
Abstract
Background
Accreditation is viewed as a reputable tool to evaluate and enhance the quality of health care. However, its effect on performance and outcomes remains unclear. This review aimed to identify and analyze the evidence on the impact of hospital accreditation.
Methods
We systematically searched electronic databases (PubMed, CINAHL, PsycINFO, EMBASE, MEDLINE (OvidSP), CDSR, CENTRAL, ScienceDirect, SSCI, RSCI, SciELO, and KCI) and other sources using relevant subject headings. We included peer-reviewed quantitative studies published over the last two decades, irrespective of its design or language. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, two reviewers independently screened initially identified articles, reviewed the full-text of potentially relevant studies, extracted necessary data, and assessed the methodological quality of the included studies using a validated tool. The accreditation effects were synthesized and categorized thematically into six impact themes.
Results
We screened a total of 17,830 studies, of which 76 empirical studies that examined the impact of accreditation met our inclusion criteria. These studies were methodologically heterogeneous. Apart from the effect of accreditation on healthcare workers and particularly on job stress, our results indicate a consistent positive effect of hospital accreditation on safety culture, process-related performance measures, efficiency, and the patient length of stay, whereas employee satisfaction, patient satisfaction and experience, and 30-day hospital readmission rate were found to be unrelated to accreditation. Paradoxical results regarding the impact of accreditation on mortality rate and healthcare-associated infections hampered drawing firm conclusions on these outcome measures.
Conclusion
There is reasonable evidence to support the notion that compliance with accreditation standards has multiple plausible benefits in improving the performance in the hospital setting. Despite inconclusive evidence on causality, introducing hospital accreditation schemes stimulates performance improvement and patient safety. Efforts to incentivize and modernize accreditation are recommended to move towards institutionalization and sustaining the performance gains.
PROSPERO registration number CRD42020167863.
Similar content being viewed by others


Background
“To Err is Human,” a landmark report that was published by the Institute of Medicine (IOM) in 1999 [1], recommended reinforcement of quality and safety in healthcare [2]. The report suggested that quality is multifaceted and quality assessment is one of the driving forces to establish performance improvement [3, 4]. In response, various approaches have been employed globally to regulate healthcare quality internally and externally [5]. External review systems facilitate organizational change, enhance the quality of services, and strive toward quality standards [6]. Accreditation has been cited as the oldest and most common strategic external quality assessment tool in healthcare [7, 8].
It should be acknowledged that the embryonic seeds of hospital accreditation were planted a century earlier by the American College of Surgeons [9]. Since then, hospital accreditation programs have thrived ubiquitously and become an integral part of healthcare quality systems [10,11,12]. In the last two decades, many countries have adopted or adapted hospital accreditation systems [13].
Accreditation refers to the external peer review that evaluates a healthcare organization’s compliance against pre-defined performance standards [14], with the ultimate aim to improve healthcare quality [15]. It is overseen by various governmental and non-governmental entities, using different modalities in voluntary or mandatory approaches. The scope of accreditation can cover the entire healthcare facility or only a specialty or even a sub-specialty [6, 16]. Several leading international healthcare organizations have viewed accreditation as a valid marker of quality [12] and discussed the effectiveness of using accreditation standards as a tool to enhance organizational and clinical performance [17,18,19]. Nevertheless, the available evidence in the literature supporting this assumption remains scarce.
Despite the ostensible promising effect of healthcare accreditation [20, 21], the literature presents a complex view of its impact [22]. The legitimacy concerns about accreditation are due to the scant of high-quality trials and conflicting reported results [23,24,25]. Contradictory findings have generated inconsistency in the conclusions of previously published reviews [6, 12, 13, 23, 26,27,28,29,30,31,32,33,34,35]. On the one hand, positive impacts of hospital accreditation on organizational culture [12, 32, 34], clinical practice, organizational performance [23], clinical leadership, patient safety systems [28], quality of services [29], care delivery process [30], and efficiency [35] have been demonstrated. On the other hand, several reviews reported insufficient evidence pertaining to the impact of accreditation on measurable changes in quality of care [12], health outcomes [26], patient satisfaction [31], and economic outcomes [13, 26, 34]. For instance, Greenfield and Braithwaite [13] present diverging findings on the impact of accreditation as the effect was limited to promoting change and professional development, while on other impact categories such as quality measures, financial impact, and public disclosure results were inconclusive. In addition, some reviews questioned the cost-effectiveness of accreditation [6, 32, 33].
Previously published accreditation reviews included the impact of specialty [30] or disease-specific [34] accreditation programs which could dilute the overall impact of hospital accreditation, used stringent inclusion designs that could limit its contribution room [6, 12], restricted search languages, or overlooked several important relevant studies [35]. This review has overcome such hindrances and aimed to identify and analyze the evidence on the impact of hospital accreditation.
Methodology
Our review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [36], presented in Additional file 1. We verified that there was no running or completed systematic review like ours in Prospero and Health Systems Evidence (HSE) database at the commencing phase. Thereafter, we registered the protocol of our review as PROSPERO ID: 167863 on 04-Feb-2020 to avert “HARKing” [37].
Databases and search terms
Electronic bibliographic databases were searched systematically to retrieve relevant publications using relevant subject headings and controlled vocabulary terms, as shown in Additional file 2. Databases include; PubMed, CINAHL, PsycINFO, EMBASE, MEDLINE (OvidSP), ScienceDirect, Cochrane Database of Systematic Reviews (CDSR), Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science, including Social Sciences Citation Index (SSCI), Russian Science Citation Index (RSCI), SciELO Citation Index, and KCI-Korean Journal Database. The search reported here was effectuated by the primary author on 18-Feb-2020 after being reviewed by a specialist librarian.
Additionally, we searched Google Scholar using keywords in different combinations, including accreditation, hospital, quality, impact, and healthcare services. Furthermore, we scanned the websites of the most popular accreditation entities for additional papers that we might have overlooked.
Screening and eligibility assessment
We included full-text publications that evaluated the impact of overall hospital accreditation programs on the quality of healthcare services in the last two decades (i.e., since “To Err Is Human”) from January 2000 – February 2020. All quantitative studies were included irrespective of their design. No language restriction was added. Following the search, titles and abstracts were retrieved and uploaded into the bibliographic reference management software EndNote X9, and deduplicated. Thereafter, two authors (MH, MG) independently screened all titles and abstracts to identify potentially relevant articles and read the full text of relevant studies to assess eligibility. Studies were assessed for eligibility using the PICO criteria [38]: population— all types of hospitals; intervention— all types of overall accreditation; comparison— unaccredited hospitals, before-and-after, or different accreditation levels; outcomes— measurable impacts on the structure, process, or outcome parameters. At any stage, disagreement between the two authors was reunited by consensus or arbitration by a third author (MP).
We excluded unpublished/unindexed studies, review articles, or studies published in an “abstract” format. Studies conducted in healthcare settings other than hospitals, studies that evaluated the impact of accreditation on a specialty or disease-specific, or examined accreditation preparation cost were excluded. In addition, studies that assessed the perceived benefits of accreditation have been excluded. However, to evaluate the impact from different perspectives, comparative studies that examined accreditation effects on self-reported subjective outcome parameters (e.g., patient satisfaction, job stress) using a validated instrument were included.
