
Abstract
Background
A new special reimbursement scheme (SRS) for non-insulin medications used for treatment of hyperglycaemia in type 2 diabetes (T2D) was implemented in Finland on January 1, 2017. The new SRS affected all community-dwelling Finnish T2D patients as all community-dwelling residents are eligible for reimbursement for prescription medications. The aim of the study was to evaluate the impact of this co-payment increase on glycaemic control among Finnish T2D patients.
Methods
Data on glycaemic control were collected with HbA1c measures from electronic health records from primary health care and specialized care in the North Karelia region, Finland, from patients with a confirmed T2D diagnosis in 2012 who were alive on January 1, 2017 (n = 8436). Average HbA1c levels were measured monthly 36 months before and 33 months after the policy change. Consumption of diabetes medications was measured with defined daily doses (DDDs) based on reimbursed medication purchases. Interrupted time series design analysed with segmented regression model was applied to examine the effect of the policy change on average HbA1c levels.
Results
Eight thousand one hundred forty-three T2D patients had at least one HbA1c measurement within 01/2014–9/2019. Mean age of the patients was 68.1 (SD 11.3) years and 53.0% were women. Average time since T2D diagnosis was 11.5 (SD 6.1) years. An estimated increase of 0.81 (95% confidence interval, CI, 0.04–1.58) mmol/mol in average HbA1c levels was detected at the time of the policy change. In subgroup analyses, strongest effects were detected among patients who used only other diabetes medications than insulin or metformin in 2016 (3.56 mmol/mol, 95% CI 2.50–4.62). Meanwhile, yearly consumption of diabetes medications decreased slightly from 618.9 (SD 487.8) DDDs/patient in 2016 to 602.9 (SD 475.6) DDDs/patient in 2017 (p = 0.048).
Conclusions
Simultaneously with the increase of the co-payment level, the average HbA1c level increased among T2D patients from the North Karelia region, Finland. This may be explained by the decreased consumption of diabetes medications between 2016 and 2017. Special attention should be allocated to glycaemic control of patients utilizing only other antidiabetic medications than metformin or insulin.
Similar content being viewed by others


Background
Type 2 diabetes (T2D) is a widespread disease with rapidly increasing prevalence. In Finland alone, the current prevalence of T2D is around 8% and the disease is causing around 15% of the total expenditures of the Finnish health care system [1, 2]. When compared with other Nordic countries, consumption of diabetes medications is high in Finland [3] causing high pharmaceutical expenditure. For this, a new special reimbursement scheme (SRS) for non-insulin medications used for treatment of hyperglycaemia in T2D was implemented in Finland on January 1, 2017 [4,5,6]. The new SRS affected all community-dwelling Finnish T2D patients utilizing any other diabetes medication than insulin because in Finland, all community-dwelling residents are eligible for reimbursement for prescription medications. During the first year of the new legislation coming into effect, the medication reimbursement costs lowered by 24% (EUR 26 million), but simultaneously the co-payments of T2D patients more than tripled (from EUR 11.9 million to EUR 39.7 million, + 334%) [7].
In previous studies, co-payment increase related to diabetes medications is reported to be associated with decreased use of [8, 9] and lower adherence to medications [10,11,12,13,14,15,16], and therefore, with reduced glycaemic control [15, 16]. These changes may have clinical implications in terms of glycaemic control, which in turn is known to be associated with long-term micro- and macrovascular complications [17,18,19]. Therefore, the aim of the present study was to evaluate the impact of the co-payment increase on glycaemic control among Finnish T2D patients. To provide reasons for possible changes in glycaemic control, we also investigated changes in consumption of diabetes medications before and after the policy change.
Methods
Setting
The Finnish SRS and the policy change are described in detail in Lavikainen et al. (2020) and Suviranta et al. (2019) [20, 21]. Briefly, all Finnish residents are eligible for reimbursement for prescription medications purchased from community pharmacies according to three categories based on medical grounds [22] after an initial deductible of EUR 50 per calendar year (since 2015) [23]. The reimbursement is received directly at the community pharmacies. In 2014, 35% of the medication cost in the Basic Refund Category, 65% of the cost in the Lower and 100% of the cost after a fixed co-payment in the Higher Special Refund Categories were reimbursed by the National Health Insurance Scheme [24]. If a patient’s co-payments exceed a certain limit during a calendar year (varying between EUR 572.00 and EUR 612.62 during 2014–2019), the patient becomes eligible for an Additional Refund [7, 23,24,25,26]. After reaching the Additional Refund limit, the patient pays only a fixed co-payment for each purchased, reimbursable medication.
