID-19 infection than other occupations and general populations [17, 18]. Hence, it is crucial to study the factors associated with severe COVID-19 disease in HCWs. Therefore, this article aims to describe the prevalence of severe COVID-19 infection among HCWs in Sabah, Malaysia, and to determine the factors associated with severe COVID-19 disease.
Methods
Study design, location, and duration
A retrospective cross-sectional study was carried out by assessing the data of COVID-19-infected healthcare workers (HCWs) in Sabah, Malaysia from 1st March 2021 until 30th September 2021. Sabah is one of the biggest states in Malaysia, situated in the northern portion of Borneo Island. It shares its border with the Malaysian state of Sarawak, Vietnam, the Philippines, and Indonesia. Sabah has a geographical area of 73,904 km2 and is divided into 25 districts. The state's population is 3.9 million and it is among the state with lowest population density in the country (44 people/km2).
Study population
The study population involved all laboratory confirmed-COVID-19 infection among HCWs working in public healthcare facilities in Sabah that was registered from 1st March 2021 until 30th September 2021. The study was conducted when the COVID-19 vaccine (Pfizer BioNTech©) was available in Malaysia in February 2021. Thus, secondary data of infected HCWs after vaccination was available was collected. Registered infected HCWs represent all occupational categories working in Sabah government health facilities and confirmed by laboratory tests. Confirmed COVID-19 infection among HCWs was reported by the Occupational Safety and Health (OSH) unit from various government health facilities across Sabah state, including 24 hospitals, 25 area health offices, nine area dental offices, eight headquarters, and one public health laboratory in Kota Kinabalu, Sabah.
Data collection instruments and procedure
The data of HCWs that have been registered and confirmed COVID-19 were obtained from Public Health Division, Sabah State Health Department. The data contain sociodemographic characteristics, clinical characteristics, co-morbidity, occupational categories, COVID-19 patient work involvement, and probable source of infection. The data was collected through an investigation conducted by trained district health officials through phone call interviews. Two public health professionals provided continuous supervision and monitoring to ensure the quality of information collected to ensure completeness and consistency of data collected.
Data in patients' line-listing were extracted in Microsoft Excel format from 1st March 2021 until 30th September 2021. Data extracted were cleaned to remove any irrelevant observations before analyses were performed. All registered and confirmed COVID-19 HCWs in government health facilities were included, and any probable cases or notified but not registered cases were excluded from the analysis. The data analysis was done using Statistical Package for Social Science (SPSS version 22.0) software. The descriptive data were presented as mean ± standard deviation (SD). Univariate and multivariate logistic regression were used to analyze factors associated with COVID-19 severity. A value of p < 0.05 is considered statistically significant.
Outcome measures and operational definitions
Confirmed COVID-19 infections can be defined as a person who is either alive or dead with positive real-time reverse transcriptase polymerase chain reaction (RT-PCR) or a person who has positive rapid test kit antigen (RTK-Ag) in pre-determined areas/locality with the prevalence of COVID-19 > 10% [19]. The clinical specimens sent for RT-PCR and RTK-Ag were obtained from the nasopharyngeal swabs, sputum, tracheal aspiration, or bronchoalveolar lavage.
For vaccination status, complete vaccination means those HCWs who have completed two vaccination doses. The protected period was valid if the disease onset was after 14 days from the second dose vaccination. Whereas incomplete vaccination means the recipient only received one dose of vaccine or two doses but less than the reasonable protective period, 14 days.
Under the staff categories, there are several worker positions such as nurses, doctors, PPP (Penolong Pegawai Perubatan or Assistant Medical Officer), PPK (Pembantu Perawatan Kesihatan or Health Assistant), PPKP (Penolong Pegawai Kesihatan Persekitaran or Assistant Environmental Health Officer), PKA (Pembantu Kesihatan Awam or Public Health Assistant), Pharmacy staffs, dental staffs, and other workers categories. The PPP has a vital role as a paramedic to provide primary health care, accident and emergency services, administrative, and specific roles under certain departments such as orthopaedics, surgery, psychiatry, etc. Meanwhile, PPK's general function is as a basic healthcare provider, such as ensuring patients comfort, making patients' beds, preparing medical equipment, etc. PPKP and PKA have a public health role in investigating environmental or health hazards and subsequently taking action to eliminate or limit the risk.