A kappa inter-rater reliability (IRR) test was conducted to assess full-text assessment reliability [39, 40]. We randomly selected and matched a sample of 50 studies that were evaluated for inclusion by the two reviewers. Four differences were identified, which resulted in kappa 0.81, indicating a high agreement level.
Data extraction
Studies that met our inclusion criteria were interrogated independently by two authors using a standardized data extraction form, and its references were screened (i.e., snowballing) for additional potentially relevant studies. Details on the research designs, goals, findings, and conclusions were extracted and compiled for analysis. Occasionally, when information insufficiency hindered data extraction, it was solicited from the corresponding author. All relevant non-English-language studies were translated through Google Translate, which has been cited as a reliable tool for translating papers published in languages other than English in systematic reviews [41, 42]. For authenticity, we e-mailed the data extracted from the included non-English studies to the corresponding author for verification and stipulated obtaining confirmation for inclusion. Studies that did not meet our inclusion requirements were summarized along with the reason for exclusion, and records were preserved for audit trail purposes.
Quality assessment
In this review, the methodological precision of included publications was assessed using Hawker et al [43]. framework as it provides an appropriate unified scale for heterogeneous study designs. The instrument consists of nine items (namely; abstract and title, introduction and aims, method and data, sampling, data analysis, ethics and bias, findings, transferability, and implications and usefulness), each scored on a 4-point scale (1 = good; 2 = fair; 3 = poor; 4 = very poor). The overall grade was judged based on the average score of these items (1.00–1.49 = good, 1.50–2.49 = fair; 2.50–3.49 = poor; 3.50–4.00 = very poor) [44].
For each included study, the coders (MH, MG) independently assessed the methodological quality, assigned an appropriate score, and calculated the overall grade accordingly. To test the assessment credibility, a kappa IRR test was employed using 20 randomly selected assessed studies. A crosswalk between decisions revealed two disparities, resulting in kappa 0.8, which indicates a trustworthy agreement level [39, 40].
Analysis
For text mining [45], extracted data were synthesized and presented narratively using the thematic analysis [46]. The effects were categorized into six impact themes, that were reported in part or entirely in previous reviews [6, 12, 13, 26, 29, 32] and models [47]. In this review, the impact of accreditation was defined as a measurable marked effect that the accreditation process demonstrated, positively or negatively. The impact was judged to be positive if all or most of the results were significantly advantageous, negative if all or most of the results were unfavorable, or neutral when no real change due to accreditation was identified [26]. The impact themes were: changes in organizational culture and management; changes at professionals’ level; changes at the patient level; changes in patient clinical outcomes; changes in performance measures; and changes in economic outcomes. Each study was classified under one or multiple outcome themes.
Results
Search results
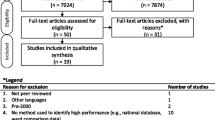
Our search identified 17,830 publications. Based on the title and abstract screening, 327 articles were deemed potentially eligible and retrieved for full-text review. Of these, 74 studies matched our inclusion criteria. This included seven non-English studies verified by their authors, while four other non-English studies were excluded due to no response to our verification request. Two additional studies were identified through screening the references of included articles, which yielded 76 studies for critical appraisal and analysis (see Fig. 1).

PRISMA flow diagram illustrating review process. * Self-reported subjective outcome parameter through a validated instrument, using comparative design
Features of the included studies
Additional file 3 summarizes the key findings of all studies included in our review. During the last decade, there has been a notable flourish in the number and spectrum of studies evaluating the impact of accreditation in the literature. Almost three fourths (n = 52) of the included studies were published during the last five years (2015–2019). The majority of studies were in English (n = 69). The seven verified and analyzed non-English studies were published in Persian, Danish, Korean, and Hungarian.
Included studies were conducted in 22 countries representing all inhabited continents. The highest number of studies were from the USA (n = 11) and Brazil (n = 9). Two studies were multinational, conducted in European hospitals [19, 28]. Studies evaluated the impact of 23 accreditation programs. The most studied scheme was the Joint Commission International Accreditation (JCIA) (n = 14). Twenty-one studies (28%) assessed the impact of accreditation in a single hospital, while the range was up to 4400 hospitals.
Assessment of the methods used
In our review, many studies have a cross-sectional design (n = 29). A before-after design was utilized in 30 studies. Cohort and quasi-experimental designs were employed in 12 and 14 studies, respectively. Notably, only one randomized clinical trial (RCT) was found and included [48]. This level of evidence may indicate an association between accreditation and performance measures; however, causal inferences should be made with considerable caution. A meta-analysis was not possible with these observational designs and the modest methodological consistency.
The appraisal of the included studies showed that 32, 37, and 7 studies were of good, fair, and poor methodological quality, respectively. Studies with poor methodological quality have shown a positive [49,50,51] (n = 3) or neutral [52,53,54,55] (n = 4) accreditation effect; albeit, their findings should be scrutinized with care. Our narrative analysis disregarded these studies to avoid jeopardizing the conclusion. This seemed unlikely to alter the review findings.
The impact themes
Included papers were thematically clustered into six impact themes (see Table 1). Two themes, namely “changes in patient clinical outcomes” and “changes in performance measures,” captured more than 60% of included publications. Although our themes are collectively exhaustive, they are not mutually exclusive as 16% (n = 12) of the studies examined the impact of accreditation on at least two measures in separate themes.
Changes in organizational culture and management
The impact of hospital accreditation on organizational culture and management was examined quantitively in five studies [56,57,58,59,60]. Several studies have examined the effect of hospital accreditation on safety culture through self-reported surveys. Most [56,57,58] but not all found a strong link between both [59]. Accreditation positively affects perceived patient safety culture [56], safety climate toward medication error reporting [57], and organizational culture as manifested by a less hierarchical culture and more group and developmental culture [58]. On the contrary, a recent study did not detect changes in the safety management culture from the nurses’ perspective after accreditation [59].
Changes at the professionals’ level
Our review identified ten studies that assessed the impact of accreditation on self-reported parameters such as job stress, job satisfaction, and work environment [49, 59, 61,62,63,64,65,66,67,68], five being before-after studies, while a comparative approach between accredited and non-accredited hospitals was used in the remaining. Authors found negative (n = 4) or no impact of accreditation (n = 4) at the professionals’ level, particularly for nurses who were the selected subjects in 7 studies.
Studies reported a consistently negative impact of hospital accreditation on professionals’ perceived job stress. For example, in 4 studies, accreditation was associated with higher job stress as perceived by health professionals [59, 61,62,63]. In addition to stress, Elkins et al. [63] reported higher anxiety and depression among nurses during the accreditation preparation phase, as well as a significant improvement in job satisfaction and sleep function post-accreditation. However, due to the limited research available, it remains uncertain if accreditation affects job satisfaction or the working environment.
Changes at the patient level
Only 14 studies that assessed the impact of hospital accreditation on measurable patient-reported outcome parameters were found [21, 48, 53, 55, 69,70,71,72,73,74,75,76,77,78]. Studies mainly used an observational cross-sectional design (n = 12).
Despite the widely held belief that accreditation contributes to improving patient satisfaction and experience, most findings provide little evidence to support whether accreditation status or ratings are measurably linked to patient satisfaction and experience in a meaningful way. Multiple studies that compared accredited with non-accredited hospitals [21, 48, 70, 71, 77, 78] or accredited hospitals at different accreditation levels [69, 72] did not find any association. For instance, Sack et al [77, 78] did not find a link between accreditation and patients’ perception of better quality, reflected by their recommendation rates of the institutions at the hospital level or the cardiology unit level.