Patients having a certain chronic disease, such as diabetes, and meeting medical criteria defined by the Social Insurance Institution of Finland (SII) can be entitled to a special reimbursement for medication costs. To be granted this entitlement for antidiabetic medications other than insulin by the SII, the patient must have a confirmed diabetes diagnosis based on criteria stated by the SII [20]. To receive special reimbursement for GLP-1 (glucagon-like peptide-1) analogues, in addition to confirmed diabetes, other antidiabetic medications need to be first tried and the patient must have a body mass index ≥30 kg/m2.
The new SRS implemented on January 1, 2017 lowered the reimbursement level of non-insulin antidiabetic medications from the Higher (100%) to the Lower Special Refund Category (65%) to achieve savings in medication costs [4,5,6]. This meant a co-payment of 35% of the cost of each purchased non-insulin medication for T2D patients instead of a fixed co-payment (EUR 3.00 in 2014–2015, EUR 4.50 in 2016) for each purchased medication.
Study design
The regional electronic health records (EHRs) from the Joint Municipal Authority for North Karelia Social and Health Services (Siun sote) were utilized in the present study. These regional EHRs cover both primary health care and specialized care. Extracted data consisted of patients with a confirmed T2D diagnosis (based on 10th revision of International Classification of Diseases, ICD-10 [27], code E11) at the end of 2012 (n = 10,204) who were alive on Jan 1, 2017 (n = 8436). Data contained information on diagnoses as well as on laboratory assays. EHR data were compiled with information on reimbursed diabetes medication purchases (such as dispensing date and Anatomical Therapeutic Chemical (ATC) classification code [28]) for the years 1995–2010 and 2016–2017 from the Finnish Prescription Register maintained by the SII. In addition, data on entitlements to higher medication reimbursement due to diabetes before 2011 were retrieved from the Special Reimbursement Register maintained also by the SII.
Outcome measures
In Finland, care of T2D is based on Current Care Guidelines [2] and the general aim of T2D care is to give means for early screening, to prevent complications of diabetes, ensure a balanced treatment and a good life quality for diabetes patients. Typically, HbA1c is used as a measure of long-term blood sugar level reflecting average glycaemic balance over the last 2–8 weeks with values less than 53 mmol/mol (7.0%) considered indicating good treatment balance [2, 29] with some exceptions for older and the most comorbid patients. According to treatment guidelines, HbA1c level should be measured regularly (every 6–12 months).
In the study data, glycaemic control was measured with glycated haemoglobin (HbA1c) with the turbidimetric inhibition immunoanalysis method (TINIA) by the Eastern Finland laboratory (ISLAB, https://www.islab.fi) which is an accredited laboratory and participates external quality surveys. Values were standardised to International Federation of Clinical Chemistry (IFCC) units. Mean HbA1c (mmol/mol) levels were calculated for each month 36 months before and 33 months after the policy change (i.e. January, 2014 – September, 2019) that was introduced on January 1, 2017. In every one-month time-window, data on all patients having measured his/hers HbA1c at that specific window were used. If a patient had more than one HbA1c measurement within a month, the latest one was selected.
Consumption of diabetes medications was estimated with defined daily doses (DDDs, [28]) based on the Prescription register data for the years 2016 and 2017.
Subgroup analyses
Patient’s age and timing of T2D diagnosis were obtained from the EHRs. Timing of T2D diagnosis was ascertained with the Finnish Prescription Register data on diabetes medication purchases and the Special Reimbursement Register data on entitlements to special refund for diabetes medications maintained by the SII. T2D diagnosis date was considered to be the first occurrence of diabetes medication purchase, entitlement to special refund or T2D diagnosis in the electronic patient database. In subgroup analyses, patients were divided to those with T2D duration from 5 to less than 10 years, 10–15 years, and those with T2D duration > 15 years at the time of policy change.