For the 'probable source of infection' variable, the question was asked to the patient on how they got the infection, either from their patient or other healthcare staff (work related); or from their family members, housemates, or through social interaction (non-work related). Meanwhile, For the 'COVID-19 involvement' variable, the patients were asked if they had to manage any COVID-19 patients during the incubation period. Co-morbidities variable refers to any reported underlying health problems that their doctor diagnosed. The health problems include but are not limited to hypertension, diabetes, pregnancy, obesity, chronic lung disease, asthma, malignancy, HIV, chronic kidney disease, and chronic liver disease.
The study used mild and severe COVID-19 infection as binary outcome measures. Mild COVID-19 infection represents stages 1 and 2, whereas severe cases represent stages 3,4 and 5. The staging of COVID-19 infection was made through clinical evaluation by a clinical specialist combined with laboratory and imaging studies assessment. Each case was staged according to clinical severity; stage I: asymptomatic, stage II: symptomatic without pneumonia, stage III: pneumonia without hypoxia, stage IV: pneumonia with hypoxia requiring oxygen supplementation therapy and stage V: critically ill. The diagnosis and staging made were according to COVID-19 Management Guidelines in Malaysia [19].
Results
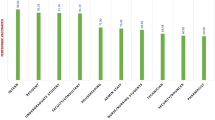
Three thousand forty (3040) healthcare workers (HCWs) were diagnosed with COVID-19 from 1st March 2021 until 30th September 2021. Of the 3040 HCWs, 2948 (97.0%) HCWs were mild, whereas 92 (3.0%) were severe (Table 1). About 2821 (92.8%) of the HCWs were vaccinated completely compared to incomplete vaccination (92, 3.0%) and not vaccinated at all (127, 4.2%), even though they were eligible. Among the positive HCWs, most were female (68.5%). HCWs with no co-morbidity contributed 2234 (73.5%) compared to those with co-morbidity, 806 (26.5%). Among the positive HCWs, nurses contributed the highest number, which is 1271 (41.8%), followed by medical assistants 527 (17.3%), doctors (256, 8.4%), inspectorate (146, 4.8%), dental (122, 4.0%), pharmacy (87, 2.9%) and other categories 631 (20.8%) such as administration, engineers, and laboratory personnel. Non-work related positive HCWs contributed 2383 (78.4%), and work-related were 657 (21.6%).
The dependent variable in this study is the staging of COVID-19 disease, which is mild and severe. There are seven independent variables: age, gender, staff categories, COVID-19 vaccination status, co-morbid, involvement in COVID-19 work, and source of infection. From the univariate logistic regression (Table 2), four variables are considered included in the multivariable logistic regression model using p-value < 0.25: age, gender, COVID-19 vaccination status, and co-morbidity.
After the four variables (age, gender, COVID-19 vaccination, and co-morbid) were included in the multivariable logistic regression model, only three variables were statistically significant (p-value ≤ 0.05), which is gender, COVID-19 vaccination and co-morbid (Table 3). The multivariable logistic regression model showed that severe COVID-19 among HCWs in Sabah was associated with those do not receive any COVID-19 vaccination (aOR 6.061, 95% CI 3.408 – 10.780), underlying co-morbidity (aOR 3.335, 95% CI 2.183 – 5.096), and female (aOR 1.833, 95% CI 1.090 – 3.081. The model has a satisfactory fit with a classification table of 97%.
Discussion
Severe COVID-19 infection among healthcare workers (HCWs) in Sabah contributed to 92 cases from 3040 total COVID-19 diseases in this study which is 3.0%. The incidence of severe COVID-19 illness among the current study population is lower than in previous studies, with around 5% to 9.9% incidence of severe disease among HCWs, as reported in meta-analyses [20, 21]. The occurrence of severe infection in the current study is also lower than the reported severe infection among all COVID-19-positive patients. For example, a survey among hospitalized patients in France reported that 41% with severe diseases, including 32% requiring ICU admission and 11% deaths [22]. A similar finding also was documented in a study among patients admitted to a tertiary medical centre, where 74 (37.6%) patients required intubation [23]. The inconsistency of the prevalence is because HCWs might have better awareness regarding COVID-19 infection. Furthermore, greater access to testing facilities also enables the population to be identified earlier, allowing early treatment of the disease.