Changes in patient clinical outcomes
Interestingly, around one third (n = 24) of the included studies examined the impact of hospital accreditation on patient outcomes [8, 21, 25, 50,51,52,53, 79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95]. Of these, 75% have been published since 2015 as an obvious response to previous appeals to investigate accreditation effects on clinical outcomes. Overall, the results showed a clear trend toward a positive relationship between accreditation and clinical outcome. Studies reported having (n = 15) or lacking (n = 5) positive effects on clinical outcomes, whereas none of the studies concluded having an overall negative impact. In-hospital mortality rate (n = 13) and the patient’s length of stay (n = 12) were studied most.
Comparative studies showed a positive effect of accreditation on mortality rates at various accreditation stages [79,80,81,82,83,84]. However, these studies were restricted to two accreditation schemes, namely, The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) in the USA and Danish healthcare quality program (DDKM in Danish: den danske kvalitetsmodel) in Denmark, which may hinder generalization. For example, relative to hospitals with low [82, 83] or persistently low [84] accreditation standards compliance, patients treated in high compliance hospitals were found to have significantly lower mortality. Dissimilarly, such a relationship was not identified in other studies [8, 21, 85,86,87,88].
Several studies consistently indicated a lack of relationship between accreditation and hospital 30-day readmission rate in various contexts [21, 84, 89, 90], whereas other studies presented contradictory effects on healthcare-associated infections [25, 85, 91, 92]. However, studies reported a consistently positive impact of accreditation on hospital [84, 86, 89, 93] and departmental [91, 94, 95] patient length of stay.
Changes in the performance measures
There is plausible evidence that hospital accreditation promotes service quality. Consequently, improvement in structure and process performance measures could be expected [21, 83]. The impact of accreditation on performance measures was the largest topic (n = 28) explored in our review [8, 18, 19, 28, 48, 51, 54, 60, 68, 79, 87, 90, 96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111]. Despite the complexity and cyclicality of accreditation effects on performance measures, about three-fourths (n = 18) of the analyzed studies showed a positive effect of accreditation on service quality at organizational and departmental levels.
Although the only included RCT reported no or low association between accreditation and quality indicators [48], the methodological quality of this study was fair but not good enough to generalize this finding. It is noteworthy that several quasi-experimental and prospective longitudinal studies reported significant positive effects of accreditation on various quality of service aspects [8, 60, 96,97,98,99]. Accumulated evidence showed that longitudinal participation in accreditation translated into higher standards compliance [60], adherence to recommended guidelines [97], enhancement in structural and process elements [19, 28], and sustained change [98]. For instance, in a stepped-wedge multi-level study, accreditation resulted in significant improvement of various processes that did not meet the target performance during the 6-month period prior to the accreditation survey [99]. Participation in accreditation has shown tangible benefits in performance measures linked to acute myocardial infarction [79, 100], heart failure, and pneumonia [100]. Nevertheless, some studies have found that accreditation is not associated with hand hygiene compliance [101], medication administration error rates [102], and other performance measures [87, 103, 104].
Changes in economic outcomes
A total of eight studies evaluating the economic effects of accreditation have been included [83, 90, 112,113,114,115,116,117]. Most of them (n = 5) showed a positive impact on various economic outcomes, particularly healthcare efficiency.
Apart from estimating the cost of accreditation, which varied dramatically between countries and programs, accreditation was shown to have a significantly favorable effect on cost reduction [90], increase in the share of outpatient revenue [83], higher productivity [112], and improved efficiency [113,114,115]. For example, a large retrospective longitudinal study, tracking 748 hospitals over 10 years, reported a significant positive net impact of hospital accreditation on improving the mean efficiency as estimated through bootstrapped data envelopment analysis (DEA) at accreditation year and the 2 years following [113]. Another observational study found that hospital accreditation, ceteris paribus, was associated with 119% improvement on a quality index relative to baseline data, which translated into a combined saving of US$ 593.000 in two hospitals over 3 years [90]. On the contrary, participating in accreditation programs was found to have an inverse effect on hospital efficiency secondary to higher staffing demand and investment in equipment [116]. Other studies did not detect a major impact of accreditation on operating room efficiency [117], cash-flow margin, and total cost per case [83].
Discussion
This review has comprehensively analyzed the hospital accreditation literature during the last two decades to understand its effect on the quality of health services. In total, 76 studies have been included and assigned to a relevant impact category.
Despite the mixed views expressed, a positive accreditation effect was found in more than 55% of the included studies. Our results indicate a consistent positive accreditation effect on process-related performance measures, safety culture, hospital efficiency, and patient length of stay. In contrast, staff job stress was found to be consistently negatively affected. Heterogenous results on mortality and healthcare-associated infection hampered the drawing of firm conclusions on those outcome measures. Staff job satisfaction, patient satisfaction and experience, and 30-day readmission rate were found to be unrelated to accreditation. However, the variation in accreditation schemes [19], the inability to isolate extrinsic confounders, and diversity in hospital characteristics may influence these conclusions.
Although culture is an oft-cited reason for failure, consistent with previous studies [13, 22, 32], our review found a positive effect of accreditation on safety culture at the organizational level. However, at the individual level, accreditation has an adverse impact on professionals’ stress level [59, 61,62,63]. This may indicate a need for a balance between accreditation risks and benefits to encourage health practitioners’ acceptance and participation in the accreditation journey [30, 118]. Such negative consequence seems inevitable. However, awareness campaigns, leadership support, and better design of accreditation standards and processes are vital remedies that need to be considered [119].
As an extension of previous reviews [13, 31, 32, 34], our analysis did not find a correlation between accreditation and higher patient satisfaction or experience. The earlier presumption that patient satisfaction is a reverberation of hospital quality of service [120] was not confirmed in our review. While our findings support the view that accreditation is a tool that stimulates improving internal processes delivery [121], the appropriate improvement threshold for being tangible is equivocal. Likely, the answer depends on the design of the accreditation standards and processes [4, 122].
Our review found that hospital accreditation benefits appear before [56, 96], during [80], and after accreditation [97, 107]. Nevertheless, the question of the cyclicality of the impact of accreditation and how long the effect lasts is a matter of concern [16, 81, 99, 123]. For the economic outcomes, studies attribute the favorable impact of accreditation to performance improvement [90]. However, the low number of studies hindered definite conclusions. Isolating the accreditation’s financial impact from other contextual factors is challenging and may explain the paucity of studies in this domain [13, 124].
More studies on the impact of hospital accreditation are needed to elucidate part of the jigsaw puzzle. An argument might be that the heterogeneity in the accreditation literature and its observational nature limits its value in providing convincing conclusions on accreditation effectiveness [125]. However, the absence of firm evidence of the effects is not evidence of a lack of effect. Having realized the ethical and practical challenges of conducting randomized trials on this multifaceted process [11], observational studies appear to be of doubtless merit despite their drawbacks.