Patients were classified according to the diabetes medication purchases from the Prescription register data in 2016. The following subgroups were formed: users of metformin (ATC code A10BA02) only, users of metformin and other oral antidiabetic medications (A10BA02 + other A10B), users of only other diabetes medications than insulin or metformin (A10B excluding A10BA02 and A10A), users of insulin and oral antidiabetic medication (including metformin) (A10A + A10B), and users of insulin (A10A) only in 2016.
Other variables
Information of concordant and discordant diseases was retrieved from the EHRs and they were measured from the time period before the policy change in Dec 31, 2016. Concordant, T2D-coexisting diseases consisted of hypertension (ICD-10: I10), coronary heart disease (I20–I25), atrial fibrillation (I48), heart failure (I50, I11.0, I13.0, I13.2), peripheral arterial diseases (I70.2, I73.9), stroke (incl. SAH, I60, I61, I63, I64, but excluding I63.6), chronic kidney disease (N18, N19), neuropathies (G59, G63, G73, G99), blindness (H54), or diabetes complications (E11.2–E11.8 sublevels). Discordant diseases consisted of cancers (C00–C43, C45–C97), asthma (J45, J46), gout (M10), glaucoma (H40–H42), depression (F32, F33), dementia (F00–F03, G30), mental diseases (F20–F48), chronic obstructive pulmonary disease (J43–J44), rheumatoid and other arthritis (M05–M13, M32, M33, M45), osteoporosis (M80–M85), neuromuscular diseases (G70–G72), or liver diseases excluding cancers (K70–K77).
Statistical analyses
Differences in baseline characteristics between patients with and without HbA1c measurements during the follow-up were examined using standardized difference that is independent of sample size [30]. Standardized mean difference values > 10% were considered to indicate meaningful differences between the patients.
Interrupted time series [31] design was applied to examine the effect of the policy change on average monthly HbA1c levels. Time periods of 30 days 36 months before and 33 months after the policy change were utilized to define a pre-policy change segment, time of the policy change, and a post- policy change segment. Interrupted time series is a strong quasi-experimental design. It was estimated with segmented linear autoregressive error models [32]. Autocorrelation between the time points was estimated utilizing a Durbin–Watson test [31]. Autocorrelation refers to the dependency of regression residuals over the measured time points. For the results of the Durbin–Watson test, p < 0.05 was considered to indicate statistically significant serial autocorrelation. Autocorrelation was automatically adjusted for in the regression models when needed.
In the primary analysis, data on the total population were utilized. However, subgroup analyses were performed based on age and T2D duration at the time of the policy change as well as diabetes medication use in 2016. Sensitivity analyses against the primary analysis were conducted ruling out time-periods of 1–6 months after policy change (January–June, 2017) to examine the impact of potential lag time on the effect of diabetes medications on HbA1c levels. In addition, in the second sensitivity analysis, two-month time periods instead of one-month periods were applied to stabilize the potential variation due to short time-windows and to increase sample sizes within time-windows. All the analyses were conducted with SAS version 9.4 (SAS Institute Inc., Cary, North Carolina, USA).
Ethics statement
Use of the data was approved by the Ethics Committee of the Northern Savonia Hospital District (diary number 81/2012). The study protocol was also approved by the register administrator, the Joint Municipal Authority for North Karelia Social and Health Services (Siun sote). A separate permission to link data on medication purchases and entitlements to special reimbursements was achieved from the SII (diary number 110/522/2018). Only register-based data were utilized and thus, consent from the patients was not needed.
Results
Patients with at least one HbA1c measurement during 1/2014–9/2019 (n = 8143) were on average 68.1 years (SD 11.3) old at the baseline and 53.0% were female (Table 1). A bit over two thirds (69.2%) were on good glycaemic control (i.e. HbA1c less than 53 mmol/mol) at the time of the policy change. Roughly a third (35.4%) of patients had concordant diseases only in addition to T2D and 9.7% discordant diseases only, whereas 24.6% had both concordant and discordant diseases and 30.3% had neither of them. Most patients used only metformin in 2016, followed by users of insulin and oral antidiabetic medication. Patients without HbA1c measurements (n = 293 or 3.5%) during the time period were on average healthier (no concordant or discordant diseases), but, however, more of them died during the follow-up when compared to patients with HbA1c measurements (7.9% vs. 5.8%, respectively, see Additional file 1).