The current study identified several independent risk factors associated with severe COVID-19 infection among HCWs. The female gender is significantly associated with a greater risk of having severe COVID-19 disease than the male. However, the finding is inconsistent with previous studies that identified infected males as more likely to get severe COVID-19 infection than females [22, 24,25,26,27]. Conflicting results in the current study might be explained by the imbalance in proportions of sex differences among all COVID-19 patients and among HCW. In the present study population, almost 70% of infected HCWs were female, most of whom were nursing staff. The more significant proportion of nursing staff in the current study might hinder the effect of the male gender on severe COVID-19 infection. Furthermore, the previous study also found the association of the male gender with severe COVID-19 illness is weak [25,26,27,28]. In a physiological context, females have a higher copy number of immune-related genes, providing a more robust immune response, leading to high-stress endurance levels and better viral clearance. Consequently, lower mortality was observed [29].
Co-morbidity was also significantly associated with severe COVID-19 infection among HCWs. The current study found that HCWs with co-morbidity have a three times greater risk of acquiring severe COVID-19 infection than those without co-morbidity. Previous studies reported that co-morbidity such as immunosuppression [22, 30], diabetes [22, 25, 27, 28, 30, 31], hypertension [26, 28], acute or chronic kidney disease [22, 23], chronic obstructive pulmonary disease [31], bronchial asthma [25, 30], and gastrointestinal condition [27, 28, 30] were associated with severe COVID-19 infection and death. Furthermore, the previous study also similarly found that patients with haematological co-morbidities such as acute myeloid leukaemia (3·49, 1·56–7·81), indolent non-Hodgkin lymphoma (2·19, 1·07–4·48), aggressive non-Hodgkin lymphoma (2·56, 1·34–4·89), and plasma cell neoplasms were associated with worse COVID-19 survival [32]. Previous meta-analyses found that severity is most remarkable in patients with a history of cerebrovascular disease: OR 4.85 (95% CI: 3.11–7.57), cardiovascular disease: OR 4.81 (95% CI: 3.43–6.74), chronic lung disease: OR 4.19 (95% CI: 2.84–6.19), and cancer: OR 3.18, 95% CI: 2.09–4.82 [33]. The high prevalence of co-morbidity among infected HCWs in our study requires urgent intervention to protect the affected HCWs from serious sequelae of COVID-19 infection, including long COVID-19 syndrome, acute respiratory distress syndrome (ARDS), multi-organ failure, septic shock, and death [34, 35].
Vaccination is one of the essential public health interventions to prevent severe COVID-19 infection. The current study found that HCWs who are unvaccinated or had incomplete vaccination history are more likely to have severe COVID-19 disease by two to six times respectively, than those who had completed COVID-19 vaccination. The finding is supported by a previous study that found that receiving at least two doses of vaccination reduces the risk of hospital admission by 93%, 92% for severe COVID-19, and 81% for COVID-19-related deaths [36]. This finding further underscores the importance of vaccination among HCWs and those with co-morbidities [37]. A recent study also highlights the importance of third-dose mRNA vaccination in protecting individuals against severe COVID-19-related outcomes [36].
Previous studies among the general population have found that advancing age, especially greater than 60 years old, was an independent risk factor for severe COVID-19 infection and deaths [22, 25,26,27]. The elderly population is at high risk for severe COVID-19 disease because they have weakened immunity and viral-induced cytokine storms, resulting in life-threatening respiratory failure and multisystemic involvement [38]. Since HCWs are among productive age groups, the age factor was not significantly associated with severe COVID-19 infection in the current study. In the present study, even though the age factor is not a significant concern, these populations must be regularly screened for co-morbidity, especially before retirement, to protect them when they enter high-risk age groups. The current study also found that the various HCW professions and probable sources of infection were not significantly associated with severe COVID-19 disease. However, in past literature, it was observed that HCWs working at the front door, intensive care unit and aerosol-generating procedure settings were associated with hospital admission [8]. The inconsistency of findings with the current study might be because the present study did not stratify the staff's background, as some HCWs might not work directly with COVID-19 patients. Furthermore, the current study also identified that most of the infection originated from non-work-related conditions.