The bulk of the studies in our review used cross-sectional or two-point comparative (i.e., before-and-after) designs. Therefore, an argument could be that the observed improvement in observational studies is not necessarily attributed to the accreditation per se. However, this assumption does not rationalize abandoning what has been found already, and if observed improvements were secondary to other accreditation-driven factors, it is indeed still a win-win situation.
Our review has several strengths and limitations. This study is one of the largest systematic reviews conducted to understand the impact of hospital accreditation. The study extensively discussed the measures and aspects being addressed and affected by introducing hospital accreditation to elucidate the complex view for researchers, policymakers, and stakeholders in the accreditation field. The use of pre-decided inclusion criteria, citation indices, and broad range of databases were enablers to enhance the likelihood of identifying all relevant publications. We recognize that overlooking some studies that are not published in peer-reviewed journals is still possible. However, our comprehensive search suggests that results’ bias is unlikely. We should acknowledge that not searching the grey literature is a limitation in our review. The grey literature can provide a valuable contribution to the review and may reduce publication bias [126]. However, to maintain the validity of the results, we limited our search to studies rigorously peer-reviewed or indexed in academic journals [127]. Despite the fact that our review included evidence on accreditation effectiveness in both developing and developed countries, no distinction between these settings was made.
Conclusion
Accreditation must be viewed as one element that complements other performance improvement strategies to achieve a tactile effect in the health system. The view must be compatible with the fact that accreditation is a “knowledge translation” intervention that aids in the integration of standards into everyday activities [128]. The advantages of accreditation outweigh potential drawbacks. However, we echo previous reviews [6, 12, 23, 32, 33, 129] in calling for further rigorous studies to investigate the impact of accreditation, particularly on economic outcomes to evaluate if the benefits genuinely justify the costs. Utilizing longitudinal designs and controlling for exogenous confounders could help detect causal conclusions of accreditation effects and enrich consequential decisions in this realm.
Our review underpins the notion that compliance with accreditation standards has multiple plausible benefits in improving the performance in hospital settings and outcomes. Despite inconclusive evidence on causality and minor unintended negative consequences of hospital accreditation, such as those on job stress, we conclude that introducing hospital accreditation stimulates performance improvement and patient safety. In synchronization with other health policies, efforts to incentivize and modernize accreditation are recommended to move towards institutionalization and sustaining the performance gains.
Availability of data and materials
Data relevant to the study are included in the article or uploaded as Additional files. Detailed ratings of methodological quality are available upon reasonable request.
Abbreviations
- IOM:
-
Institute of medicine
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- HSE:
-
Health systems evidence
- CDSR:
-
Cochrane database of systematic reviews
- CENTRAL:
-
Cochrane central register of controlled trials
- SSCI:
-
Social sciences citation index
- RSCI:
-
Russian science citation index
- PICO:
-
Population, intervention, comparison, outcomes
- IRR:
-
Inter-rater reliability (IRR)
- JCIA:
-
Joint commission international accreditation
- RCT:
-
Randomized clinical trial
- JCAHO:
-
The Joint commission on accreditation of healthcare organizations
- DDKM:
-
Danish healthcare quality program (in Danish: den danske kvalitetsmodel)
- DEA:
-
Data envelopment analysis
References
Institute of Medicine Committee on Quality of Health Care in America. In: Kohn LT, Corrigan JM, Donaldson MS, editors. To Err is Human: Building a Safer Health System. Washington (DC): National Academies Press (US); 2000. https://doi.org/10.17226/9728.
Altman DE, Clancy C, Blendon RJ. Improving patient safety--five years after the IOM report. N Engl J Med. 2004;351(20):2041–3. https://doi.org/10.1056/NEJMp048243.
Devers KJ, Pham HH, Liu G. What is driving hospitals' patient-safety efforts? A study of twelve communities suggests that a regulatory body, not market forces, is having the strongest impact on hospitals' efforts to improve patient safety. Health Aff (Millwood). 2004;23(2):103–15. https://doi.org/10.1377/hlthaff.23.2.103.
Moffett M, Bohara A. Hospital quality oversight by the joint commission on the accreditation of healthcare organizations. East Econ J. 2005;31:629–47.
Greenfield D, Hinchcliff R, Hogden A, Mumford V, Debono D, Pawsey M, et al. A hybrid health service accreditation program model incorporating mandated standards and continuous improvement: interview study of multiple stakeholders in Australian health care. Int J Health Plann Manag. 2016;31(3):e116–30. https://doi.org/10.1002/hpm.2301.
Flodgren G, Gonçalves-Bradley DC, Pomey MP. External inspection of compliance with standards for improved healthcare outcomes. Cochrane Database Syst Rev. 2016;12:CD008992. https://doi.org/10.1002/14651858.CD008992.pub3.
Viswanathan HN, Salmon JW. Accrediting organizations and quality improvement. Am J Manag Care. 2000;6(10):1117–30.
Petrović GM, Vuković M, Vraneš AJ. The impact of accreditation on health care quality in hospitals. Vojnosanit Pregled. 2018;75(8):803–8. https://doi.org/10.2298/VSP160728390M.
Hornsby JA. Hospitals as they are: the hospital problem of today—what is it? Bull Am Coll Surg. 1917;1:4–11.
Shaw CD. External quality mechanisms for health care: summary of the ExPeRT project on visitatie, accreditation, EFQM and ISO assessment in European Union countries. External peer review techniques. European Foundation for quality management. International Organization for Standardization. Int J Qual Health Care. 2000;12(3):169–75. https://doi.org/10.1093/intqhc/12.3.169.
Braithwaite J, Westbrook J, Pawsey M, Greenfield D, Naylor J, Iedema R, et al. A prospective, multi-method, multi-disciplinary, multi-level, collaborative, social-organisational design for researching health sector accreditation [LP0560737]. BMC Health Serv Res. 2006;6(1):113. https://doi.org/10.1186/1472-6963-6-113.
Brubakk K, Vist GE, Bukholm G, Barach P, Tjomsland O. A systematic review of hospital accreditation: the challenges of measuring complex intervention effects. BMC Health Serv Res. 2015;15(1):280. https://doi.org/10.1186/s12913-015-0933-x.
Greenfield D, Braithwaite J. Health sector accreditation research: a systematic review. Int J Qual Health Care. 2008;20(3):172–83. https://doi.org/10.1093/intqhc/mzn005.
Shaw CD. Toolkit for accreditation programs. Australia: The International Society for Quality In Health Care; 2004.
Pomey MP, Francois P, Contandriopoulos AP, Tosh A, Bertrand D. Paradoxes of French accreditation. Qual Saf Health Care. 2005;14(1):51–5. https://doi.org/10.1136/qshc.2004.011510.
Pomey MP, Lemieux-Charles L, Champagne F, Angus D, Shabah A, Contandriopoulos AP. Does accreditation stimulate change? A study of the impact of the accreditation process on Canadian healthcare organizations. Implement Sci. 2010;5(1):31. https://doi.org/10.1186/1748-5908-5-31.
Rooney AL, van Ostenberg PR. Licensure accreditation and certification: approaches to health services quality. Washington, DC: Center for Human Services; 1999.
Braithwaite J, Greenfield D, Westbrook J, Pawsey M, Westbrook M, Gibberd R, et al. Health service accreditation as a predictor of clinical and organisational performance: a blinded, random, stratified study. Qual Saf Health Care. 2010;19(1):14–21. https://doi.org/10.1136/qshc.2009.033928.