In the primary analysis, for the total population, the average HbA1c level was 52.4 (95% confidence interval, CI, 51.9–52.9) mmol/mol at the baseline on January, 2014 and HbA1c level increased by 0.07 mmol/mol (95% CI 0.04–0.09) per month until December 2016 (Fig. 1, Table 2). An estimated average increase of 0.81 (95% CI 0.04–1.58) mmol/mol was detected in HbA1c levels at the time of policy change on January, 2017. Thereafter, the average HbA1c level remained stable until September 2019.

Observed time series of average glycaemic control for all patients by month. Estimated trend lines show predicted values from the segmented regression analysis for all patients and by drug groupings
In subgroup analyses, stronger point estimates for immediate changes in HbA1c levels at the time of the policy change than in the primary analysis were detected among patients utilizing only other diabetes medications than insulin or metformin in 2016 (3.56 mmol/mol, 95% CI 2.50–4.62) (Table 2). In addition, stronger point estimates for immediate changes in HbA1c levels at the time of the policy change were also detected among patients aged ≥75 years (Table 2).
In sensitivity analyses, ruling out time-periods of 1 to 6 months (January–June, 2017) after the policy change diluted the effect of the policy change to statistically non-significant except in the analysis excluding the period from January to May (Table 3). Neither using two-month instead of one-month time-windows nor restricting the population to those who survived until October 2019 altered the results from the primary analysis (Table 3).
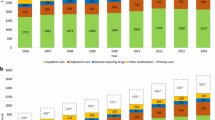
In total, consumption of diabetes medications decreased from 11,619 daily DDDs in 2016 to 11,446 daily DDDs in 2017 among those who were alive on Jan 1, 2018 (Table 4). Meanwhile, the number of purchases increased from 52,050 purchases in 2016 to 56,764 purchases in 2017 and the number of users decreased from 6793 patients in 2016 to 6780 patients in 2017. Number of purchases increased from an average 7.7 (SD 7.4) purchases per patient in 2016 to an average 8.4 (SD 8.2) purchases per patient in 2017 (p < 0.001). Consumption of diabetes medications per patient per purchase decreased from 81.5 (SD 60.9) DDDs/patient/purchase in 2016 to 73.6 (SD 59.3) DDDs/patient/purchase in 2017 (p < 0.001). Even the total consumption of medications calculated as DDDs decreased, the total yearly consumption of diabetes medications per patient who had purchases did not change between 2016 and 2017. In total, consumption of SGLT2 (sodium/glucose cotransporter 2) inhibitors increased heavily from 144,018 DDDs in 2016 to 245,228 DDDs in 2017 whereas consumption of other diabetes medications decreased during the same period (Additional file 2).
Of those utilizing only other diabetes medications than insulin or metformin in 2016 and surviving until Jan 1, 2018 (n = 726), 6.8% started using metformin and 5.9% insulin in addition to other diabetes medications than insulin or metformin in 2017 (Table 5).
Discussion
A small 0.8 mmol/mol (~ 0.08%) immediate increase in average HbA1c levels during the first month after the new SRS was detected in glycaemic control among T2D patients from the North Karelia region, Finland. However, the largest immediate increase (3.56 mmol/mol, 95% CI 2.50–4.62, or 0.33%) was observed among patients utilizing only other diabetes medications than insulin or metformin in 2016. Patients were observed to purchase smaller packages and more frequently after the policy change than before it.
The estimated yearly increase of 0.84 mmol/mol (12*0.07 mmol/mol, 0.08% units) in average HbA1c levels observed in this study until the policy change at the beginning of 2017 is a bit over the magnitude of the estimated increase of 0.75 mmol/mol (0.07% units in HbA1c) per year that was observed in our previous study among the same population in 2011–2016 [33]. The small differences in results are due to differences in densities of follow-up (monthly level in the current study vs. yearly level in the paper by Nazu et al. (2019)) in addition to differences in lengths of follow-up [33]. In the current study, an additional, immediate increase of 0.81 mmol/mol (0.08%) was detected at the time of the policy change in the current study. Thereafter, HbA1c values continued to increase 0.36 mmol/mol (0.03%) per year. Compared with other international publications on changes in treatment balance over time, rates of 1.4–1.5 mmol/mol (0.12–0.14% units in HbA1c) of increase per year are reported [34, 35]. The lower rate of increase in our studies may reflect the early detection and active treatment of T2D patients in the North Karelia region [36]. In addition, SGLT2 inhibitors became reimbursable in 2016 and the price of newer medications, such as GLP-1 analogues, has decreased over the study period increasing their use and, thus, reducing the use of insulins.