From the study, there are several recommendations. Assessing awareness and practice regarding preventive measures against COVID-19 might help determine the need for tailored health education programs among HCWs to improve the appropriate method of COVID-19 prevention practices [39]. With the advancement of technology and computer science, the current surveillance system for early detection of COVID-19 infection among HCWs could be improved through disruptive technology such as the Internet of things, artificial intelligence, and blockchain [40]. Previous research has reported that ventilation is essential in transmitting infectious diseases, such as severe acute respiratory syndrome and influenza [41]. Therefore, a future study in assessing indoor air quality in healthcare settings might be needed to determine the potential neglected source of infection with subsequent intervention to improve ventilation. For HCWs, strict adherence to preventive measures, including vaccination, early and self-referral to the physician upon identification of severe COVID-19 infection may help to prevent further progression and complications of COVID-19. For public health practitioners, early screening and treatment of co-morbidity are of utmost importance for preventing severe COVID-19 infection among HCWs. HCWs with uncontrolled co-morbidities are the group to be prioritized to get the vaccination. Occupational health policy emphasizing the protection of HCWs from COVID-19 infection should be prioritized in public and private healthcare facilities.
This study is not without limitations. A cross-sectional study design where the data was collected at a single time point and the association between predictors and outcome may not be taken as an indication of causality, and reverse causality is possible. Furthermore, because of the retrospective nature of this study, some of the critical variables, especially potential confounders such as the laboratory, inflammatory, infection markers, and behavioural risk factors, were unavailable. In addition, a possible lack of detailed clinical data and self-reporting of co-morbidity could limit our findings. Thus, some variables' role in predicting severe COVID-19 infection could have been underestimated. Nonetheless, the heterogenicity of our study population, involving all healthcare staff regardless of whether they work in clinical or non-clinical practice, provides valuable information on potential predictors of severe disease in the population.
Conclusion
In conclusion, the study has elucidated the list of vulnerable populations among HCWs that predicted severe COVID-9 infection, including gender, vaccination status, and co-morbidity. The findings from our study have several implications for various stakeholders, such as HCWs, public health practitioners, policymakers, physicians at healthcare facilities, and intensive care physicians. Regardless of the co-morbidity status, the HCW are recommended to stay up to date with their COVID-19 vaccination, including booster doses. Strict adherence to preventive measures and occupational health policy is of the utmost importance to prevent severe COVID-19 infection among HCWs.
Availability of data and materials
The datasets obtained for this study are not publicly available to protect patients' confidentiality. Any interested parties may request related information from Malaysian Ministry of Health or directly from the first author (carolimkj@gmail.com) on reasonable request.
References
Roslan NS, Yusoff MSB, Asrenee AR, Morgan K. Burnout prevalence and its associated factors among malaysian healthcare workers during covid-19 pandemic: an embedded mixed-method study. Healthc. 2021;9(1):90.
Wu JT, Leung K, Bushman M, Kishore N, Niehus R, de Salazar PM, et al. Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan. China Nat Med. 2020;26(4):506–10.
Buselli R, Corsi M, Baldanzi S, Chiumiento M, Del Lupo E, Dell’oste V, et al. Professional quality of life and mental health outcomes among health care workers exposed to Sars-Cov-2 (Covid-19). Int J Environ Res Public Health [Internet]. 2020;17(17):1–12 Available from: /pmc/articles/PMC7504107/. [Cited 2022 14th March].
Chow SK, Francis B, Ng YH, Naim N, Beh HC, Ariffin MAA, et al. Religious coping, depression and anxiety among healthcare workers during the covid-19 pandemic: a Malaysian perspective. Healthc. 2021;9(1):79.
Raudenská J, Steinerová V, Javůrková A, Urits I, Kaye AD, Viswanath O, et al. Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract Res Clin Anaesthesiol. 2020;34(3):553 Available from: /pmc/articles/PMC7367798/. [Cited 2022 14th March].