Shaw C, Groene O, Mora N, Sunol R. Accreditation and ISO certification: do they explain differences in quality management in European hospitals? Int J Qual Health Care. 2010;22(6):445–51. https://doi.org/10.1093/intqhc/mzq054.
Desveaux L, Mitchell JI, Shaw J, Ivers NM. Understanding the impact of accreditation on quality in healthcare: a grounded theory approach. Int J Qual Health Care. 2017;29(7):941–7. https://doi.org/10.1093/intqhc/mzx136.
Lam MB, Figueroa JF, Feyman Y, Reimold KE, Orav JE, Jha AK. Association between patient outcomes and accreditation in US hospitals: observational study. BMJ. 2018;20:363. https://doi.org/10.1136/bmj.k4011.
Saleh SS, Bou Sleiman J, Dagher D, Sbeit H, Natafgi N. Accreditation of hospitals in Lebanon: is it a worthy investment? Int J Qual Health Care. 2013;25(3):284–90. https://doi.org/10.1093/intqhc/mzt018.
Greenfield D, Pawsey M, Hinchcliff R, Moldovan M, Braithwaite J. The standard of healthcare accreditation standards: a review of empirical research underpinning their development and impact. BMC Health Serv Res. 2012;12(1):329. https://doi.org/10.1186/1472-6963-12-329.
Greenfield D, Braithwaite J. Developing the evidence base for accreditation of health care organisations: a call for transparency and innovation. Qual Saf Health Care. 2009;18(3):162–3. https://doi.org/10.1136/qshc.2009.032359.
Salim FM, Rahman MH. The impact of joint commission international healthcare accreditation on infection control performance: a study in Dubai hospital. Glob J Bus Soc Sci Rev. 2017;5(1):37–45. https://doi.org/10.35609/gjbssr.2017.5.1(6).
de Santé HA. Literature review on the impact of hospital accreditation. Paris: MATRIX Knowledge group; 2010.
Flodgren G, Pomey MP, Taber SA, Eccles MP. Effectiveness of external inspection of compliance with standards in improving healthcare organisation behaviour, healthcare professional behaviour or patient outcomes. Cochrane Database Syst Rev. 2011;11:CD008992. https://doi.org/10.1002/14651858.CD008992.pub2.
Shaw CD, Groene O, Botje D, Sunol R, Kutryba B, Klazinga N, et al. The effect of certification and accreditation on quality management in 4 clinical services in 73 European hospitals. Int J Qual Health Care. 2014;26(Suppl 1):100–7. https://doi.org/10.1093/intqhc/mzu023.
Avia I, Hariyati RTS. Impact of hospital accreditation on quality of care: a literature review. Enferm Clin. 2019;29(Suppl 2):315–20. https://doi.org/10.1016/j.enfcli.2019.06.003.
Alkhenizan A, Shaw C. Impact of accreditation on the quality of healthcare services: a systematic review of the literature. Ann Saudi Med. 2011;31(4):407–16. https://doi.org/10.4103/0256-4947.83204.
Almasabi M, Yang H, Thomas S. A systematic review of the association between healthcare accreditation and patient satisfaction. World Appl Sci J. 2014;31(9):1618–23.
Hinchcliff R, Greenfield D, Moldovan M, Westbrook JI, Pawsey M, Mumford V, et al. Narrative synthesis of health service accreditation literature. BMJ Qual Saf. 2012;21(12):979–91. https://doi.org/10.1136/bmjqs-2012-000852.
Kilsdonk M, Siesling S, Otter R, Harten W. Evaluating the impact of accreditation and external peer review. Int J Health Care Qual Assur. 2015;28(8):757–77. https://doi.org/10.1108/IJHCQA-05-2014-0055.
Park IT, Jung YY, Park SH, Hwang JH, Suk SH. Impact of healthcare accreditation using a systematic review: balanced score card perspective [in Korean]. Quality Improvement in Health Care. 2017;23(1):69–90. https://doi.org/10.14371/QIH.2017.23.1.69.
Araujo CAS, Siqueira MM, Malik AM. Hospital accreditation impact on healthcare quality dimensions: a systematic review. Int J Qual Health Care. 2020;32(8):531–44. https://doi.org/10.1093/intqhc/mzaa090.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097.
Kerr NL. HARKing: hypothesizing after the results are known. Personal Soc Psychol Rev. 1998;2(3):196–217. https://doi.org/10.1207/s15327957pspr0203_4.
Richardson WS, Wilson MC, Nishikawa J, Hayward RS. The well-built clinical question: a key to evidence-based decisions. ACP J Club. 1995;123(3):A12–3. https://doi.org/10.7326/ACPJC-1995-123-3-A12.
Fleiss JL, Levin B, Paik MC. Statistical methods for rates and proportions. 3rd ed. Hoboken, NJ: John Wiley & Sons; 2003. https://doi.org/10.1002/0471445428.
Belur J, Tompson L, Thornton A, Simon M. Interrater reliability in systematic review methodology: exploring variation in coder decision-making. Sociol Methods Res. 2018;50(2):837–65. https://doi.org/10.1177/0049124118799372.
Groves M, Mundt K. Friend or foe? Google translate in language for academic purposes. Engl Specif Purp. 2015;37:112–21. https://doi.org/10.1016/j.esp.2014.09.001.
Jackson JL, Kuriyama A, Anton A, Choi A, Fournier JP, Geier AK, et al. The accuracy of google translate for abstracting data from non-English-language trials for systematic reviews. Ann Intern Med. 2019;171(9):677–9. https://doi.org/10.7326/M19-0891.
Hawker S, Payne S, Kerr C, Hardey M, Powell J. Appraising the evidence: reviewing disparate data systematically. Qual Health Res. 2002;12(9):1284–99. https://doi.org/10.1177/1049732302238251.
Groene O, Botje D, Suñol R, Lopez MA, Wagner C. A systematic review of instruments that assess the implementation of hospital quality management systems. Int J Qual Health Care. 2013;25(5):525–41. https://doi.org/10.1093/intqhc/mzt058.
Salloum SA, Al-Emran M, Monem AA, Shaalan K. Using Text Mining Techniques for Extracting Information from Research Articles. In: Shaalan K, Hassanien A, Tolba F, editors. Intelligent Natural Language Processing: Trends and Applications. Studies in Computational Intelligence. Cham, Switzerland: Springer; 2018. p. 373–97.
Assarroudi A, Heshmati F, Armat MR, Ebadi A, Vaismoradi M. Directed qualitative content analysis: the description and elaboration of its underpinning methods and data analysis process. J Res Nurs. 2018;23(1):42–55. https://doi.org/10.1177/1744987117741667.
Program BPE. 2019–2020 Baldrige excellence framework (health care): proven leadership and management practices for high performance. Gaithersburg, MD: U.S. Department of Commerce, National Institute of Standards and Technology; 2019. https://www.nist.gov/baldrige
Salmon J, Heavens J, Lombard C, Tavrow P. The Impact of Accreditation on the Quality of Hospital Care: KwaZulu-Natal Province, Republic of South Africa. Operations Research Results 2:17. Bethesda MD: Published for the US Agency for International Development (USAID) by the Quality Assurance Project, University Research Co., LLC; 2003.