The new SRS has already been reported to effect patient’s medication use, cause financial difficulties to purchase diabetes medications, and worsen patient’s satisfaction to diabetes care [20, 21]. In our study, almost 13% of the patients utilizing only other medications than insulin or metformin in 2016 started using metformin or insulin in addition to other diabetes medications in 2017. In our previous study, 28% of patients with T2D reported they discontinued non-insulin diabetes medication use due to financial reasons and 8% had initiated insulin use due to the same reasons within the first 11 months after the implementation of the new SRS [20]. In another study, we also observed that almost half (47%) of the study participants reported some kind of an effect of the co-payment level increase on their life in an open-ended question 11 months after the new SRS coming into effect [21]. Most commonly reported effects were economic effects (33%), such as increased expenditure (17%) or difficulty in purchasing medicines (9%), after the co-payment level increased. However, only 2% reported they had discontinued diabetes medication use.
The previously reported effects of the new SRS [20, 21] may show as a decline in treatment balance observed in the current study. Increases in co-payment levels are also reported to decrease adherence to diabetes medications [15, 16, 37] which may further show as a decline in treatment balance [15]. In addition, the observed results of elevated HbA1c levels at the time of the policy change may be explained by the decreased consumption of diabetes medications between 2016 and 2017. We observed that the number of purchases increased while the number of users decreased due to mortality indicating that the patients purchased smaller packages and more frequently after the policy change than before it. Similar findings were observed at the national level: the consumption of diabetes medications decreased by 1% between August, 2016 and August, 2017 although the number of users increased by 3% [38]. However, the decreasing trend in consumption of diabetes medications observed in both studies may be explained by stockpiling at the end of 2016; patients anticipated the upcoming higher prices and utilized the benefits of possibly reaching the Additional Refund limit. In another previous national level study, the annual co-payment increase was estimated to be EUR 157 on average among those utilizing DPP-4 (dipeptidyl peptidase 4) inhibitors or GLP-1 analogues, while corresponding figure for patients using older antidiabetic medicines (e.g., metformin and sulfonylureas) was EUR 12 [39]. This may be the reason why the largest immediate effects of the new SRS were seen among patients utilizing only other diabetes medications than insulin or metformin in 2016 in this study. To remind, insulins remained in the Higher Special Refund Category (100%) at the time of the policy change. Furthermore, increasing prices may delay initiation of diabetes medications other than insulin or metformin. Further examination on use of these medications is needed among new T2D patients with a longer follow-up.
Strengths of our study are inclusion of all patients with a diagnosed T2D in 2012 in the North Karelia region and application of data on all available HbA1c measurements, and, thus, avoiding selection bias. In addition, all the municipalities of the North Karelia use the same regional laboratory and the same standardized methods for HbA1c testing. Utilization of register-based data allows us to avoid recall bias, too.
However, our study also includes some weaknesses. At the same time of the introduction of the new SRS, the Joint Municipal Authority for North Karelia Social and Health Services (Siun sote) was launched in the North Karelia region, Eastern Finland. Siun sote is a consortium of municipalities and organizes health care services for 14 municipalities in North Karelia instead of each municipality arranging its own services. However, how introduction of new structure for organizing health care services could affect T2D patients and their glycaemic control, remains unknown. To our knowledge, treatment routines remained similar as before the introduction of the consortium. Still, we were not able to separate the effect of the new SRS of that of the new service structure. It should be noted that all the patients included in our study were diagnosed with T2D at least 1 year before the start of the follow-up of HbA1c development and at least 4 years before the policy change in Jan, 2017. In addition, according to our previous study, younger patients with T2D were poorly monitored compared with the older patients in the North Karelia region [33]. Furthermore, we did not have information on patients using private health care services. However, as persons utilizing private health care services are not likely to use only private health care services in the care of T2D due to, for example, economic issues, this is not a big concern.