COVID-19 clusters and outbreaks in occupational settings in the EU/EEA and the UK. https://www.ecdc.europa.eu/en/publications-data/covid-19-clusters-and-outbreaks-occupational-settings-eueea-and-uk. Available from: [Cited 2022 14th March].
Lapolla P, Mingoli A, Lee R. Deaths from COVID-19 in healthcare workers in Italy—What can we learn? Infect Control Hosp Epidemiol. 2021 Mar 1 [cited 2022 Mar 14];42(3):364–5. Available from: https://www.cambridge.org/core/journals/infection-control-and-hospital-epidemiology/article/deaths-from-covid19-in-healthcare-workers-in-italywhat-can-we-learn/BDA8BA987868E2B86B50F0D070496827.
Shah ASV, Wood R, Gribben C, Caldwell D, Bishop J, Weir A, et al. risk of hospital admission with coronavirus disease 2019 in healthcare workers and their households: nationwide linkage cohort study. BMJ. 2020 28th October [cited 2022 14th March];371. Available from: https://www.bmj.com/content/371/bmj.m3582.
Mutambudzi M, Niedwiedz C, Macdonald EB, Leyland A, Mair F, Anderson J, et al. Occupation and risk of severe COVID-19: prospective cohort study of 120 075 UK Biobank participants. Occup Environ Med. 2021 May 1 [cited 2022 Mar 14];78(5):307–14. Available from: https://oem.bmj.com/content/78/5/307.
Chou R, Dana T, Buckley DI, Selph S, Fu R, Totten AM. Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers: A Living Rapid Review. Ann Intern Med. 2020 Jul 21 [cited 2022 Mar 14];173(2):120–36. Available from: /pmc/articles/PMC7240841/.
Nuzzo D, Picone P. Potential neurological effects of severe COVID-19 infection. Neurosci Res. 2020;1(158):1–5.
Wang F, Kream RM, Stefano GB. Long-Term Respiratory and Neurological Sequelae of COVID-19. Med Sci Monit. 2020 1st November [cited 2022 7th May];26:e928996–1. Available from: /pmc/articles/PMC7643287/.
Lang M, Buch K, Li MD, Mehan WA, Lang AL, Leslie-Mazwi TM, et al. Leukoencephalopathy Associated with Severe COVID-19 Infection: Sequela of Hypoxemia? Am J Neuroradiol. 2020 Sep 1 [cited 2022 May 7];41(9):1641–5. Available from: http://www.ajnr.org/content/41/9/1641.
Nardo AD, Schneeweiss-Gleixner M, Bakail M, Dixon ED, Lax SF, Trauner M. Pathophysiological mechanisms of liver injury in COVID-19. Liver Int. 2021 Jan 1 [cited 2022 May 7];41(1):20–32. Available from: https://onlinelibrary.wiley.com/doi/full/https://doi.org/10.1111/liv.14730.
Long B, Brady WJ, Koyfman A, Gottlieb M. Cardiovascular complications in COVID-19. Am J Emerg Med. 2020;38(7):1504–7.
Zoumot Z, Bonilla MF, Wahla AS, Shafiq I, Uzbeck M, El-Lababidi RM, et al. Pulmonary cavitation: an under-recognized late complication of severe COVID-19 lung disease. BMC Pulm Med. 2021 1st December [cited 2022 7th May];21(1):1–8. Available from: https://link.springer.com/articles/https://doi.org/10.1186/s12890-020-01379-1.
Mutambudzi M, Niedwiedz C, Macdonald EB, Leyland A, Mair F, Anderson J, et al. Occupation and risk of severe COVID-19: prospective cohort study of 120 075 UK Biobank participants. Occup Environ Med. 2021 May 1 [cited 2022 May 7];78(5):307–14. Available from: https://oem.bmj.com/content/78/5/307.