Domingues AL, dos Santos SVM, Góes FSN, Martinez MR. Evaluation of the contribution of hospital accreditation in the process of permanent health education. J Nurs UFPE Line. 2017;11(suppl 5):2177–84.
Mørk Hansen G, Jensen CS, Østergaard LM, Dethlefsen C, Luther P, Andreasen JJ. Possible decrease in the prevalence of nosocomial infections after the accreditation process in the region of northern Jutland, Denmark [in Danish]. Ugeskr Laeger. 2013;175(8):495–8.
Al Awa B, De Wever A, Almazrooa A, Habib H. al-Noury K, el Deek B, et al. the impact of accreditation on patient safety and quality of care indicators at king Abdulaziz University hospital in Saudi Arabia. Res J Med Sci. 2011;5(1):43–51. https://doi.org/10.3923/rjmsci.2011.43.51.
Almasabi M, Thomas S. The impact of Saudi hospital accreditation on quality of care: a mixed methods study. Int J Health Plann Manag. 2017;32(4):e261–e78. https://doi.org/10.1002/hpm.2373.
Marzban S, Ramezankhani A, Rezai-Rad M, Daneshkohan A, Najafi A. Status of accessible quality indices in the hospitals of Shahid Beheshti University of Medical Sciences according to accreditation in 2015. Ann Trop Med Public Health. 2017;10(4):956–62. https://doi.org/10.4103/ATMPH.ATMPH_265_17.
Abedi G, Abedini E, Malakzadeh R, Mojarad F. Medical errors management before and after implementation of accreditation in hospital. Iran J Health Sci. 2014;2(4):59–66. https://doi.org/10.18869/acadpub.jhs.2.4.59.
Joseph S. The effect of accreditation on patient satisfaction in public healthcare delivery: a comparative study of accredited and non-accredited hospitals in Kerala. Rajagiri J Soc Dev. 2018;10(2):123–36.
Lám J, Merész G, Bakacsi G, Belicza E, Surjan C, Takacs E. Changing of the patient safety culture in the pilot institutes of the Hungarian accreditation program [in Hungarian]. Orv Hetil. 2016;157(42):1667–73. https://doi.org/10.1556/650.2016.30556.
Lee E. Safety climate and attitude toward medication error reporting after hospital accreditation in South Korea. Int J Qual Health Care. 2016;28(4):508–14. https://doi.org/10.1093/intqhc/mzw058.
Andres EB, Song W, Schooling CM, Johnston JM. The influence of hospital accreditation: a longitudinal assessment of organisational culture. BMC Health Serv Res. 2019;19(1):467. https://doi.org/10.1186/s12913-019-4279-7.
Kim MR, Kim MS. Awareness, job stress, turnover intention, safety management perception change of nurses in a general hospital - before and after medical institution certification system [in Korean]. J Korea Contents Assoc. 2019;19(1):385–95.
Greenfield D, Lawrence SA, Kellner A, Townsend K, Wilkinson A. Health service accreditation stimulating change in clinical care and human resource management processes: a study of 311 Australian hospitals. Health Policy. 2019;123(7):661–5. https://doi.org/10.1016/j.healthpol.2019.04.006.
Al-Faouri I, Al-Dmour A, Al-Ali N, Abu ALRub R, Abu Moghli F. Effect of health care accreditation council survey site visit on perceived stress level among Jordanian healthcare providers. Nurs Forum. 2019;54(1):30–7. https://doi.org/10.1111/nuf.12294.
Higashi P, Simonetti JP, Carvalhaes MABL, Spiri WC, Parada CMGL. Potentially stressful situations for nurses considering the condition of accreditation of hospitals. Rev Rene. 2013;14(6):1141–8.
Elkins G, Cook T, Dove J, Markova D, Marcus JD, Meyer T, et al. Perceived stress among nursing and administration staff related to accreditation. Clin Nurs Res. 2010;19(4):376–86. https://doi.org/10.1177/1054773810373078.
Kagan I, Farkash-Fink N, Fish M. Effect of joint commission international accreditation on the nursing work environment in a tertiary medical center. J Nurs Care Qual. 2016;31(4):E1–8. https://doi.org/10.1097/NCQ.0000000000000180.
Oliveira JLC, Souza VS, Pereira ACS, Haddad MCFL, Marcon SS, Matsuda LM. Work environment and accreditation: analysis by mixed explanatory sequential method. Escola Anna Nery. 2018;22(4):e20170379. https://doi.org/10.1590/2177-9465-ean-2017-0379.
Oliveira PB, Spiri WC, Dell’Acqua MC, Mondini CC. Comparison between the accredited and nonaccredited public hospital working environments. Acta Paul Enferm. 2016;29(1):53–9. https://doi.org/10.1590/1982-0194201600008.
Oliveira JLC, Magalhães AMM, Bernardes A, Haddad MCFL, Wolff LDG, Marcon SS, et al. Influence of hospital accreditation on professional satisfaction of the nursing team: mixed method study. Rev Lat Am Enferm. 2019;27:e3109. https://doi.org/10.1590/1518-8345.2799.3109.
Um MH, Lyu ES, Lee SM, Park YK. International hospital accreditation and clinical nutrition service in acute care hospitals in South Korea: results of a nationwide cross-sectional survey. Asia Pac J Clin Nutr. 2018;27(1):158–66. https://doi.org/10.6133/apjcn.032017.25.
Heuer AJ. Hospital accreditation and patient satisfaction: testing the relationship. J Healthc Qual. 2004;26(1):46–51. https://doi.org/10.1111/j.1945-1474.2004.tb00471.x.
Hayati NI, Azimatun NA, Rozita H, Ezat WA, Rizal AM. In-patients' satisfaction in the medical and surgical wards - a comparison between accredited and non accredited hospital in the state of Selangor. J Commun Health. 2010;16(1):60–8.
Barghouthi ED, Imam A. Patient satisfaction: comparative study between Joint Commission International accredited and non-accredited Palestinian hospitals. Health Sci J. 2018;12:547.
Haj-Ali W, Bou Karroum L, Natafgi N, Kassak K. Exploring the relationship between accreditation and patient satisfaction - the case of selected Lebanese hospitals. Int J Health Policy Manag. 2014;3(6):341–6. https://doi.org/10.15171/ijhpm.2014.116.
Al-Qahtani MF, Al-Dohailan SK, Al-Sharani HT, Al-Medaires MA, Khuridah EN, Al-Dossary NM. The impact of the status of hospital accreditation on patient satisfaction with the obstetrics and gynecology clinics in the Eastern Province. J Med Med Sci. 2012;3(10):665–73.
Ajarmah BS, Hashem TN. Patient satisfaction evaluation on hospitals; comparison study between accredited and non accredited hospitals in Jordan. Eur Sci J. 2015;11(32):298–314.
Mohebbifar R, Rafiei S, Asl AM, Ranjbar M, Khodayvandi M. Association between hospital accreditation and patient satisfaction: a survey in the Western Province of Iran. Bangladesh J Med Sci. 2017;16(1):77–84. https://doi.org/10.3329/bjms.v16i1.31137.
Andres EB, Song W, Song W, Johnston JM. Can hospital accreditation enhance patient experience? Longitudinal evidence from a Hong Kong hospital patient experience survey. BMC Health Serv Res. 2019;19(1):623. https://doi.org/10.1186/s12913-019-4452-z.