Conclusions
T2D is a lifelong, progressing disease that, among others, affects quality of life, introduces comorbidities and increases mortality risk [2]. Higher HbA1c levels (> 53 mmol/mol or 7.0%) in turn are reported to increase the risk of micro- and macrovascular complications [17,18,19]. We observed that the co-payment level increase of antidiabetic medications had the strongest, immediate average effect on glycaemic control among those who were utilizing only other diabetes medications than insulin or metformin at the time of the policy change. The observed HbA1c increase of 3.56 mmol/mol (0.33%) at the time of the policy change equals over 17% increase in the risk of microvascular complications, almost 5% increase in the risk of myocardial infarctions and 9% increase in the risk of diabetes related deaths according to the risk models from the UKPDS study [40]. Therefore, future studies are warranted to monitor long-term incidence of complications as well as related health and economic outcomes as an outcome of this policy change in this specific subgroup of patients.
Availability of data and materials
Due to individual privacy law, data sharing is not possible and are not publicly available. An anonymised version of the data is available upon reasonable request from the corresponding author with appropriate permissions of the Joint Municipal Authority For North Karelia Social and Health Services (Siun sote) and the Social Insurance Institute.
Abbreviations
- ATC:
-
Anatomical Therapeutic Chemical
- CI:
-
Confidence interval
- DDD:
-
Defined daily dose
- DPP-4:
-
Inhibitors of dipeptidyl peptidase 4
- EHRs:
-
Electronic health records
- GLP-1:
-
Glucagon-like peptide-1
- ICD-10:
-
10th revision of International Classification of Diseases
- SGLT2:
-
Sodium/glucose cotransporter 2
- SII:
-
The Social Insurance Institute of Finland
- SRS:
-
Special reimbursement scheme
- T2D:
-
Type 2 diabetes
References
Koski S. Diabetes barometer 2019 (in Finnish). The Finnish diabetes association, 2019. Available at: https://diabetes.fi/diabetesbarometri. Accessed January 8, 2020.
Type 2 diabetes, Current Care Guidelines. Working group set up by the Finnish Medical Society Duodecim, the Finnish Society of Internal Medicine and the Medical Advisory Board of the Finnish Diabetes Society. Helsinki: The Finnish Medical Society Duodecim, 2018 (Referred October 26, 2018). Available online at: www.kaypahoito.fi. Accessed January 8, 2020.
Health Statistics for the Nordic Countries 2017. Nordic Medico-Statistical Committee; 2017. p. 108. Available at: https://norden.diva-portal.org/smash/get/diva2:1148509/FULLTEXT05.pdf. Accessed 25 Nov 2020.
Finland, a land of solutions. Strategic Programme of Prime Minister Juha Sipilä’s Government 29 May 2015. Government Publications 12/2015. Available at: https://vnk.fi/documents/10616/1095776/Ratkaisujen+Suomi_EN.pdf/c2f3123a-d891-4451-884a-a8cb6c747ddd/Ratkaisujen+Suomi_EN.pdf.pdf?version=1.0. Accessed January 8, 2020.
Finnish Government. Government proposal 184/2016 [in Finnish]. Available at: https://www.eduskunta.fi/FI/vaski/HallituksenEsitys/Documents/HE_184+2016.pdf. Accessed 8 Jan 2020.
Ruskoaho H. Inspection of the medicine reimbursement scheme regarding the savings in medicines in 2017 [in Finnish]. Reports and memos of the Ministry of Social Affairs and Health 31/2016. Available at: http://urn.fi/URN: ISBN:978–952–00-3815-1. Accessed January 8, 2020.
Finnish medicines agency fimea and social insurance institution. Finnish Statistics on Medicines 2017. Helsinki; 2018. Available at: http://urn.fi/URN:NBN:fi-fe2018112148808. Accessed 25 Nov 2020.
Goldman DP, Joyce GF, Escarce JJ, Pace JE, Solomon MD, Laouri M, Lansman PB, Teutsch SM. Pharmacy benefits and the use of drugs by the chronically ill. JAMA. 2004;291:2344–50.
Roblin DW, Platt R, Goodman MJ, Hsu J, Nelson WW, Smith DH, Andrade SE, Soumerai SB. Effect of increased cost-sharing on oral hypoglycemic use in five managed care organizations: how much is too much? Med Care. 2005;43:951–9.
Barron J, Wahl P, Fisher M, Plauschinat C. Effect of prescription copayments on adherence and treatment failure with oral antidiabetic medications. P T. 2008;33:532–53.