Antonio-Villa NE, Bello-Chavolla OY, Vargas-Vázquez A, Fermín-Martínez CA, Márquez-Salinas A, Pisanty-Alatorre J, et al. Assessing the Burden of Coronavirus Disease 2019 (COVID-19) Among Healthcare Workers in Mexico City: A Data-Driven Call to Action. Clin Infect Dis. 2021 Jul 1 [cited 2022 May 7];73(1):e191–8. Available from: https://academic.oup.com/cid/article/73/1/e191/5912602.
Home | COVID-19 MALAYSIA. [cited 2022 7th May]. Available from: https://covid-19.moh.gov.my/.
Sahu AK, Amrithanand VT, Mathew R, Aggarwal P, Nayer J, Bhoi S. COVID-19 in health care workers – a systematic review and meta-analysis. Am J Emerg Med. 2020;38(9):1727–31.
Gómez-Ochoa SA, Franco OH, Rojas LZ, Raguindin PF, Roa-Díaz ZM, Wyssmann BM, et al. COVID-19 in Health-Care Workers: A Living Systematic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am J Epidemiol. 2021 Jan 4 [cited 2022 Nov 20];190(1):161–75. Available from: https://academic.oup.com/aje/article/190/1/161/5900120.
Kaeuffer C, Le Hyaric C, Fabacher T, Mootien J, Dervieux B, Ruch Y, et al. Clinical characteristics and risk factors associated with severe COVID-19: Prospective analysis of 1,045 hospitalized cases in North-Eastern France, March 2020. Eurosurveillance. 2020 3rd December [cited 2022 15th March];25(48):2000895. Available from: https://www.eurosurveillance.org/content/https://doi.org/10.2807/1560-7917.ES.2020.25.48.2000895.
Bhargava A, Fukushima EA, Levine M, Zhao W, Tanveer F, Szpunar SM, et al. Predictors for Severe COVID-19 Infection. Clin Infect Dis. 2020 Nov 5 [cited 2022 Mar 15];71(8):1962–8. Available from: https://academic.oup.com/cid/article/71/8/1962/5848851.
Kumar A, Arora A, Sharma P, Anikhindi SA, Bansal N, Singla V, et al. Clinical Features of COVID-19 and Factors Associated with Severe Clinical Course: A Systematic Review and Meta-analysis. Soc Sci Res Netw. 2020 Apr.
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nat 2020 5847821. 2020 Jul 8 [cited 2022 Mar 15];584(7821):430–6. Available from: https://www.nature.com/articles/s41586-020-2521-4.
Shi Y, Yu X, Zhao H, Wang H, Zhao R, Sheng J. Host susceptibility to severe COVID-19 and establishment of a host risk score: Findings of 487 cases outside Wuhan. Crit Care. 2020 18th March [cited 2022 15th March];24(1):1–4. Available from: https://ccforum.biomedcentral.com/articles/https://doi.org/10.1186/s13054-020-2833-7.
Jiang N, Liu YN, Bao J, Li R, Ni WT, Tan XY, et al. Clinical features and risk factors associated with severe COVID-19 patients in China. Chin Med J (Engl). 2021 [cited 2022 Mar 15];134(8):944–53. Available from: www.cmj.org.
Kumar A, Arora A, Sharma P, Anikhindi SA, Bansal N, Singla V, et al. Clinical Features of COVID-19 and Factors Associated with Severe Clinical Course: A Systematic Review and Meta-analysis. Soc Sci Res Netw. 2020 Apr 22 [cited 2022 Mar 15]; Available from: /pmc/articles/PMC7366815/.
Pradhan A, Olsson PE. Sex differences in severity and mortality from COVID-19: are males more vulnerable? Biol Sex Differ. 2020 18th September [cited 2022 20th November];11(1):1–11. Available from: https://bsd.biomedcentral.com/articles/https://doi.org/10.1186/s13293-020-00330-7.
Graff K, Smith C, Silveira L, Jung S, Curran-Hays S, Jarjour J, et al. Risk Factors for Severe COVID-19 in Children. Pediatr Infect Dis J [Internet]. 2021 [cited 2022 15th March];E137–45. Available from: https://journals.lww.com/pidj/Fulltext/2021/04000/Risk_Factors_for_Severe_COVID_19_in_Children.2.aspx.