Sack C, Lütkes P, Günther W, Erbel R, Jöckel KH, Holtmann GJ. Challenging the holy grail of hospital accreditation: a cross sectional study of inpatient satisfaction in the field of cardiology. BMC Health Serv Res. 2010;10(1):120. https://doi.org/10.1186/1472-6963-10-120.
Sack C, Scherag A, Lütkes P, Günther W, Jöckel KH, Holtmann G. Is there an association between hospital accreditation and patient satisfaction with hospital care? A survey of 37 000 patients treated by 73 hospitals. Int J Qual Health Care. 2011;23(3):278–83. https://doi.org/10.1093/intqhc/mzr011.
Chen J, Rathore SS, Radford MJ, Krumholz HM. JCAHO accreditation and quality of care for acute myocardial infarction. Health Aff (Millwood). 2003;22(2):243–54. https://doi.org/10.1377/hlthaff.22.2.243.
Barnett ML, Olenski AR, Jena AB. Patient mortality during unannounced accreditation surveys at US hospitals. JAMA Intern Med. 2017;177(5):693–700. https://doi.org/10.1001/jamainternmed.2016.9685.
Towers TJ, Clark J. Pressure and performance: buffering capacity and the cyclical impact of accreditation inspections on risk-adjusted mortality. J Healthc Manag. 2014;59(5):323–35. https://doi.org/10.1097/00115514-201409000-00005.
Falstie-Jensen AM, Larsson H, Hollnagel E, Nørgaard M, Svendsen MLO, Johnsen SP. Compliance with hospital accreditation and patient mortality: a Danish nationwide population-based study. Int J Qual Health Care. 2015;27(3):165–74. https://doi.org/10.1093/intqhc/mzv023.
Griffith JR, Knutzen SR, Alexander JA. Structural versus outcomes measures in hospitals: a comparison of joint commission and Medicare outcomes scores in hospitals. Qual Manag Health Care. 2002;10(2):29–38. https://doi.org/10.1097/00019514-200210020-00007.
Falstie-Jensen AM, Bogh SB, Johnsen SP. Consecutive cycles of hospital accreditation: persistent low compliance associated with higher mortality and longer length of stay. Int J Qual Health Care. 2018;30(5):382–9. https://doi.org/10.1093/intqhc/mzy037.
Miller MR, Pronovost P, Donithan M, Zeger S, Zhan C, Morlock L, et al. Relationship between performance measurement and accreditation: implications for quality of care and patient safety. Am J Med Qual. 2005;20(5):239–52. https://doi.org/10.1177/1062860605277076.
Arab M, Mousavi SM. Khesal AA, Akbarisari a. the effect of accreditation system on the key performance indicators of hospitals affiliated to Tehran university of medical sciences: an interrupted time series analysis in 2012-2014 [in Persian]. J Hosp. 2017;16(1):17–26.
Mosadeghrad AM, Shahebrahimi SS, Ghazanfari M. Exploring the relationship between accreditation and hospital performance: using data mining approach [in Persian]. J School Public Health Inst Public Health Res. 2018;16(1):33–50.
Wardhani V, van Dijk JP, Utarini A. Hospitals accreditation status in Indonesia: associated with hospital characteristics, market competition intensity, and hospital performance? BMC Health Serv Res. 2019;19(1):372. https://doi.org/10.1186/s12913-019-4187-x.
Falstie-Jensen AM, Nørgaard M, Hollnagel E, Larsson H, Johnsen SP. Is compliance with hospital accreditation associated with length of stay and acute readmission? A Danish nationwide population-based study. Int J Qual Health Care. 2015;27(6):451–8. https://doi.org/10.1093/intqhc/mzv070.
Halasa YA, Zeng W, Chappy E, Shepard DS. Value and impact of international hospital accreditation: a case study from Jordan. East Mediterr Health J. 2015;21(2):90–9. https://doi.org/10.26719/2015.21.90.
Janati A, Tabrizi JS, Toofan F, Algalandis K, Ebrahimoghli R. Hospital accreditation: what is its effect on quality and safety indicators? Experience of an Iranian teaching hospital. Bali Med J. 2016;5(2):303–7. https://doi.org/10.15562/bmj.v5i2.241.
Mumford V, Reeve R, Greenfield D, Forde K, Westbrook J, Braithwaite J. Is accreditation linked to hospital infection rates? A 4-year, data linkage study of Staphylococcus aureus rates and accreditation scores in 77 Australian acute hospitals. Int J Qual Health Care. 2015;27(6):479–85. https://doi.org/10.1093/intqhc/mzv078.
Jarrah S, Judeh M, AbuRuz ME, Masa'Deh R. The impact of health care accreditation on patients' safety. Int Med J. 2019;24(3):129–39.
Leite CD, Pereira TC, Freitas MP, Tinôco NLW, Pereira FG, Menezes RVLV, et al. Effect of hospital accreditation process in outcomes of patients with acute coronary syndrome. Int J Cardiovasc Sci. 2019;32(6):607–14. https://doi.org/10.5935/2359-4802.20190034.
Al-Sughayir MA. Effect of accreditation on length of stay in psychiatric inpatients: pre-post accreditation medical record comparison. Int J Ment Health Syst. 2016;10(1):55. https://doi.org/10.1186/s13033-016-0090-6.
Devkaran S, O'Farrell PN. The impact of hospital accreditation on quality measures: an interrupted time series analysis. BMC Health Serv Res. 2015;15(1):137. https://doi.org/10.1186/s12913-015-0784-5.
Falstie-Jensen AM, Bogh SB, Hollnagel E, Johnsen SP. Compliance with accreditation and recommended hospital care-a Danish nationwide population-based study. Int J Qual Health Care. 2017;29(5):625–33. https://doi.org/10.1093/intqhc/mzx104.
Devkaran S, O'Farrell PN, Ellahham S, Arcangel R. Impact of repeated hospital accreditation surveys on quality and reliability, an 8-year interrupted time series analysis. BMJ Open. 2019;9(2):e024514. https://doi.org/10.1136/bmjopen-2018-024514.
Bogh SB, Falstie-Jensen AM, Hollnagel E, Holst R, Braithwaite J, Johnsen SP. Improvement in quality of hospital care during accreditation: a nationwide stepped-wedge study. Int J Qual Health Care. 2016;28(6):715–20. https://doi.org/10.1093/intqhc/mzw099.
Schmaltz SP, Williams SC, Chassin MR, Loeb JM, Wachter RM. Hospital performance trends on national quality measures and the association with joint commission accreditation. J Hosp Med. 2011;6(8):454–61. https://doi.org/10.1002/jhm.905.
Mumford V, Greenfield D, Hogden A, Debono D, Gospodarevskaya E, Forde K, et al. Disentangling quality and safety indicator data: a longitudinal, comparative study of hand hygiene compliance and accreditation outcomes in 96 Australian hospitals. BMJ Open. 2014;4(9):e005284. https://doi.org/10.1136/bmjopen-2014-005284.
Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed in 36 health care facilities. Arch Intern Med. 2002;162(16):1897–903. https://doi.org/10.1001/archinte.162.16.1897.
Braga AT, Pena MM, Melleiro MM. Metrics of assistance indicators of certified hospitals. J Nurs UFPE Line. 2018;12(3):665–75. https://doi.org/10.5205/1981-8963-v12i3a230715p665-675-2018.