Colombi AM, Yu-Isenberg K, Priest J. The effects of health plan copayments on adherence to oral diabetes medication and health resource utilization. J Occup Environ Med. 2008;50:535–41. https://doi.org/10.1097/JOM.0b013e31816ed011.
Eaddy MT, Cook CL, O’Day K, Burch SP, Cantrell CR. How patient cost-sharing trends affect adherence and outcomes: a literature review. P T. 2012;37:45–55.
Gu Q, Zeng F, Patel BV, Tripoli LC. Part D coverage gap and adherence to diabetes medications. Am J Manag Care. 2010;16:911–8.
Henk HJ, Lopez JMS, Bookhart BK. Novel type 2 diabetes medication access and effect of patient cost sharing. J Manag Care Spec Pharm. 2018;24:847–55. https://doi.org/10.18553/jmcp.2018.24.9.847.
Hunt J, Rozenfeld Y, Shenolikar R. Effect of patient medication cost share on adherence and glycemic control. Manag Care. 2009;18:47–53.
Thornton Snider J, Seabury S, Lopez J, McKenzie S, Wu Y, Goldman DP. Impact of type 2 diabetes medication cost sharing on patient outcomes and health plan costs. Am J Manag Care. 2016;22:433–40.
Selvin E, Marinopoulos S, Berkenblit G, Rami T, Brancati FL, Powe NR, Golden SH. Meta-analysis: glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med. 2004;141:421–31.
Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D, Turner RC, Holman RR. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321:405–12.
UKPDS Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837–53.
Lavikainen P, Aarnio E, Mäntyranta P, Niskanen L, Martikainen J. Short-term impact of co-payment level increase on the use of medication and patient-reported outcomes in Finnish patients with type 2 diabetes. Health Policy. 2020. https://doi.org/10.1016/j.healthpol.2020.08.001.
Suviranta T, Timonen J, Martikainen J, Aarnio E. The effects of reimbursement reform of antidiabetic medicines from the patients’ perspective – a survey among patients with type 2 diabetes in Finland. BMC Health Serv Res. 2019;19:769.
Ministry of Social Affairs and Health. Health Insurance Act 2004/1224 (in Finnish). Available at: https://www.finlex.fi/fi/laki/ajantasa/2004/20041224. Accessed January 8, 2020.
Finnish Medicines Agency Fimea and Social Insurance Institution. Finnish Statistics on Medicines 2015. Helsinki; 2016. Available at: http://urn.fi/URN:NBN:fi-fe2016112829993. Accessed 25 Nov 2020.
Finnish Medicines Agency Fimea and Social Insurance Institution. Finnish Statistics on Medicines 2014. Helsinki; 2015. Available at: http://urn.fi/URN:NBN:fi-fe201602247346. Accessed 25 Nov 2020.
Finnish Medicines Agency Fimea and Social Insurance Institution. Finnish Statistics on Medicines 2016. Helsinki; 2017. Available at: http://urn.fi/URN:NBN:fi-fe2017111750773. Accessed 25 Nov 2020.
Finnish Medicines Agency Fimea and Social Insurance Institution. Finnish Statistics on Medicines 2018. Helsinki; 2019. Available at: http://urn.fi/URN:NBN:fi-fe2019123149481. Accessed 25 Nov 2020.
WHO. International Statistical Classification of Diseases and Related Health Problems 10th revision. Available at: http://apps.who.int/classifications/icd10/browse/2010/en. Accessed October 10, 2019.
WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2020. Oslo; 2019. Available at: http://www.whocc.no/atc_ddd_index/. Accessed 25 Nov 2020.
American Diabetes Association. 8. Pharmacologic Approaches to Glycemic Treatment. Diab Care 2017; 40(Suppl 1):S64–S74. DOI: https://doi.org/10.2337/dc17-S011.
Austin PC. Goodness-of-fit diagnostics for the propensity score model when estimating treatment effects using covariate adjustment with the propensity score. Pharmacoepidemiol Drug Saf. 2008;17:1202–17.
Penfold RB, Zhang F. Use of interrupted time series analysis in evaluating health care quality improvements. Acad Pediatr. 2013;13(Suppl 6):S38–44.