Li K, Wu J, Wu F, Guo D, Chen L, Fang Z, et al. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Invest Radiol. 2020 Jun 1 [cited 2022 Mar 15];55(6):327–31. Available from: /pmc/articles/PMC7147273/.
Passamonti F, Cattaneo C, Arcaini L, Bruna R, Cavo M, Merli F, et al. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: a retrospective, multicentre, cohort study. Lancet Haematol. 2020 1st October;7(10):e737–45.
Honardoost M, Janani L, Aghili R, Emami Z, Khamseh ME. The Association between Presence of Comorbidities and COVID-19 Severity: A Systematic Review and Meta-Analysis. Cerebrovasc Dis. 2021 Apr 1 [cited 2022 Nov 20];50(2):132–40. Available from: https://www.karger.com/Article/FullText/513288.
Proal AD, VanElzakker MB. Long COVID or post-acute sequelae of COVID-19 (PASC): an overview of biological factors that may contribute to persistent symptoms. Front Microbiol. 2021;12:1494.
Logue JK, Franko NM, McCulloch DJ, McConald D, Magedson A, Wolf CR, et al. Sequelae in Adults at 6 Months After COVID-19 Infection. JAMA Netw Open. 2021 Feb 1 [cited 2022 Mar 15];4(2):e210830–e210830. Available from: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2776560.
Barda N, Dagan N, Cohen C, Hernán MA, Lipsitch M, Kohane IS, et al. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: an observational study. Lancet. 2021;398(10316):2093–100.
Russell FM, Greenwood B. Who should be prioritized for COVID-19 vaccination?. 2020 [cited 2022 Mar 15];17(5):1317–21. Available from: https://www.tandfonline.com/doi/abs/https://doi.org/10.1080/21645515.2020.1827882.
Perrotta F, Corbi G, Mazzeo G, Boccia M, Aronne L, D'Agnano V, et al. COVID-19 and the elderly: insights into pathogenesis and clinical decision-making. Aging Clin Exp Res. 2020 Aug 1 [cited 2022 Mar 15];32(8):1599–608. Available from: https://link.springer.com/article/https://doi.org/10.1007/s40520-020-01631-y.
Sazali MF, Rahim SSSA, Mohamed MH, Omar A, Pang NTP, Jeffree MS, et al. Knowledge, attitude and practice on COVID-19 among students during the early phase of pandemic in a university in Borneo, Malaysia. J Public health Res. 2021 24th March [cited 2021 12th April];10:2122. Available from: https://jphres.org/index.php/jphres/article/view/2122.
Amir PN, Sazali MF, Salvaraji L, Dulajis N, Syed S, Rahim A, et al. Public health informatics in global health surveillance : a review. Borneo Epidemilogy J. 2021;2(December):74–88.
Tham KW. Indoor air quality and its effects on humans—a review of challenges and developments in the last 30 years. Energy Build. 2016;15(130):637–50.
Acknowledgements
We appreciate everyone who was involved in this study. We would also like to thank the Director-General of Health Malaysia for the permission to publish this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
KJL planned and directed this project under the supervision of VJG. KJL, MFS, MG, ACZ and MCMM were involved in the document review. KJL and MG performed the data cleaning and data analysis. KJL and RA performed in results interpretation. All authors contributed to the write-up, reviewed, and approved the final version of this manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All procedures in this study were conducted following the principles of the Declaration of Helsinki and the Malaysian Good Clinical Practice Guidelines. This study was registered with Malaysian National Medical Research Register. Informed consent is waived from the Malaysian Medical Research Ethics Committee (MREC) requirement. The ethical approval for this study was obtained from MREC, Ministry of Health Malaysia (Ethics Initial Approval: NMRR ID-21–02324-RAS). The patient's personal information was anonymized upon data extraction and analysis to protect subjects' confidentiality.
Consent for publication
Not applicable.
Competing interests
No potential conflict of interest was reported by the authors(s).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Joo, L.K., Sazali, M.F., Goroh, M. et al. Predictors of severe COVID-19 among healthcare workers in Sabah, Malaysia. BMC Health Serv Res 22, 1541 (2022). https://doi.org/10.1186/s12913-022-08920-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-022-08920-4