Bogh SB, Falstie-Jensen AM, Bartels P, Hollnagel E, Johnsen SP. Accreditation and improvement in process quality of care: a nationwide study. Int J Qual Health Care. 2015;27(5):336–43. https://doi.org/10.1093/intqhc/mzv053.
Lutfiyya MN, Sikka A, Mehta S, Lipsky MS. Comparison of US accredited and non-accredited rural critical access hospitals. Int J Qual Health Care. 2009;21(2):112–8. https://doi.org/10.1093/intqhc/mzp003.
Al-Sughayir MA. Administered antipsychotic pro re nata medications in psychiatric inpatients. Pre- and post-accreditation comparison. Saudi Med J. 2014;35(2):172–7.
Wang HF, Jin JF, Feng XQ, Huang X, Zhu LL, Zhao XY, et al. Quality improvements in decreasing medication administration errors made by nursing staff in an academic medical center hospital: a trend analysis during the journey to joint commission international accreditation and in the post-accreditation era. Ther Clin Risk Manag. 2015;11:393–406. https://doi.org/10.2147/TCRM.S79238.
Nomura AT, Silva MB, Almeida MA. Quality of nursing documentation before and after the hospital accreditation in a university hospital. Rev Lat Am Enfermagem. 2016;24:e2813.
Habib RR, Blanche G, Souha F, El-Jardali F, Nuwayhid I. Occupational health and safety in hospitals accreditation system: the case of Lebanon. Int J Occup Environ Health. 2016;22(3):201–8. https://doi.org/10.1080/10773525.2016.1200211.
Pourreza A, Mosadeghrad AM, Zoleikani P. The impact of accreditation on the performance of hospital emergency departments [in Persian]. J Health Based Res. 2017;3(3):277–95.
Al-Sughayir MA. Does accreditation improve pro re nata benzodiazepines administration in psychiatric inpatients? Pre-post accreditation medical record comparison. Int J Ment Health Syst. 2017;11(1):16. https://doi.org/10.1186/s13033-017-0124-8.
Salehian M, Riahi L, Biglarian A. The impact of accreditation on productivity indexes in Firoozgar hospital in Tehran [in Persian]. J Health Adm. 2015;18(60):79–89.
Lindlbauer I, Schreyögg J, Winter V. Changes in technical efficiency after quality management certification: a DEA approach using difference-in-difference estimation with genetic matching in the hospital industry. Eur J Oper Res. 2016;250(3):1026–36. https://doi.org/10.1016/j.ejor.2015.10.029.
Okumura Y, Inomata T, Iwagami M, Eguchi A, Mizuno J, Shiang T, et al. Shortened cataract surgery by standardisation of the perioperative protocol according to the joint commission international accreditation: a retrospective observational study. BMJ Open. 2019;9(6):e028656. https://doi.org/10.1136/bmjopen-2018-028656.
Lin F, Deng YJ, Lu WM, Kweh QL. Impulse response function analysis of the impacts of hospital accreditations on hospital efficiency. Health Care Manag Sci. 2019;22(3):394–409. https://doi.org/10.1007/s10729-019-09472-6.
Saquetto TC, Araujo CAS. Efficiency evaluation of private hospitals in Brazil: a two-stage analysis. Rev Adm Mackenzie. 2019;20(5):eRAMR190183.
Inomata T, Mizuno J, Iwagami M, Kawasaki S, Shimada A, Inada E, et al. The impact of joint commission international accreditation on time periods in the operating room: a retrospective observational study. PLoS One. 2018;13(9):e0204301. https://doi.org/10.1371/journal.pone.0204301.
Pomey MP, Contandriopoulos AP, François P, Bertrand D. Accreditation: a tool for organizational change in hospitals? Int J Health Care Qual Assur. 2004;17(3):113–24. https://doi.org/10.1108/09526860410532757.
Park IT, Jung YY, Suk SH. The perception of healthcare employees and the impact of healthcare accreditation on the quality of healthcare in Korea. J Hosp Adm. 2017;6(6):20–7. https://doi.org/10.5430/jha.v6n6p20.
Singh J. The patient satisfaction concept: a review and reconceptualization. In: Srull T, editor. NA - advances in consumer research. Provo, UT: Association for Consumer Research; 1989. p. 76–9.
Hirose M, Imanaka Y, Ishizaki T, Evans E. How can we improve the quality of health care in Japan? Learning from JCQHC hospital accreditation. Health Policy. 2003;66(1):29–49. https://doi.org/10.1016/S0168-8510(03)00043-5.
Jha AK. Accreditation, quality, and making hospital care better. JAMA. 2018;320(23):2410–1. https://doi.org/10.1001/jama.2018.18810.
Devkaran S, O'Farrell PN. The impact of hospital accreditation on clinical documentation compliance: a life cycle explanation using interrupted time series analysis. BMJ Open. 2014;4(8):e005240. https://doi.org/10.1136/bmjopen-2014-005240.
Mumford V, Forde K, Greenfield D, Hinchcliff R, Braithwaite J. Health services accreditation: what is the evidence that the benefits justify the costs? Int J Qual Health Care. 2013;25(5):606–20. https://doi.org/10.1093/intqhc/mzt059.
Ivers N, Tricco AC, Trikalinos TA, Dahabreh IJ, Danko KJ, Moher D, et al. Seeing the forests and the trees--innovative approaches to exploring heterogeneity in systematic reviews of complex interventions to enhance health system decision-making: a protocol. Syst Rev. 2014;3(1):88. https://doi.org/10.1186/2046-4053-3-88.
Paez A. Gray literature: an important resource in systematic reviews. J Evid Based Med. 2017;10(3):233–40. https://doi.org/10.1111/jebm.12266.
Pappas C, Williams I. Grey literature: its emerging importance. J Hosp Librariansh. 2011;11(3):228–34. https://doi.org/10.1080/15323269.2011.587100.
Mitchell JI, Graham ID, Nicklin W. The unrecognized power of health services accreditation: more than external evaluation. Int J Qual Health Care. 2020;32(7):445–55. https://doi.org/10.1093/intqhc/mzaa063.
Ng GK, Leung GK, Johnston JM, Cowling BJ. Factors affecting implementation of accreditation programmes and the impact of the accreditation process on quality improvement in hospitals: a SWOT analysis. Hong Kong Med J. 2013;19(5):434–46. https://doi.org/10.12809/hkmj134063.
Acknowledgements
Not applicable.
Funding
The author(s) received no specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors collaboratively designed the review. MH led the development of the search strategy and conducted the searches. MH and MG carried out studies selection, data extraction, quality appraisal, analysis, and interpretation. MP and WG contributed to the study design and data interpretation. MP and WG were responsible for supervision or mentorship. MH wrote the manuscript and all authors contributed to reviewing the manuscript and approve the final version of this article. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. WG is the senior author of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:.
PRISMA Checklist.
Additional file 2:
Database Search Strategies.
Additional file 3:
Summary of the key findings of all studies included in the review (n = 76).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hussein, M., Pavlova, M., Ghalwash, M. et al. The impact of hospital accreditation on the quality of healthcare: a systematic literature review. BMC Health Serv Res 21, 1057 (2021). https://doi.org/10.1186/s12913-021-07097-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-021-07097-6