Wagner AK, Soumerai SB, Zhang F, Ross-Degnan D. Segmented regression analysis of interrupted time series studies in medication use research. J Clin Pharm Ther. 2002;27:299–309.
Nazu NA, Lindström J, Rautiainen P, Tirkkonen H, Wikström K, Repo T, Laatikainen T. Maintenance of good glycaemic control is challenging – a cohort study of type 2 diabetes patient in North Karelia, Finland. Int J Clin Pract. 2019;73:e13313.
Donnelly LA, Zhou K, Doney ASF, Jennison C, Franks PW, Pearson ER. Rates of glycaemic deterioration in a real-world population with type 2 diabetes. Diabetologia. 2018;61:607–15.
Kahn SE, Haffner SM, Heise MA, Herman WH, Holman RR, Jones NP, et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006;355:2427–43.
Wikström K, Toivakka M, Rautianen P, Tirkkonen H, Repo T, Laatikainen T. Electronic health records as valuable data sources in health care quality improvement process. Health Serv Res Manag Epidemiol. 2019;6:2333392819852879. https://doi.org/10.1177/2333392819852879.
Gibson TB, Song X, Alemayehu B, Wang SS, Waddell JL, Bouchard JR, Forma F. Cost sharing, adherence, and health outcomes in patients with diabetes. Am J Manag Care. 2010;16(7):589–600.
Kurko T, Martikainen J, Rättö H, Aaltonen K. Consumption of diabetes medications decreased to some extent in 2017 (in Finnish). Kelan Tutkimusblogi, published on March 16, 2018. Available at: https://tutkimusblogi.kela.fi/arkisto/4466.
Kurko T, Heino P, Martikainen JE, Aaltonen K. Use of diabetes drugs and the impact of lowering of the reimbursement rate on diabetic patients’ annual copayments – a microsimulation study [in Finnish with an English abstract]. Finn Med J. 2018;73:1584–9.
Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D, Turner RC, Holman RR. Association of Glycaemia with Macrovascular and Microvascular Complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12.
Acknowledgements
This study has been presented as a poster at the ISPOR Europe 2019 in Copenhagen, Denmark in November 2019 (Lavikainen P, Aarnio E, Jalkanen K, Tirkkonen H, Rautiainen P, Laatikainen T, Martikainen J. PDB76 - Impact of copayment increase of antidiabetic medications on glycaemic control in Finnish patients with type 2 diabetes. Value in Health 2019;22(S3):S586-S587. DOI: https://doi.org/10.1016/j.jval.2019.09.958).
Funding
This study was partly funded by the Social Insurance Institution of Finland (diary number 34/26/2018), Finnish Diabetes Association, the Research Committee of the Kuopio University Hospital Catchment Area for the State Research Funding (project QCARE, Joensuu, Finland), the Strategic Research Council at the Academy of Finland (project IMPRO, 312703).
The funders had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
PL, EA, KJ, TL, and JM planned the study. TL acquired the data. PL pre-processed the data, performed statistical analyses, and drafted the first version of the manuscript. PL had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analyses. PL, EA, KJ, HT, PR, TL, and JM contributed to the interpretation of the data, revised the manuscript, and approved the final manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Use of the data was approved by the Ethics Committee of the Northern Savonia Hospital District (diary number 81/2012). The study protocol was also approved by the register administrator, the Joint Municipal Authority For North Karelia Social and Health Services (Siun sote). A separate permission to link data on drug purchases and special reimbursements was achieved from the Social Insurance Institute (diary number 110/522/2018). We utilized only register-based data and thus, consent from the patients was not needed.
Consent for publication
Not applicable.
Competing interests
JM is a founding partner of ESiOR Oy and a board member of Siltana Oy. These companies were not involved in carrying out this research. PL, EA, KJ, HT, PR and TL declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Characteristics of T2D patients at the time of the co-payment increase on Jan 1, 2017 as frequencies (proportions) unless otherwise stated.
Additional file 2.
Number of purchases and total DDDs by ATC subgroups in 2016 and 2017.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lavikainen, P., Aarnio, E., Jalkanen, K. et al. Impact of co-payment level increase of antidiabetic medications on glycaemic control: an interrupted time-series study among Finnish patients with type 2 diabetes. BMC Health Serv Res 20, 1095 (2020). https://doi.org/10.1186/s12913-020-05952-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-020-05952-6